
The Relationship between Addictive Eating and Dietary Intake: A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Criteria
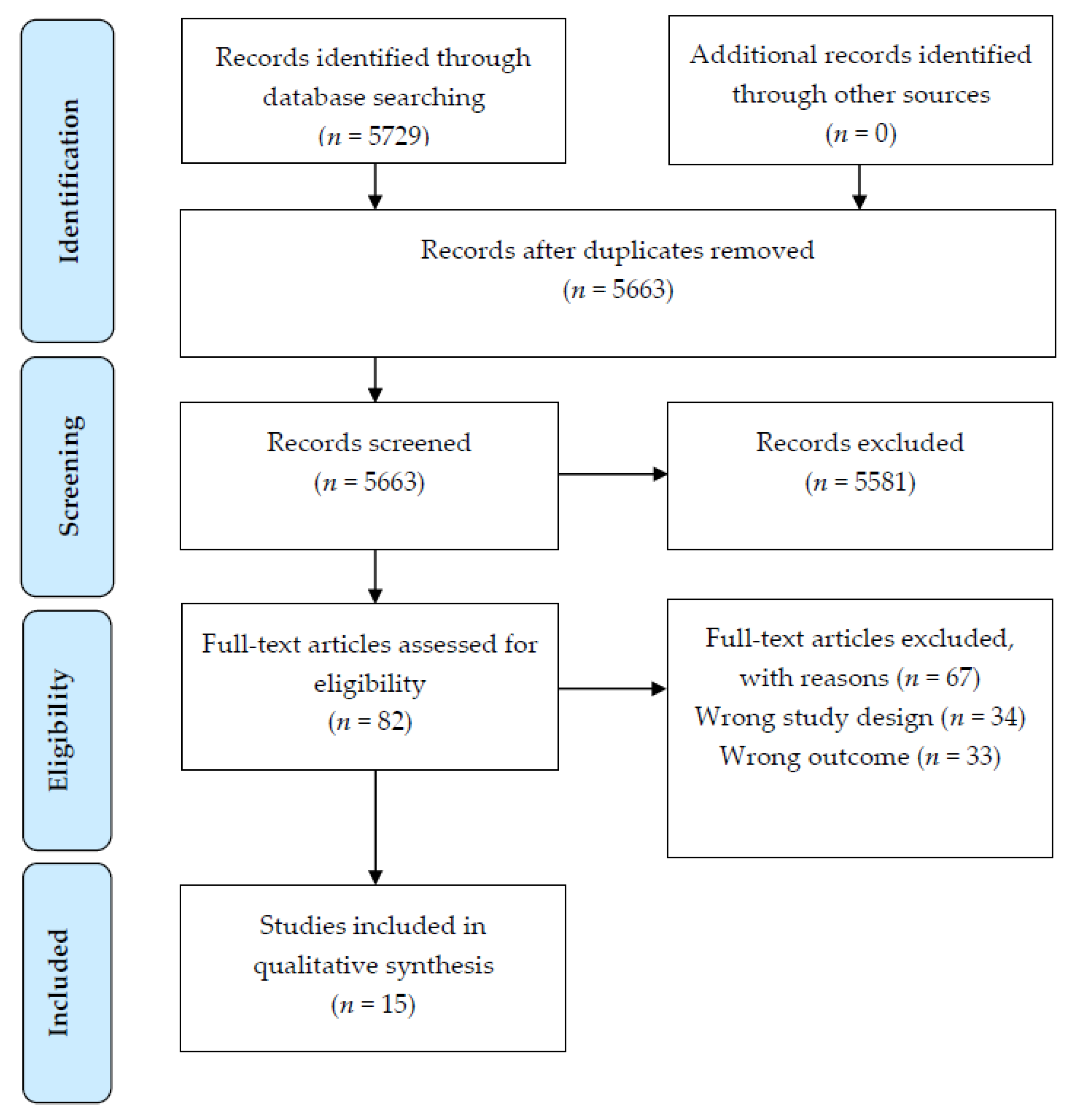
2.3. Study Selection
2.4. Data Extraction and Synthesis
2.5. Quality of Evidence
3. Results
3.1. Description of Included Studies
3.2. Quality of Included Studies
3.3. Participant Characteristics
3.4. Addictive Eating Assessment and Outcomes
3.5. Dietary Intake Assessment and Outcomes
3.6. Relationships and Associations between Addictive Eating and Dietary Outcomes
3.6.1. Energy Intake
3.6.2. Macronutrient Intakes
3.6.3. Micronutrient Intakes
3.6.4. Food Items/Food Groups
3.6.5. Overall Dietary Quality/Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Food addiction: An examination of the diagnostic criteria for dependence. J. Addict. Med. 2009, 3, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Volkow, N.D.; Wang, G.J.; Tomasi, D.; Baler, R.D. Obesity and addiction: Neurobiological overlaps. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2013, 14, 2–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenny, P.J. Common cellular and molecular mechanisms in obesity and drug addiction. Nat. Rev. Neurosci. 2011, 12, 638–651. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Loxton, N.J. A Psycho-Genetic Study of Hedonic Responsiveness in Relation to “Food Addiction”. Nutrients 2014, 6, 4338–4353. [Google Scholar] [CrossRef]
- Pursey, K.; Stanwell, P.; Gearhardt, A.; Collins, C.E.; Burrows, T.L. The prevalence of food addiction as assessed by the Yale Food Addiction Scale: A systematic review. Nutrients 2014, 6, 4552–4590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burrows, T.; Kay-Lambkin, F.; Pursey, K.; Skinner, J.; Dayas, C. Food addiction and associations with mental health symptoms: A systematic review with meta-analysis. J. Hum. Nutr. Diet. 2018, 31, 544–572. [Google Scholar] [CrossRef]
- Skinner, J.; Jebeile, H.; Burrows, T. Food addiction and mental health in adolescents: A systematic review. Lancet Child Adolesc. Health 2021, 5, 751–766. [Google Scholar] [CrossRef]
- Pursey, K.M.; Davis, D.; Burrows, T. Nutritional Aspects of Food Addiction. Curr. Addict. Rep. 2017, 4, 142–150. [Google Scholar] [CrossRef]
- Ziauddeen, H.; Farooqi, I.S.; Fletcher, P.C. Obesity and the brain: How convincing is the addiction model? Nat. Rev. Neurosci. 2012, 13, 279–286. [Google Scholar] [CrossRef]
- Hebebrand, J.; Albayrak, Ö.; Adan, R.; Antela, J.; Dieguez, C.; de Jong, J.; Leng, G.; Menzies, J.; Mercer, J.G.; Murphy, M.; et al. “Eating addiction”, rather than “food addiction”, better captures addictive-like eating behavior. Neurosci. Biobehav. Rev. 2014, 47, 295–306. [Google Scholar] [CrossRef] [Green Version]
- Hauck, C.; Cook, B.; Ellrott, T. Food addiction, eating addiction and eating disorders. Proc. Nutr. Soc. 2020, 79, 103–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulte, E.M.; Potenza, M.N.; Gearhardt, A.N. A commentary on the “eating addiction” versus “food addiction” perspectives on addictive-like food consumption. Appetite 2017, 115, 9–15. [Google Scholar] [CrossRef]
