Abstract
Context-appropriate nutrition education interventions targeting middle school students have the potential to promote healthy dietary patters that may help prevent unnecessary weight gain at a point in childhood development when youth experience increasing agency over their food choices. The aim of this review was to identify and synthesize themes in train-the-trainer approaches, intervention content and delivery, and youth receptivity across teacher, mentor, and peer-led nutrition education interventions that targeted middle school-age youth in urban, primarily low-income settings. A systematic, electronic literature search was conducted in seven electronic databases, PubMed/Medline, CINAHL, ERIC, PsycINFO, Scopus, SPORTDiscus, and Cochrane CENTRAL, using fixed inclusion and exclusion criteria. A total of 53 papers representing 39 unique interventions were selected for data extraction and quality assessment. A framework synthesis approach was used to organize the interventions into six categories and identify themes according to whether the intervention was classroom-based or out-of-school-based and whether adults, cross-age peers or same-age peers delivered the intervention. Ten of the interventions contained multiple components such that they were included in two of the categories. The review findings indicated that trainings should be interactive, include opportunities to role-play intervention scenarios and provide follow-up support throughout intervention delivery. Interventions targeting middle school youth should include positive messaging and empower youth to make healthy choices within their specific food environment context.
1. Introduction
The prevalence of childhood obesity in the United States is a major public health concern, particularly because obesity in youth often persists into adulthood and is associated with multiple chronic diseases, increased health care costs, and diminished quality of life [1,2]. Obesity prevalence is significantly higher among non-Hispanic black and Hispanic youth compared with non-Hispanic white and non-Hispanic Asian youth [3], and obesity prevalence tends to be higher in youth from households with lower head-of-household education levels and incomes [4]. Regular physical activity and healthy eating patterns are both important habits for obesity prevention, yet the vast majority of U.S. youth do not meet physical activity or fruit, vegetable, and water intake recommendations [5,6,7]. Historically under-resourced, urban neighborhoods in the U.S. have high concentrations of the populations identified as being at greatest risk for childhood obesity, and structural inequities in the built and food environments in these communities can make healthy choices even more difficult. Accordingly, obesity prevention interventions that target the physical activity and nutrition habits of at-risk youth have the potential to improve health outcomes in these communities for years to come.
Previous reviews that have examined the effectiveness of nutrition education interventions targeting youth, primarily in school-based settings, suggest the following components are important for successful interventions: behaviorally focused education, use of theoretical methods (e.g., skill building, self-assessment, social support, etc.), adequate dosage, and thorough training for those delivering the intervention [8,9,10,11,12]. Despite evidence for the importance of training and a reliance on those outside the nutrition profession—from classroom teachers to out-of-school program volunteers to older student peers—to deliver intervention programming, there is a lack of information on the most effective training methods for those delivering nutrition education interventions (e.g., training-the-trainer models). Furthermore, most reviews have lumped middle school age students with either elementary or high school students, rather than focusing specifically on strategies for targeting this age group as they are transitioning to adolescence and gaining increased agency over their food choices. The purpose of this review, therefore, was to build a larger evidence base for early adolescent nutrition education programs by identifying and synthesizing themes in training approaches, intervention content and delivery, and youth receptivity across teacher, mentor, and peer-led nutrition education interventions that targeted middle school-age youth in urban, primarily low-income settings.
2. Methods
This systematic review was conducted in accordance with the criteria set forth in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [13]. While we searched the International prospective register of systematic reviews (PROSPERO) to ensure we were not duplicating a similar review, we did not register our protocol due to time constraints for finalizing our review and COVID-19 related processing delays at the time our protocol was developed. Primary research articles, protocol papers, and process evaluation papers were identified by searching PubMed/Medline, CINAHL, ERIC, PsycINFO, Scopus, SPORTDiscus, and Cochrane CENTRAL. The search strategy was developed by the research team and reviewed by a research librarian prior to initiation. An example of the search term strategy is provided in Supplementary Material Figure S1. The search was conducted in May 2020 and limited to English language results published between 2005 and 2020. The search was limited to results published in 2005 and later because it was in the middle part of the 2000s when the literature began to expand beyond raising the alarm about childhood obesity to the implementation and evaluation of health promotion interventions aimed at obesity prevention.
