
Dietary Intake Patterns and Lifestyle Behaviors of Pregnant Women Living in a Manitoba First Nations Community: Implications for Fetal Alcohol Spectrum Disorder


Abstract
:1. Introduction
2. Experimental Design and Methodology
3. Results
3.1. Basic Demographics
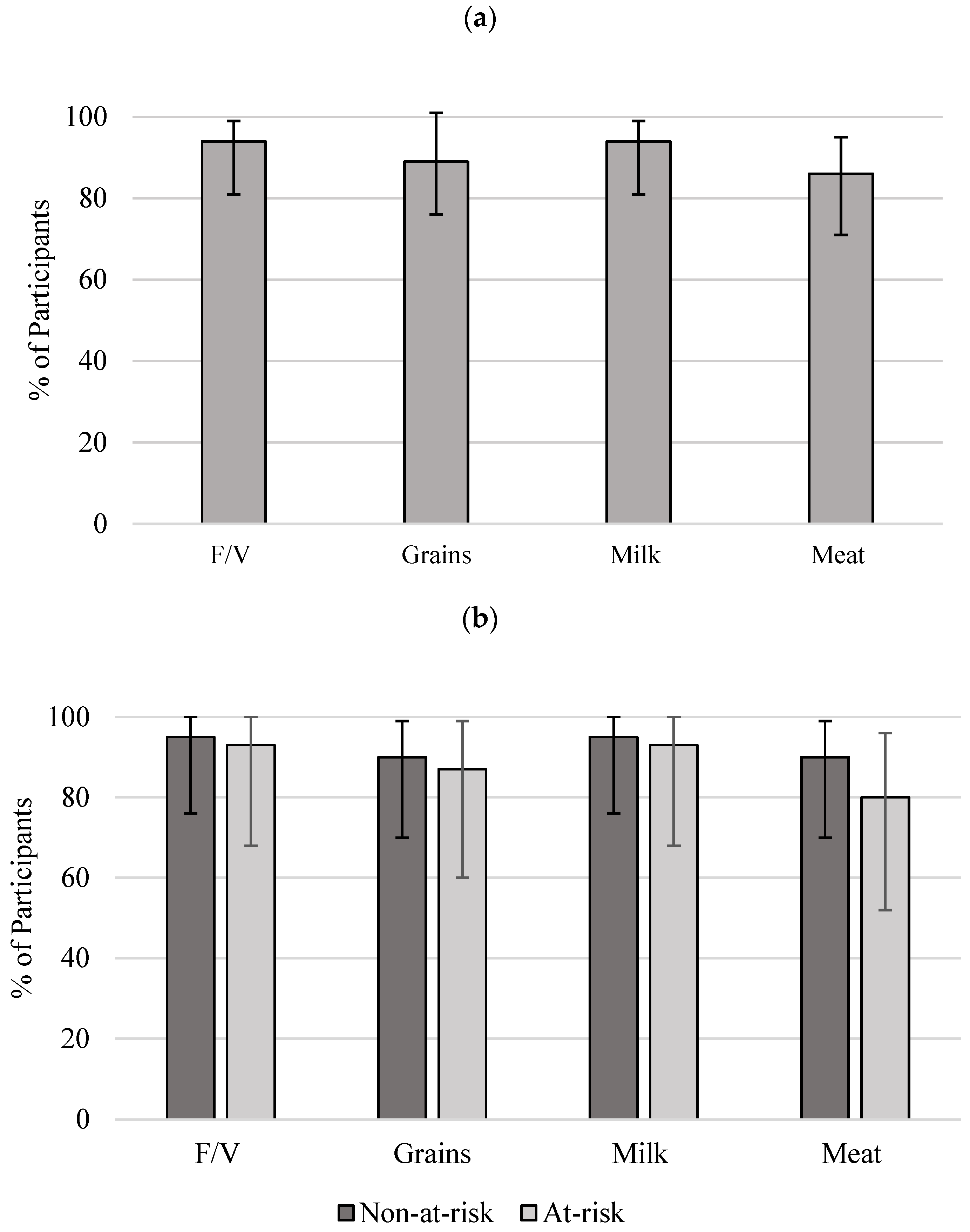
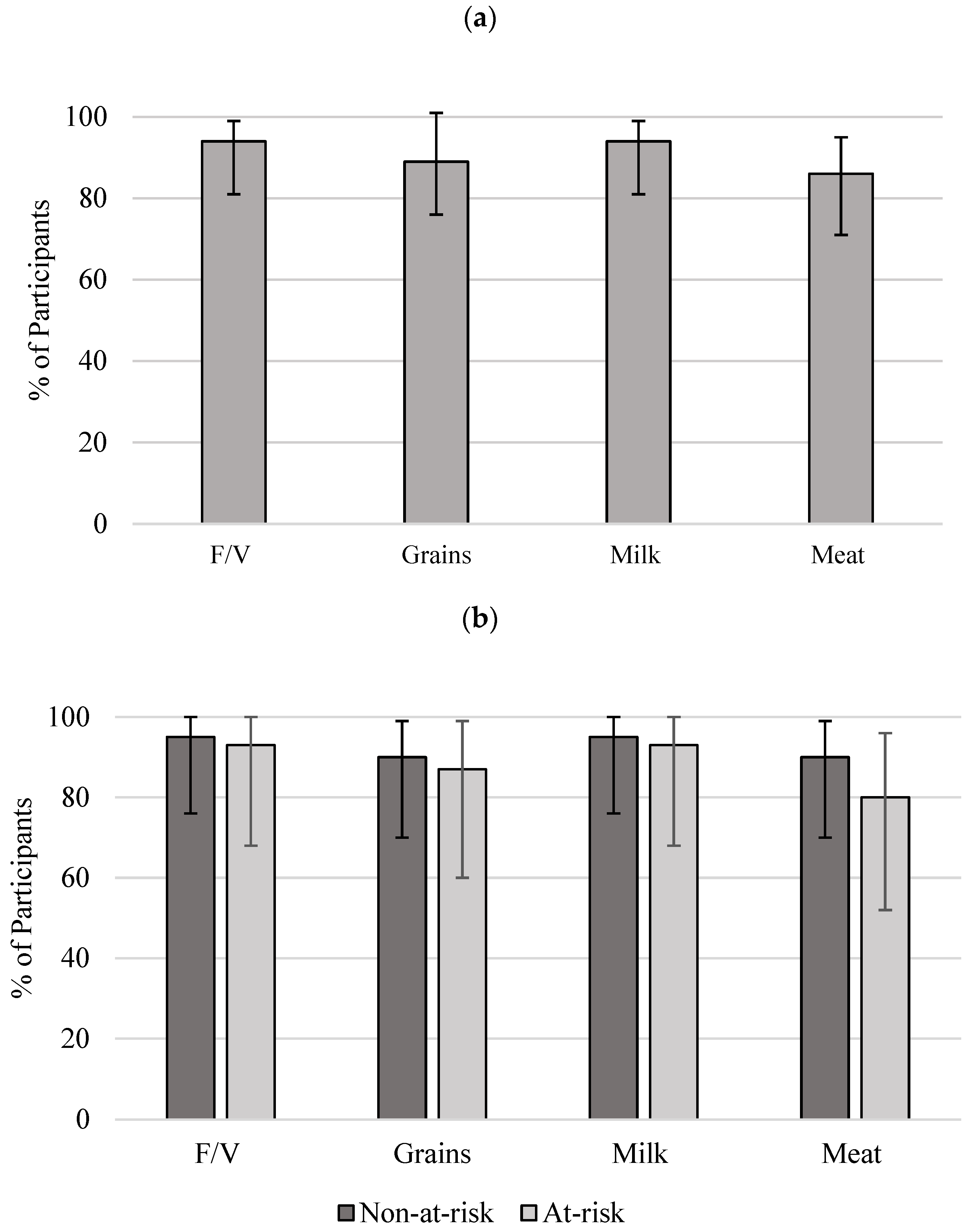
3.2. Food Group Intake
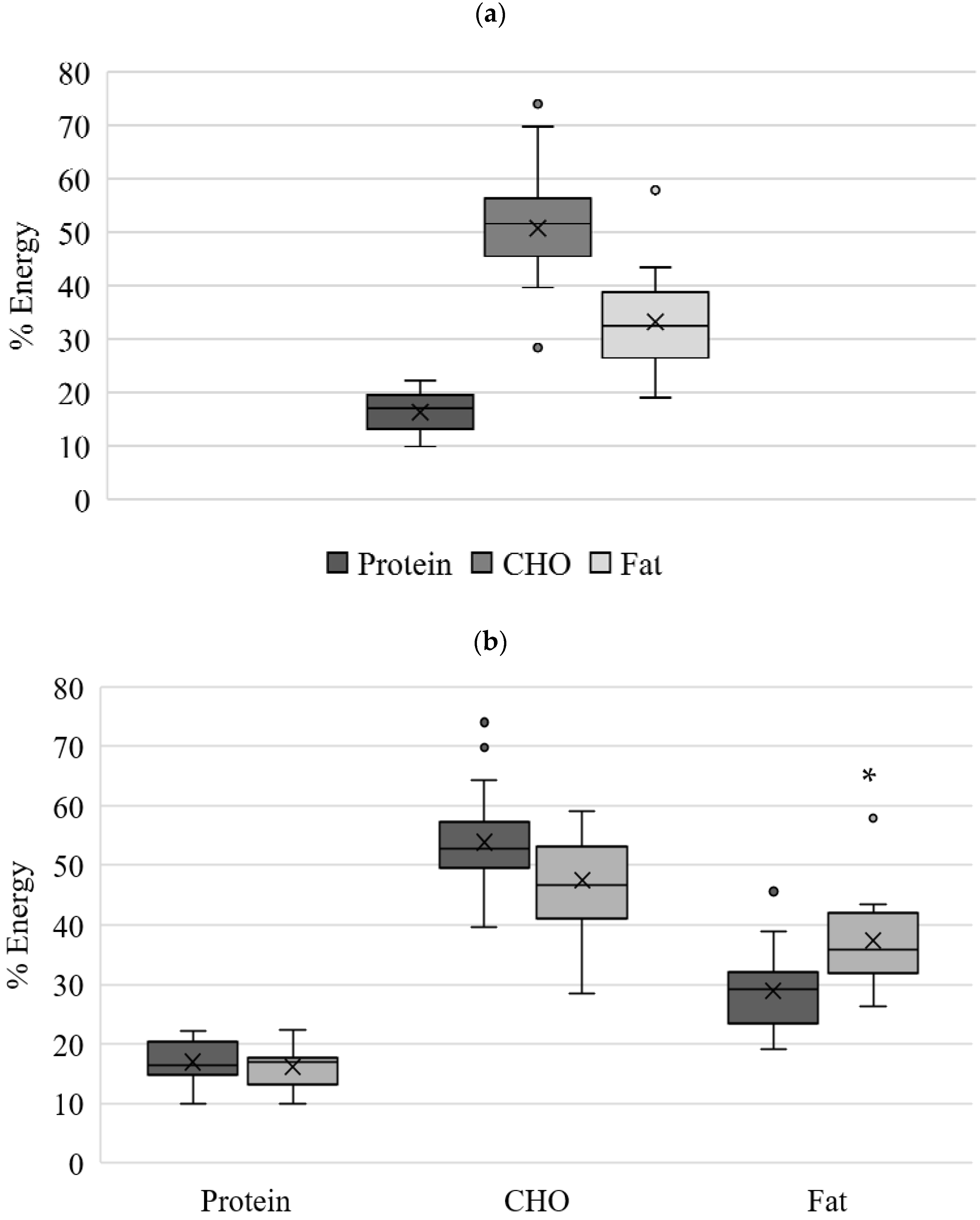
3.3. Macronutrient and Energy Intake
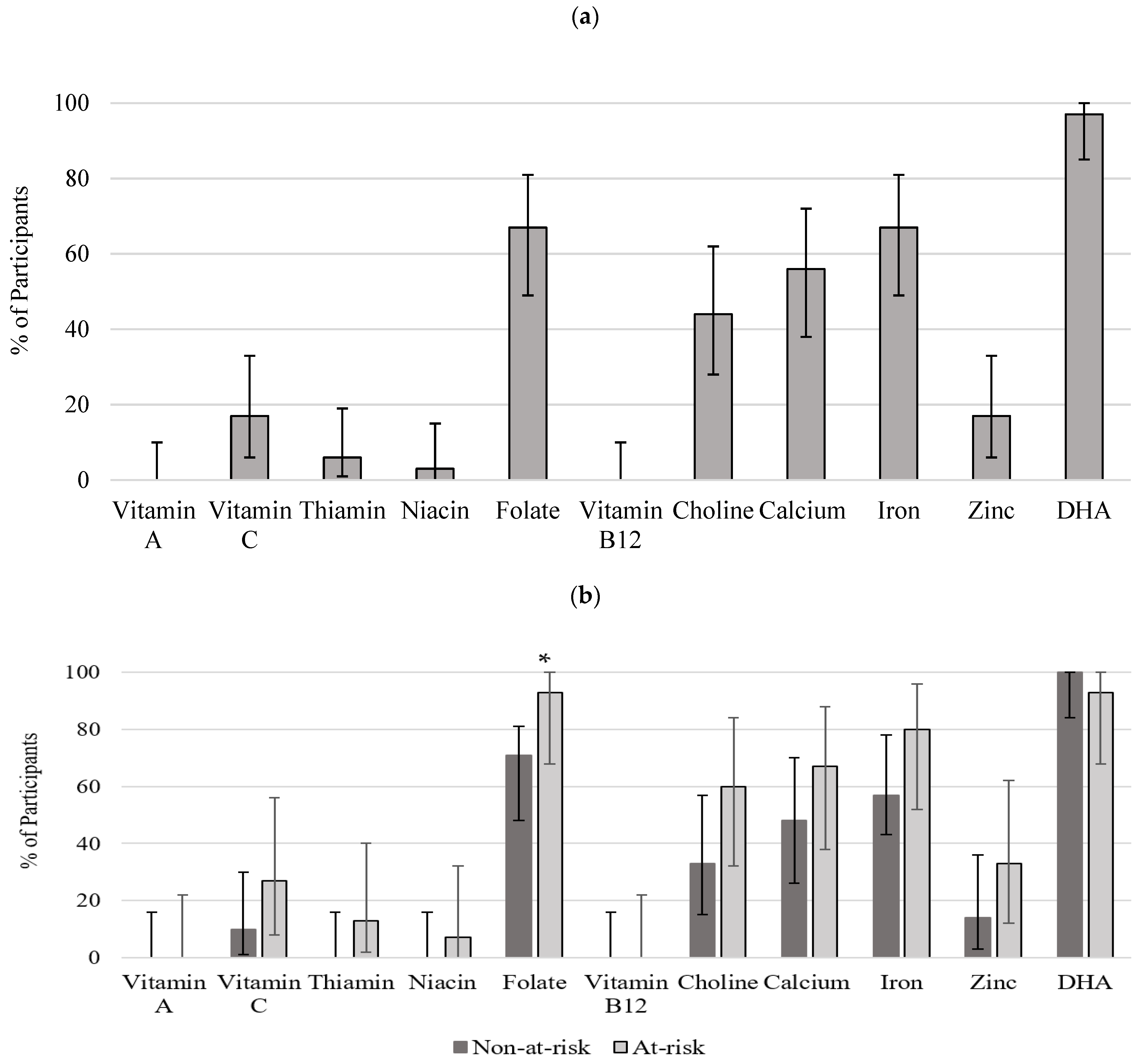
3.4. Micronutrient Intake
4. Discussion
4.1. Demographics and Maternal Health Status
4.2. Food Group and Macronutrient Intake
4.3. Micronutrient Intake
4.4. Strengths
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine. Dietary reference intakes (DRIs). 2014. Available online: http://iom.edu/Activities/Nutrition/SummaryDRIs/~/media/Files/Activity%20Files/Nutrition/DRIs/New%20Material/5DRI%20Values%20SummaryTables%2014.pdf (accessed on 1 February 2022).
