
Pregnancy and COVID-19: The Possible Contribution of Vitamin D

 , , , ,
, , , ,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Enrolment
2.2. SARS-CoV-2 Detection Methods
2.2.1. Molecular Swabs
2.2.2. Detection of Antibodies against SARS-CoV-2
2.3. Genetic Polymorphism Analyses
2.4. 25-Hydroxyvitamin D Quantification
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
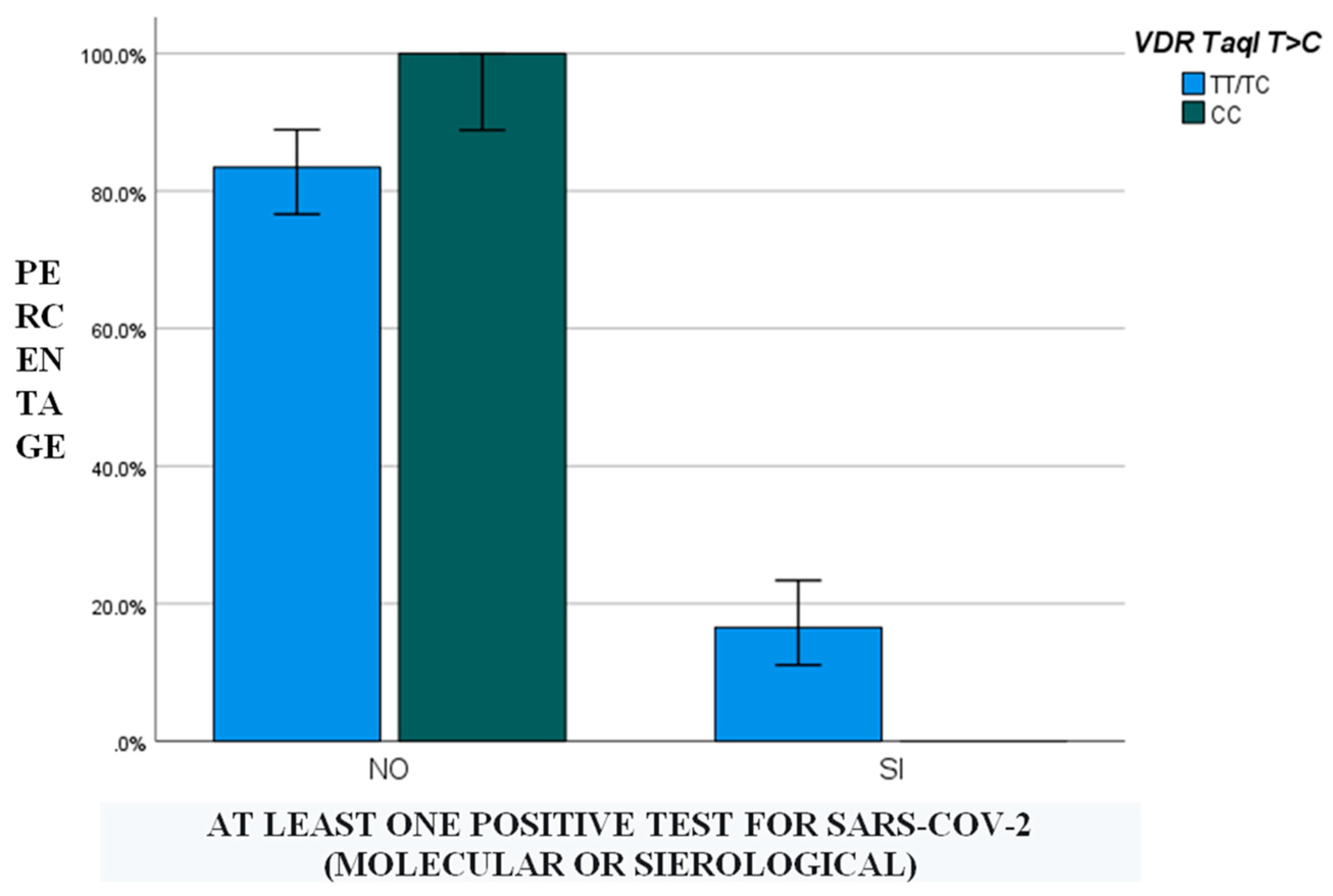
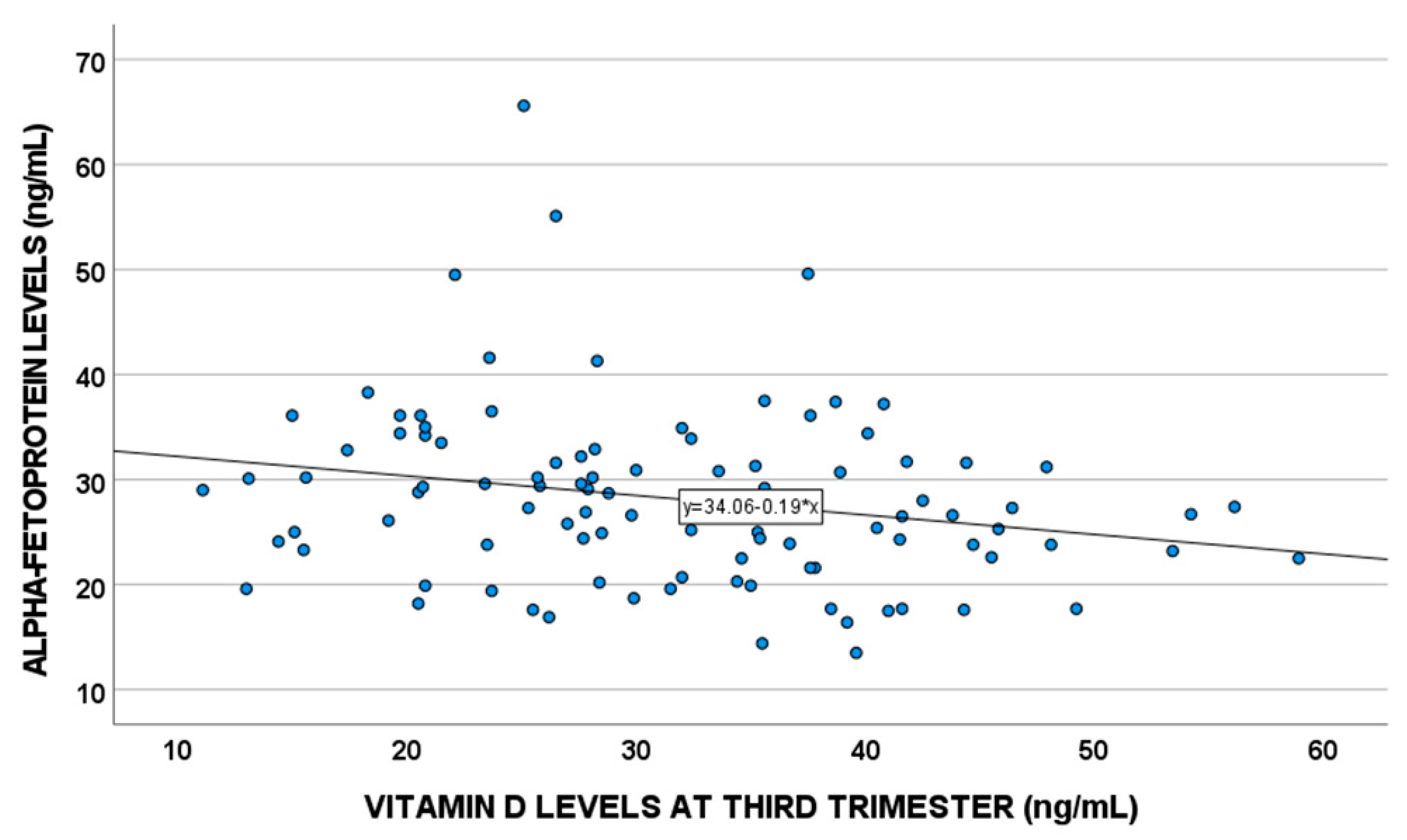
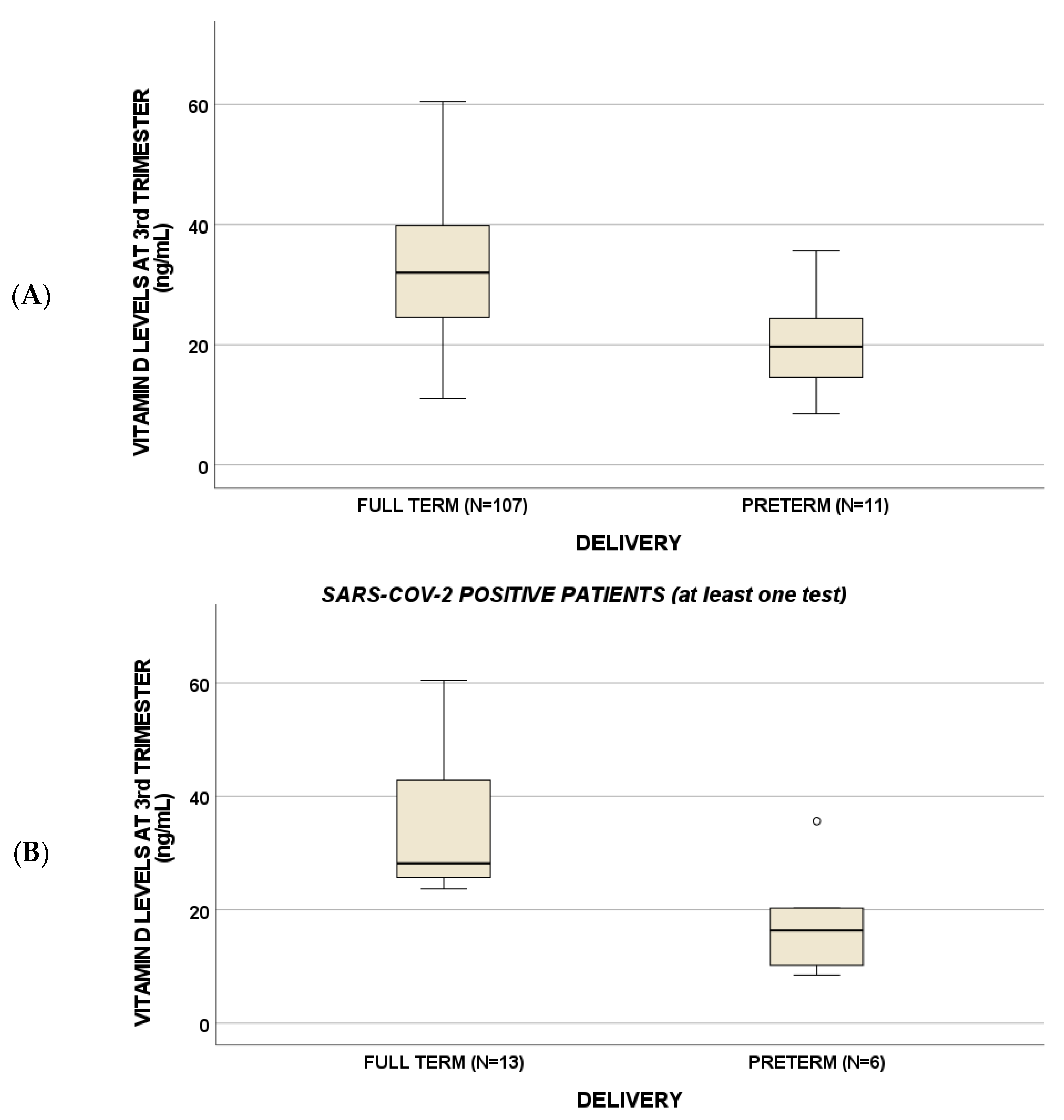
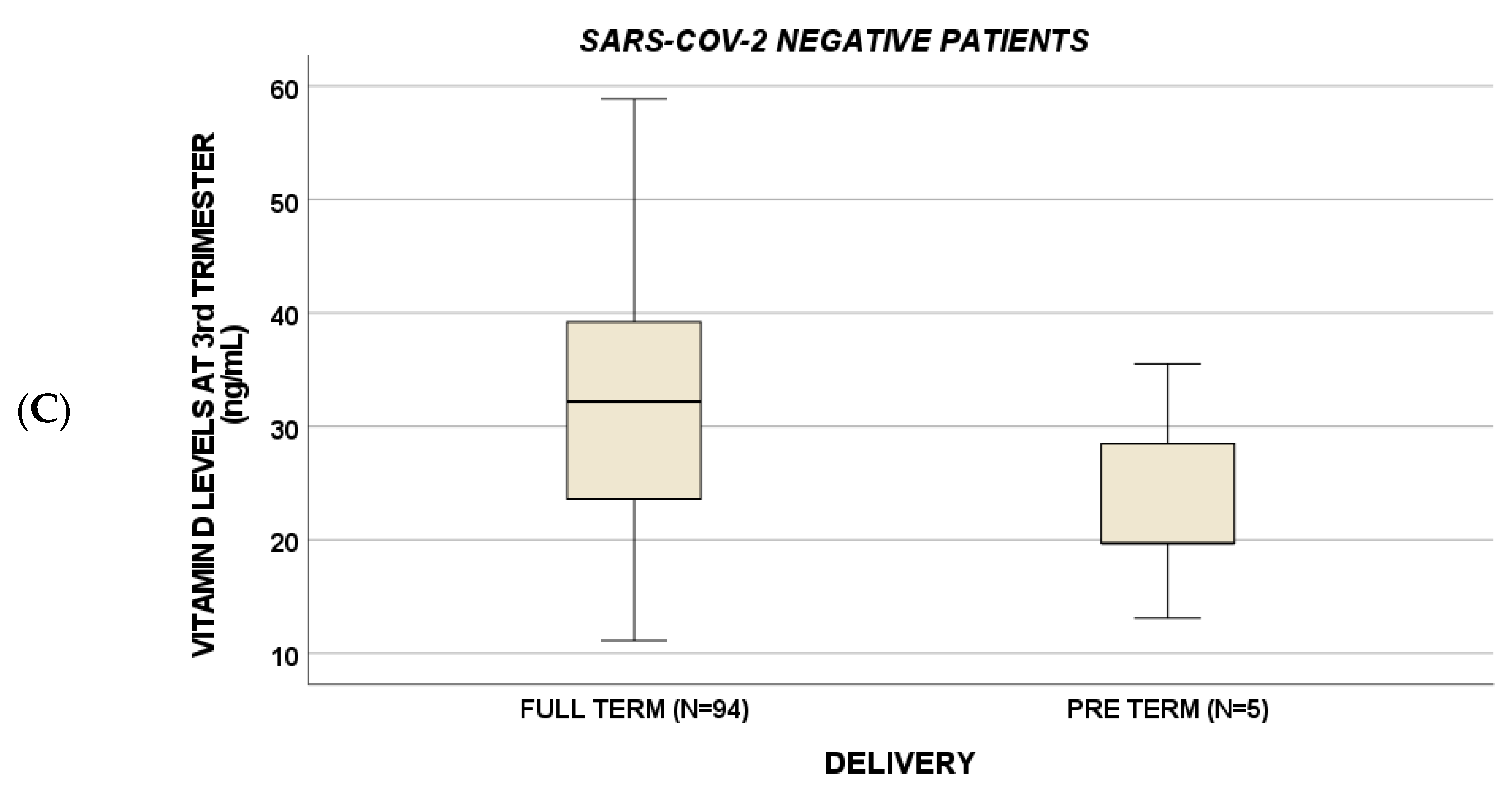
3.2. Vitamin D Polymorphisms, Vitamin D Levels and COVID-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, M.-Y.; Zhao, R.; Gao, L.-J.; Gao, X.-F.; Wang, D.-P.; Cao, J.-M. SARS-CoV-2: Structure, Biology, and Structure-Based Therapeutics Development. Front. Cell. Infect. Microbiol. 2020, 10, 587269. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.G.; Lin, T.; Wang, P. Mechanisms of SARS-CoV-2 Transmission and Pathogenesis. Trends Immunol. 2020, 41, 1100–1115. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Huang, S.; Yin, L. The cytokine storm and COVID-19. J. Med. Virol. 2020, 93, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Asakura, H.; Ogawa, H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int. J. Hematol. 2020, 113, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, T.; Majumder, R.; Majumder, S. Role of vitamin D in treating COVID-19-associated coagulopathy: Problems and perspectives. Mol. Cell. Biochem. 2021, 476, 2421–2427. [Google Scholar] [CrossRef] [PubMed]
