
Nitrogen Balance after the Administration of a Prolonged-Release Protein Substitute for Phenylketonuria as a Single Dose in Healthy Volunteers



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Blood AA and Nitrogen Concentrations
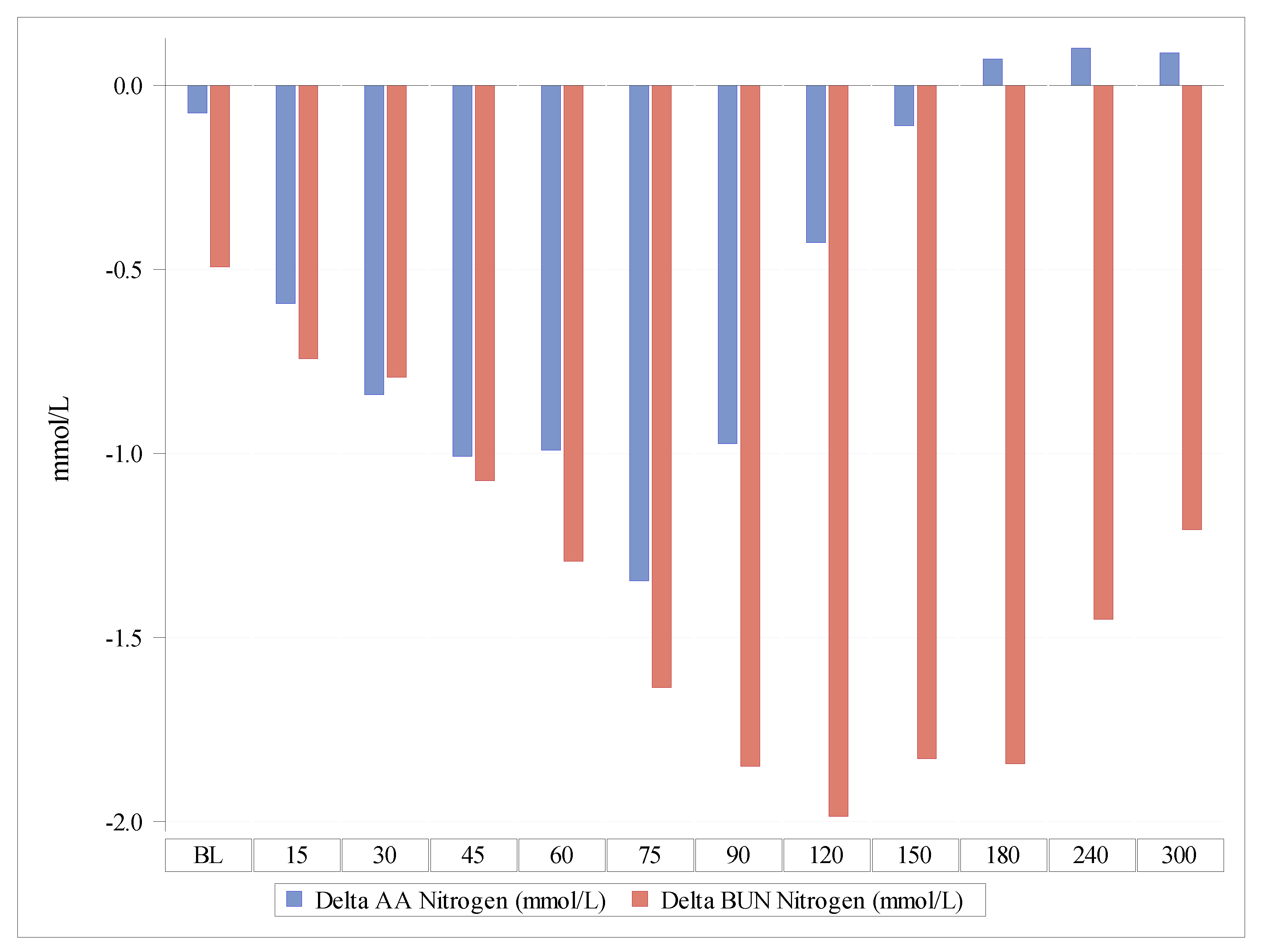
3.2. BUN and Nitrogen Concentrations
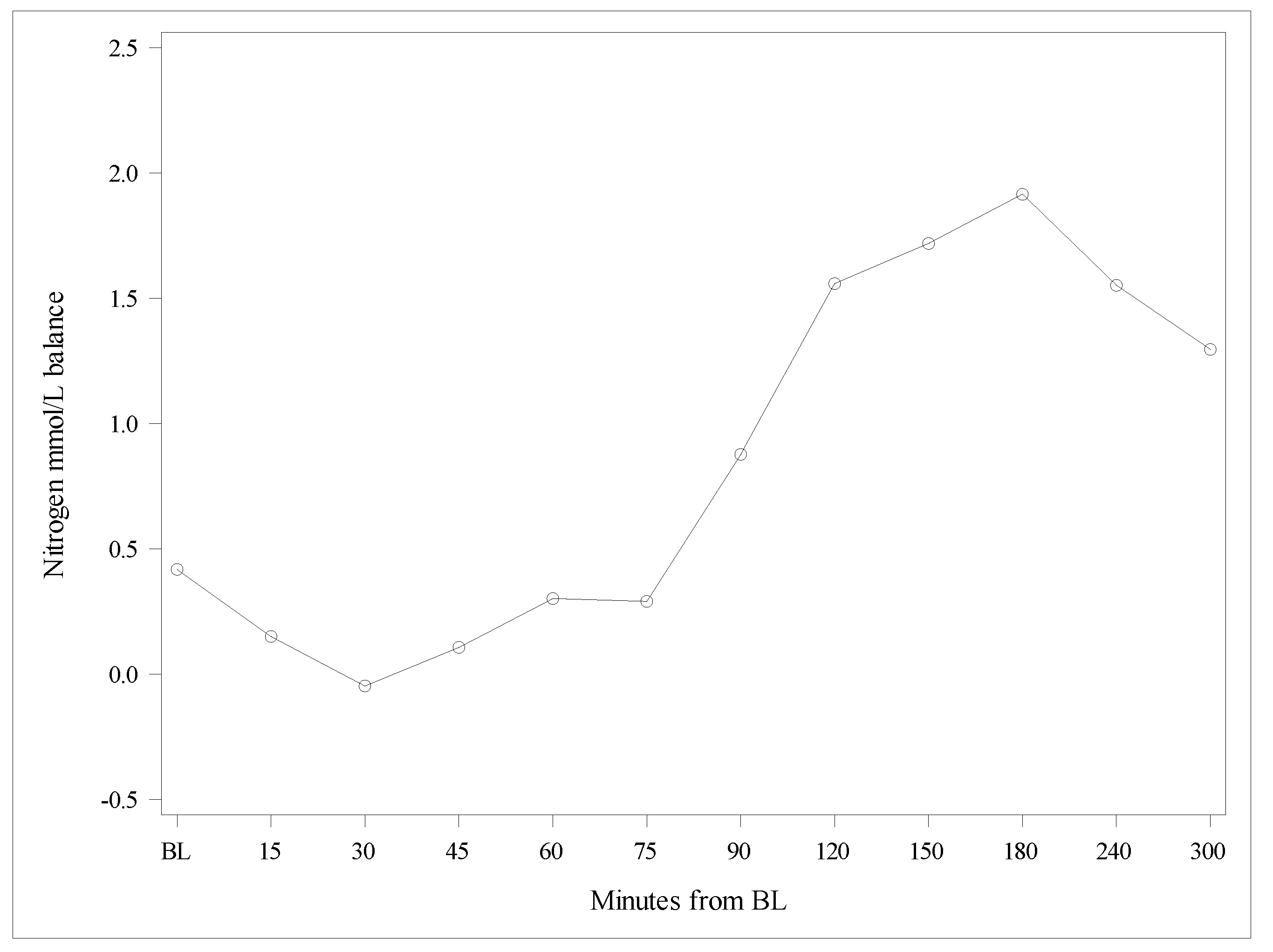
3.3. Balance between Nitrogen Concentrations from AA Administration in Blood and BUN
3.4. Total Quantities of Nitrogen from the AUC0–300 Contained in AAs and in BUN
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Shoraka, H.R.; Haghdoost, A.A.; Baneshi, M.R.; Bagherinezhad, Z.; Zolala, F. Global prevalence of classic phenylketonuria based on Neonatal Screening Program Data: Systematic review and meta-analysis. Clin. Exp. Pediatr. 2020, 63, 34–43. [Google Scholar] [CrossRef]
- Ilgaz, F.; Pinto, A.; Gokmen-Ozel, H.; Rocha, J.C.; van Dam, E.; Ahring, K.; Belanger-Quintana, A.; Dokoupil, K.; Karabulut, E.; MacDonald, A. Long-Term Growth in Phenylketonuria: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 2070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hood, A.; Grange, D.K.; Christ, S.E.; Steiner, R.; White, D.A. Variability in phenylalanine control predicts IQ and executive abilities in children with phenylketonuria. Mol. Genet. Metab. 2014, 111, 445–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeRoche, K.; Welsh, M. Twenty-five years of research on neurocognitive outcomes in early-treated phenylketonuria: Intelligence and executive function. Dev. Neuropsychol. 2008, 33, 474–504. [Google Scholar] [CrossRef] [PubMed]