- NeuroFAST. NeuroFAST Consensus Opinion on Food Addiction; NeuroFAST: Bucksburn, UK, 2013. [Google Scholar]
- Gearhardt, A.N.; Davis, C.; Kuschner, R.; Brownell, K.D. The Addiction Potential of Hyperpalatable Foods. Curr. Drug Abus. Rev. 2011, 4, 140–145. [Google Scholar] [CrossRef]
- Schulte, E.M.; Avena, N.M.; Gearhardt, A.N. Which Foods May Be Addictive? The Roles of Processing, Fat Content, and Glycemic Load. PLoS ONE 2015, 10, e0117959. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Grilo, C.M.; DiLeone, R.J.; Brownell, K.D.; Potenza, M.N. Can food be addictive? Public Health Policy Implic. Addict. 2011, 106, 1208–1212. [Google Scholar]
- Avena, N.M.; Rada, P.; Hoebel, B.G. Evidence for sugar addiction: Behavioral and neurochemical effects of intermittent, excessive sugar intake. Neurosci. Biobehav. Rev. 2008, 32, 20–39. [Google Scholar] [CrossRef] [Green Version]
- Corwin, R.L.; Wojnicki, F.H.; Fisher, J.O.; Dimitriou, S.G.; Rice, H.B.; Young, M.A. Limited access to a dietary fat option affects ingestive behavior but not body composition in male rats. Physiol. Behav. 1998, 65, 545–553. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Schulte, E.M. Is Food Addictive? A Review of the Science. Annu. Rev. Nutr. 2021, 41, 387–410. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Levy, R.B.; Claro, R.M.; Castro, I.R.; Cannon, G. A New Classification of Foods Based on the Extent and Purpose of Their Processing; Cadernos de Saúde Pública: Rio de Janeiro, Beazil, 2010; Volume 26, pp. 2039–2049. [Google Scholar]
- Gibney, M.J.; Forde, C.G.; Mullally, D.; Gibney, E.R. Ultra-processed foods in human health: A critical appraisal. Am. J. Clin. Nutr. 2017, 106, 717–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Zhang, Z.; Yang, H.; Qiu, P.; Wang, H.; Wang, F.; Zhao, Q.; Fang, J.; Nie, J. Consumption of ultra-processed foods and health outcomes: A systematic review of epidemiological studies. Nutr. J. 2020, 19, 86. [Google Scholar] [CrossRef]
- Kirkpatrick, S.I.; Baranowski, T.; Subar, A.F.; Tooze, J.A.; Frongillo, E.A. Best Practices for Conducting and Interpreting Studies to Validate Self-Report Dietary Assessment Methods. J. Acad. Nutr. Diet. 2019, 119, 1801–1816. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Preliminary validation of the Yale Food Addiction Scale. Appetite 2009, 52, 430–436. [Google Scholar] [CrossRef] [Green Version]
- Ruddock, H.K.; Christiansen, P.; Halford, J.C.G.; Hardman, C.A. The development and validation of the Addiction-like Eating Behaviour Scale. Int. J. Obes. 2017, 41, 1710–1717. [Google Scholar] [CrossRef] [Green Version]
- Academy of Nutrition and Dietetics. Evidence Analysis Manual: Steps in the Academy Evidence Analysis Process. 2016. Available online: https://www.andeal.org/evidence-analysis-manual (accessed on 8 March 2017).