- Dusso, A.S.; Brown, A.J.; Slatopolsky, E. Vitamin D. Am. J. Physiol. Ren. Physiol. 2005, 289, 8–28. [Google Scholar] [CrossRef]
- Mohan, M.; Cherian, J.J.; Sharma, A. Exploring links between vitamin D deficiency and COVID-19. PLoS Pathog. 2020, 16, e1008874. [Google Scholar] [CrossRef]
- Quesada-Gomez, J.M.; Entrenas-Castillo, M.; Bouillon, R. Vitamin D receptor stimulation to reduce acute respiratory distress syndrome (ARDS) in patients with coronavirus SARS-CoV-2 infections. J. Steroid Biochem. Mol. Biol. 2020, 202, 105719. [Google Scholar] [CrossRef]
- Bishop, E.L.; Ismailova, A.; Dimeloe, S.K.; Hewison, M.; White, J.H. Vitamin D and Immune Regulation: Antibacterial, Antiviral, Anti-Inflammatory. JBMR Plus 2020, 5, e10405. [Google Scholar] [CrossRef]
- Irani, M.; Merhi, Z. Role of vitamin D in ovarian physiology and its implication in reproduction: A systematic review. Fertil. Steril. 2014, 102, 460–468.e3. [Google Scholar] [CrossRef]
- Schmitt, G.; Labdouni, S.; Soulimani, R.; Delamare, C.; Bouayed, J. Oxidative stress status and vitamin D levels of asymptomatic to mild symptomatic COVID-19 infections during the third trimester of pregnancy: A retrospective study in Metz, France. J. Med. Virol. 2022, 94, 2167–2173. [Google Scholar] [CrossRef] [PubMed]