- Al Hafid, N.; Christodoulou, J. Phenylketonuria: A review of current and future treatments. Transl. Pediatr. 2015, 4, 304–317. [Google Scholar]
- Simon, E.; Schwarz, M.; Roos, J.; Dragano, N.; Geraedts, M.; Siegrist, J.; Kamp, G.; Wendel, U. Evaluation of quality of life and description of the sociodemographic state in adolescent and young adult patients with phenylketonuria (PKU). Health Qual. Life Outcomes 2008, 6, 25. [Google Scholar] [CrossRef] [Green Version]
- Daly, A.; Evans, S.; Chahal, S.; Santra, S.; Pinto, A.; Gingell, C.; Rocha, J.C.; van Spronsen, F.; Jackson, R.; MacDonald, A. The Effect of Glycomacropeptide versus Amino Acids on Phenylalanine and Tyrosine Variability over 24 Hours in Children with PKU: A Randomized Controlled Trial. Nutrients 2019, 11, 520. [Google Scholar] [CrossRef] [Green Version]
- Evans, S.; Ford, S.; Adam, S.; Adams, S.; Ash, J.; Ashmore, C.; Caine, G.; Carruthers, R.; Cawtherley, S.; Chahal, S.; et al. Development of national consensus statements on food labelling interpretation and protein allocation in a low phenylalanine diet for PKU. Orphanet J. Rare Dis. 2019, 14, 2. [Google Scholar] [CrossRef]
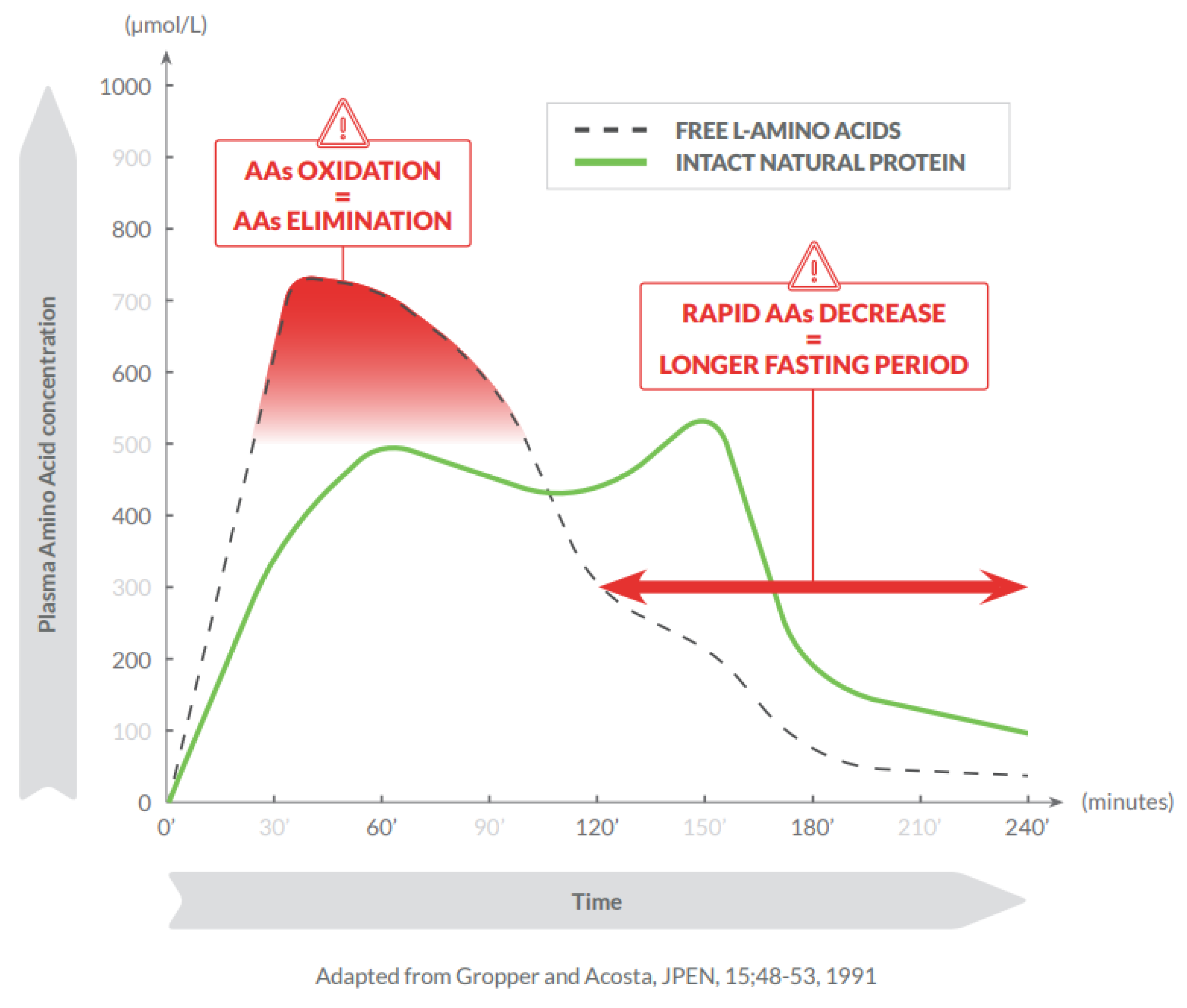
- Gropper, S.S.; Acosta, P.B. Effect of simultaneous ingestion of L-amino acids and whole protein on plasma amino acid and urea nitrogen concentrations in humans. J. Parenter. Enter. Nutr. 1991, 15, 48–53. [Google Scholar] [CrossRef]
- Pasini, E.; Corsetti, G.; Aquilani, R.; Romano, C.; Picca, A.; Calvani, R.; Dioguardi, F.S. Protein-Amino Acid Metabolism Disarrangements: The Hidden Enemy of Chronic Age-Related Conditions. Nutrients 2018, 10, 391. [Google Scholar] [CrossRef] [Green Version]