2.1. Inclusion and Exclusion Criteria
Given that our review question sought to identify and synthesize themes across the content and protocols of various nutrition interventions, we defined our inclusion criteria using the following PICo tool (Population, Interest, Context): Population targeted in the intervention should include at least part of the 10–14-year-old age range and should not be focused on youth with eating disorders or other specific nutrition needs related to a medical condition. Interest was interventions that were (1) nutrition, diet, or food-related and (2) included a description of the process for training those delivering the intervention or for training youth within the target population to deliver nutrition content to others. Context for the interventions were an urban school or community-based setting, either in the U.S. or in a setting comparable to a U.S. urban environment. Home-based interventions were excluded.
Qualitative studies related to the development or evaluation of an intervention were included if they described participatory research with youth from the target population or if interview subjects were those participating in or delivering the intervention and if there was at least one accompanying paper describing results of the intervention.
Given the challenges of following the same students consistently over a prolonged period of time in interventions that occur outside the classroom, papers were excluded if the intervention content was scaffolded and delivered over more than one academic year. Cross-sectional studies, review articles, book chapters, and poster abstracts were also excluded.
2.2. Secreening and Selection Process
Search results were uploaded to the Covidence online systematic review tool (Covidence, Melbourne, Australia), where duplicates were automatically removed by the review tool. A screening team consisting of four members worked in pairs so that two people independently screened the titles and abstracts of all articles identified through the search process and voted on inclusion or exclusion according to the criteria in the above section. The same process was followed in the full-text screening stage so that all papers were independently read and voted on for inclusion or exclusion by two screeners. At both stages, conflicts between screening team member votes were resolved by the first author. Two additional papers were added to the full-text review after the clinical trial registry for the study was identified through the systematic search process. Where multiple papers existed for the same intervention, all were included if the intervention met the inclusion criteria. Five additional papers were identified during the full-text stage that pertained to included interventions and were used in the data extraction stage.
2.3. Data Extraction and Synthesis Approach
Our focus on qualitative aspects of nutrition education interventions—namely train-the-trainer process and design, intervention content and delivery, and youth receptivity—led us to examine qualitative and mixed-methods approaches to synthesizing results. We sought to examine a wide variety of interventions—from those with a full nutrition education curriculum as in a classroom or a structured after-school program, to interventions that trained same-age peers to have informal conversations about nutrition, as well as scenarios in-between such as out-of-school settings led by community volunteers or young adult near-peers. We therefore set the inclusion criteria to allow for a diversity of methods, believing important themes would emerge among different types of interventions that would aid in developing new nutrition education programs with a robust training component. Based on our scoping searches, nutrition intervention expertise within the research team, and a review of qualitative synthesis methods, we selected a framework synthesis approach [14,15,16]. Framework synthesis is an application of the ‘framework analysis’ method used in primary research to systematic reviews [14]. It provides an a priori scaffold for organizing and mapping data from included studies, while permitting flexibility to iterate as the data is integrated into the framework [17].
In order to describe the elements of the nutrition education interventions identified through our search process consistently, we developed an analytical framework for grouping similar settings and training audiences, and then identified commonalities within each group. We wanted to examine classroom-based and extracurricular interventions separately to compare and contrast approaches in each of these settings. We also differentiated between populations trained to deliver the intervention to determine whether training approaches, intervention design or youth receptivity varied depending on whether adults, cross-age or near peers (older than target population but under age 23), or same-age peers delivered the intervention (see Table 1 below).

Table 1.
Framework for categorizing nutrition education interventions.
Once the categories A–F described above were identified, we organized the themes within each subgroup according to the following dimensions, driven by our review purpose stated previously: (1) train-the-trainer approaches, including number and duration of sessions and follow-up or support during the intervention; (2) common nutrition topics covered across the interventions; (3) format and delivery of the interventions, (4) youth receptivity, feedback, and outcomes measured; and (5) feedback and outcomes from those delivering the intervention, if assessed. All four members of the screening team extracted data independently and systematically for each of the categories and dimensions described above. The team members were once again partnered to independently extract data for each category or dimension. The lead author resolved any discrepancies in data extraction. Extracted data also included author information, funding source, study aims and location, demographic characteristics of participants, and theoretical basis for the intervention, if available.
