
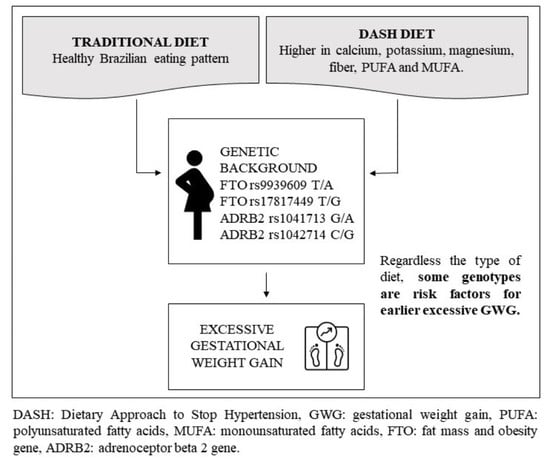
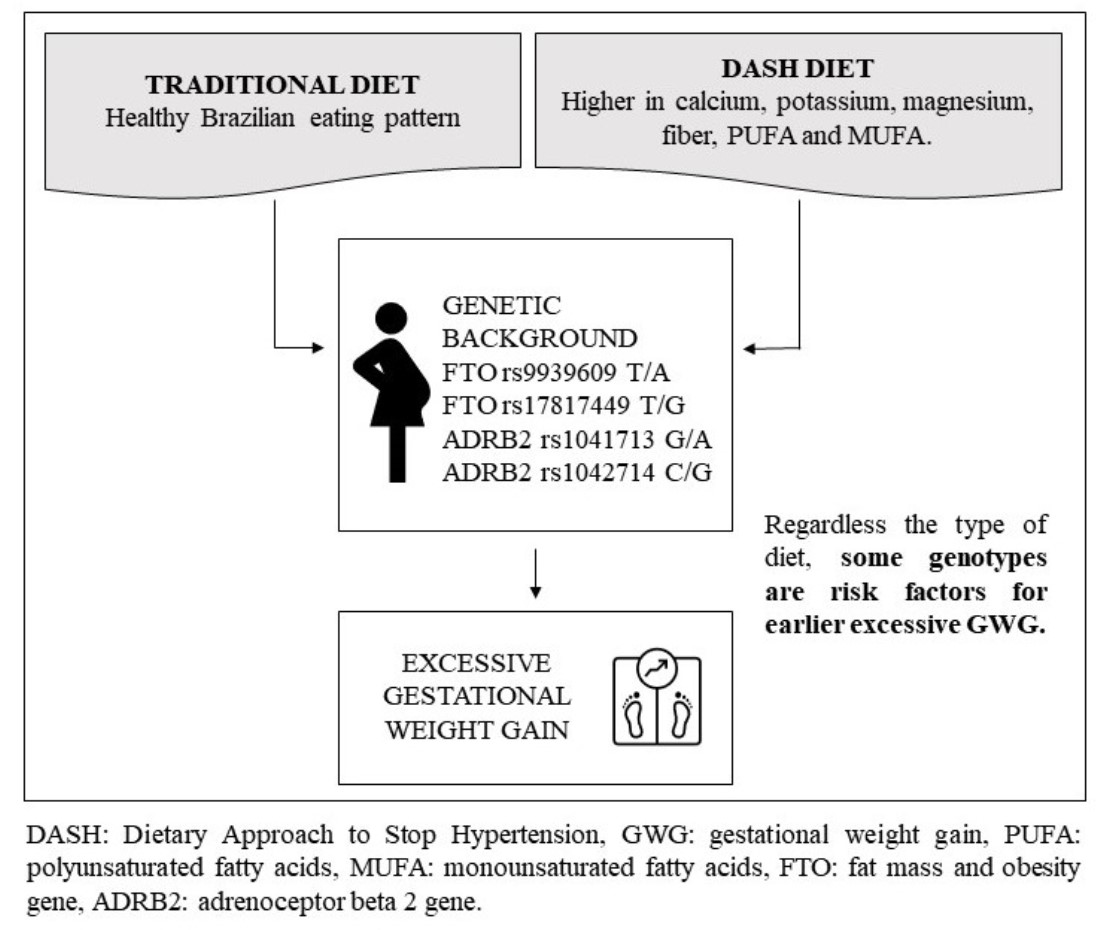
FTO and ADRB2 Genetic Polymorphisms Are Risk Factors for Earlier Excessive Gestational Weight Gain in Pregnant Women with Pregestational Diabetes Mellitus: Results of a Randomized Nutrigenetic Trial

 ,
, 

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Pregestational Diabetes Diagnosis and Treatment
2.3. Diet Groups and Nutritional Guidance
2.4. Outcome
2.5. Genotyping
2.6. Co-Variates
2.7. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis. J. Am. Med. Assoc. 2017, 317, 2207–2225. [Google Scholar] [CrossRef]
- Brandão, T.; de Carvalho Padilha, P.; de Barros, D.C.; Dos Santos, K.; Nogueira da Gama, S.G.; Leal, M.D.C.; da Silva Araújo, R.G.P.; Esteves Pereira, A.P.; Saunders, C. Gestational weight gain adequacy for favourable obstetric and neonatal outcomes: A nationwide hospital-based cohort gestational weight gain for favourable obstetric and neonatal outcomes. Clin. Nutr. ESPEN 2021, 45, 374–380. [Google Scholar] [CrossRef]
- Egan, A.M.; Dennedy, M.C.; Al-Ramli, W.; Heerey, A.; Avalos, G.; Dunne, F. ATLANTIC-DIP: Excessive gestational weight gain and pregnancy outcomes in women with gestational or pregestational diabetes mellitus. J. Clin. Endocrinol. Metab. 2014, 99, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Gualdani, E.; Di Cianni, G.; Seghieri, M.; Francesconi, P.; Seghieri, G. Pregnancy outcomes and maternal characteristics in women with pregestational and gestational diabetes: A retrospective study on 206,917 singleton live births. Acta Diabetol. 2021, 58, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- McDowell, M.; Cain, M.A.; Brumley, J. Excessive Gestational Weight Gain. J. Midwifery Women’s Heal. 2018, 64, 46–54. [Google Scholar] [CrossRef]
- Institute of Medicine. Weight Gain during Pregnancy: Reexamining the Guidelines; The National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Institute of Medicine. Implementing Guidelines on Weight Gain and Pregnancy; The National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- Warrington, N.M.; Richmond, R.; Fenstra, B.; Myhre, R.; Gaillard, R.; Paternoster, L.; Wang, C.A.; Beaumont, R.N.; Das, S.; Murcia, M.; et al. Maternal and fetal genetic contribution to gestational weight gain. Int. J. Obes. 2018, 42, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, A.; Magnano San Lio, R.; La Rosa, M.C.; Giunta, G.; Panella, M.; Cianci, A.; Caruso, M.A.T.; Agodi, A.; Barchitta, M. The Relationship between Telomere Length and Gestational Weight Gain: Findings from the Mamma & Bambino Cohort. Biomedicines 2021, 10, 67. [Google Scholar] [CrossRef]
- Loos, R.J.; Yeo, G.S. The bigger picture of FTO: The first GWAS-identified obesity gene. Nat. Rev. Endocrinol. 2014, 10, 51–61. [Google Scholar] [CrossRef]
- Fonseca, A.C.P.D.; Marchesini, B.; Zembrzuski, V.M.; Voigt, D.D.; Ramos, V.G.; Carneiro, J.R.I.; Nogueira Neto, J.F.; Cabello, G.M.K.; Cabello, P.H. Genetic variants in the fat mass and obesity-associated (FTO) gene confer risk for extreme obesity and modulate adiposity in a Brazilian population. Genet Mol. Biol. 2020, 43, e20180264. [Google Scholar] [CrossRef]
