


Continuous versus Intermittent Enteral Feeding in Critically Ill Children: A Systematic Review
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. PICO and Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Synthesis
3. Results
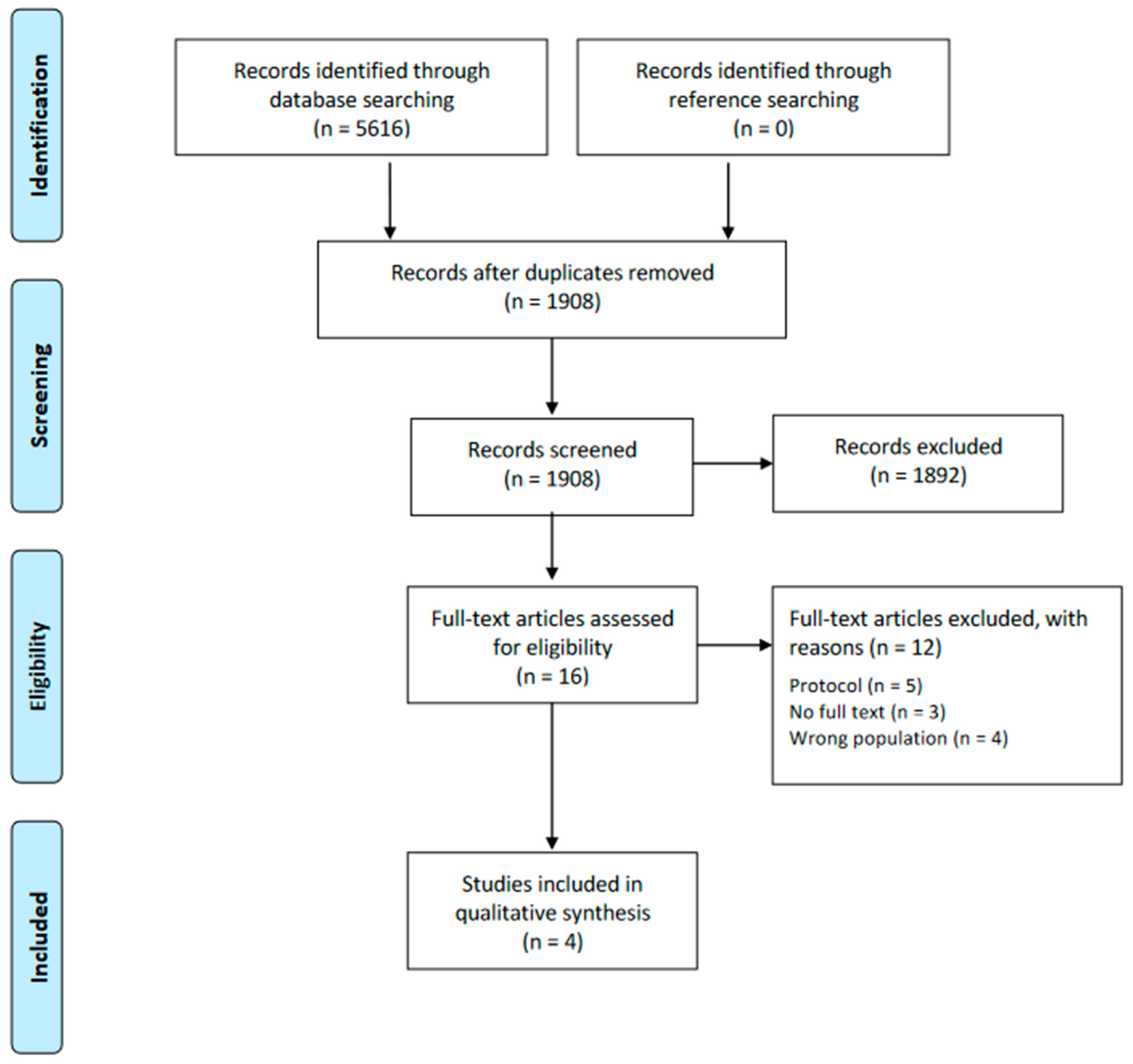
3.1. Selection of Trials
3.2. Trial Characteristics
3.3. Primary Outcomes
3.3.1. Time Taken to Reach Total Target Caloric Intake
3.3.2. Length of PICU Stay
3.3.3. Adverse Events
3.4. Secondary Outcomes
3.4.1. Time Taken to Reach Total Target Protein Intake
3.4.2. Time of Weaning from Mechanical Respiratory Support
3.4.3. Gastric Residual Volume (GRV)
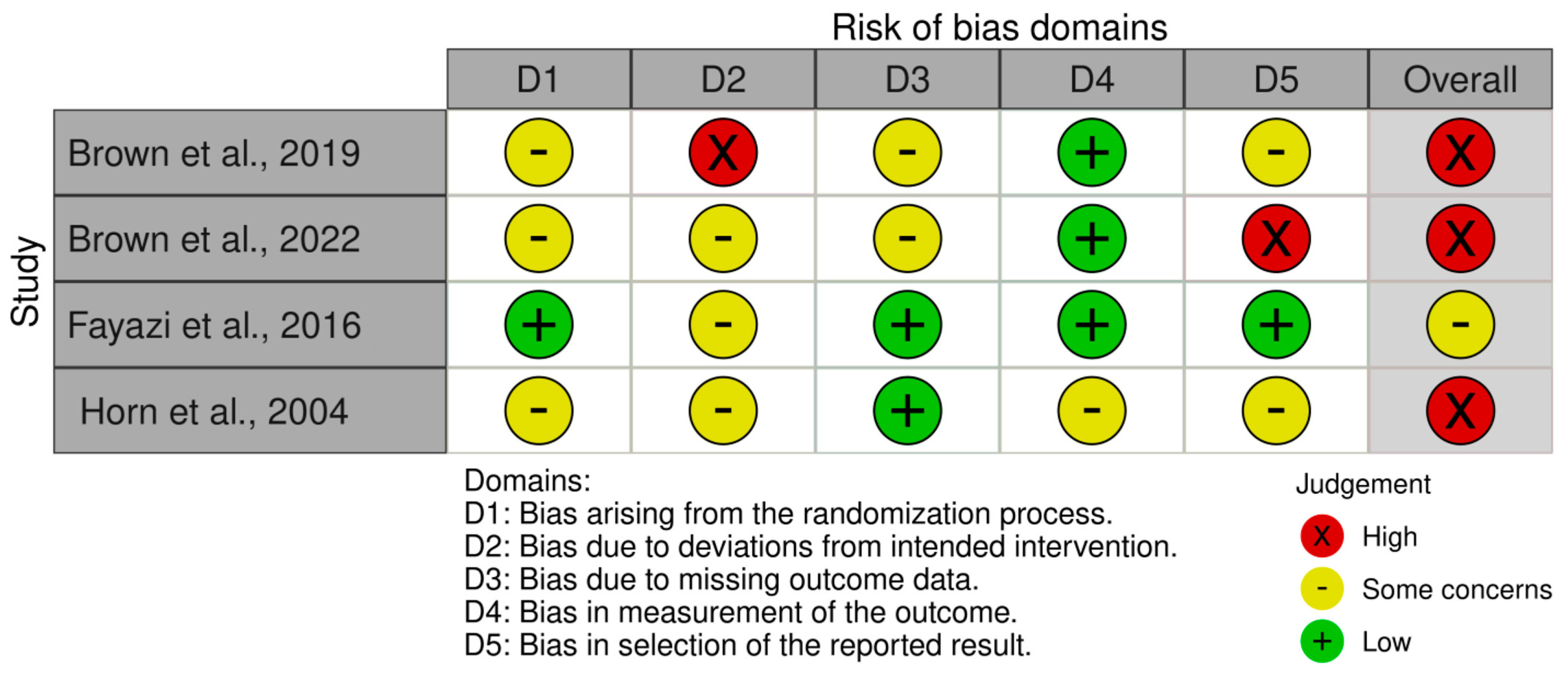
3.5. Risk of Bias Assessment
3.6. Summary of SWiM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- van Puffelen, E.; Hulst, J.M.; Vanhorebeek, I.; Dulfer, K.; van den Berghe, G.; Joosten, K.F.M.; Verbruggen, S.C.A.T. Effect of Late versus Early Initiation of Parenteral Nutrition on Weight Deterioration during PICU Stay: Secondary Analysis of the PEPaNIC Randomised Controlled Trial. Clin. Nutr. 2020, 39, 104–109. [Google Scholar] [CrossRef]
- Littler, H.; Tume, L.N. Is Bolus or Continuous Enteral Feeding Better in Critically Ill Children: An Evidence-Based Review. Nurs. Crit. Care 2022. [Google Scholar] [CrossRef]
- Ventura, J.C.; de Almeida Oliveira, L.D.; Silveira, T.T.; Hauschild, D.B.; Mehta, N.M.; Moreno, Y.M.F. Admission Factors Associated with Nutritional Status Deterioration and Prolonged Pediatric Intensive Care Unit Stay in Critically Ill Children: PICU-ScREEN Multicenter Study. JPEN J. Parenter. Enteral. Nutr. 2022, 46, 330–338. [Google Scholar] [CrossRef]
- Curtis, L.J.; Bernier, P.; Jeejeebhoy, K.; Allard, J.; Duerksen, D.; Gramlich, L.; Laporte, M.; Keller, H.H. Costs of Hospital Malnutrition. Clin. Nutr. 2017, 36, 1391–1396. [Google Scholar] [CrossRef]
- Kratochvíl, M.; Klučka, J.; Klabusayová, E.; Musilová, T.; Vafek, V.; Skříšovská, T.; Djakow, J.; Havránková, P.; Osinová, D.; Štourač, P. Nutrition in Pediatric Intensive Care: A Narrative Review. Children 2022, 9, 1031. [Google Scholar] [CrossRef]
- Eveleens, R.D.; Hulst, J.M.; de Koning, B.A.E.; van Brakel, J.; Rizopoulos, D.; Garcia Guerra, G.; Vanhorebeek, I.; van den Berghe, G.; Joosten, K.F.M.; Verbruggen, S.C.A.T. Achieving Enteral Nutrition during the Acute Phase in Critically Ill Children: Associations with Patient Characteristics and Clinical Outcome. Clin. Nutr. 2021, 40, 1911–1919. [Google Scholar] [CrossRef]