- Green, C.; Blanchard, J.; Young, T.K.; Griffith, J. The epidemiology of diabetes in the Manitoba-registered First Nation population: Current patterns and comparative trends. Diabetes Care 1998, 26, 1993–1998. [Google Scholar] [CrossRef] [Green Version]
- Ramakrishnan, U.; Grant, F.; Goldenberg, T.; Zongrone, A.; Martorell, R. Effect of women’s nutrition before and during early pregnancy on maternal and infant outcomes: A systematic review. Paediatr. Perinat. Epidemiol. 2012, 26, 285–301. [Google Scholar] [CrossRef]
- Zakhari, S. Overview: How is alcohol metabolized by the body? Alcohol Res. Health 2006, 29, 245–254. [Google Scholar]
- World, M.J.; Ryle, P.R.; Thomson, A.D. Alcoholic malnutrition and the small intestine. Alcohol Alcohol. 1985, 20, 89–124. [Google Scholar]
- Ballard, M.S.; Sun, M.; Ko, J. Vitamin A, folate, and choline as a possible preventive intervention to fetal alcohol syndrome. Med. Hypotheses 2012, 78, 489–493. [Google Scholar] [CrossRef]
- May, P.A.; Gossage, J.P. Maternal risk factors for fetal alcohol spectrum disorders: Not as simple as it might seem. Alcohol Res. Health 2011, 34, 15–26. [Google Scholar]
- Public Health Agency of Canada. What Mothers Say: The Canadian Maternity Experiences Survey. 2009. Available online: https://www.canada.ca/content/dam/phac-aspc/migration/phac-aspc/rhs-ssg/pdf/survey-eng.pdf (accessed on 15 March 2022).
- AMC Health Information Research and Governance Committee; Elias, B.; LaPlante, J. Manitoba First Nations Regional Longitudinal Health Survey (RHS) Report (2002/03); Assembly of Manitoba Chiefs, Manitoba First Nations Centre for Aboriginal Health Research: Winnipeg, MB, Canada, 2006; Available online: http://www.fnhssm.com/images/PDF/manitoba-first-nations-regional-health-survey-report-2002-03.pdf (accessed on 20 February 2021).
- Park, J.; Tjepkema, M.; Goedhuis, N.; Pennock, J. Avoidable mortality among First Nations adults in Canada: A cohort analysis. Health Rep. 2015, 26, 10–16. [Google Scholar]
- First Nations Information Governance Centre (FNIGC). First Nations Regional Health Survey (RHS) 2008/10: National Report on Adults, Youth and Children Living in First Nation Communities; FNIGC: Ottawa, ON, Canada, 2012; Available online: http://www.fnigc.ca/sites/default/files/First%20Nations%20Regional%20Health%20Survey%20(RHS)%202008-10%20-%20National%20Report.pdf (accessed on 20 February 2020).