- Groth, S.W.; LaLonde, A.; Wu, T.; Fernandez, I.D. Obesity candidate genes, gestational weight gain, and body weight changes in pregnant women. Nutrition 2018, 48, 61–66. [Google Scholar] [CrossRef]
- Groth, S.W.; Morrison-Beedy, D. GNB3 and FTO Polymorphisms and Pregnancy Weight Gain in Black Women. Biol. Res. Nurs. 2014, 17, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Gesteiro, E.; Sánchez-Muniz, F.J.; Ortega-Azorín, C.; Guillén, M.; Corella, D.; Bastida, S. Maternal and neonatal FTO rs9939609 polymorphism affect insulin sensitivity markers and lipoprotein profile at birth in appropriate-for-gestational-age term neonates. J. Physiol. Biochem. 2016, 72, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.C.; Trujillo, J.; Farias, D.R.; Struchiner, C.J.; Kac, G. Association of the FTO (rs9939609) and MC4R (rs17782313) gene polymorphisms with maternal body weight during pregnancy. Nutrition 2016, 32, 1223–1230. [Google Scholar] [CrossRef]
- Al-Ogaidi, S.O.; Abdulsattar, S.; Al-dulaimi, M. FTO rs17817449 Gene Polymorphism as a Predictor for Maternal Obesity in Iraqi Pregnant Women. Indian J. Public Heal. Res. Dev. 2019, 10, 678–683. [Google Scholar] [CrossRef]
- Steemburgo, T.; Azevedo, M.J.; Martínez, J.A. Interação entre gene e nutriente e sua associação à obesidade e ao diabetes melito [Gene-nutrient interaction and its association with obesity and diabetes mellitus]. Arq. Bras. de Endocrinol. Metabol. 2009, 53, 497–508. (In Portuguese) [Google Scholar] [CrossRef]
- Zhang, H.; Wu, J.; Yu, L. Association of Gln27Glu and Arg16Gly polymorphisms in Beta2-adrenergic receptor gene with obesity susceptibility: A meta-analysis. PLoS ONE 2014, 9, e100489. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Favara, G.; La Rosa, M.C.; La Mastra, C.; Magnano San Lio, R.; Agodi, A. Maternal Dietary Patterns Are Associated with Pre-Pregnancy Body Mass Index and Gestational Weight Gain: Results from the “Mamma & Bambino”. Cohort. Nutr. 2019, 11, 1308. [Google Scholar] [CrossRef]
- American Diabetes Association. 14. Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes—2021. Diabetes Care 2020, 44, S200–S210. [Google Scholar] [CrossRef]
- Svetkey, L.P.; Sacks, F.M.; Obarzanek, E.; Vollmer, W.M.; Appel, L.J.; Lin, P.H.; Karanja, N.M.; Harsha, D.W.; Bray, G.A.; Aickin, M.; et al. The DASH Diet, Sodium Intake and Blood Pressure Trial (DASH-sodium): Rationale and design. DASH-Sodium Collaborative Research Group. J. Am. Diet. Assoc. 1999, 99, S96–S104. [Google Scholar] [CrossRef]
- Asemi, Z.; Tabassi, Z.; Samimi, M.; Fahiminejad, T.; Esmaillzadeh, A. Favourable effects of the Dietary Approaches to Stop Hypertension diet on glucose tolerance and lipid profiles in gestational diabetes: A randomised clinical trial. Br. J. Nutr. 2012, 109, 2024–2030. [Google Scholar] [CrossRef]
- Li, S.; Gan, Y.; Chen, M.; Wang, M.; Wang, X.; Santos, H.O.; Okunade, K.; Kathirgamathamby, V. Effects of the Dietary Approaches to Stop Hypertension (DASH) on Pregnancy/Neonatal Outcomes and Maternal Glycemic Control: A Systematic Review and Meta-analysis of Randomized Clinical Trials. Complement. Ther. Med. 2020, 54, 102551. [Google Scholar] [CrossRef]
