
Australian Ready Meals: Does a Higher Health Star Rating Mean Lower Sodium Content?

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
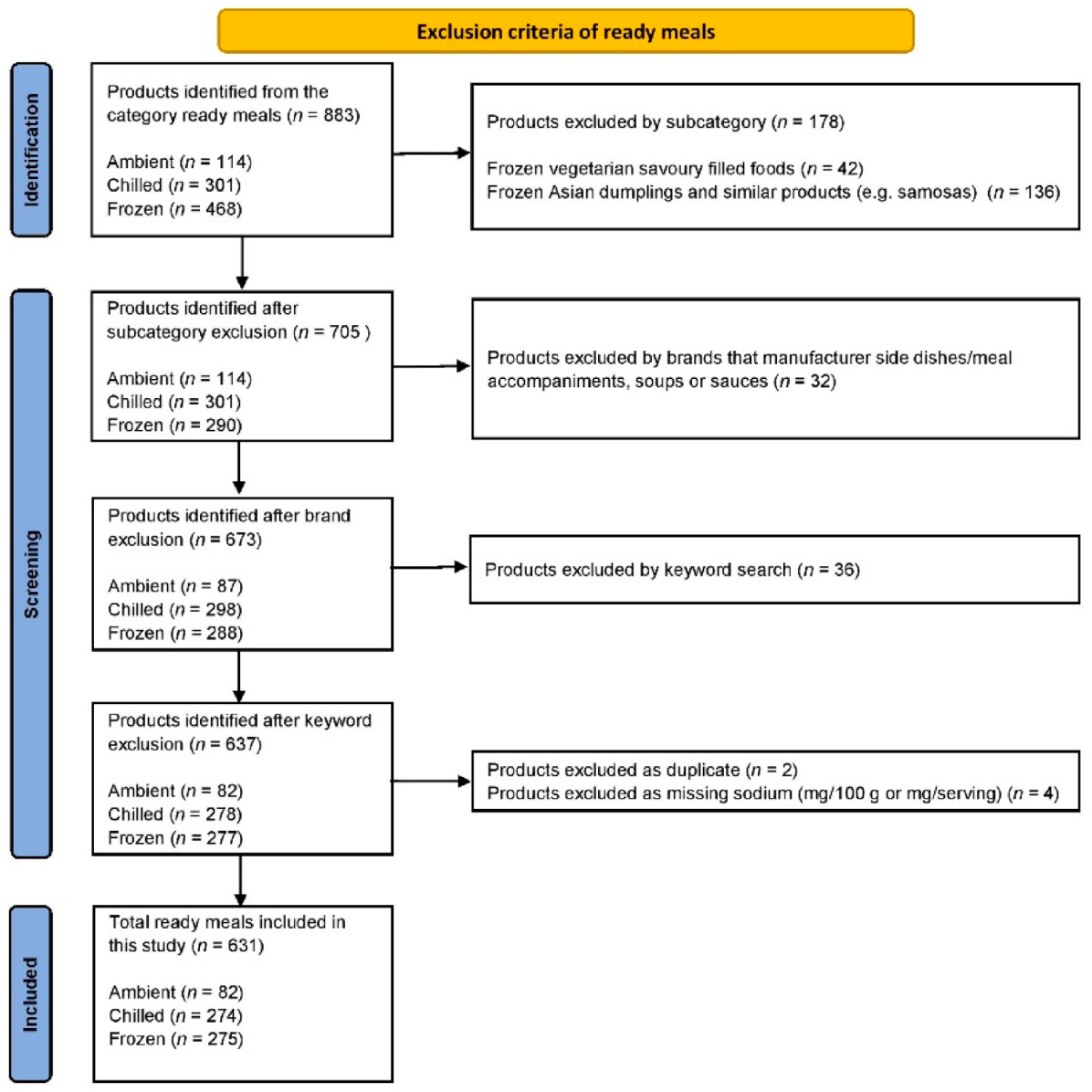
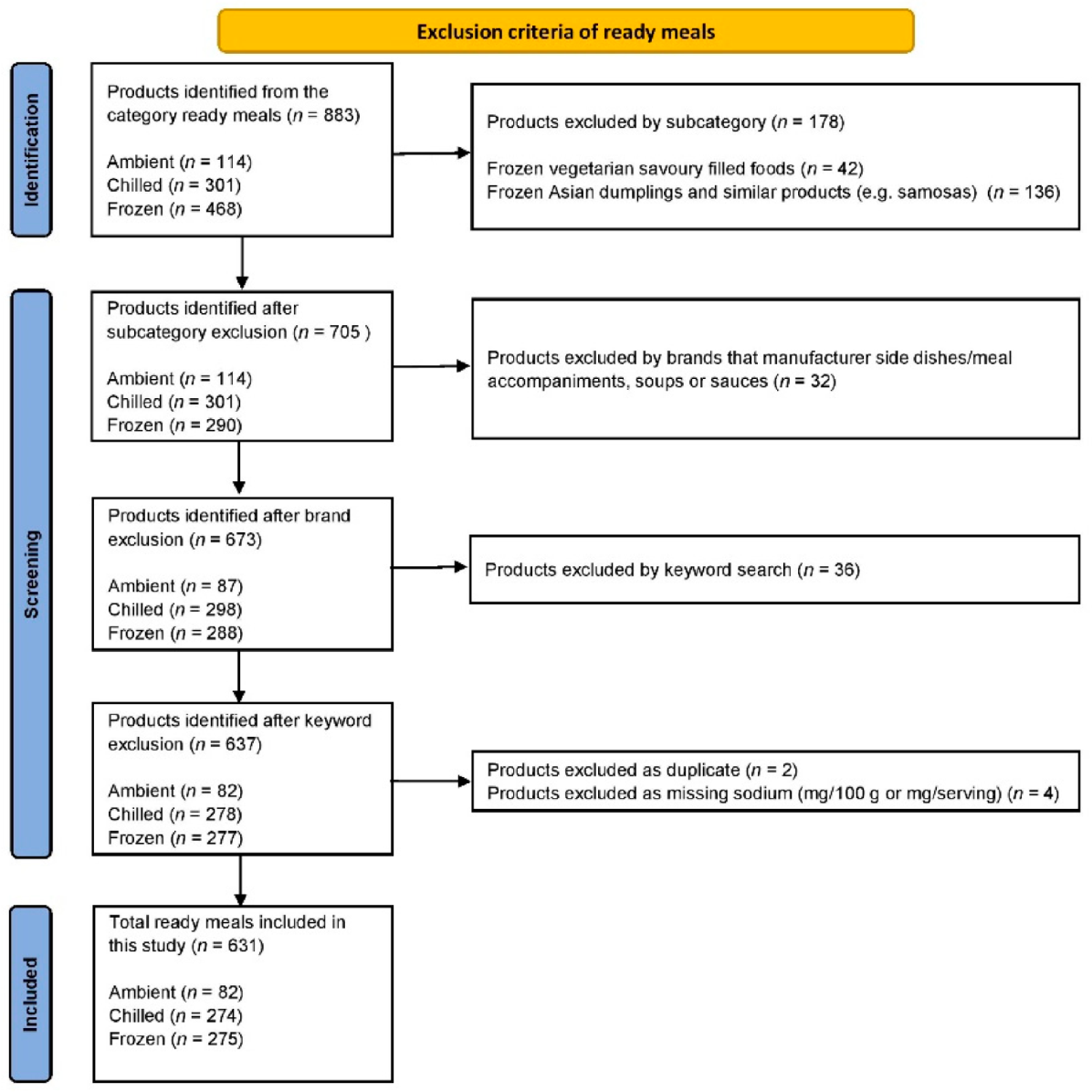
2.1. Data Collection Process
2.2. Product Inclusion
2.3. Data Analysis
3. Results
3.1. All Ready Meals and Subcategories
3.2. Comparison of Products with and without HSR
3.3. Comparison by Health Star Rating
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Venn, D.; Banwell, C.; Dixon, J. Australia’s evolving food practices: A risky mix of continuity and change. Public Health Nutr. 2017, 2014, 2549–2558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christoforou, A.K.; Dunford, E.K.; Neal, B.C. Changes in the Sodium Content of Australian Ready Meals between 2008 and 2011. Asia Pac. J. Clin. Nutr. 2013, 221, 138–143. [Google Scholar]
- Van der Horst, K.; Brunner, T.A.; Siegrist, M. Ready-meal consumption: Associations with weight status and cooking skills. Public Health Nutr. 2011, 142, 239–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celnik, D.; Gillespie, L.; Lean, M.E.J. Time-scarcity, ready-meals, ill-health and the obesity epidemic. Trends Food Sci. Technol. 2012, 271, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Wooldridge, K.; Riley, M.D.; Hendrie, G.A. Growth of Ready Meals in Australian Supermarkets: Nutrient Composition, Price and Serving Size. Foods 2021, 107, 1667. [Google Scholar] [CrossRef] [PubMed]
- Farrand, C.; Joseph, S. Changes in Salt Levels in Ready Meals, Australia (2010–2017); The George Institute for Global Health and VicHealth: Sydney, Australia, 2017. [Google Scholar]
- Food and Drink Business. The Rise of Ready Meals. 2020. Available online: https://www.foodanddrinkbusiness.com.au/news/the-rise-of-ready-meals (accessed on 11 October 2021).