- Ayaz, A.; Nergiz-Unal, R.; Dedebayraktar, D.; Akyol, A.; Pekcan, A.G.; Besler, H.T.; Buyuktuncer, Z. How does food addiction influence dietary intake profile? PLoS ONE 2018, 13, e0195541. [Google Scholar] [CrossRef] [Green Version]
- Burrows, T.; Skinner, J.; McKenna, R.; Rollo, M. Food Addiction, Binge Eating Disorder, and Obesity: Is There a Relationship? Behav. Sci. 2017, 7, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filgueiras, A.R.; de Almeida, V.B.P.; Nogueira, P.C.K.; Domene, S.M.A.; da Silva, C.E.; Sesso, R.; Sawaya, A.L. Exploring the consumption of ultra-processed foods and its association with food addiction in overweight children. Appetite 2019, 135, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Grammatikopoulou, M.G.; Gkiouras, K.; Markaki, A.; Theodoridis, X.; Tsakiri, V.; Mavridis, P.; Dardavessis, T.; Chourdakis, M. Food addiction, orthorexia, and food-related stress among dietetics students. Eat Weight Disord. 2018, 23, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Keser, A.; Yuksel, A.; Yesiltepe-Mutlu, G.; Bayhan, A.; Ozsu, E.; Hatun, S. A new insight into food addiction in childhood obesity. Turk. J. Pediatr. 2015, 57, 219–224. [Google Scholar] [PubMed]
- Kucukerdonmez, O.; Urhan, M.; Altin, M.; Haciraifoglu, O.; Yildiz, B. Assessment of the relationship between food addiction and nutritional status in schizophrenic patients. Nutr. Neurosci. 2019, 22, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Moghaddam, S.A.P.; Amiri, P.; Saidpour, A.; Hosseinzadeh, N.; Abolhasani, M.; Ghorbani, A. The prevalence of food addiction and its associations with plasma oxytocin level and anthropometric and dietary measurements in Iranian women with obesity. Peptides 2019, 122, 170151. [Google Scholar] [CrossRef]
- Pedram, P.; Sun, G. Hormonal and dietary characteristics in obese human subjects with and without food addiction. Nutrients 2015, 7, 223–238. [Google Scholar] [CrossRef] [Green Version]
- Pedram, P.; Wadden, D.; Amini, P.; Gulliver, W.; Randell, E.; Cahill, F.; Vasdev, S.; Goodridge, A.; Carter, J.C.; Zhai, G.; et al. Food addiction: Its prevalence and significant association with obesity in the general population. PLoS ONE 2013, 8, e74832. [Google Scholar] [CrossRef] [Green Version]
- Pursey, K.M.; Collins, C.E.; Stanwell, P.; Burrows, T.L. Foods and dietary profiles associated with ‘food addiction’ in young adults. Addict. Behav. Rep. 2015, 2, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulte, E.M.; Jacques-Tiura, A.J.; Gearhardt, A.N.; Naar, S. Food addiction prevalence and concurrent validity in African American adolescents with obesity. Psychol. Addict. Behav. 2018, 32, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Sengor, G.; Gezer, C. The association between food addiction, disordered eating behaviors and food intake. Rev. Nutr.-Braz. J. Nutr. 2020, 33, 10. [Google Scholar] [CrossRef] [Green Version]
- Skinner, J.A.; Garg, M.L.; Dayas, C.V.; Burrows, T.L. Is weight status associated with peripheral levels of oxytocin? A pilot study in healthy women. Physiol. Behav. 2019, 212, 112684. [Google Scholar] [CrossRef] [PubMed]
- Ben-Porat, T.; Weiss, R.; Sherf-Dagan, S.; Rottenstreich, A.; Kaluti, D.; Khalaileh, A.; Abu Gazala, M.; Zaken Ben-Anat, T.; Mintz, Y.; Sakran, N.; et al. Food Addiction and Binge Eating During One Year Following Sleeve Gastrectomy: Prevalence and Implications for Postoperative Outcomes. Obes. Surg. 2020, 31, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Lemeshow, A.R.; Rimm, E.B.; Hasin, D.S.; Gearhardt, A.N.; Flint, A.J.; Field, A.E.; Genkinger, J.M. Food and beverage consumption and food addiction among women in the Nurses’ Health Studies. Appetite 2018, 121, 186–197. [Google Scholar] [CrossRef]
- Nansel, T.R.; Lipsky, L.M.; Faith, M.; Liu, A.; Siega-Riz, A.M. The accelerator, the brake, and the terrain: Associations of reward-related eating, self-regulation, and the home food environment with diet quality during pregnancy and postpartum in the pregnancy eating attributes study (PEAS) cohort. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 149. [Google Scholar] [CrossRef]