- Hosseini-Esfahani, F.; Koochakpoor, G.; Daneshpour, M.S.; Sedaghati-Khayat, B.; Mirmiran, P.; Azizi, F. Mediterranean Dietary Pattern Adherence Modify the Association between FTO Genetic Variations and Obesity Phenotypes. Nutrients 2017, 9, 1064. [Google Scholar] [CrossRef]
- Hosseini-Esfahani, F.; Koochakpoor, G.; Mirmiran, P.; Daneshpour, M.S.; Azizi, F. Dietary patterns modify the association between fat mass and obesity-associated genetic variants and changes in obesity phenotypes. Br. J. Nutr. 2019, 121, 1247–1254. [Google Scholar] [CrossRef]
- Martínez, J.A.; Corbalán, M.S.; Sánchez-Villegas, A.; Forga, L.; Marti, A.; Martínez-González, M.A. Obesity risk is associated with carbohydrate intake in women carrying the Gln27Glu beta2-adrenoceptor polymorphism. J. Nutr. 2003, 133, 2549–2554. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, L.R.; De Caterina, R.; Görman, U.; Allayee, H.; Kohlmeier, M.; Prasad, C.; Choi, M.S.; Curi, R.; de Luis, D.A.; Gil, Á.; et al. Guide and Position of the International Society of Nutrigenetics/Nutrigenomics on Personalised Nutrition: Part 1-Fields of Precision Nutrition. J. Nutr. Nutr. 2016, 9, 12–27. [Google Scholar] [CrossRef]
- Saunders, C.; Moreira, T.M.; Belfort, G.P.; da Silva, C.F.M.; dos Santos, K.; da Silva, L.B.G.; Scancetti, L.B.; Fagherazzi, S.; Pereira, A.F.; Rosado, E.L.; et al. Procedimentos metodológicos para elaboração de plano alimentar adaptado baseado na dieta DASH para gestantes com diabetes mellitus. BJD 2021, 7, 116769–116788. [Google Scholar] [CrossRef]
- Della Líbera, B.; Ribeiro Baião, M.; de Souza Santos, M.M.; Padilha, P.; Dutra Alves, P.; Saunders, C. Adherence of pregnant women to dietary counseling and adequacy of total gestational weight gain. Nutr. Hosp. 2011, 26, 79–85. [Google Scholar]
- Carrilho, T.R.B.; Rasmussen, K.; Farias, D.R.; Freitas Costa, N.C.; Araújo Batalha, M.; Reichenheim, M.E.; Ohuma, E.O.; Hutcheon, J.A.; Kac, G.; Brazilian Maternal and Child Nutrition Consortium. Agreement between self-reported pre-pregnancy weight and measured first-trimester weight in Brazilian women. BMC Pregnancy Childbirth 2020, 20, 734. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Physical Status: The Use and Interpretation of Anthropometry; Report of a WHO Expert Committee; WHO: Geneva, Switzerland, 1995; Volume 452, pp. 1–542. [Google Scholar]
- Aidar, M.; Line, S.R.P. A simple and cost-effective protocol for DNA isolation from buccal epithelial cells. Braz. Dent. J. 2007, 18, 148–152. [Google Scholar] [CrossRef]
- Matsudo, S.; Araújo, T.; Matsudo, V.; Andrade, D.; Andrade, E.; Oliveira, L.C.; Braggion, G. Questionário Internacional de Atividade Física (IPAQ): Estudo de validade e reprodutibilidade no Brasil. RBAFS 2001, 6, 5–18. [Google Scholar]
- Núcleo de Estudos e Pesquisas em Alimentação (NEPA). Tabela Brasileira de Composição de Alimentos (TACO/NEPA-Unicamp). Available online: http://www.nepa.unicamp.br/taco/tabela.php?ativo=tabela (accessed on 25 February 2022).
- United States Department of Agriculture. USDA National Nutrient Database for Standard Reference. Available online: https://fdc.nal.usda.gov/ (accessed on 25 February 2022).