- Webster, J.L.; Dunford, E.K.; Neal, B.C. A systematic survey of the sodium contents of processed foods. Am. J. Clin. Nutr. 2010, 912, 413–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, M.; Brunton, N.P.; Wilkinson, M.G. Sodium and ready meals: A survey of Irish consumer awareness: Sodium and ready meals: Irish consumer awareness. Int. J. Consum. Stud. 2012, 363, 317–326. [Google Scholar] [CrossRef]
- AlOudat, M.; Magyar, N.; Simon-Sarkadi, L.; Lugasi, A. Nutritional content of ready-to-eat meals sold in groceries in Hungary. Int. J. Gastron. Food Sci. 2021, 24, 100318. [Google Scholar] [CrossRef]
- Depatment of Health. Healthy Food Partnership. Available online: https://www.health.gov.au/initiatives-and-programs/healthy-food-partnership (accessed on 11 October 2021).
- Department of Health. Healthy Food Partnership—Reformulation Working Group. 2021. Available online: https://www.health.gov.au/committees-and-groups/healthy-food-partnership-reformulation-working-group (accessed on 11 October 2021).
- Department of Health. Partnership Reformulation Program—Summary of Submissions and Reformulation Working Group Considerations. 2021. Available online: https://www.health.gov.au/resources/publications/partnership-reformulation-program-summary-of-submissions-and-reformulation-working-group-considerations (accessed on 28 January 2022).
- Mente, A.; O’Donnell, M.J.; Rangarajan, S.; McQueen, M.J.; Poirier, P.; Wielgosz, A.; Morrison, H.; Li, W.; Wang, X.; Di, C.; et al. Association of Urinary Sodium and Potassium Excretion with Blood Pressure. N. Engl. J. Med. 2014, 3717, 601–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Salt Intake. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3082 (accessed on 11 October 2021).
- Santos, J.A.; Webster, J.; Land, M.-A.; Flood, V.; Chalmers, J.; Woodward, M.; Neal, B.; Petersen, K.S. Dietary salt intake in the Australian population. Public Health Nutr. 2017, 2011, 1887–1894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health. The Health Star Rating System. Available online: http://healthstarrating.gov.au/internet/healthstarrating/publishing.nsf/content/home (accessed on 11 October 2021).
- Health Star Rating Advisory Committee (HSRAC). Guidance for Industry. 2021. Available online: http://www.healthstarrating.gov.au/internet/healthstarrating/publishing.nsf/Content/guide-for-industry (accessed on 11 October 2021).
- Mpconsulting. Health Star Rating System Five Year Review Report. 2019. Available online: http://www.healthstarrating.gov.au/internet/healthstarrating/publishing.nsf/Content/D1562AA78A574853CA2581BD00828751/$File/Health-Star-Rating-System-Five-Year-Review-Report.pdf (accessed on 11 October 2021).
- Dunford, E.; Webster, J.; Metzler, A.B.; Czernichow, S.; Mhurchu, C.N.; Wolmarans, P.; Snowdon, W.; L’Abbe, M.; Li, N.; Maulik, P.K.; et al. International collaborative project to compare and monitor the nutritional composition of processed foods. Eur. J. Prev. Cardiol. 2012, 196, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- Finder. Supermarket Statistics 2021. Available online: https://www.finder.com.au/supermarket-statistics-2021 (accessed on 23 August 2021).