2.4. Quality Assessment
Traditional methods of quality assessment used in systematic reviews do not always translate easily to qualitative reviews that include papers with a wide variety of study designs, as was the case for our review [14]. Our focus on training approaches, intervention messaging, and methods of evaluation rather than a primary emphasis on outcomes meant that the inclusion criteria allowed for a range of study types, from cluster randomized trials to protocol papers, that could not be directly compared to one another in terms of quality. While we determined that studies would not be excluded on the basis of quality due to their potential to provide information valuable to our review question, we assessed the methodological strengths and limitations of the included studies in order to consider the effect of limitations on our review findings [18]. For this assessment, we used a modified version the CASP tool for qualitative research [19]. We omitted the question asking whether qualitative methodology is appropriate, given that many of our included studies had quantitative research questions and were not designed to be assessed according to qualitative criteria. However, when the questions were applied according to the aim of each study, the tool provided a consistent framework for identifying methodological strengths and limitations. Without a definitive tool for such an assessment across a range of study types, the CASP tool was the best fit for our analysis.
We dichotomized studies into those with adequate methodological strength and those that were methodologically limited. The review team decided that studies with four or more ‘no’ responses using the CASP tool would be categorized as methodologically limited. Any differences in opinion in quality assessment were discussed among the review team until we reached consensus on categorization of each study. Following our review synthesis, we conducted a sensitivity analysis to determine whether the exclusion of methodologically limited studies affected the themes identified or the complexity of detail within each theme [19,20].
3. Results
The database search yielded 2041 articles after duplicates were removed; following title and abstract screening, 88 papers were retained for full text screening. Two additional full text papers were added from hand searching after the intervention was identified in a clinical trial protocol captured by the database search. The screening process identified 48 papers meeting the criteria for inclusion in the review, representing 39 unique interventions. An additional five papers were identified during the full text review that pertained to included interventions, for a total of 53 papers used in the data extraction process [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73]. The most common reasons for exclusion at the full text stage included a target population outside the 10–14-year-old age range (n = 16), lack of description of the training process (n = 14), and an intervention scaffolded over multiple school years (n = 8). The flowchart in Figure 1 details the screening and selection process.
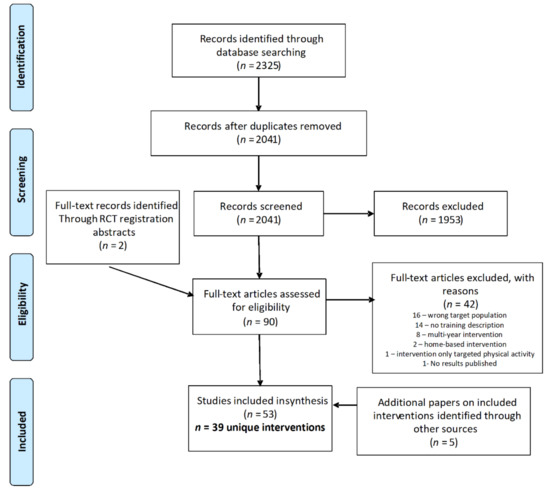
Figure 1.
PRISMA flowchart of study selection process.
Of the 39 interventions included, the majority (n = 23) took place in the United States. Interventions outside the U.S. were in Europe (n = 7), Canada (n = 2), China (n = 2), and one each in Australia, New Zealand, Aruba, and Ethiopia. The framework shown in Table 1 above was applied to each of the 39 interventions to divide them into categories. Eight of the interventions [21,40,45,52,53,59,65,70,72,73] included two different groups that were trained as facilitators, so they were included in both applicable categories. Two interventions [33,46,47] had both an in-class curriculum component and an out-of-school component where students interacted with professional athletes; these are included in both groups A and D. Five interventions trained the target population themselves to deliver the intervention to others. These were classified into the same age peer groups since the training was targeted at 10–14-year-olds. The trained youth then delivered nutrition information to the community (Group F) [45,48,55,63], or taught younger students (Group C) [67].
In our quality assessment, 34 of the 39 studies were categorized as having adequate methodological strength. We observed the following limitations most commonly across included studies: (1) study design, as not all interventions could be conducted in a randomized setting or include a comparison group, (2) insufficient power to detect an intervention effect, (3) short follow-up periods that do not allow for assessment of long-term behavior change, and (4) difficulty in obtaining reliable dietary intake information from participant self-report. We conducted a sensitivity analysis by excluding the five studies identified as methodologically limited [22,27,58,64,68] from the synthesis, and still identified the same themes. Although these studies made contributions toward our review question, such as incorporating the community into intervention design [22] or empowering youth to advocate in their community [58], these details were also present in other included studies. The “thickness” of the themes was not diminished when the sensitivity analysis was performed, as none of the details identified within each theme were dependent on only one study.