- Biddanda, A.; Rice, D.P.; Novembre, J. A variant-centric perspective on geographic patterns of human allele frequency variation. Elife 2020, 9, e60107. [Google Scholar] [CrossRef] [PubMed]
- Scliar, M.O.; Sant’Anna, H.P.; Santolalla, M.L.; Leal, T.P.; Araújo, N.M.; Alvim, I.; Borda, V.; Magalhães, W.C.S.; Gouveia, M.H.; Lyra, R.; et al. Admixture/fine-mapping in Brazilians reveals a West African associated potential regulatory variant (rs114066381) with a strong female-specific effect on body mass and fat mass indexes. Int. J. Obes. 2021, 45, 1017–1029. [Google Scholar] [CrossRef] [PubMed]
- Kroll, C.; Farias, D.R.; Carrilho, T.R.B.; Kac, G.; Mastroeni, M.F. Association of ADIPOQ-rs2241766 and FTO-rs9939609 genetic variants with body mass index trajectory in women of reproductive age over 6 years of follow-up: The PREDI study. Eur. J. Clin. Nutr. 2021, 76, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Kroll, C.; de França, P.H.C.; Mastroeni, M.F. Association between FTO gene polymorphism and excess body weight in women from before to after pregnancy: A cohort study. Am. J. Hum. Biol. 2018, 30, e23164. [Google Scholar] [CrossRef]
- Beysel, S.; Eyerci, N.; Ulubay, M.; Caliskan, M.; Kizilgul, M.; Hafızoğlu, M.; Cakal, E. Maternal genetic contribution to pre-pregnancy obesity, gestational weight gain, and gestational diabetes mellitus. Diabetol. Metab. Syndr. 2019, 11, 37. [Google Scholar] [CrossRef] [PubMed]
- Saucedo, R.; Valencia, J.; Gutierrez, C.; Basurto, L.; Hernandez, M.; Puello, E.; Rico, G.; Vega, G.; Zarate, A. Gene variants in the FTO gene are associated with adiponectin and TNF-alpha levels in gestational diabetes mellitus. Diabetol. Metab. Syndr. 2017, 9, 32. [Google Scholar] [CrossRef]
- Van Horn, L.; Peaceman, A.; Kwasny, M.; Vincent, E.; Fought, A.; Josefson, J.; Spring, B.; Neff, L.M.; Gernhofer, N. Dietary Approaches to Stop Hypertension Diet and Activity to Limit Gestational Weight: Maternal Offspring Metabolics Family Intervention Trial, a Technology Enhanced Randomized Trial. Am. J. Prev. Med. 2018, 55, 603–614. [Google Scholar] [CrossRef]
- Fulay, A.P.; Rifas-Shiman, S.L.; Oken, E.; Perng, W. Associations of the dietary approaches to stop hypertension (DASH) diet with pregnancy complications in Project Viva. Eur. J. Clin. Nutr. 2018, 72, 1385–1395. [Google Scholar] [CrossRef]
- Camp, K.M.; Trujillo, E. Position of the Academy of Nutrition and Dietetics: Nutritional genomics. J. Acad. Nutr. Diet. 2014, 114, 299–312. [Google Scholar] [CrossRef]
- Martins, M.C.; Trujillo, J.; Freitas-Vilela, A.A.; Farias, D.R.; Rosado, E.L.; Struchiner, C.J.; Kac, G. Associations between obesity candidate gene polymorphisms (fat mass and obesity-associated (FTO), melanocortin-4 receptor (MC4R), leptin (LEP) and leptin receptor (LEPR)) and dietary intake in pregnant women. Br. J. Nutr. 2018, 120, 454–463. [Google Scholar] [CrossRef]
- Siegel, A.M.; Tita, A.; Biggio, J.R.; Harper, L.M. Evaluating gestational weight gain recommendations in pregestational diabetes. Am. J. Obstet. Gynecol. 2015, 213, 563.e1–563.e5. [Google Scholar] [CrossRef] [PubMed]
- Alessi, J.; Wiegand, D.M.; Hirakata, V.N.; Oppermann, M.L.R.; Reichelt, A.J. Temporal changes in characteristics and outcomes among pregnant women with pre-gestational diabetes. Int. J. Gynecol. Obstet. 2018, 143, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Denize, K.M.; Acharya, N.; Prince, S.A.; da Silva, D.F.; Harvey, A.L.J.; Ferraro, Z.M.; Adamo, K.B. Addressing cultural, racial and ethnic discrepancies in guideline discordant gestational weight gain: A systematic review and meta-analysis. PeerJ 2018, 6, e5407. [Google Scholar] [CrossRef] [PubMed]