- Dunford, E.; Trevena, H.; Goodsell, C.; Ng, K.H.; Webster, J.; Millis, A.; Goldstein, S.; Hugueniot, O.; Neal, B. FoodSwitch: A Mobile Phone App to Enable Consumers to Make Healthier Food Choices and Crowdsourcing of National Food Composition Data. JMIR mHealth uHealth 2014, 23, e3230. [Google Scholar] [CrossRef] [PubMed]
- Cooper, S.L.; Butcher, L.M.; Scagnelli, S.D.; Lo, J.; Ryan, M.M.; Devine, A.; O’Sullivan, T.A. Australian Consumers Are Willing to Pay for the Health Star Rating Front-of-Pack Nutrition Label. Nutrients 2020, 1212, 3876. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. HSR System Changes. 2020. Available online: http://www.healthstarrating.gov.au/internet/healthstarrating/publishing.nsf/Content/HSR-system-changes2020 (accessed on 12 October 2021).
- Bablani, L.; Ni Mhurchu, C.; Neal, B.; Skeels, C.L.; Staub, K.E.; Blakely, T. The impact of voluntary front-of-pack nutrition labelling on packaged food reformulation: A difference-in-differences analysis of the Australasian Health Star Rating scheme. PLoS Med. 2020, 1711, e1003427. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Liu, W.G.A.; Rangan, A.; Gemming, L. A comparison of the Health Star Rating and nutrient profiles of branded and generic food products in Sydney supermarkets, Australia. Public Health Nutr. 2019, 2211, 2132–2139. [Google Scholar] [CrossRef] [PubMed]
- Mhurchu, C.N.; Eyles, H.; Choi, Y.-H. Effects of a Voluntary Front-of-Pack Nutrition Labelling System on Packaged Food Reformulation: The Health Star Rating System in New Zealand. Nutrients 2017, 98, 918. [Google Scholar] [CrossRef] [PubMed]
- Centre for Population Health. Healthy Food and Drink in NSW Health Facilities for Staff and Visiters Framework. 2017. Available online: https://www.health.nsw.gov.au/heal/Publications/hfd-framework.pdf (accessed on 8 September 2021).
- Crino, M.; Sacks, G.; Dunford, E.; Trieu, K.; Webster, J.; Vandevijvere, S.; Swinburn, B.; Wu, J.Y.; Neal, B. Measuring the Healthiness of the Packaged Food Supply in Australia. Nutrients 2018, 106, 702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vyth, E.L.; Steenhuis, I.H.M.; Roodenburg, A.J.C.; Brug, J.; Seidell, J.C. Front-of-pack Nutrition label stimulates healthier product development: A quantitative analysis. Int. J. Behav. Nutr. Phys. Act. 2010, 71, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Ready Meals 2019 | Health Star Rating | |||
|---|---|---|---|---|
| All Ready Meals | Yes | No | p-Value | |
| All ready meals, n (%) | 631 (100) | 329 (52) | 302 (48) | |
| Serving size (g), median (IQR) | 340 (90) | 350 (95) | 320 (100) | <0.001 |
| Sodium content (mg/100 g), median (IQR) | 250 (123) | 238 (91) | 274 (152) | <0.001 |
| Sodium content (mg/serving), median (IQR) | 763 (325) | 753 (286) | 772 (425) | 0.134 |
| Proportion < 250 mg/100 g, n (%) | 311 (49) | 184 (56) | 127 (42) | <0.001 |
| Ambient ready meals, n (%) | 82 (13) | 43 (52) | 39 (48) | |
| Serving size (g), median (IQR) | 213 (151) | 250 (160) | 206 (130) | 0.780 |
| Sodium content, mg/100 g, median (IQR) | 300 (174) | 264 (113) | 356 (155) | 0.001 |
| Sodium content, mg/serving, median (IQR) | 735 (372) | 725 (481) | 757 (446) | 0.059 |
| Proportion < 250 mg/100 g, n (%) | 21 (26) | 16 (37) | 5 (13) | 0.012 |
| Chilled ready meals, n (%) | 274 (43) | 122 (45) | 152 (55) | |
| Serving size (g), median (IQR) | 350 (75) | 350 (106) | 330 (73) | 0.020 |
| Sodium content, mg/100 g, median (IQR) | 233 (145) | 217 (106) | 249 (160) | 0.010 |