- Rafoth, R.J.; Onstad, G.R. Urea synthesis after oral protein ingestion in man. J. Clin. Investig. 1975, 56, 1170–1174. [Google Scholar] [CrossRef]
- Mönch, E.; Herrmann, M.; Brösicke, H.; Schöffer, A.; Keller, M. Utilisation of amino acid mixtures in adolescents with phenylketonuria. Eur. J. Pediatr. 1996, 155, S115–S120. [Google Scholar] [CrossRef] [PubMed]
- Boirie, Y.; Dangin, M.; Gachon, P.; Vasson, M.-P.; Maubois, J.-L.; Beaufrère, B. Slow and fast dietary proteins differently modulate postprandial protein accretion. Proc. Natl. Acad. Sci. USA 1997, 94, 14930–14935. [Google Scholar] [CrossRef] [Green Version]
- Herrmann, M.-E.; Brösicke, H.; Keller, M.; Monch, E.; Helge, H. Dependence of the utilization of a phenylalanine-free amino acid mixture on different amounts of single dose ingested. A case report. Eur. J. Pediatr. 1994, 153, 501–503. [Google Scholar] [CrossRef]
- Groschl, M.; Knerr, I.; Topf, H.; Schmid, P.; Rascher, W.; Rauh, M. Endocrine responses to the oral ingestion of a physiological dose of essential amino acids in humans. J. Endocrinol. 2003, 179, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Weigel, C.; Rauh, M.; Kiener, C.; Rascher, W.; Knerr, I. Effects of various dietary amino acid preparations for phenylketonuric patients on the metabolic profiles along with postprandial insulin and ghrelin responses. Ann. Nutr. Metab. 2007, 51, 352–358. [Google Scholar] [CrossRef] [Green Version]