- Thompson, S.; Kamal, A.; Alam, M.; Wiebe, J. Community development to feed the family in northern Manitoba communities: Evaluating food activities based on their food sovereignty, food security, and sustainable livelihood outcomes. ANSERJ 2012, 2, 43–66. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, I.M.; Horbar, J.D.; Badger, G.J.; Ohlsson, A.; Golan, A. Morbidity and mortality among very-low-birth-weight neonates with intrauterine growth restriction. The Vermont Oxford Network. Am. J. Obstet. Gynecol. 2000, 182, 198–206. [Google Scholar] [CrossRef]
- Petrelli, B.; Bendelac, L.; Hicks, G.G.; Fainsod, A. Insights into retinoic acid deficiency and the induction of craniofacial malformations and microcephaly in fetal alcohol spectrum disorder. Genesis 2019, 57, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Didier, G. Obesity and Eating Habits of the Aboriginal Population. Health Rep. 2008, 19, 21–35. [Google Scholar]
- Cottrell, E.; Tropea, T.; Ormesher, L.; Greenwood, S.; Wareing, M.; Johnstone, E.; Myers, J.; Sibley, C. Dietary interventions for fetal growth restriction—therapeutic potential of dietary nitrate supplementation in pregnancy. J. Physiol. 2017, 595, 5095–5102. [Google Scholar] [CrossRef]
- Government of Canada. Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans—TCPS 2 (2018). 2020. Available online: https://ethics.gc.ca/eng/policy-politique_tcps2-eptc2_2018.html (accessed on 20 February 2020).
- First Nations Information Governance Centre (FNIGC). The Fundamental of OCAP. 2020. Available online: https://fnigc.ca/ocap-training/ (accessed on 20 February 2020).
- Giesbrecht, H. Laying the Groundwork for Prenatal Dietary Assessment Research among First Nations Women at Risk for Alcohol Use: Implications for Fetal Alcohol Spectrum Disorder. Master’s Thesis, University of Manitoba, Winnipeg, MB, Canada, 2015. [Google Scholar]
- Health Canada. Canada’s Food Guide. 2007. Available online: https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/fn-an/alt_formats/fnihb-dgspni/pdf/pubs/fnim-pnim/2007_fnim-pnim_food-guide-aliment-eng.pdf (accessed on 1 March 2021).
- Government of Canada. Canadian Nutrient File (CNF). 2018. Available online: https://food-nutrition.canada.ca/cnf-fce/index-eng.jsp (accessed on 1 March 2021).
- Young, J.K.; Giesbrecht, H.E.; Eskin, M.N.; Aliani, M.; Suh, M. Nutrition implications for fetal alcohol spectrum disorder. Adv. Nutr. 2014, 5, 675–692. [Google Scholar] [CrossRef] [Green Version]
- Sauvageot, N.; Alkerwi, A.; Albert, A.; Guillaume, M. Use of food frequency questionnaire to assess relationships between dietary habits and cardiovascular risk factors in NESCAV study: Validation with biomarkers. Nutr. J. 2013, 12, 143. [Google Scholar] [CrossRef] [Green Version]
- International Society for the Study of Fatty Acids and Lipids. Global Recommendations for EPA and DHA Intake. 2014. Available online: https://www.issfal.org/assets/globalrecommendationssummary19nov2014landscape_-3-.pdf (accessed on 1 March 2022).
- Oliveira, A.P.; Kalra, S.; Wahi, G. Maternal and new-born health profile in a first nations community in Canada. J. Obstet. Gynaecol. Can. 2013, 35, 905–913. [Google Scholar] [CrossRef]
- Wenman, W.M.; Joffres, M.R.; Tataryn, I.V.; The Edmonton Perinatal Infections Group. A prospective cohort study of pregnancy risk factors and birth outcomes in Aboriginal women. CMAJ 2004, 171, 585–589. [Google Scholar] [CrossRef] [Green Version]
- Dyck, R.; Klomp, H.; Tan, L.K.; Turnell, R.W.; Boctor, M.A. A Comparison of Rates, Risk Factors, and Outcomes of Gestational Diabetes Between Aboriginal and Non-Aboriginal Women in the Saskatoon Health District. Diabetes Care 2002, 25, 487–493. [Google Scholar] [CrossRef] [Green Version]
- Christian, L.M.; Iams, J.; Porter, K.; Leblebicioglu, B. Self-rated health among pregnant women: Associations with objective health indicators, psychological functioning, and serum inflammatory markers. Ann. Behav. Med. 2014, 46, 295–309. [Google Scholar] [CrossRef] [Green Version]
- Stupin, J.H.; Arabin, B. Overweight and obesity before, during and after pregnancy. Part 1: Pathophysiology, molecular biology and epigenetic consequences. Geburtsh Frauenheilk 2014, 74, 639–645. [Google Scholar]
- Ovesen, P.; Rassmussen, S.; Kesmodel, U. Effect of prepregnancy overweight and obesity on pregnancy outcome. Obstet. Gynecol. 2001, 118, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Plagemann, A. Fetal programming and functional teratogenesis: On epigenetic mechanisms and prevention of perinatally acquired lasting health risks. J. Perinat. Med. 2004, 32, 297–305. [Google Scholar] [CrossRef]