- Edlow, A.G.; Castro, V.M.; Shook, L.L.; Kaimal, A.J.; Perlis, R.H. Neurodevelopmental Outcomes at 1 Year in Infants of Mothers Who Tested Positive for SARS-CoV-2 During Pregnancy. JAMA Netw. Open 2022, 5, e2215787. [Google Scholar] [CrossRef]
- Garcia-Flores, V.; Romero, R.; Xu, Y.; Theis, K.R.; Arenas-Hernandez, M.; Miller, D.; Peyvandipour, A.; Bhatti, G.; Galaz, J.; Gershater, M.; et al. Maternal-fetal immune responses in pregnant women infected with SARS-CoV-2. Nat. Commun. 2022, 13, 320. [Google Scholar] [CrossRef] [PubMed]
- Okano, T. The role of the liver in vitamin D metabolism. Clin. Calcium 2015, 25, 1613–1618. [Google Scholar]
- Bertero, L.; Borella, F.; Botta, G.; Carosso, A.; Cosma, S.; Bovetti, M.; Carosso, M.; Abbona, G.; Collemi, G.; Papotti, M.; et al. Placenta histopathology in SARS-CoV-2 infection: Analysis of a consecutive series and comparison with control cohorts. Virchows Arch. 2021, 479, 715–728. [Google Scholar] [CrossRef] [PubMed]
- Mohr-Sasson, A.; Chayo, J.; Bart, Y.; Meyer, R.; Sivan, E.; Mazaki-Tovi, S.; Yinon, Y. Laboratory characteristics of pregnant compared to non-pregnant women infected with SARS-CoV-2. Arch. Gynecol. Obstet. 2020, 302, 629–634. [Google Scholar] [CrossRef]
- Sinaci, S.; Ocal, D.F.; Yetiskin, D.F.Y.; Hendem, D.U.; Buyuk, G.N.; Ayhan, S.G.; Tanacan, A.; Ozgu-Erdinc, A.S.; Tekin, O.M.; Sahin, D. Impact of vitamin D on the course of COVID-19 during pregnancy: A case control study. J. Steroid Biochem. Mol. Biol. 2021, 213, 105964. [Google Scholar] [CrossRef]