- Abad-Jorge, A. Nutrition Management of the Critically Ill Pediatric Patient. ICAN Infant Child Adolesc. Nutr. 2013, 5, 221–230. [Google Scholar] [CrossRef]
- Tume, L.N.; Valla, F.V. A Review of Feeding Intolerance in Critically Ill Children. Eur. J. Pediatr. 2018, 177, 1675–1683. [Google Scholar] [CrossRef]
- Prieto, M.B.; López-Herce Cid, J. Malnutrition in the Critically Ill Child: The Importance of Enteral Nutrition. Int. J. Environ. Res. Public Health 2011, 8, 4353–4366. [Google Scholar] [CrossRef]
- Tume, L.N.; Eveleens, R.D.; Verbruggen, S.C.A.T.; Harrison, G.; Latour, J.M.; Valla, F.V. Barriers to Delivery of Enteral Nutrition in Pediatric Intensive Care: A World Survey. Pediatr. Crit. Care Med. 2020, 21, E661–E671. [Google Scholar] [CrossRef]
- Moreno, Y.M.F.; Hauschild, D.B.; Barbosa, E.; Bresolin, N.L.; Mehta, N.M. Problems With Optimal Energy and Protein Delivery in the Pediatric Intensive Care Unit. Nutr. Clin. Pract. 2016, 31, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Ichimaru, S. Methods of Enteral Nutrition Administration in Critically Ill Patients: Continuous, Cyclic, Intermittent, and Bolus Feeding. Nutr. Clin. Pract. 2018, 33, 790–795. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.J.; Rosenthal, M.D.; Heyland, D.K. Intermittent versus Continuous Feeding in Critically Ill Adults. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without Meta-Analysis (SWiM) in Systematic Reviews: Reporting Guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Wiley: Hoboken, NJ, USA, 2019; ISBN 9781119536604. [Google Scholar]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-Bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-Bias Assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- McKenzie, J.E.; Brennan, S.E. Synthesizing and Presenting Findings Using Other Methods. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; pp. 321–347. [Google Scholar] [CrossRef]
- Thomson, H.J.; Thomas, S. The Effect Direction Plot: Visual Display of Non-Standardised Effects across Multiple Outcome Domains. Res. Synth. Methods 2013, 4, 95. [Google Scholar] [CrossRef]
- Boon, M.H.; Thomson, H. The Effect Direction Plot Revisited: Application of the 2019 Cochrane Handbook Guidance on Alternative Synthesis Methods. Res. Synth. Methods 2021, 12, 29–33. [Google Scholar] [CrossRef]
- Brown, A.M.; Fisher, E.; Forbes, M.L. Bolus vs. Continuous Nasogastric Feeds in Mechanically Ventilated Pediatric Patients: A Pilot Study. JPEN J. Parenter. Enteral. Nutr. 2019, 43, 750–758. [Google Scholar] [CrossRef]