- Haste, F.M.; Brooke, O.G.; Anderson, H.R.; Bland, J.M.; Shaw, A.; Griffin, J.; Peacock, J.L. Nutrient intakes during pregnancy: Observations on the influence of smoking and social class. Am. J. Clin. Nutr. 1990, 51, 29–36. [Google Scholar] [CrossRef]
- Johnson-Down, L.; Egeland, G.M. How is nutrition transition affecting dietary adequacy in Eeyouch (Cree) adults of Northern Quebec, Canada? Appl. Physiol. Nutr. Metab. 2012, 38, 300–305. [Google Scholar] [CrossRef] [Green Version]
- Tarasuk, V.; Cheng, J.; de Oliveira, C.; Dachner, N.; Gundersen, C.; Kurdyak, P. Association between household food insecurity and annual health care costs. CMAJ 2015, 187, 429–436. [Google Scholar] [CrossRef] [Green Version]
- Back, L.; Hui, A.; Reid, A.; Sevenhuysen, G.; Gardiner, P.; Ludwig, S.; Shen, G.X. Comparison of Physical Activity and Nutritional Intake in First Nations Pregnant Women in Remote Communities and Urban-Living Pregnant Women. Can. J. Diabetes 2012, 36, 64–67. [Google Scholar] [CrossRef]
- Carter, R.C.; Senekal, M.; Duggan, C.P.; Dodge, N.C.; Meintjes, E.M.; Molteno, C.D.; Jacobson, J.L.; Jacobson, S.W. Gestational weight gain and dietary energy, iron, and choline intake predict severity of fetal alcohol growth restriction in a prospective birth cohort. Am. J. Clin. Nutr. 2022, 116, 460–469. [Google Scholar] [CrossRef]
- Wang, Y.; Feltham, B.A.; Eskin, M.N.A.; Suh, M. Differential effects of maternal diets on birth outcomes and metabolic parameters in rats after ethanol consumption during pregnancy. Br. J. Nutr. 2021, 126, 1130–1139. [Google Scholar] [CrossRef]
- Berti, P.R.; Soueida, R.; Kuhnlein, H.V. Dietary assessment of Indigenous Canadian Arctic women with a focus on pregnancy and lactation. Int. J. Circumpolar Health 2008, 67, 349–362. [Google Scholar] [CrossRef]
- First Nations Food, Nutrition and Environment Study (FNFNES): Results from Manitoba (2010). University of Northern British Columbia, Université de Montréal and Assembly of First Nations 2012. Available online: http://www.fnfnes.ca/docs/MB%20Reports/FNFNES%20Report-MB_WEB_rev.pdf (accessed on 1 March 2022).
- Halsted, C.H.; Villanueva, J.A.; Devlin, A.M.; Chandler, C.J. Metabolic Interactions of Alcohol and Folate. J. Nutr. 2002, 132, 2367–2372. [Google Scholar] [CrossRef] [Green Version]
- McMartin, K.E.; Collins, T.D.; Eisenga, B.H.; Fortney, T.; Bates, W.R.; Bairnsfather, L. Effects of chronic ethanol and diet treatment on urinary folate excretion and development of folate deficiency in the rat. J. Nutr. 1989, 119, 1490–1497. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations. Fats and Fatty Acids in Human Nutrition: Report of an Expert Consultation; FAO Food and Nutrition: Rome, Italy, 2010. [Google Scholar]
- Denomme, J.; Stark, K.D.; Holub, B.J. Directly quantitated dietary (n-3) fatty acid intakes of pregnant Canadian women are lower than current dietary recommendations. J. Nutr. 2005, 135, 206–211. [Google Scholar] [CrossRef]
- Friesen, R.W.; Innis, S.M. Linoleic acid is associated with lower long-chain n-6 and n-3 fatty acids in red blood cell lipids of Canadian pregnant women. Am. J. Clin. Nutr. 2010, 91, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Bishop, N.A.; Leblanc, C.P. Dietary Intake of DHA and EPA in a Group of Pregnant Women in the Moncton Area. Can. J. Diet. Pract. Res. 2017, 78, 59–65. [Google Scholar] [CrossRef]
- Ford, S.M.; Pedersen, C.J.; Ford, M.R.; Kim, J.W.; Karunamuni, G.H.; McPheeters, M.T.; Jawaid, S.; Jenkins, M.W.; Rollins, A.M.; Watanabe, M. Folic acid prevents functional and structural heart defects induced by prenatal ethanol exposure. Am. J. Physiol. Heart Circ. 2021, 320, H1313–H1320. [Google Scholar] [CrossRef]
- MacDonand, K. The Impact of Colonization and Western Assimilation on Health and Wellbeing of Canadian Aboriginal People. Int. J. Reg. Local Hist. 2015, 10, 32–46. [Google Scholar] [CrossRef]
- Heart, M. The historical trauma response among Natives and its relationship with substance abuse: A Lakota illustration. J. Psychoact. Drugs 2003, 35, 7–13. [Google Scholar] [CrossRef]
- Bourassa, C.; McKay-McNabb, K.; Hampton, M.R. Racism, Sexism, and Colonialism: The Impact on the Health of Aboriginal Women in Canada. Can Woman Stud. 2004, 24, 23–29. [Google Scholar]
- Sheridan, B. “Strangers in a Strange Land”: A Literature Review of Women in Science; Simmons Institute for Leadership and Change: Boston, MA, USA, 1998. [Google Scholar]
- Canada FASD Research Network (CanFASD). Prevention of Fetal Alcohol Spectrum Disorder (FASD) A Multi-Level Model. 2013. Available online: http://fasd.alberta.ca/documents/CanFASD_4_levels_of_prevention_brief.pdf (accessed on 1 February 2022).