- Westwater, M.L.; Fletcher, P.C.; Ziauddeen, H. Sugar addiction: The state of the science. Eur. J. Nutr. 2016, 55, 55–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulte, E.M.; Sonneville, K.R.; Gearhardt, A.N. Subjective experiences of highly processed food consumption in individuals with food addiction. Psychol. Addict. Behav. 2019, 33, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Schulte, E.M.; Smeal, J.K.; Gearhardt, A.N. Foods are differentially associated with subjective effect report questions of abuse liability. PLoS ONE 2017, 12, e0184220. [Google Scholar] [CrossRef] [Green Version]
- Fazzino, T.L.; Rohde, K.; Sullivan, D.K. Hyper-Palatable Foods: Development of a Quantitative Definition and Application to the US Food System Database. Obesity 2019, 27, 1761–1768. [Google Scholar] [CrossRef] [Green Version]
- Davis, C. From Passive Overeating to “Food Addiction”: A Spectrum of Compulsion and Severity. Int. Sch. Res. Not. Obes. 2013, 2013, 435027. [Google Scholar] [CrossRef]
- Vainik, U.; García-García, I.; Dagher, A. Uncontrolled eating: A unifying heritable trait linked with obesity, overeating, personality and the brain. Eur. J. Neurosci. 2019, 50, 2430–2445. [Google Scholar] [CrossRef] [Green Version]
- DePierre, J.A.; Puhl, R.M.; Luedicke, J. Public perceptions of food addiction: A comparison with alcohol and tobacco. J. Subst. Use 2014, 19, 1–6. [Google Scholar] [CrossRef]
- Lee, N.M.; Lucke, J.; Hall, W.D.; Meurk, C.; Boyle, F.M.; Carter, A. Public Views on Food Addiction and Obesity: Implications for Policy and Treatment. PLoS ONE 2013, 8, e74836. [Google Scholar] [CrossRef] [Green Version]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V.; et al. Addressing Current Criticism Regarding the Value of Self-Report Dietary Data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gearhardt, A.; White, M.; Potenza, M. Binge Eating Disorder and Food Addiction. Curr. Drug Abus. Rev. 2011, 4, 210–217. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| PICOS Criteria | Description |
|---|---|
| Population | Males and females of all ages with and without addictive eating |
| Intervention | Studies that evaluated dietary intake by FFQ, 24 h recall methods, food records or similar instruments |
| Comparators | Studies using a control group of individuals without addictive eating or no comparator |
| Outcomes | Addictive eating status; food and nutrient intakes, dietary profiles, and dietary patterns |
| Setting | All settings (observational or experimental study designs) |
| Author, Year, Country | Type of Study | Number of Participants | Population Studied | Participant Characteristics–Mean age ± SD; % Female; Mean BMI/BMIz ± SD (Range); Ethnicity | Addictive Eating Assessment Measures— Tool Used; Administration Method | Symptom Score (SS) or Diagnosis (D) Used | Dietary Outcomes Assessed | Dietary Assessment—Measure Used; Administration Method; Reporting Period; Analysis FCD(s) and/or Software; Adjustments for Misreporting |
|---|---|---|---|---|---|---|---|---|
| Ayaz [28], 2018, Turkey | Cross- sectional | 851 | Healthy adults living in Ankara aged 19–65 y | Age: 34.6 ± 12.8 y; 57.7% F; Median (min-max) BMI in NFA 23.7 kg/m2 (15.4–43.8) and in FA 26.8 kg/m2 (17.0–47.6), 9.4% underweight, 47.2% healthy weight, 27.7% overweight, 15.6% obesity; ethnicity NR | YFAS, 25-item, Turkish version; interview conducted by intern dietitian | D | Energy, macronutrients and micronutrient intake (protein, total fat, SFA, MUFA, PUFA, cholesterol, CHO, fibre, K, Ca, Mg, Fe, Zn, folic acid; Vit A, B1, B2, B12, C and E) | 24 h dietary recall; via interview with dietitian; NR; photographic atlas and BeBIS-6.1 (Nutrition Information Systems Software); misreporters excluded from analysis using Goldberg cut-offs |
| Ben Porat [41], 2020, Israel | Prospective cohort study (3, 6 and 12-month post-operative follow up) | 54(n = 54, 3, 6 and 12-month follow up) | Females with BMI ≥ 40 kg/m2 or BMI ≥ 35 kg/m2 with comorbidities presenting for sleeve gastrectomy surgery, aged 18–65 y | Age: NFA 32.9 ± 11.4 y, FA 30.8 ± 10.8 y; 100% F; BMI in NFA 44.9 ± 4.4 kg/m2 and in FA 44.9 ± 5.6 kg/m2; 100% obesity; ethnicity NR | YFAS, 25-item, Hebrew and Arab translations; NR | D + SS | Energy, protein and CHO intake (fat intake at 12-month follow-up only) | Food diary; NR; 3 days (unclear if weekend and/or week days assessed, or average of 3 days used); Zameret Israeli nutritional software; misreporting not assessed |