- Brown, A.M.; Irving, S.Y.; Pringle, C.; Allen, C.; Brown, M.F.; Nett, S.; Singleton, M.N.; Mikhailov, T.A.; Madsen, E.; Srinivasan, V.; et al. Bolus Gastric Feeds Improve Nutrition Delivery to Mechanically Ventilated Pediatric Medical Patients: Results of the COntinuous vs BOlus Multicenter Trial. JPEN J. Parenter. Enteral. Nutr. 2022, 46, 1011–1021. [Google Scholar] [CrossRef]
- Horn, D.; Chaboyer, W. Gastric Feeding in Critically Ill Children: A Randomized Controlled Trial. Am. J. Crit. Care 2003, 12, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Fayazi, S.; Adineh, M.; Fard, S.Z.; Payam, H.F.; Batvandy, Z.A. Comparing Two Methods of Enteral Nutrition in Terms of Their Complications and the Time Needed to Reach Goal Calorie in Children Hospitalized in ICU. Int. J. Pediatr. 2016, 4, 2119–2130. [Google Scholar]
- Horn, D.; Chaboyer, W.; Schluter, P.J. Gastric Residual Volumes in Critically Ill Paediatric Patients: A Comparison of Feeding Regimens. Aust. Crit. Care 2004, 17, 98–103. [Google Scholar] [CrossRef]
- Martinez, E.E.; Bechard, L.J.; Brown, A.-M.; Coss-Bu, J.A.; Kudchadkar, S.R.; Mikhailov, T.A.; Srinivasan, V.; Staffa, S.J.; Verbruggen, S.C.A.T.; Zurakowski, D.; et al. Intermittent versus Continuous Enteral Nutrition in Critically Ill Children: A Pre-Planned Secondary Analysis of an International Prospective Cohort Study. Clin. Nutr. 2022, 41, 2621–2627. [Google Scholar] [CrossRef]
- Thong, D.; Halim, Z.; Chia, J.; Chua, F.; Wong, A. Systematic Review and Meta-Analysis of the Effectiveness of Continuous vs Intermittent Enteral Nutrition in Critically Ill Adults. J. Parenter. Enter. Nutr. 2022, 46, 1243–1257. [Google Scholar] [CrossRef]
- Lee, H.Y.; Lee, J.K.; Kim, H.J.; Ju, D.L.; Lee, S.M.; Lee, J. Continuous versus Intermittent Enteral Tube Feeding for Critically Ill Patients: A Prospective, Randomized Controlled Trial. Nutrients 2022, 14, 664. [Google Scholar] [CrossRef]
- Evans, D.C.; Forbes, R.; Jones, C.; Cotterman, R.; Njoku, C.; Thongrong, C.; Tulman, D.; Bergese, S.D.; Thomas, S.; Papadimos, T.J.; et al. Continuous versus Bolus Tube Feeds: Does the Modality Affect Glycemic Variability, Tube Feeding Volume, Caloric Intake, or Insulin Utilization? Int. J. Crit. Illn. Inj. Sci. 2016, 6, 9–15. [Google Scholar] [CrossRef]
- MacLeod, J.B.A.; Lefton, J.; Houghton, D.; Roland, C.; Doherty, J.; Cohn, S.M.; Barquist, E.S. Prospective Randomized Control Trial of Intermittent versus Continuous Gastric Feeds for Critically Ill Trauma Patients. J. Trauma 2007, 63, 57–61. [Google Scholar] [CrossRef]