- Giarratana, N.; Gallina, G.; Panzeri, V.; Frangi, A.; Canobbio, A.; Reiner, G. A new Phe-free protein substitute engineered to allow a physiological absorption of free amino acids for phenylketonuria. J. Inborn Errors Metab. 2018, 6, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Scheinin, M.; Barassi, A.; Junnila, J.; Lovro, Z.; Reiner, G.; Sarkkinen, E.; MacDonald, A. Amino Acid Plasma Profiles from a Prolonged-Release Protein Substitute for Phenylketonuria: A Randomized, Single-Dose, Four-Way Crossover Trial in Healthy Volunteers. Nutrients 2020, 12, 1653. [Google Scholar] [CrossRef]
- Brown, C.S.; Lichter-Konecki, U. Phenylketonuria (PKU): A problem solved? Mol. Genet. Metab. Rep. 2016, 6, 8–12. [Google Scholar] [CrossRef]
- Walter, J.H.; White, F.J. Blood phenylalanine control in adolescents with phenylketonuria. Int. J. Adolesc. Med. Health 2004, 16, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Walter, J.H.; White, F.J.; Hall, S.K.; MacDonald, A.; Rylance, G.; Boneh, A.; Francis, D.E.; Shortland, G.J.; Schmidt, M.; Vail, A. How practical are recommendations for dietary control in phenylketonuria? Lancet 2002, 360, 55–57. [Google Scholar] [CrossRef]
- Rohde, C.; von Teeffelen-Heithoff, A.; Thiele, A.G.; Arelin, M.; Mutze, U.; Kiener, C.; Gerloff, J.; Baerwald, C.; Schultz, S.; Heller, C.; et al. PKU patients on a relaxed diet may be at risk for micronutrient deficiencies. Eur. J. Clin. Nutr. 2014, 68, 119–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, B.; Bremer, H.J. Nutrient intake and food consumption of adolescents and young adults with phenylketonuria. Acta Paediatr. 1995, 84, 743–748. [Google Scholar] [CrossRef]
- Walter, J.H. Vitamin B12 deficiency and phenylketonuria. Mol. Genet. Metab. 2011, 104, S52–S54. [Google Scholar] [CrossRef]