In the sections that follow, we identify the key themes from each of the intervention groups, and a summary table is provided for each group. We summarize the training design, intervention format and delivery, and the evaluation indicators used for each intervention, along with notable results. For outcome results, we focused on significant changes in food groups of concern for adolescents: fruit and vegetables, and sugar-sweetened beverages. We also summarized qualitative feedback from intervention participants and those delivering the intervention when it was reported in studies.
3.1. Group A: Classroom-Based Interventions That Trained Adults
Nutrition education interventions delivered in a classroom setting where adults were the population trained to deliver the intervention was the largest group in our categorization system (n = 19 unique interventions). Teachers were the primary population trained, though in some instances, graduate students, volunteers, or assistants were also trained as co-teachers [22,49,50,51,54,56,57,69]. In five of the interventions, the authors describe an initial training with follow-up trainings or regular meetings with teachers during the intervention to provide support or resolve any issues that arose [22,28,29,30,31,32,45,46,47,51]. Most trainings are described as in-services or professional development for teachers, and several note that trainings were interactive, giving teachers the opportunity to practice delivering the content to the trainers and their peers. Four interventions emphasized encouraging those delivering the intervention to tailor examples and references to the local context [22,45,49,50,51].
Basic nutrition concepts were covered across the interventions, e.g., energy balance, food groups, portion sizes, healthy meals, and snacks. Key messages included increasing fruit and vegetable consumption, decreasing sugar-sweetened beverage and unhealthy snack consumption, and eating out less often. Several of the interventions included activities where students learned to read nutrition labels, track their food intake, set goals, or make plans for healthy eating, assess their neighborhood food environment, and develop strategies for making healthy choices within their context.
In four of the interventions, the curriculum was incorporated into students’ PE class [21,22,46,47,72,73], while in two others, it was incorporated into science class and specifically mentioned an inquiry-based approach for student learning [27,28,29,30,31,32,33]. Eight of the interventions explicitly mentioned aligning the content with state or national standards or curriculums [27,28,29,30,31,32,34,36,37,49,50,51,64]. In three instances, homework was included in the intervention design that was meant to facilitate students engaging with their family about the nutrition information [34,37,49,50]. Four interventions also involved a connection to school meals, often engaging students in advocating for healthy meal options they would enjoy [45,54,56,57,69].
Evaluation measures varied by intervention but commonly included analysis of anthropometric changes, shifts in dietary intake, and differences in knowledge or attitudes between pre-and post-intervention. For process evaluation, six of the interventions included observations of a portion of the classroom lessons by research staff to assess fidelity and student engagement [21,28,29,30,31,32,45,61,69,72,73]. Four of the interventions held student focus groups post-intervention to gain qualitative feedback [22,27,54,69], and two used a student satisfaction survey [28,29,30,31,32,33]. Table 2 below further describes the interventions included in Group A.
Table 2.
Group A: Classroom-based interventions that trained adults.
3.2. Group B: Classroom-Based Interventions That Trained Cross-Age Peers
There were four interventions that trained cross-age peers to deliver classroom-based lessons. Three of the interventions trained high school students [21,35,38], and the remaining one trained undergraduate university students [59]. In three of the four interventions, cross-age peers taught as a group [38,59] or with teachers [19]. Two of the interventions had weekly training for cross-age peers [21,35], and two emphasized the opportunity to practice delivering the intervention as part of the training [21,38].
One of the interventions focused specifically on healthy beverages [59]; the other three all included both nutrition and physical activity content. In each of the interventions, there was an emphasis on games as a medium for delivering the nutrition content. Compared with the interventions in Group A, these interventions were delivered over a shorter period of time, except for the one where cross-age peers worked with PE teachers [21]. Role-modeling healthy habits was a key emphasis with cross-age peers.
Outcome measurers were similar to Group A, though one of the studies evaluated outcomes and intervention acceptability for the cross-age peers [38], which could serve as indicators of the engagement level of those delivering the intervention. Of note, for one intervention, only the group that received the intervention from cross-age and same-age peers showed a sustained significant decrease in SSB consumption [59]. The four interventions are described in Table 3.
Table 3.