| Sodium content, mg/serving, median (IQR) | 730 (400) | 683 (294) | 795 (576) | 0.011 |
| Proportion < 250 mg/100 g, n (%) | 157 (57) | 81 (66) | 76 (50) | 0.006 |
| Frozen ready meals, n (%) | 275 (44) | 164 (60) | 111 (40) | |
| Serving size (g), median (IQR) | 350 (75) | 350 (80) | 320 (100) | <0.001 |
| Sodium content, mg/100 g, median (IQR) | 251 (88) | 240 (77) | 274 (117) | 0.017 |
| Sodium content, mg/serving, median (IQR) | 791 (315) | 799 (305) | 767 (345) | 0.251 |
| Proportion < 250 mg/100 g, n (%) | 133 (48) | 87 (53) | 46 (41) | 0.059 |
| Ready Meals 2019 | Health Star Rating (HSR) | ||||
|---|---|---|---|---|---|
| No HSR | ≤3 Stars | 3.5 Stars | ≥4 Stars | p-Value | |
| All ready meals, n (%) | 302 (48) | 60 (18) | 188 (57) | 81 (25) | |
| Serving size (g), median (IQR) | 320 (100) | 335 (186) | 350 (94) | 350 (80) | 0.212 |
| Sodium content, mg/100 g, median (IQR) | 274 (152) | 280 (154) | 240 (83) | 190 (86) | <0.001 |
| Sodium content, mg/serving, median (IQR) | 772 (425) | 943 (524) | 770 (237) | 634 (249) | <0.001 |
| Proportion <250 mg/100 g, n (%) | 127 (42) | 17 (28) | 100 (53) | 67 (83) | <0.001 |
| Ambient ready meals, n (%) | 39 (48) | 12 (28) | 25 (58) | 6 (14) | |
| Serving size (g), median (IQR) | 206 (130) | 206 (209) | 250 (144) | 195 (175) | 0.452 |
| Sodium content, mg/100 g, median (IQR) | 356 (155) | 240 (199) | 275 (114) | 274 (152) | 0.365 |
| Sodium content, mg/serving, median (IQR) | 757 (446) | 734 (670) | 729 (310) | 574 (395) | 0.284 |
| Proportion <250 mg/100 g †, n (%) | 5 (13) | 7 (58) | 7 (28) | 2 (33) | 0.221 |
| Chilled ready meals, n (%) | 152 (55) | 18 (15) | 54 (44) | 50 (41) | |
| Serving size (g), median (IQR) | 330 (73) | 275 (108) | 350 (79) | 350 (50) | 0.002 |
| Sodium content, mg/100 g, median (IQR) | 249 (160) | 283 (230) | 232 (100) | 177 (80) | <0.001 |
| Sodium content, mg/serving, median (IQR) | 795 (576) | 820 (434) | 729 (260) | 626 (278) | <0.001 |
| Proportion <250 mg/100 g, n (%) | 76 (50) | 4 (22) | 32 (59) | 45 (90) | <0.001 |
| Frozen ready meals, n (%) | 111 (40) | 30 (18) | 109 (66) | 25 (15) | |
| Serving size (g), median (IQR) | 320 (100) | 388 (85) | 350 (75) | 350 (73) | 0.066 |
| Sodium content, mg/100 g, median (IQR) | 274 (117) | 300 (128) | 238 (77) | 223 (67) | <0.001 |
| Sodium content, mg/serving, median (IQR) | 767 (345) | 1058 (538) | 795 (205) | 689 (216) | <0.001 |
| Proportion <250 mg/100 g, n (%) | 46 (41) | 6 (20) | 61 (56) | 20 (80) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davies, A.; Santos, J.A.; Rosewarne, E.; Rangan, A.; Webster, J. Australian Ready Meals: Does a Higher Health Star Rating Mean Lower Sodium Content? Nutrients 2022, 14, 1269. https://doi.org/10.3390/nu14061269
Davies A, Santos JA, Rosewarne E, Rangan A, Webster J. Australian Ready Meals: Does a Higher Health Star Rating Mean Lower Sodium Content? Nutrients. 2022; 14(6):1269. https://doi.org/10.3390/nu14061269
Chicago/Turabian StyleDavies, Alyse, Joseph Alvin Santos, Emalie Rosewarne, Anna Rangan, and Jacqui Webster. 2022. "Australian Ready Meals: Does a Higher Health Star Rating Mean Lower Sodium Content?" Nutrients 14, no. 6: 1269. https://doi.org/10.3390/nu14061269
APA StyleDavies, A., Santos, J. A., Rosewarne, E., Rangan, A., & Webster, J. (2022). Australian Ready Meals: Does a Higher Health Star Rating Mean Lower Sodium Content? Nutrients, 14(6), 1269. https://doi.org/10.3390/nu14061269