- Seven, B.; Gunduz, O.; Ozgu-Erdinc, A.S.; Sahin, D.; Tekin, O.M.; Keskin, H.L. Correlation between 25-hydroxy vitamin D levels and COVID-19 severity in pregnant women: A cross-sectional study. J. Matern. Neonatal Med. 2021, 23, 1–6. [Google Scholar] [CrossRef]
- Lian, R.H.; Qi, P.A.; Yuan, T.; Yan, P.J.; Qiu, W.W.; Wei, Y.; Hu, Y.G.; Yang, K.H.; Yi, B. Systematic review and meta-analysis of vitamin D deficiency in different pregnancy on preterm birth: Deficiency in middle pregnancy might be at risk. Medicine 2021, 100, e26303. [Google Scholar] [CrossRef]
- Zhou, S.-S.; Tao, Y.-H.; Huang, K.; Zhu, B.-B.; Tao, F.-B. Vitamin D and risk of preterm birth: Up-to-date meta-analysis of randomized controlled trials and observational studies. J. Obstet. Gynaecol. Res. 2017, 43, 247–256. [Google Scholar] [CrossRef] [Green Version]
- McDonnell, S.L.; Baggerly, K.A.; Baggerly, C.A.; Aliano, J.L.; French, C.B.; Baggerly, L.L.; Ebeling, M.D.; Rittenberg, C.S.; Goodier, C.G.; Mateus Nino, J.F.; et al. Maternal 25(OH)D concentrations >/= 40 ng/mL associated with 60% lower preterm birth risk among general obstetrical patients at an urban medical center. PLoS ONE 2017, 12, e0180483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poon, A.H.; Laprise, C.; Lemire, M.; Montpetit, A.; Sinnett, D.; Schurr, E.; Hudson, T.J. Association of Vitamin D Receptor Genetic Variants with Susceptibility to Asthma and Atopy. Am. J. Respir. Crit. Care