| Burrows [29], 2017, Australia | Cross-sectional | 1344 | Adults living in Australia aged ≥ 18–91 y | Age of 39.8 ± 13.1 y; 75.7% F; BMI 27.7 ± 9.5 kg/m2, 45.2% healthy weight, 26.0% overweight, 28.8% obesity; 2.0% indigenous | YFAS 2.0, 35-item; online survey | D + SS | Corea and non-coreb food intake | Standardised questions derived from the New South Wales Health Survey, 20-item; online survey; 7 days; N/A; misreporting not assessed |
| Filgueras [30], 2019, Brazil | Cross-sectional | 139 | Low-income school children with overweight or obesity enrolled in a longitudinal study, aged 9–11 y | Age 9.6 ± 0.7 y; 54% F; BMI z-score 1.9 ± 0.7, 56.1% overweight, 36.7% obesity, 6.6% severe obesity; ethnicity NR | YFAS-C, 25-item; paper-based survey, interviewer assisted | D + SS | Energy, macronutrient and micronutrient intake (total protein, animal protein, vegetable protein, total fat, trans fat CHO, total sugar, added sugar, fructose, fibre, Na) from total diet, unprocessed/minimally processed foods and ultra-processed foods | Brazilian FFQ, semi-quantitative, 88 items (41 ultra-processed items, 12 processed items, 35 unprocessed/minimally processed items), portion sizes estimated using a photographic manual; interviewer administered; NR; Nutrition Data System Research (NDS-R version 2014) and TACO (Brazilian FCD), NOVA for processed food classification; misreporting not assessed |
| Grammatikopolou [31], 2018, Greece | Cross- sectional | 176 | Undergraduate students from Department of Nutrition and Dietetics in Thessaloniki, Greece, aged 18–40 y | Age 21.7 ± 1.9 y; 79.5% F; BMI in non-orthorexic (n = 56) 21.5 ± 3.5 kg/m2 and in orthorexic (n = 120) 22.3 ± 2.9 kg/m2; ethnicity NR | mYFAS, 9-item; paper-based survey | D + SS | Energy, macronutrient (protein, total fat, SFA, MUFA, PUFA, trans fat, CHO, fibre) and Na intake | Food diary; online; 3 days (unclear if weekend and/or week days assessed, or average of 3 days used); ESHA’s Food Processor ® Nutrition Analysis software; nutrient intake adjusted for energy consumption using the residual method |
| Keser [32], 2015, Turkey | Cross- sectional | 100 | Children and adolescents with overweight and obesity attending a paediatric outpatient clinic, aged 10–18 y | Age: NFA 13.9 ±1.96 y, FA 14.6 ± 2.07 y; 63% F; BMI-z score in NFA 2.6 ± 1.18 (0.6–6.6) and in FA 2.6 ± 0.65 (1.0–4.1), 20% overweight (>+1 SD), 80% obesity (>+2 SD); ethnicity NR | YFAS, 25-item; NR, completed by participant not parent | D | Energy dense food/beverage intake; most addictive foods reported | FFQ (Not specified. Other details of diet intake method may be available in cited reference, however English publication unavailable); NR; NR; N/A; misreporting not assessed |
| Kucukerdonmez [33], 2017, Turkey | Cross-sectional | 104 | Adults with DSM-5 diagnosed schizophrenia, aged 20–40 y | Age: 39.4 ±10.78 y; 60.8% F; BMI 28.5 ± 6.13 kg/m2, 69.3% overweight and obesity; ethnicity NR | YFAS, 25-item; NR | D + SS | Energy and macronutrient intake (protein, fat, SFA, MUFA, PUFA, CHO, fibre) | Food record; NR; 3 days (unclear if weekend and/or week days assessed, or average of 3 days used); Nutrition Information Systems Package; misreporting not assessed |
| Lemeshow [42], 2017, USA | Prospective cohort study (Cross-sectional analyses) | 123,688 (NHS, n = 58,625; NHSII, n = 65,063) | Female nurses participating in the Nurses’ Health Study (NHS) and Nurses’ Health Study II (NHSII) | Age range 45–87 y (mean age NR); 100% F; Mean BMI NR, BMI categories (n = 122,316) 43.4% healthy weight, 31.6% overweight, 25.0% obesity; 92.6% Caucasian, 1.0% African American, 1.0% Asian, 0.9% Hispanic, 4.4% Other/Unknown | mYFAS, 9-items; NR. FA data collected in 2008 (NHS) and 2009 (NHSII). | D | Energy intake, intake of food groups (Red/processed meats, snacks, sweets and desserts, refined grains, fruits and vegetables, no/low fat snacks and sweets, no/low fat dairy, low calorie beverages, sugar sweetened beverages) and 39 positively reinforcing food items in contrast to non-reinforcing food items (identified from published research) | Semi-quantitative FFQ, 131-item; NR diet data collected in 2006 (NHS) and 2007 (NHSII); NR; Method for analysis of energy intake NR; misreporting not assessed |