- Collares, F.M.; Korevaar, T.I.M.; Hofman, A.; Steegers, E.A.P.; Peeters, R.P.; Jaddoe, V.W.V.; Gaillard, R. Maternal thyroid function, prepregnancy obesity and gestational weight gain-The Generation R Study: A prospective cohort study. Clin. Endocrinol. 2017, 87, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Alexander, E.K.; Pearce, E.N.; Brent, G.A.; Brown, R.S.; Chen, H.; Dosiou, C.; Grobman, W.A.; Laurberg, P.; Lazarus, J.H.; Mandel, S.J.; et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid 2017, 27, 315–389. [Google Scholar] [CrossRef]
- Cheney, K.; Berkemeier, S.; Sim, K.A.; Gordon, A.; Black, K. Prevalence and predictors of early gestational weight gain associated with obesity risk in a diverse Australian antenatal population: A cross-sectional study. BMC Pregnancy Childbirth 2017, 17, 296. [Google Scholar] [CrossRef] [PubMed]
- Herring, S.J.; Oken, E.; Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Stuebe, A.M.; Kleinman, K.P.; Gillman, M.W. Weight gain in pregnancy and risk of maternal hyperglycemia. Am. J. Obstet. Gynecol. 2009, 201, 61.e1–61.e7. [Google Scholar] [CrossRef]
- Mamun, A.A.; Mannan, M.; Doi, S.A. Gestational weight gain in relation to offspring obesity over the life course: A systematic review and bias-adjusted meta-analysis. Obes. Rev. 2013, 15, 338–347. [Google Scholar] [CrossRef]
- Hivert, M.F.; Rifas-Shiman, S.L.; Gillman, M.W.; Oken, E. Greater early and mid-pregnancy gestational weight gains are associated with excess adiposity in mid-childhood. Obesity 2016, 24, 1546–1553. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Traditional Diet | DASH Diet | |
|---|---|---|
| Saturated fatty acids * | 9.7% E | 7.2% E |
| Monounsaturated fatty acids * | 8.5% E | 9.2% E |
| Polyunsaturated fatty acids * | 2.8% E | 5.6% E |
| Fiber | 42 g | 55 g |
| Calcium | 1500 mg | 2280 mg |
| Magnesium | 315 mg | 496 mg |
| Potassium | 4081 mg | 4418 mg |
| Sodium | 2400 mg | 2400 mg |
| Overall n = 70 | Trad. Diet n = 41 | DASH Diet n = 29 | p-Value * | |
|---|---|---|---|---|
| Age (years) | 32 (25.7–36.0) | 31 (25.0–35.0) | 34 (28.0–37.0) | 0.28 |
| Gestational age (weeks) | 15.0 (11.1–20.1) | 14.4 (11.6–21.6) | 16.0 (10.1–18.6) | 0.66 |
| DM type n (%) | ||||
| DM1 | 36 (51.4) | 21 (51.2) | 15 (51.7) | 0.97 |
| DM2 | 34 (48.6) | 20 (48.8) | 14 (48.3) | |
| Years living with DM | 8 (2.0–13.5) | 6 (1.9–12.5) | 9 (2.0–14.5) | 0.36 |
| Skin color n (%) | ||||
| Brown | 27 (38.6) | 15 (36.6) | 12 (41.4) | 0.59 |
| White | 22 (31.4) | 12 (29.3) | 10 (34.5) | |
| Black | 16 (22.9) | 11 (26.8) | 5 (17.2) | |
| Yellow | 1 (1.4) | 0 (0) | 1 (3.4) | |
| Unknown | 4 (5.7) | 3 (7.3) | 1 (3.4) | |
| Marital status n (%) | ||||
| Married | 56 (80.0) | 33 (80.5) | 23 (79.3) | 0.57 |
| Single | 12 (17.1) | 6 (14.6) | 6 (20.7) | |
| Missing | 2 (2.9) | 2 (4.9) | 0 (0) | |
| Education level n (%) | ||||
| Elementary/middle school | 46 (65.7) | 26 (63.4) | 20 (69.0) | 0.73 |
| High school | 23 (32.9) | 14 (34.2) | 9 (31.0) | |
| Missing | 1 (1.4) | 1 (2.4) | 0 (0) | |
| Employment n (%) | ||||
| Yes | 42 (60.0) | 26 (63.4) | 16 (55.2) | 0.41 |
| No | 27 (38.6) | 14 (34.1) | 13 (44.8) | |
| Missing | 1 (1.4) | 1 (2.4) | 0 (0) | |
| per capita income (USD †) | 151.51 (103.04–227.27) | 154.54 (113.33–228.78) | 136.36 (91.67–221.04) | 0.59 |