Med. 2004, 170, 967–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wastnedge, E.A.N.; Reynolds, R.M.; Van Boeckel, S.R.; Stock, S.J.; Denison, F.C.; Maybin, J.A.; Critchley, H.O.D. Pregnancy and COVID-19. Physiol. Rev. 2021, 101, 303–318. [Google Scholar] [CrossRef] [PubMed]
- Jing, Y.; Run-Qian, L.; Hao-Ran, W.; Hao-Ran, C.; Ya-Bin, L.; Yang, G.; Fei, C. Potential influence of COVID-19/ACE2 on the female reproductive system. Mol. Hum. Reprod. 2020, 26, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Getachew, B.; Tizabi, Y. Vitamin D and COVID-19: Role of ACE2, age, gender, and ethnicity. J. Med. Virol. 2021, 93, 5285–5294. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Number of patients (n) | 160 |
| Age (years), median (IQR) | 32 (28) |
| Positive molecular swabs, n (%) | 15 (9) |
| At least one positive molecular swab or serological test, n (%) | 23 (14) |
| Cardioaspirin administration, n (%) | 4 (3) |
| Administration of low-molecular-weight heparin, n (%) | 2 (1) |
| Amniocentesis, n (%) | 5 (3) |
| Malformations, n (%) | 3 (2) |
| Abortions, n (%) | 2 (1) |
| Preterm birth, n (%) | 15 (11) |
| Alpha-fetoprotein (ng/mL), median (IQR) | 1 (0.9–1.2) |
| Estriol (ng/mL), median (IQR) | 1 (0.9–1.3) |
| Human chorionic gonadotropin (mlU/mL), median (IQR) | 1 (1.8–1.4) |
| Pregnancy-associated plasma protein A (UI/L), median (IQR) | 1 (0.7–1.6) |
| Nuchal translucency (mm), median (IQR) | 1.1 (0.9–1.2) |