- Yasuda, H.; Kondo, N.; Yamamoto, R.; Asami, S.; Abe, T.; Tsujimoto, H.; Tsujimoto, Y.; Kataoka, Y. Monitoring of Gastric Residual Volume during Enteral Nutrition. Cochrane Database Syst. Rev. 2021, 9, CD013335. [Google Scholar] [CrossRef]
- McClave, S.A.; Dibaise, J.K.; Mullin, G.E.; Martindale, R.G. ACG Clinical Guideline: Nutrition Therapy in the Adult Hospitalized Patient. Am. J. Gastroenterol. 2016, 111, 315–334. [Google Scholar] [CrossRef]
- Dorling, J.; Tume, L.; Arch, B.; Woolfall, K.; Latten, L.; Roper, L.; Deja, E.; Pathan, N.; Eccleson, H.; Hickey, H.; et al. Gastric Residual Volume Measurement in British Neonatal Intensive Care Units: A Survey of Practice. BMJ Paediatr. Open 2020, 4, e000601. [Google Scholar] [CrossRef]
- Tume, L.N.; Arch, B.; Woolfall, K.; Latten, L.; Deja, E.; Roper, L.; Pathan, N.; Eccleson, H.; Hickey, H.; Brown, M.; et al. Gastric Residual Volume Measurement in UK Paediatric Intensive Care Units: A Survey of Practice. Pediatr. Crit. Care Med. 2019, 20, 707. [Google Scholar] [CrossRef]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient. J. Parenter. Enter. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef]
- Al Tamimi, D.; Ahmad, M. Risk of Malnutrition and Clinical Outcomes Among Mechanically Ventilated Patients in Intensive Care Units. Dimens. Crit. Care Nurs. 2022, 41, 18–23. [Google Scholar] [CrossRef]
- Albadi, M.S.; Bookari, K. Is Undernutrition Associated With Deterioration of Outcomes in the Pediatric Intensive Care Unit (PICU): Systematic and Meta-Analysis Review. Front. Pediatr. 2022, 10, 519. [Google Scholar] [CrossRef]
- Zevallos, M.S.C.; Jara, K.S.S.; Ramírez, C.A.C.; Carreazo, N.Y. Impact of Early Enteral Nutrition on the Hospital Stay of Pediatric Patients Undergoing Mechanical Ventilation. J. Pediatr. Intensive Care 2022. [Google Scholar] [CrossRef]
- Sirianansopa, K.; Rassameehirun, C.; Chomtho, S.; Suteerojntrakool, O.; Kongkiattikul, L. Optimal Enteral Nutrition Support Preserved Muscle Mass in Critically Ill Children. J. Nutr. Metab. 2022, 2022, 7004543. [Google Scholar] [CrossRef]
- Davis, T.A.; Fiorotto, M.L.; Suryawan, A. Bolus versus Continuous Feeding to Optimize Anabolism in Neonates. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 102. [Google Scholar] [CrossRef]