Group B: Classroom-based interventions that trained cross-age peers.
3.3. Group C: Classroom-Based Intereventions That Trained Same-Age Peers
Two classroom-based interventions trained same-age peers as facilitators; in both cases the peers had strong support and mentorship from either adults or cross-age peers. Both interventions also put the same-age peers in groups to deliver the intervention material. In one of the interventions, those trained were in our target population age range and delivered the intervention to younger elementary students [67]. This intervention is included here and not in Group B in order to examine it alongside other trainings designed for the same age group. The training elements in these interventions provide insight into strategies for empowering the target age group, which is a key component of many nutrition education interventions for middle schoolers. Table 4 describes the interventions included in Group C.
Table 4.
Group C: Classroom-based interventions that trained same-age peers.
3.4. Group D: Community, Afterschool, or Extracurricular Interventions That Trained Adults
Ten interventions trained adults to deliver nutrition education in a context outside the classroom: four were based in the community [33,46,47,58,62], four were afterschool programs [40,60,71,72,73], one was delivered in multiple settings that included both community and afterschool programs [52,53], and one took place during school lunch [70]. Four of the interventions also included classroom-based components [33,46,47,70,72,73].
The types of interventions varied widely, as did the training format, but a common theme across all the interventions in this group was an expansion beyond basic nutrition education. Four of the interventions particularly emphasized role models/mentors [33,46,47,58,70]; two of which included activities with professional sports teams in the community. Interventions in this group also went deeper into the food environment, food sources, student advocacy for healthy changes, and addressing barriers to healthy eating than did the interventions that were classroom- based. In terms of evaluation, two interventions used student surveys to measure acceptability [33,52,53], and two conducted focus groups with youth to assess barriers and facilitators to healthy eating [60,62]. Of note in these focus groups with youth in different parts of the U.S.: both groups expressed limited availability of healthy food in their home and neighborhood environments as a major limiting factor in healthy eating, especially when it came to fresh fruit and vegetables. The interventions included in Group D are presented in Table 5 below.
Table 5.
Group D: Community, afterschool, or extracurricular interventions that trained adults.
3.5. Group E: Community, Afterschool or Extracurricular Interventions That Trained Cross-Age Peers
Four interventions trained cross-age peers to implement interventions outside a classroom setting. All interventions trained high school students, though one intervention also trained undergraduate college students in their first wave [41,42,43,44]. Similar to classroom-based interventions using cross-age peers, facilitators taught as groups of leaders rather than as individuals. One intervention paired cross-age peers with adults with the goal of training them throughout the intervention to facilitate sessions on their own [40]. Another gave cross-age peers autonomy in scheduling intervention events with younger peers, with adult support available for planning and guidance [65]. Both of these interventions had less consistency in participation among cross-age peers than the one that had a more structured intervention delivery plan [41,42,43,44]. The fourth intervention in this group used cross-age peers to develop intervention content that was then used in a virtual format and accompanied lessons taught by adults [52,53]. This element of the intervention was noteworthy because it encouraged cross-age peers to tap into their interests, whether sports, ballet, art, etc., and connect that to nutrition content.
One of the interventions conducted post-intervention focus groups with both youth participants and cross-age peers [41,42,43,44]. Youth reported they particularly enjoyed the games and cooking lessons. Cross-age peers reported that discussions were the most difficult intervention element in which to engage youth. They noted that it would have been helpful to have more role-playing opportunities during the training to address various scenarios. The leaders also emphasized the importance of communicating simple nutrition messages and having cross-age peers that are representative of the community where they are working. Table 6 describes the interventions included in Group E.
Table 6.
Group E: Community, afterschool, or extracurricular interventions that trained cross-age peers.
3.6. Group F: Community, Afterschool or Extracurricular Interventions That Trained Same-Age Peers
Ten interventions in our review trained same-age peers to deliver nutrition education information outside a classroom context. These interventions were generally less structured than those that were classroom-based; only one had a weekly schedule of lessons that peers delivered [68]. A key theme across this group of interventions was having simple messaging that was easy for same-age peers to use in conversation, whether in an informal or more formal context.
Three interventions were informal in their structure: same-age peers were trained and then tasked with spreading the messages through their normal social networks [23,39,66]. Two of these were essentially the same intervention implemented in two different countries and focused on promoting water consumption [39,66]. Peers brought up water consumption in conversation and also modeled drinking water throughout the day. Of note, these interventions measured changes in SSB intake as well as in water intake, but the message was positively focused on water consumption rather than on decreasing SSB consumption.