| Vitamin D levels in first trimester (ng/mL), median (IQR) | 23 (17–29) |
| Vitamin D levels in second trimester (ng/mL), median (IQR) | 25 (19–35) |
| Vitamin D levels in third trimester (ng/mL), median (IQR) | 30 (23–39) |
| p-Values for Patients Negative for Every Test for SARS-CoV-2 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| A | E3 | AFP | NT | ABD-C | FFL | MAL | GD | AB | LRF DNA GD | AMNIO | PTB |
| VDR Taq I (TC_CC) | 0.02 | 0.003 | |||||||||
| VDR Taq I (CC) | 0.02 | ||||||||||
| VDR ApaI (CA_AA) | 0.03 | ||||||||||
| VDR FokI (CC) | 0.03 | ||||||||||
| VDR FokI (TC_CC) | 0.04 | ||||||||||
| VDR BsmI (AA) | 0.01 | ||||||||||
| VDR BsmI (GA_AA) | 0.03 | ||||||||||
| VDBP GC1296 (AC_CC) | 0.04 | ||||||||||
| CYP27A1 345 (GG) | 0.02 | ||||||||||
| CYP24A1 3999 (CC) | 0.03 | ||||||||||
| CYP24A1 22776 (TT) | 0.05 | ||||||||||
| B | p-Values for Patients with at Least One Positive Test for SARS-CoV-2 | ||||||||||
| CYP27B1 −1260 (TT) | 0.03 | ||||||||||
| CYP24A1 22776 (CT_TT) | 0.02 | ||||||||||
| VDR ApaI (AA) | 0.03 | 0.01 | 0.03 | ||||||||
| VDR FokI (CC) | 0.04 | ||||||||||
| CYP24A1 8620 (AG_GG) | 0.05 | ||||||||||
| CYP24A1 8620 (GG) | 0.01 | ||||||||||
| CYP27A1 345 (AG_GG) | 0.04 | ||||||||||
| CYP24A1 22776 (TT) | 0.01 | ||||||||||
| TOTAL | Patients Negative for Every Test for SARS-CoV-2 | Patients with at Least One Positive Test for SARS-CoV-2 | |
|---|---|---|---|