- MacDonald, A.; Rylance, G.; Davies, P.; Asplin, D.; Hall, S.K.; Booth, I.W. Administration of protein substitute and quality of control in phenylketonuria: A randomized study. J. Inherit. Metab. Dis. 2003, 26, 319–326. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | Test Product (AA, mmol/L) Mean (SD) | Reference Product (AA, mmol/L) Mean (SD) | Delta + AA Test vs. Reference (mmol/L) Mean (SD) | Delta ‡ Nitrogen Test vs. Reference (mmol/L) Mean (SD) |
|---|---|---|---|---|
| Baseline * | 2.30 (0.30) | 2.34 (0.26) | −0.05 (0.31) | −0.08 (0.43) |
| 15 min | 2.52 (0.33) | 3.00 (0.46) | −0.43 (0.44) | −0.59 (0.60) |
| 30 min | 3.05 (0.44) | 3.76 (0.59) | −0.65 (0.55) | −0.84 (0.72) |
| 45 min | 3.33 (0.48) | 4.18 (0.61) | −0.80 (0.56) | −1.01 (0.76) |
| 60 min | 3.43 (0.48) | 4.21 (0.54) | −0.80 (0.41) | −0.99 (0.58) |
| 75 min | 3.33 (0.48) | 4.37 (0.64) | −1.06 (0.60) | −1.35 (0.82) |
| 90 min | 3.22 (0.44) | 3.95 (0.55) | −0.77 (0.58) | −0.97 (0.81) |
| 120 min | 3.02 (0.43) | 3.33 (0.37) | −0.35 (0.53) | −0.43 (0.73) |
| 150 min | 2.82 (0.38) | 2.90 (0.31) | −0.10 (0.42) | −0.11 (0.58) |
| 180 min | 2.67 (0.38) | 2.59 (0.26) | 0.06 (0.35) | 0.07 (0.49) |
| 240 min | 2.48 (0.30) | 2.40 (0.24) | 0.08 (0.33) | 0.10 (0.48) |
| 300 min | 2.33 (0.29) | 2.26 (0.23) | 0.07 (0.29) | 0.09 (0.40) |
| Concentration BUN (mmol/L) | ||||
|---|---|---|---|---|
| Time | Test Product Mean (SD) | Reference Product Mean (SD) | Delta BUN * (mmol/L) Mean (SD) | Delta Nitrogen ** (mmol/L) Mean (SD) |
| Baseline | 3.89 (0.72) | 4.08 (0.87) | −0.25 (0.56) | −0.49 (1.12) |
| 15 min | 3.82 (0.68) | 4.16 (0.86) | −0.37 (0.56) | −0.74 (1.11) |