Four of the interventions took place either during the school lunch period or after school. Same-age peers promoted healthy eating and conducted taste tests in the cafeteria [24,25,26], planned their own events with peers [65], or taught lessons and promoted nutrition messages through club activities [68]. The remaining three interventions involved a small group of the target population who participated in afterschool programs where nutrition was incorporated into another activity. Two of these interventions were photovoice projects, where youth took pictures in their neighborhoods that gave visual representation to the food environment and then showcased their work in a community exhibition [55,63]. In one of the photovoice projects, a student took her photographs of the school cafeteria food to the food service director and successfully advocated for healthier options [63]. The third of these types of interventions was an afterschool theater program in which youth wrote a play about healthy eating and performed it in a dinner theater setting for their friends and family [48]. These interventions represent creative ways for youth to connect nutrition with other hobbies or interests and to use their voices to advocate for the health of their community. The interventions in Group F are further described in Table 7.
Table 7.
Group F: Community, afterschool or extracurricular interventions that trained same-age peers.
4. Discussion
This review synthesizes components of nutrition education interventions targeting middle school-age students across a wide range of settings and program designs, all of which incorporate some version of a train-the-trainer model. The use of a framework synthesis approach to organize the interventions allowed for key themes to emerge from various settings that can inform future nutrition education interventions that employ train-the-trainer methodology and target the middle school population, especially in low-resource, urban settings. By focusing on training components, intervention content and design, and process evaluation results rather than primarily on outcomes [10,11], this review makes a unique contribution to the literature on youth nutrition education interventions.
Our first dimension for synthesis of themes centered on train-the trainer approaches, and we found that engaging sessions that provide opportunities for role play and talking through scenarios that may arise with the target youth were well-received [49,50,51,56,57,70,72,73], especially when those being trained were cross-age or same-age peers [24,25,38,65]. For example, the Foley et al. paper describes trainers interactively teaching the curriculum to cross-age peers and then giving the youth the opportunity to practice teaching the lessons during the training [38]. Additionally, providing follow-up training sessions and/or regular contact with intervention facilitators to provide support and troubleshoot can help ensure intervention fidelity [28,29,30,31,32,45,46,47,51,65,70]. Training sessions also included emphasis on adapting interventions to the local context and using culturally relevant examples [49,50,52,53,69,71]. The interventions included here underscore the importance of mentors and role-models who go beyond teaching nutrition information to modeling healthy behaviors themselves, which has been identified previously in the literature [74,75]. Additionally, when interventions engage trainers and allow them to connect their interests—whether in sports, gardening, or the arts—to nutrition, the youth receiving the intervention will also be more engaged [48,52,53].
Our second dimension focused on the intervention content. We found fruit and vegetable consumption [24,25,26,34,37,48,49,50,52,53,54,60,68,69], healthy beverages [23,33,34,39,40,41,42,43,44,46,47,59,61,66], and healthy breakfast [23,33,38,40,45,48,49,50,52,53,54,61,68] to be common topics. Beyond basic nutrition information, the interventions in this review commonly included goal setting [38,49,50,51,60], building skills to identify healthy options (including reading food labels) [52,53,54,59,60], and developing strategies to make healthy choices through an awareness of the food environment context [40,41,42,43,44,55,58,62,63]. Interventions included in this review also indicated that youth can be change agents in their communities and advocate for healthier food options in their school and neighborhoods [55,58,63]. In Leung et al., the intervention aimed to understand youth perceptions of food justice in their community using photovoice and equip them to promote positive change in their community food environment [55].
The third dimension focused on the format and delivery of the interventions, which as might be expected, varied by setting. Classroom based interventions followed a more structured curriculum, as did some afterschool programs, while other interventions relied on informal conversations among peers to disseminate information. When peers were delivering interventions, less structure sometimes led to less consistency [40,65]. One of the key findings within this theme was creating nutrition messages that are positive and simple, especially if the intervention is delivered in a less structured context outside the classroom [39,41,42,43,44,66]. Smit et al. and Franken et al. demonstrated this with their water promotion intervention implemented in the Netherlands and Aruba, respectively. The main intervention message was framed positively, encouraging water consumption, rather than discouraging sugar-sweetened beverage consumption, yet participants still reported significant decreases in their intake of sugar-sweetened beverages [39,66].