| Moghaddam [34], 2019, Iran | Cross- sectional | 244 | Females with obesity attending a weight management clinic, aged 18–60 y | Age 39 ± 10 y; 100% F; Median BMI (IQR) 36.37 (30.0–78.3); ethnicity NR | YFAS, 25-item, Iranian version; NR | D | Energy and macronutrient intake (protein, fat, SFA MUFA PUFA, trans fat, CHO, sucrose) | FFQ, semi-quantitative, 147 items; interviewer administered; 12 months; USDA FCD, Nutritionist IV software; misreporting not assessed |
| Pedram [36], 2013, Canada | Cross- sectional | 652 | Third generation healthy adults living in Canadian province of Newfoundland and Labrador, aged > 19–90 y | Age: 44.3 ± 12.9 y; 63.7% F; BMI 27.4 ± 5.4 kg/m2 (17.05–54.2), 38.2% underweight/normal weight, 61.8%. overweight or obese; ethnicity NR | YFAS, 25-item; NR | D | Macronutrient intake (protein, fat, CHO, fibre) | Willett FFQ, semi-quantitative, 61 items; NR; 12 months; NutriBase Clinical Nutrition Manager software (version 9); misreporting not assessed |
| Pedram, 2015 [35], Canada | Cross- sectional (subsample analysis of Pedram, 2013) | 58 | Adults with overweight and obesity with YFAS defined food addiction, and non–food addicted matched controls, aged > 19 y | Age NFA 42 ± 8.9 y, FA 42.5 ± 9.4 y; 82.8% F; BMI in NFA 32 ± 4.42 kg/m2 and in FA 32.5 ± 6 kg/m2; ethnicity NR | YFAS, 25-item; NR | D | Energy, macronutrient and micronutrient intake (protein, total fat, SFA, MUFA, PUFA, trans fat, CHO, sugar, omega 3 and 6, Na, K, Ca, Se; vitamins B1, D, E and K) | Willett FFQ, semi-quantitative, 61 items; NR; 12 months; NutriBase Clinical Nutrition Manager software (version 9); misreporting not assessed |
| Pursey [37], 2015, Australia | Cross- sectional | 462 | Adults living in Australia aged 18–35 y | Age 25.1 ± 4.0 y; 86.0% F; BMI: 23.2 ± 4.5 kg/m2 (15.9–54.0), 5.4% underweight, 72.9% healthy weight, 13.9% overweight, 7.8% obesity; ethnicity NR | YFAS, 25-item; online survey | D + SS | Energy, macronutrient and micronutrient intake (protein, total fat, SFA, MUFA, PUFA, cholesterol, CHO, sugars, fibre, alcohol, folate, Na, K, Mg. Ca, P, Fe, Zn; vitamins A, B1, B2, B3, and C); energy from food groups (vegetables, fruit, meat, grains, dairy, sweet drink, savoury packaged snacks, candy, baked sweet products, take-out, breakfast cereal); energy from core a and non-core foods b; diet quality score | Australian Eating Survey FFQ semi-quantitative, 120 items, and Australian Recommended Food Score (ARFS) derived from subset of 70 items (scores range from 0–73, higher scores reflect overall higher nutritional quality of usual eating pattern); online survey; 6 months; AUSNUT Australian FCD |
| Schulte [38], 2018, USA | Intervention study (baseline data reported) | 181 | Adolescents with obesity participating in weight management program, 12–16 y | Age 13.75 ± 1.35 y; 67% F; BMI: 38.2 ± 7.5 kg/m2 (25.7–60.5); 100% African American | YFAS-C, 25-item; paper-based form, completed by participant not parent | D + SS | Energy, total fat, SFA, trans fat, CHO, total sugar and added sugar intake | The Block Kids FFQ; paper-based form; one week; NutritionQuest assessment and analysis service |
| Sengor [39], 2020, Turkey | Cross- sectional | 370 | University students aged 18–25 y | Age 18–25 years (mean age NR); 56.8% F; BMI NR; ethnicity NR | YFAS, 25-item. Turkish version; via interview | D + SS | Energy, macronutrient and micronutrient intake (protein, fat, cholesterol, CHO and fibre, K, Ca, Mg, P, Fe, Zn, folic acid; and vitamins A, B1, B2, B3, B6, B12, C and E); and intake of food items/groups (milk and dairy products; bread and grains; oily seeds; meat and egg; sausage; vegetables; potato, starch and mushroom; fruits; sweets; cakes, cookies and biscuits; oil and fat) | FFQ (not specified), 54 food items, Turkish adaptation; paper-based form; one month; BeBIS-7.2 (Nutrition Information Systems Software) |
| Skinner [40], 2019, Australia | RCT (baseline data reported) | 18 | Healthy females aged 18–85 y | Age 43.0 ± 16.5 y; 100.0% F; BMI in NFA 25.64 ± 2.84 kg/m2 (21.22–29.97) and in FA 33.55 ± 6.02 kg/m2 (25.66–41.48), 33.3% healthy weight, 50.0% overweight, 16.7% obesity; ethnicity NR | YFAS 2.0, 35-item; online survey | D + SS | Energy from core a and non-core b foods, diet quality score | Australian Eating Survey FFQ semi-quantitative, 120 items, and Australian Recommended Food Score (ARFS) derived from subset of 70 items (scores range from 0–73, higher scores reflect overall higher nutritional quality of usual eating pattern); online survey; 6 months; AUSNUT Australian FCD |