| Housing conditions | ||||
| Adequate | 64 (91.4) | 37 (90.2) | 27 (93.1) | 1.00 |
| Inadequate | 3 (4.3) | 2 (4.9) | 1 (3.5) | |
| Missing | 3 (4.3) | 2 (4.9) | 1 (3.5) | |
| Parity n (%) | 1 (0–1.25) | 1 (0–1.5) | 1 (0–1.5) | 0.92 |
| Preexisting chronic disease n (%) | ||||
| None | 48 (68.4) | 31 (75.6) | 17 (58.6) | 0.06 |
| Hypertension | 9 (12.9) | 4 (9.8) | 5 (17.2) | |
| Hypothyroidism | 8 (11.4) | 2 (4.9) | 6 (20.7) | |
| Both | 1 (1.4) | 0 (0) | 1 (3.4) | |
| Missing | 4 (5.7) | 4 (9.8) | 0 (0) | |
| Pre-pregnancy BMI (kg/m2) | 27.85 (24.4–32.3) | 27.10 (24.3–31.9) | 28.60 (25.7–33.3) | 0.16 |
| Pre-pregnany BMI n (%) | ||||
| Normal weight | 20 (28.6) | 14 (34.1) | 6 (20.7) | 0.45 |
| Overweight | 25 (35.7) | 14 (34.1) | 11 (37.9) | |
| Obesity | 25 (35.7) | 13 (31.7) | 12 (41.4) | |
| Energy intake (kcal) | 1808.3 (1578.7–2228.6) | 1823.8 (1528.9–2362.2) | 1780.7 (1644.5–1968.8) | 0.68 |
| Physical Activity n (%) | ||||
| Active | 30 (42.9) | 15 (36.6) | 15 (51.7) | 0.51 |
| Irregularly active | 27 (38.6) | 17 (41.5) | 10 (34.5) | |
| Sedentary | 7 (10.0) | 5 (12.1) | 2 (6.9) | |
| Missing | 6 (8.6) | 4 (9.8) | 2 (6.9) | |
| Overall n = 70 | Traditional Diet n = 41 | DASH Diet n = 29 | p-Value * | |
|---|---|---|---|---|
| FTO rs9939609 n (%) | ||||
| T Allele | 90 (64.3) | |||
| A Allele | 50 (35.7) | |||
| TT | 28 (40.0) | 17 (41.5) | 11 (37.9) | 0.48 |
| AT | 34 (48.6) | 21 (51.2) | 13 (44.8) | |
| AA | 8 (11.4) | 3 (7.3) | 5 (17.2) | |
| FTO rs17817449 n (%) | ||||
| T Allele | 95 (67.9) | |||
| G Allele | 45 (32.1) | |||
| TT | 32 (45.7) | 19 (46.3) | 13 (44.8) | 0.73 |
| GT | 31 (44.3) | 19 (46.3) | 12 (41.4) | |
| GG | 7 (10.0) | 3 (7.3) | 4 (13.8) | |
| ADRB2 rs1042713 n (%) | ||||
| G Allele | 87 (62.1) | |||
| A Allele | 53 (37.9) | |||
| GG | 25 (35.7) | 12 (29.3) | 13 (44.8) | 0.35 |
| AG | 37 (52.9) | 23 (56.1) | 14 (48.3) | |
| AA | 8 (11.4) | 6 (14.6) | 2 (6.9) | |
| ADRB2 rs1042714 n (%) | ||||
| C Allele | 101 (72.1) | |||
| G Allele | 39 (27.9) | |||
| CC | 35 (50.0) | 20 (48.3) | 15 (51.7) | 0.28 |
| CG | 31 (44.3) | 17 (41.5) | 14 (48.3) | |
| GG | 4 (5.7) | 4 (9.8) | 0 (0) |
| Characteristics | Outcome | pY | Crude Incidence/ 100 pY (CI 95%) | HR (CI 95%) | p-Value | aHR * (CI 95%) | p-Value |
|---|---|---|---|---|---|---|---|
| Overall | 37 | 44.4 | 83.29 (58.65–114.81) | - | - | - | - |
| Diet | |||||||
| Traditional diet | 18 | 26.0 | 69.12 (40.97–109.25) | Reference | - | Reference | - |
| DASH diet | 19 | 18.4 | 103.36 (62.23–161.41) | 1.66 (0.87–3.17) | 0.12 | 1.32 (0.62–2.79) | 0.46 |
| Type of DM | |||||||
| DM1 | 17 | 23.2 | 73.36 (42.73–117.46) | Reference | - | Reference | - |
| DM2 | 20 | 21.2 | 94.12 (57.49–145.37) | 1.39 (0.728–2.657) | 0.32 | 0.92 (0.38–2.22) | 0.86 |
| Years living with DM (years) | |||||||
| <8 | 18 | 25.3 | 71.25 (42.23–112.61) | Reference | - | Reference | - |
| ≥8 | 19 | 18.4 | 103.10 (62.07–161.00) | 1.62 (0.85–3.09) | 0.14 | 1.99 (1.01–3.93) | 0.04 |
| Age (years) | |||||||
| <32 | 21 | 23.0 | 91.20 (56.46–139.41) | Reference | - | Reference | - |
| ≥32 | 16 | 21.4 | 74.78 (42.74–121.44 | 0.80 (0.41–1.53) | 0.49 | 0.41 (0.21–0.80) | 0.01 |
| Color of the skin | |||||||
| Brown | 14 | 17.2 | 81.17 (44.37–136.18) | Reference | - | Reference | - |
| White | 10 | 14.0 | 71.30 (34.19–131.11) | 0.838 (0.372–1.888) | 0.67 | 0.681 (0.293–1.586) | 0.37 |
| Black | 10 | 10.2 | 98.29 (47.13–180.76) | 1.404 (0.622–3.171) | 0.41 | 1.132 (0.458–2.8) | 0.79 |
| Marital Status | |||||||