| 25-Vitamin D trimester 1 (ng/mL) | 23 (17–29) | 23 (17–28) | 27 (10–27) |
| 25-Vitamin D trimester 2 (ng/mL) | 25 (19–30) | 24 (19–30) | 28 (26–28) |
| 25-Vitamin D trimester 3 (ng/mL) | 30 (23–39) | 32 (24–40) | 20 (13–29) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manca, A.; Cosma, S.; Palermiti, A.; Costanzo, M.; Antonucci, M.; De Vivo, E.D.; Ianniello, A.; Borella, F.; Carosso, A.R.; Corcione, S.; et al. Pregnancy and COVID-19: The Possible Contribution of Vitamin D. Nutrients 2022, 14, 3275. https://doi.org/10.3390/nu14163275
Manca A, Cosma S, Palermiti A, Costanzo M, Antonucci M, De Vivo ED, Ianniello A, Borella F, Carosso AR, Corcione S, et al. Pregnancy and COVID-19: The Possible Contribution of Vitamin D. Nutrients. 2022; 14(16):3275. https://doi.org/10.3390/nu14163275
Chicago/Turabian StyleManca, Alessandra, Stefano Cosma, Alice Palermiti, Martina Costanzo, Miriam Antonucci, Elisa Delia De Vivo, Alice Ianniello, Fulvio Borella, Andrea Roberto Carosso, Silvia Corcione, and et al. 2022. "Pregnancy and COVID-19: The Possible Contribution of Vitamin D" Nutrients 14, no. 16: 3275. https://doi.org/10.3390/nu14163275
APA StyleManca, A., Cosma, S., Palermiti, A., Costanzo, M., Antonucci, M., De Vivo, E. D., Ianniello, A., Borella, F., Carosso, A. R., Corcione, S., De Rosa, F. G., Benedetto, C., D’Avolio, A., & Cusato, J. (2022). Pregnancy and COVID-19: The Possible Contribution of Vitamin D. Nutrients, 14(16), 3275. https://doi.org/10.3390/nu14163275