| Author, Year, Country | Prevalence of FA by Diagnosis | YFAS Symptoms Mean ± SD (Range or 95% CI) | Relationship/Association between YFAS and Diet | Study Limitations |
|---|---|---|---|---|
| Ayaz [28], 2018, Turkey | 11.4% | NR | Significantly higher daily intakes of energy, protein and fat, SFA, PUFA, MUFA, cholesterol Vitamin A, Vitamin E, Vitamin B12, Mg, Fe, Zn in females with FA compared to NFA. No significant difference in energy, macronutrient or micronutrient intakes in males with FA compared to NFA. | Predominantly younger adults 19–39 y |
| Ben Porat [41], 2020, Israel | 40.7% | Median and IQR NFA = 2.0 (1.0, 3.0) FA = 5.5 (4.0, 7.0) | No significant differences in daily intakes of energy, protein or CHO intake between FA and NFA at each follow-up timepoint, according to baseline FA diagnosis. Prevalence of FA decreased from baseline to 29.3% at 12-month post-surgery. In those with a FA diagnosis at 12-month post-surgery, significantly higher daily intake of CHO, compared to NFA. No significant difference in protein and fat intakes. | Specific population of adults undergoing bariatric surgery. Fat intake not reported according to baseline FA diagnosis. |
| Burrows [29], 2017, Australia | 22.2% (FA severity: 3.1% Mild, 11.8% Moderate, 85.1% Severe) | 8.1 ± 2.6 (baseline) | FA reported higher intakes of confectionary, fast food, snack foods, hot chips, potato crisps, soft drinks and lower intakes of core foods a, such as fruits and vegetables, compared to NFA. FA were less likely to consume breakfast every day. FA who ate confectionaries daily or 5–6 times per week had 2.4 times the odds of severe FA, while those who ate confectionaries two or more times a day had 7.1 times the odds of severe FA. Vegetable intake reduced the likelihood of severe FA, with each extra unit of vegetable consumption decreasing the odds by a factor of 0.8. | Predominantly younger adults 18–54 y. Predominantly female sample. |
| Filgueras [30], 2019, Brazil | 24.0% | 3.0 (95% CI: 3.1 to 3.8) | Significantly lower daily intake of fibre, and higher daily intakes of protein (total, vegetable and animal), fat (total and trans fat), CHO, sugar (total, added and fructose) and sodium in FA compared NFA. Significantly higher daily energy, macronutrient and micronutrient intakes from ultra-processed foods in FA compared to NFA. No significant difference in daily energy, macronutrient and micronutrient intakes from unprocessed/minimally processed foods in FA compared to NFA. Ultra-processed foods positively associated with FA were cookies/biscuits and sausages. | Children are participating in a school-based intervention, and it is not clear if FA or dietary intake was measured at baseline or during the intervention. |
| Grammatikopolou [31], 2018, Greece | 4.5% | 1.4 ± 1.0 | No significant difference in energy, macronutrient or micronutrient intakes between FA and NFA. | Specific population of nutrition and dietetic students, may have been motivated by health; predominantly female, small number of FA |
| Keser [32], 2015, Turkey | 71.0% | NR | Foods high in CHO and fats perceived to be the most addictive. Consumption of French fries ≥ 1–2 times per week associated with a 2.3-fold increase in FA risk. | Unclear if validated FFQ used. Intake patterns for NFA not reported and difference in mean intakes between FA and NFA not assessed. |
| Kucukerdonmez [33], 2017, Turkey | 60.6% | 3.5 ± 1.7 | Significantly higher daily intakes of energy, CHO, fibre, total fat and PUFA in FA compared to NFA. | Specific population of adults with schizophrenia |
| Lemeshow [42], 2017, USA | 2.5% and 8.0% | NR | FA was associated with higher intakes of foods hypothesised to be positively reinforcing (i.e., foods containing high amounts of refined CHO and fat) such as fast foods, snacks, desserts, fast food and candy. Odds of FA were strongest among those consuming 5+ servings/week (compared with <1 serving/month) of hamburgers, French fries and pizza. Consumption of red/processed meat, low/no fat snacks/desserts, and low-calorie beverages was positively associated with FA. Consumption of refined grains, sugar-sweetened beverages and fruit and vegetables was inversely associated with FA. | Female nurses, predominantly Caucasian, and all >45 y |