- Census Profile, 2016 Census. Opaskwayak Cree Nation 21A, Indian Reserve. 2016. Available online: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/page.cfm?Lang=E&Geo1=CSD&Code1=4621033&Geo2=PR&Code2=46&SearchText=Opaskwayak%20Cree%20Nation%2021A&SearchType=Begins&SearchPR=01&B1=All&GeoLevel=PR&GeoCode=4621033&TABID=1&type=0 (accessed on 1 February 2022).
- Keen, C.L.; Uriu-Adams, J.Y.; Skalny, A.; Grabeklis, A.; Grabeklis, S.; Green, K.; Yevtushok, L.; Wertelecki, W.W.; Chambers, C.D. The plausibility of maternal nutritional status being a contributing factor to the risk for fetal alcohol spectrum disorders: The potential influence of zinc status as an example. Biofactors 2010, 36, 125–135. [Google Scholar] [CrossRef] [Green Version]
- Sowell, K.D.; Holt, R.R.; Uriu-Adams, J.Y.; Chambers, C.D.; Coles, C.D.; Kable, J.A.; Yevtushok, L.; Zymak-Zakutnya, N.; Wertelecki, W.; Keen, C.L.; et al. Altered maternal plasma fatty acid composition by alcohol consumption and smoking during pregnancy and associations with fetal alcohol spectrum disorders. J. Am. Coll. Nutr. 2020, 39, 249–260. [Google Scholar] [CrossRef] [Green Version]
- Prentice, R.L.; Pettinger, M.; Tinker, L.F.; Huang, Y.; Thomson, C.A.; Johnson, K.C.; Beasley, J.; Anderson, G.; Shikany, J.M.; Chlebowski, R.T.; et al. Regression calibration in nutritional epidemiology: Example of fatdensity and total energy in relationship to postmenopausal breast cancer. Am. J. Epidemiol. 2013, 178, 1663–1672. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| All Women (n = 37) | Non-at-Risk (n = 22) | At-Risk (n = 15) | p-Value | |
|---|---|---|---|---|
| Age a (Range) | 24.4 ± 7.0 (14–42) | 21.5 ± 5.5 (14–31) | 28.1 ± 7.4 * (14–42) | 0.007 |
| Education b Elementary Junior high High school Post-secondary | 1 (3) 16 (44) 15 (41) 5 (14) | 1 (5) 12 (55) 6 (27) 3 (14) | 0 5 (33) 8 (53) 2 (13) | 0.196 |
| Employment b Unemployed Employed part-time Employed full-time Student Maternity Leave | 14 (39) 4 (11) 6 (16) 10 (28) 2 (6) | 8 (38) 2 (9.5) 4 (19) 5 (24) 2 (9) | 6 (40) 2 (13) 2 (13) 5 (33) 0 (0) | 0.237 |
| Social Assistance c | 19 (51) | 10 (46) | 9 (60) | 0.385 |
| Pre-pregnancy BMI a Below Normal Overweight Obese | 26.5 ± 8.8 4 (12) 11 (33) 7 (21) 11 (33) | 27.5 ± 8.3 2 (11) 6 (33) 3 (17) 7 (39) | 25.9 ± 7.8 2 (13) 5 (33) 4 (27) 4 (27) | 0.530 |
| Chronic illness: Before pregnancy b During pregnancy b | 5 (15) 7 (21) | 2 (10) 4 (20) | 3 (20) 3 (20) | 0.403 1.000 |
| Smoking | 11 (37) | 7 (35) | 6 (40) | 0.762 |
| Drugs c | 7 (19) | 4 (19) | 3 (20) | 0.943 |
| Pregnancy outcomes: # of pregnancies a # of miscarriages a # of stillbirths a # of full-term births a # of pre-term births a | 3.0 ± 2.2 0.6 ± 0.9 0.1 ± 0.4 1.0 ± 1.0 0.4 ± 1.0 | 2.7 ± 1.9 0.7 ± 1.0 0.1 ± 0.2 0.6 ± 1.4 0.3 ± 0.7 | 3.5 ± 2.6 0.5 ± 0.8 0.2 ± 0.4 1.4 ± 1.5 0.5 ± 1.6 | 0.439 0.620 0.190 0.110 0.690 |
| Bed rest during pregnancy c | 6 (18) | 5 (25) | 1 (7) | 0.179 |
| Food Group | Reference Intake | All Women (n = 37) | Non-at-Risk (n = 22) | Exposed (n = 15) | p-Value |
|---|---|---|---|---|---|
| Vegetable and Fruit | 9 | 5 ± 3 | 5 ± 3 | 5 ± 3 | 0.783 |