- Klingenberg, C.; Embleton, N.D.; Jacobs, S.E.; O’Connell, L.A.F.; Kuschel, C.A. Enteral Feeding Practices in Very Preterm Infants: An International Survey. Arch. Dis. Child. Fetal. Neonatal. Ed. 2012, 97, F56–F61. [Google Scholar] [CrossRef]
- Pahsini, K.; Marinschek, S.; Khan, Z.; Dunitz-Scheer, M.; Jaron Scheer, P. Unintended Adverse Effects of Enteral Nutrition Support: Parental Perspective. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 169–173. [Google Scholar] [CrossRef]
- Veldscholte, K.; Cramer, A.B.G.; de Jonge, R.C.J.; Eveleens, R.D.; Joosten, K.F.M.; Verbruggen, S.C.A.T. Continuous Versus Intermittent Nutrition in Pediatric Intensive Care Patients: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2022, 11, e36229. [Google Scholar] [CrossRef]
- Dobrescu, A.I.; Nussbaumer-Streit, B.; Klerings, I.; Wagner, G.; Persad, E.; Sommer, I.; Herkner, H.; Gartlehner, G. Restricting Evidence Syntheses of Interventions to English-Language Publications Is a Viable Methodological Shortcut for Most Medical Topics: A Systematic Review. J. Clin. Epidemiol. 2021, 137, 209–217. [Google Scholar] [CrossRef]
- Courtney, A.; Bernard, A.; Burgess, S.; Davies, K.; Foster, K.; Kapoor, V.; Epid, M.; Levitt, D.; Sly, P.D. Bolus Versus Continuous Nasogastric Feeds for Infants With Bronchiolitis: A Randomized Trial. Hosp. Pediatr. 2021, 12, 1–10. [Google Scholar] [CrossRef]
- Dhingra, A.; Agrawal, S.K.; Kumar, P.; Narang, A. A randomised controlled trial of two feeding schedules in neonates weighing ≤ 1750 g. J. Matern. Neonatal Med. 2009, 22, 198–203. [Google Scholar] [CrossRef]
- Dmytriiev, D.; Katilov, O. PP039-SUN: Initial Trophic VS Full Enteral Feeding in Children After Thoracic Operation. Clin. Nutr. 2014, 33, S33. [Google Scholar] [CrossRef]
- Kamath, P.; Longden, J.; Stack, C.; Mayer, A. A randomised prospective trial to compare the efficacy of bolus versus continuous nasogastric feeding in paediatric intensive care. Crit. Care 2009, 13, P142. [Google Scholar] [CrossRef]
- Macdonald, P.D.; Skeoch, C.H.; Carse, H.; Dryburgh, F.; Alroomi, L.G.; Galea, P.; Gettinby, G. Randomised trial of continuous nasogastric, bolus nasogastric, and transpyloric feeding in infants of birth weight under 1400 g. Arch. Dis. Child. 1992, 67, 429–431. [Google Scholar] [CrossRef]
- Bolus Versus Continuous Feeding Regimens Post Gastrostomy Tube Placement. Available online: https://clinicaltrials.gov/ct2/show/NCT02006953 (accessed on 10 December 2013).
- COntinuous vs BOlus Nasogastric Feeding in Mechanically Ventilated Pediatric Patients 2 (COBO2). Available online: https://clinicaltrials.gov/ct2/show/NCT02566070 (accessed on 1 October 2015).