| Moghaddam [34], 2019, Iran | 27.9% | NR | Significantly higher intakes of energy, protein, CHO, total fat, SFA, MUFA, PUFA and cholesterol in FA compared to NFA. No significant difference in intakes of sucrose and trans fat between FA and NFA. | Specific population of females with obesity attending a weight management clinic |
| Pedram [36], 2013, Canada | 5.4% | NR | Significant higher percent energy from protein and fat in FA compared to NFA. No significant difference in intakes of protein, CHO and fat when expressed as gram per kg of body weight. | Predominantly female, few nutrients assessed |
| Pedram [35], 2015, Canada | 50.0% | NR | Significantly higher percent energy from fat in FA compared to NFA. When expressed as gram per kg of body weight, FA had significantly higher intakes of energy, CHO, dietary sugar, fat, SFA, trans fat, MUFA, PUFA, omega 3, omega 6, Na, P, Ca, Se, vitamin B1, vitamin D, gamma-tocopherol and dihydrophylloquinone compared to NFA. | Small sample, predominantly female |
| Pursey [37], 2015, Australia | 14.7% | 2.4 ± 1.8 | Higher YFAS scores associated with higher intakes of energy-dense, nutrient-poor foods (candy, take out and baked sweet products) and lower intakes of nutrient-dense core foods a (whole-grain products and breakfast cereals). Higher intakes of total fat and MUFA, and lower intakes of wholegrain foods in FA compared to NFA. Odds of FA diagnosis increased with higher intakes of fat and MUFA. Odds of FA diagnosis decreased with higher intakes of wholegrain foods. | Predominantly female, and well-educated, sample |
| Schulte [38], 2018, USA | 9.9% | 2.11 ± 1.75 | Significantly higher intakes of energy, total fat, trans fat, total CHO, total sugar, and added sugar in FA compared to NFA. Significant positive associations between YFAS-C scores and total calories, fat, SFA, trans fat, total CHO, total sugar, and added sugar. | All African American sample; short reporting duration of dietary intake. |
| Sengor [39], 2020, Turkey | 21.1% | NR | Higher YFAS scores associated with higher intakes of energy, CHO and fat in males and females. Females with FA had higher daily intakes of energy, CHO and fat; and lower intakes of Vit C. No difference in energy, macro- and micronutrient intakes between males with and without FA. Females with FA consumed greater amounts of meat and egg; sausage; and cakes, cookies and biscuits per day compared to females without FA; and males with FA consumed greater amounts of oily seeds; oil and fat; lower amounts of cakes, cookies and biscuits per day compared to males without FA. | Mean age and weight status not reported. Unclear if validated FFQ used. |
| Skinner [40], 2019, Australia | 33.3% | 1.1 ± 1.2 | Significantly lower intakes of core a foods and higher intakes of non-core b foods in FA compared to NFA. No significant difference in diet quality score between FA and NFA. | Small sample, females only, large age range. Significant difference in BMI between FA and NFA groups. Subgroups of core and non-core foods not reported. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pursey, K.M.; Skinner, J.; Leary, M.; Burrows, T. The Relationship between Addictive Eating and Dietary Intake: A Systematic Review. Nutrients 2022, 14, 164. https://doi.org/10.3390/nu14010164
Pursey KM, Skinner J, Leary M, Burrows T. The Relationship between Addictive Eating and Dietary Intake: A Systematic Review. Nutrients. 2022; 14(1):164. https://doi.org/10.3390/nu14010164
Chicago/Turabian StylePursey, Kirrilly M., Janelle Skinner, Mark Leary, and Tracy Burrows. 2022. "The Relationship between Addictive Eating and Dietary Intake: A Systematic Review" Nutrients 14, no. 1: 164. https://doi.org/10.3390/nu14010164
APA StylePursey, K. M., Skinner, J., Leary, M., & Burrows, T. (2022). The Relationship between Addictive Eating and Dietary Intake: A Systematic Review. Nutrients, 14(1), 164. https://doi.org/10.3390/nu14010164