| Grain Products | 8 | 5 ± 3 | 5 ± 3 | 5 ± 3 | 0.835 |
| Milk and Alternatives | 3 | 2 ± 1 | 2 ± 1 | 2 ± 2 | 0.570 |
| Meat and Alternatives | 2 | 3 ± 2 | 2 ± 2 | 3 ± 3 | 0.174 |
| Macronutrient (Grams/Day) | All Women (n = 37) | Non-at-Risk (n = 22) | At-Risk (n = 15) | p-Value * |
|---|---|---|---|---|
| Protein | 87 ± 35 | 82 ± 35 | 93 ± 35 | 0.390 |
| CHO 1 | 257 ± 96 | 244 ± 105 | 272 ± 85 | 0.430 |
| Fat | 78 ± 49 | 58 ± 27 | 102 ± 59 * | 0.010 |
| Sugar | 84 ± 46 | 89 ± 55 | 77 ± 33 | 0.510 |
| All Women (n = 37) | Non-at-Risk (n = 22) | At-Risk (n = 15) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Micronutrient | Ref. DRI/Day | Intake | %DRI | Intake | %DRI | Intake | %DRI | |
| Vitamin A (RE) | 550 (mcg) | 1552 ± 1254 | 288 ± 229 | 1396 ± 613 | 258 ± 114 | 1815 ± 1833 | 339 ± 333 | 0.307 |
| Vitamin C | 70 (mg) | 171 ± 128 | 251 ± 189 | 214 ± 152 | 313 ± 224 | 115 ± 53 * | 172 ± 81 | 0.013 |
| Thiamin (Vit B1) | 1.2 (mg) | 3 ± 3 | 272 ± 245 | 3 ± 1 | 267 ± 104 | 4 ± 4 | 294 ± 368 | 0.747 |
| Niacin (Vit B2) | 14 (mg) | 34 ± 16 | 241 ± 116 | 39 ± 17 | 281 ± 123 | 29 ± 12 * | 198 ± 80 | 0.029 |
| Folate (Vit B9) | 520 (mcg) | 453 ± 194 | 86 ± 36 | 522 ± 200 | 70 ± 38 | 377 ± 142 * | 10 ± 22 | 0.009 |
| Vitamin B12 | 2.2 (mcg) | 12 ± 10 | 540 ± 436 | 12 ± 6 | 565 ± 279 | 12 ± 13 | 535 ± 601 | 0.841 |
| Choline | 450 (mg) | 524 ± 265 | 116 ± 59 | 601 ± 298 | 128 ± 65 | 441 ± 165 | 99 ± 46 | 0.123 |
| Calcium | 800 (mg) | 1011 ± 531 | 116 ± 58 | 1126 ± 546 | 129 ± 62 | 885 ± 491 | 101 ± 47 | 0.153 |
| Iron | 22 (mg) | 20 ± 10 | 88 ± 40 | 23 ± 9 | 101 ± 74 | 18 ± 9 * | 74 ± 30 | 0.039 |
| Zinc | 9.5 (mg) | 18 ± 10 | 176 ± 102 | 21 ± 12 | 206 ± 121 | 15 ± 8 | 142 ± 45 | 0.060 |
| DHA | 200 (mg) | 78 ± 49 | 39 ± 25 | 93 ± 56 | 42 ± 24 | 79 ± 50 | 35 ± 26 | 0.383 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kloss, O.; Jebb, M.; Chartrand, L.; Chudley, A.E.; Eskin, M.N.A.; Suh, M. Dietary Intake Patterns and Lifestyle Behaviors of Pregnant Women Living in a Manitoba First Nations Community: Implications for Fetal Alcohol Spectrum Disorder. Nutrients 2022, 14, 3233. https://doi.org/10.3390/nu14153233
Kloss O, Jebb M, Chartrand L, Chudley AE, Eskin MNA, Suh M. Dietary Intake Patterns and Lifestyle Behaviors of Pregnant Women Living in a Manitoba First Nations Community: Implications for Fetal Alcohol Spectrum Disorder. Nutrients. 2022; 14(15):3233. https://doi.org/10.3390/nu14153233
Chicago/Turabian StyleKloss, Olena, Marie Jebb, Linda Chartrand, Albert E. Chudley, Michael N. A. Eskin, and Miyoung Suh. 2022. "Dietary Intake Patterns and Lifestyle Behaviors of Pregnant Women Living in a Manitoba First Nations Community: Implications for Fetal Alcohol Spectrum Disorder" Nutrients 14, no. 15: 3233. https://doi.org/10.3390/nu14153233
APA StyleKloss, O., Jebb, M., Chartrand, L., Chudley, A. E., Eskin, M. N. A., & Suh, M. (2022). Dietary Intake Patterns and Lifestyle Behaviors of Pregnant Women Living in a Manitoba First Nations Community: Implications for Fetal Alcohol Spectrum Disorder. Nutrients, 14(15), 3233. https://doi.org/10.3390/nu14153233