- Parker, P.; Stroop, S.; Greene, H. A controlled comparison of continuous versus intermittent feeding in the treatment of infants with intestinal disease. J. Pediatr. 1981, 99, 360–364. [Google Scholar] [CrossRef]
- Silvestre, M.A.A.; Morbach, C.A.; Brans, Y.W.; Shankaran, S. A prospective randomized trial comparing continuous versus intermittent feeding methods in very low birth weight neonates. J. Pediatr. 1996, 128, 748–752. [Google Scholar] [CrossRef]
- Does Volume-Based Enteral Feeding Improve Nutrient Delivery in Hospitalized Critically Ill Children? Available online: https://clinicaltrials.gov/ct2/show/NCT05286177 (accessed on 1 October 2015).



{kind=link}
{kind=link}
| First Author, Year, Country | Protocol | Masking | Population | Participants (N) | Primary Diagnosis | Age Range | Intervention | Intervention Feeding Route | Comparator | Comparator Feeding Route |
|---|---|---|---|---|---|---|---|---|---|---|
| Brown, 2022 [22], USA | NCT02566070 | Unblinded | Mechanically ventilated PICU patients | 158 | Cardiovascular, hematologic, infections, injury/poisoning/adverse events, neurologic, oncologic, respiratory | BGF | Nasogastric feeding | Continuous feeding | CGF | |
| Brown, 2019 [21], USA | N/A | N/R | Intubated critically ill PICU patients | 25 | Respiratory, cardiac, post-operative | 1.0–80.3 months | BGF | Nasogastric feeding | Continuous feeding | CGF |
| Fayazi, 2016 [24], Iran | IRCT201109287655N1 | N/R | Pediatric patients hospitalized in the ICU | 60 | N/A | 5–17 years old | Intermittent nutrition method by using NGT or OGT | Nasogastric or Orophagial-gastric feeding | Continuous feeding | Nasogastric or Orophagial-gastric feeding, feeding pump |
| Horn, 2003 [23], Australia | N/A | N/R | Paediatric patients admitted to the PICU | 45 | N/A | 0.0–153.0 months | Intermittent gastric feeds | Polyvinyl gastric tube of an appropriate size | Continuous feeding | Polyvinyl gastric tube of an appropriate size, feeding pump |
| Adverse Events | Horn et al., 2003 [23] Horn et al., 2004 [25] | Fayazi et al., 2016 [24] | Brown et al., 2019 [21] | Brown et al., 2022 [22] | ||||
|---|---|---|---|---|---|---|---|---|
| Number of participants | IF 23 | CF 22 | IF 30 | CF 30 | BF 11 | CF 14 | BF 72 | CF 75 |
| Emesis | 5 (22.0%) | 4 (18.0%) | 5 (16.7%) | 5 (16.7%) | 2 (18.2%) | 1 (7.1%) | 6 (8.3%) | 14 (18.7%) |
| Diarrhea | 9 (39.0%) | 6 (27.0%) | 14 (46.7%) | 18 (60.0%) | ||||