| Married | 30 | 36.9 | 81.30 (54.86–116.07) | Reference | - | Reference | - |
| Single | 7 | 6.8 | 102.84 (41.35–211.90) | 1.44 (0.63–3.29) | 0.38 | 1.92 (0.79–4.68) | 0.15 |
| Employment | |||||||
| Yes | 20 | 26.9 | 74.18 (45.31–114.56) | Reference | - | Reference | - |
| No | 17 | 16.7 | 101.54 (59.15–162.58) | 1.40 (0.74–2.68) | 0.30 | 1.45 (0.76–2.79) | 0.26 |
| Housing Conditions | |||||||
| Adequate | 35 | 41.1 | 85.10 (59.27–118.35) | Reference | - | Reference | - |
| Inadequate | 2 | 1.1 | 183.54 (22.23–663.01) | 4.49 (1.04–19.43) | 0.04 | 4.25 (0.84–21.59) | 0.08 |
| Pre-pregnancy BMI | |||||||
| Normal weight | 6 | 13.5 | 44.43 (16.31–96.71) | Reference | - | Reference | - |
| Overweight | 16 | 15.6 | 102.54 (58.61–166.52) | 3.15 (1.23–8.09) | 0.02 | 3.15 (1.23–8.09) | 0.02 |
| Obesity | 15 | 15.3 | 97.94 (54.82–161.53) | 2.87 (1.11–7.42) | 0.03 | 2.87 (1.11–7.42) | 0.03 |
| Chronic disease | |||||||
| None | 24 | 31.1 | 70.74 (44.33–107.10) | Reference | - | Reference | - |
| Chronic hypertension | 5 | 5.6 | 89.26 (28.98–208.30) | 1.53 (0.58–4.04) | 0.39 | 1.33 (0.48–3.70) | 0.59 |
| Hypothyroidism | 7 | 4.9 | 141.02 (56.70–290.56) | 2.66 (1.13–6.30) | 0.02 | 4.37 (1.62–11.77) | 0.00 |
| Both | 1 | 0.7 | 141.02 (3.57–785.72) | 1.64 (0.22–12.19) | 0.63 | 1.21 (0.15–9.98) | 0.86 |
| Genotypes | Outcome | pY | Crude Incidence/100 pY (CI 95%) | HR (CI 95%) | p | aHR * (CI 95%) | p | |
|---|---|---|---|---|---|---|---|---|
| Overall | 37 | 44.4 | 83.29 (58.65–114.31) | - | - | - | - | |
| rs9939609 | ||||||||
| Additive Model | TT | 12 | 18.6 | 64.33 (33.24–112.38) | Reference | - | Reference | - |
| AT | 19 | 20.6 | 92.06 (55.43–143.77) | 1.56 (0.76–3.21) | 0.23 | 2.44 (1.03–5.78) | 0.04 | |
| AA | 6 | 5.1 | 116.94 (42.92–254.53) | 2.08 (0.78–5.55) | 0.14 | 2.83 (0.93–8.62); | 0.07 | |
| Dominant Model | TT | 12 | 18.6 | 64.33 (33.24–112.38) | Reference | - | Reference | - |
| AT/AA | 25 | 25.8 | 97.02 (62.78–143.21) | 1.66 (0.83–3.30); | 0.15 | 2.55 (1.14–5.69) | 0.02 | |
| Recessive Model | AA | 6 | 5.1 | 116.94 (42.92–254.53) | Reference | - | Reference | - |
| AT/TT | 31 | 39.3 | 78.9 (53.61–111.99) | 0.62 (0.26–1.48) | 0.28 | 0.54 (0.20–1.49) | 0.24 | |
| rs17817449 | ||||||||
| Additive Model | TT | 15 | 21.0 | 71.42 (39.97–117.80) | Reference | - | Reference | - |
| GT | 17 | 18.8 | 90.55 (52.75–144.98) | 1.30 (0.65–2.61) | 0.46 | 1.66 (0.75–3.65) | 0.21 | |
| GG | 5 | 4.6 | 107.62 (34.94–251.14) | 1.54 (0.56–4.25) | 0.40 | 2.18 (0.65–7.33) | 0.21 | |
| Dominant Model | TT | 15 | 21.0 | 71.42 (39.97–117.8) | Reference | - | Reference | - |
| GT/GG | 22 | 23.4 | 93.94 (58.87–142.22) | 1.35 (0.70–2.60) | 0.37 | 1.74 (0.82–3.70) | 0.15 | |
| Recessive Model | GG | 5 | 4.6 | 107.62 (34.94–251.14) | Reference | - | Reference | - |
| GT/TT | 32 | 39.8 | 80.45 (55.03–113.57) | 0.74 (0.29–1.90) | 0.53 | 0.60 (0.20–1.83) | 0.37 | |
| Genotypes | Outcome | pY | Crude Incidence/100 pY (CI 95%) | HR (CI 95%) | p | aHR * (CI 95%) | p | |
|---|---|---|---|---|---|---|---|---|
| Overall | 37 | 44.4 | 83.29 (58.65–114.31) | - | - | - | - | |
| rs1042713 | ||||||||
| Additive Model | GG | 10 | 16.3 | 61.44 (29.46–112.99) | Reference | - | Reference | - |
| AG | 22 | 23.6 | 93.36 (58.51–141.35) | 1.72 (0.81–3.64) | 0.16 | 2.14 (0.89–5.14) | 0.09 | |
| AA | 5 | 4.6 | 109.16 (35.44–254.74) | 2.05 (0.70–6.02) | 0.19 | 3.91 (1.12–13.70) | 0.03 | |
| Dominant Model | GG | 10 | 61.44 (29.46–112.99) | Reference | - | Reference | - | |