| 30 min | 3.94 (0.69) | 4.30 (0.86) | −0.40 (0.86) | −0.79 (1.72) |
| 45 min | 4.04 (0.75) | 4.57 (0.95) | −0.54 (0.58) | −1.07 (1.16) |
| 60 min | 4.15 (0.73) | 4.77 (0.93) | −0.65 (0.57) | −1.29 (1.14) |
| 75 min | 4.28 (0.66) | 5.08 (0.92) | −0.82 (0.58) | −1.64 (1.15) |
| 90 min | 4.37 (0.66) | 5.26 (0.92) | −0.93 (0.65) | −1.85 (1.31) |
| 120 min | 4.50 (0.63) | 5.47 (0.93) | −0.99 (0.62) | −1.99 (1.24) |
| 150 min | 4.58 (0.62) | 5.45 (0.89) | −0.91 (0.65) | −1.83 (1.29) |
| 180 min | 4.55 (0.66) | 5.45 (0.89) | −0.92 (0.76) | −1.84 (1.51) |
| 240 min | 4.58 (0.64) | 5.26 (0.89) | −0.73 (0.64) | −1.45 (1.28) |
| 300 min | 4.53 (0.63) | 5.10 (0.82) | −0.60 (0.63) | −1.21 (1.24) |
| Time | Delta Nitrogen in AAs (mmol/L) Mean (SD) | Delta Nitrogen in BUN (mmol/L) Mean (SD) | Delta Nitrogen in AAs Minus Delta Nitrogen in BUN (mmol/L) Mean (SD) |
|---|---|---|---|
| Baseline | −0.08 (0.43) | −0.49 (1.12) | 0.42 (1.07) |
| 15 min | −0.59 (0.60) | −0.74 (1.11) | 0.15 (0.93) |
| 30 min | −0.84 (0.72) | −0.79 (1.72) | −0.05 (1.66) |
| 45 min | −1.01 (0.76) | −1.07 (1.16) | 0.11 (1.23) |
| 60 min | −0.99 (0.58) | −1.29 (1.14) | 0.30 (1.26) |
| 75 min | −1.35 (0.82) | −1.64 (1.15) | 0.29 (1.27) |
| 90 min | −0.97 (0.81) | −1.85 (1.31) | 0.88 (1.39) |
| 120 min | −0.43 (0.73) | −1.99 (1.24) | 1.56 (1.43) |
| 150 min | −0.11 (0.58) | −1.83 (1.29) | 1.72 (1.35) |
| 180 min | 0.07 (0.49) | −1.84 (1.51) | 1.92 (1.55) |
| 240 min | 0.10 (0.48) | −1.45 (1.28) | 1.55 (1.28) |
| 300 min | 0.09 (0.40) | −1.21 (1.25) | 1.30 (1.24) |
| Mean AAs AUC0–300 (mol/L/300 min) Mean (SD) | Quantity of Nitrogen (mol/L/300 min) Mean (SD) | |
|---|---|---|