| Incidence of food intolerance | 18 (60.0%) | 9 (30.0%) | ||||||
| Procedures | 1 (9.1%) | 1 (7.1%) | 2 (2.8%) | 6 (8.0%) | ||||
| Worsening clinical status | 4 (5.6%) | 2 (2.7%) | ||||||
| Elevated GRV | 1 (9.1%) | 1 (7.1%) | 4 (5.6%) | 3 (4.0%) | ||||
| Consecutive measures of elevated GRV | 0 (0.0%) | 2 (14.3%) | 16 (22.2%) | 23 (30.7%) | ||||
| Elevated GRV and abdominal girth | 0 (0.0%) | 1 (7.1%) | ||||||
| Proportion of GRV values above 5 mL/kg | 6 (26.0%) | 6 (27.0%) | ||||||
| Other | 1 (9.1%) | 2 (14.3%) | 6 (8.3%) | 2 (2.7%) | ||||
| Study | Study Design | Time Taken to Reach Total Target Caloric Intake | Length of PICU | Time to Weaning from MV |
|---|---|---|---|---|
| Horn et al., 2003 [23] | RCT | |||
| Fayazi et al., 2016 [24] | RCT | ▲ a | ◀▶ | |
| Brown et al., 2019 [21] | RCT | ◀▶ | ||
| Brown et al., 2022 [22] | RCT |  b b |  |
 —no change/mixed effects/conflicting results. Sample size: final sample size (individuals) in the intervention group: medium arrow
—no change/mixed effects/conflicting results. Sample size: final sample size (individuals) in the intervention group: medium arrow  50–300; small arrow ▲ < 50. Study quality (according to RoB 2.0 assessment) denoted by row color: green—low risk of bias; yellow—some concerns; red—high risk of bias.
50–300; small arrow ▲ < 50. Study quality (according to RoB 2.0 assessment) denoted by row color: green—low risk of bias; yellow—some concerns; red—high risk of bias.Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theodoridis, X.; Chrysoula, L.; Evripidou, K.; Kalaitzopoulou, I.; Chourdakis, M. Continuous versus Intermittent Enteral Feeding in Critically Ill Children: A Systematic Review. Nutrients 2023, 15, 288. https://doi.org/10.3390/nu15020288
Theodoridis X, Chrysoula L, Evripidou K, Kalaitzopoulou I, Chourdakis M. Continuous versus Intermittent Enteral Feeding in Critically Ill Children: A Systematic Review. Nutrients. 2023; 15(2):288. https://doi.org/10.3390/nu15020288
Chicago/Turabian StyleTheodoridis, Xenophon, Lydia Chrysoula, Kleo Evripidou, Ioustini Kalaitzopoulou, and Michail Chourdakis. 2023. "Continuous versus Intermittent Enteral Feeding in Critically Ill Children: A Systematic Review" Nutrients 15, no. 2: 288. https://doi.org/10.3390/nu15020288
APA StyleTheodoridis, X., Chrysoula, L., Evripidou, K., Kalaitzopoulou, I., & Chourdakis, M. (2023). Continuous versus Intermittent Enteral Feeding in Critically Ill Children: A Systematic Review. Nutrients, 15(2), 288. https://doi.org/10.3390/nu15020288