| AG/AA | 27 | 95.93 (63.22–139.57) | 1.772 (0.856–3.667) | 0.12 | 2.37 (1.01–5.52) | 0.04 | ||
| Recessive Model | AA | 5 | 4.6 | 109.16 (35.44–254.74) | Reference | - | Reference | - |
| AG/GG | 32 | 39.8 | 80.32 (54.94–113.38) | 0.69 (0.27–1.77) | 0.44 | 0.41 (0.14–1.21) | 0.11 | |
| rs1042714 | ||||||||
| Additive Model | CC | 20 | 21.2 | 94.11 (57.49–145.35) | Reference | - | Reference | - |
| CG | 15 | 20.4 | 73.41 (41.09–121.08) | 0.71 (0.36–1.39) | 0.32 | 0.78 (0.37–1.63) | 0.51 | |
| GG | 2 | 2.7 | 73.05 (8.85–263.88) | 0.65 (0.15–2.80) | 0.57 | 0.29 (0.04–1.91) | 0.20 | |
| Dominant Model | CC | 20 | 21.2 | 94.11 (57.49–145.35) | Reference | - | Reference | - |
| CG/GG | 17 | 23.2 | 73.37 (42.74–117.47) | 0.70 (0.37–1.34) | 0.29 | 0.70 (0.34–1.44) | 0.33 | |
| Recessive Model | GG | 2 | 2.7 | 73.05 (8.85–263.88) | Reference | - | Reference | - |
| CG/CC | 35 | 41.7 | 83.96 (58.48–116.77) | 1.30 (0.31–5.40) | 0.72 | 3.20 (0.48–21.53) | 0.23 | |
| Haplotypes | Outcome | pY | Crude Incidence/ 100 pY (CI 95%) | HR (CI 95%) | p-Value | aHR * (CI 95%) | p-Value |
|---|---|---|---|---|---|---|---|
| ADRB2 rs1042713:rs1042714 | |||||||
| AC | 32 | 32.7 | 97.78 (66.88–138.04) | Reference | - | Reference | - |
| GC | 23 | 30.2 | 76.13 (48.26–114.24) | 0.74 (0.43–1.26) | 0.26 | 0.63 (0.36–1.12) | 0.12 |
| GG | 19 | 25.9 | 73.33 (44.15–114.52) | 0.67 (0.38–1.19) | 0.17 | 0.59 (0.32–1.09) | 0.09 |
| FTO rs9939609:rs17817449 | |||||||
| TT | 43 | 57.2 | 75.17 (54.40–101.26) | Reference | - | Reference | - |
| AG | 27 | 27.3 | 98.81 (65.12–143.77) | 1.37 (0.85–2.22) | 0.18 | 1.79 (1.04–3.06) | 0.02 |
| AT | 4 | 3.6 | 111.87 (30.48–286.42) | 2.03 (0.73–5.67) | 0.26 | 1.40 (0.46–4.28) | 0.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, K.d.; Rosado, E.L.; da Fonseca, A.C.P.; Belfort, G.P.; da Silva, L.B.G.; Ribeiro-Alves, M.; Zembrzuski, V.M.; Martínez, J.A.; Saunders, C. FTO and ADRB2 Genetic Polymorphisms Are Risk Factors for Earlier Excessive Gestational Weight Gain in Pregnant Women with Pregestational Diabetes Mellitus: Results of a Randomized Nutrigenetic Trial. Nutrients 2022, 14, 1050. https://doi.org/10.3390/nu14051050
Santos Kd, Rosado EL, da Fonseca ACP, Belfort GP, da Silva LBG, Ribeiro-Alves M, Zembrzuski VM, Martínez JA, Saunders C. FTO and ADRB2 Genetic Polymorphisms Are Risk Factors for Earlier Excessive Gestational Weight Gain in Pregnant Women with Pregestational Diabetes Mellitus: Results of a Randomized Nutrigenetic Trial. Nutrients. 2022; 14(5):1050. https://doi.org/10.3390/nu14051050
Chicago/Turabian StyleSantos, Karina dos, Eliane Lopes Rosado, Ana Carolina Proença da Fonseca, Gabriella Pinto Belfort, Letícia Barbosa Gabriel da Silva, Marcelo Ribeiro-Alves, Verônica Marques Zembrzuski, J. Alfredo Martínez, and Cláudia Saunders. 2022. "FTO and ADRB2 Genetic Polymorphisms Are Risk Factors for Earlier Excessive Gestational Weight Gain in Pregnant Women with Pregestational Diabetes Mellitus: Results of a Randomized Nutrigenetic Trial" Nutrients 14, no. 5: 1050. https://doi.org/10.3390/nu14051050
APA StyleSantos, K. d., Rosado, E. L., da Fonseca, A. C. P., Belfort, G. P., da Silva, L. B. G., Ribeiro-Alves, M., Zembrzuski, V. M., Martínez, J. A., & Saunders, C. (2022). FTO and ADRB2 Genetic Polymorphisms Are Risk Factors for Earlier Excessive Gestational Weight Gain in Pregnant Women with Pregestational Diabetes Mellitus: Results of a Randomized Nutrigenetic Trial. Nutrients, 14(5), 1050. https://doi.org/10.3390/nu14051050