| Reference product | 0.9146 (0.075) | 1.302 (0.100) |
| Test product | 0.8391 (0.099) | 1.209 (0.140) |
| Difference Test–Reference | −0.078 (0.096) | −0.098 (0.135) |
| Mean BUN AUC0–300 min (mol/L/300 min) Mean (SD) | Quantity of Nitrogen (mol/L/300 min) Mean (SD) | |
|---|---|---|
| Reference product | 1.5729 (0.266) | 3.146 (0.532) |
| Test product | 1.3574 (0.201) | 2.715 (0.402) |
| Difference Test–Reference | −0.226 (0.187) | −0.452 (0.375) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scheinin, M.; Junnila, J.; Reiner, G.; MacDonald, A.; Muntau, A.C. Nitrogen Balance after the Administration of a Prolonged-Release Protein Substitute for Phenylketonuria as a Single Dose in Healthy Volunteers. Nutrients 2021, 13, 3189. https://doi.org/10.3390/nu13093189
Scheinin M, Junnila J, Reiner G, MacDonald A, Muntau AC. Nitrogen Balance after the Administration of a Prolonged-Release Protein Substitute for Phenylketonuria as a Single Dose in Healthy Volunteers. Nutrients. 2021; 13(9):3189. https://doi.org/10.3390/nu13093189
Chicago/Turabian StyleScheinin, Mika, Jouni Junnila, Giorgio Reiner, Anita MacDonald, and Ania C. Muntau. 2021. "Nitrogen Balance after the Administration of a Prolonged-Release Protein Substitute for Phenylketonuria as a Single Dose in Healthy Volunteers" Nutrients 13, no. 9: 3189. https://doi.org/10.3390/nu13093189
APA StyleScheinin, M., Junnila, J., Reiner, G., MacDonald, A., & Muntau, A. C. (2021). Nitrogen Balance after the Administration of a Prolonged-Release Protein Substitute for Phenylketonuria as a Single Dose in Healthy Volunteers. Nutrients, 13(9), 3189. https://doi.org/10.3390/nu13093189