Our fourth and fifth dimensions synthesized outcomes and feedback from the youth participating in the intervention and from those trained to deliver the intervention, when measured. We were particularly interested in youth engagement, receptivity, and feedback provided through surveys and focus groups. Participant engagement and receptivity were measured through a wide range of approaches, when they were actually included as an evaluation metric. Only three interventions explicitly mentioned using student satisfaction surveys [28,29,30,31,32,33,52,53], and all three used different scales. Other interventions obtained feedback from those delivering the intervention or observers about youth engagement [28,29,30,31,32,41,42,43,44,64], making it difficult to compare receptivity across interventions. Focus groups were helpful in identifying which nutrition messages were most commonly retained, the components of the interventions that participants most enjoyed, and barriers to making dietary changes. For example, both Luesse et al. and Molaison et al. heard from youth that the lack of availability of healthy foods at home and in their communities made it difficult to make healthy choices [60,62]. Feedback from those delivering the intervention was reported less often, but both Foley et al. and Gittlesohn et al. obtained feedback from the cross-age peers who delivered the intervention and found that the older youth were implementing what they were teaching in their own lives [38,41,42,43,44]. We extracted data on the types of outcomes that were measured in the interventions, which commonly included anthropometric data, dietary intake, and knowledge, attitudes and behaviors related to healthy eating, but we did not focus on the results of these outcome measures themselves.
While evaluation of intervention efficacy is undeniably essential, improving youth health outcomes is a long-term objective, making it difficult to quantify success in the short-term with anthropometric measurements or behavioral questionnaires. Although BMI is well-correlated with fat mass and percent body fat in youth, it can be difficult to discern whether BMI reductions post-intervention actually indicate a reduction in adiposity, the more important result for improving health outcomes [76,77]. Additionally, changes in BMI may not necessarily reflect dietary shifts, as a number of factors, including physical activity and developmental changes, also have an effect on BMI. Furthermore, dietary assessment methods for youth yield imprecise information, and validity tends to be lower for food frequency questionnaires—the type of evaluation tool favored in the interventions included in this review due to their lower administrative burden [78]. Where resources are not available to measure long-term changes in dietary behaviors and outcomes such as body composition or biochemical markers of chronic disease risk, we posit that information about youth and trainer engagement, such as the content extracted in this review, provides good indication of whether an intervention will influence the habits of youth, leading to improved nutrition outcomes and health over the long term.
4.1. Limitations
One of the major limitations of this review was the variability in process and outcome measures used to evaluate the efficacy of the interventions. Such variability, as well as the limitations of outcome evaluation measures described above, make it difficult to determine which methodologies or designs would be most efficacious for training those delivering the intervention and for improving youth nutrition outcomes. The variability in process measures also limited our ability to assess youth acceptability of the interventions in a systematic way, though we were still able to identify components that were particularly engaging for youth across multiple interventions. The review was also limited in that few of the studies examined the effect of the intervention on the “trainers,” which could serve as another important marker of long-term impact in creating a culture of health for youth. Finally, while including a wide range of study types was beneficial in the additional insight provided through qualitative methods and study protocols, it did limit the depth of our quality assessment
4.2. Application of Findings
We incorporated the major themes identified through this review into a nutrition training for the COACHES project, a sports-based youth development intervention targeting middle school students in New Orleans, Louisiana. In the initial training for the near-peer coaches working with the youth, we emphasized three key messages that were simple, positive, and focused: fruit and vegetable consumption, maintaining hydration-primarily through water intake, and eating breakfast regularly. These three messages were included in nearly every intervention in this study and are highly relevant for our target population, particularly due to their participation in sports [79,80]. In the initial training, we covered goal setting, as well as skills and strategies for making healthy choices, in the context of the three key messages. We communicated this content to the coaches through interactive games and activities that they could then use with their youth. We conducted a follow-up training four months after the initial training to address strategies for overcoming both internal (e.g., reluctance to share about food choices due to self-consciousness) and external (e.g., lack of affordable, healthy options in the food environment) barriers youth face when seeking to make healthful dietary choices, and we used role-playing activities to address scenarios that coaches encounter in their work.
5. Conclusions
This review provides important insights and enhances understanding of the design, methodology, and structure of train-the-trainer nutrition education interventions for middle school youth in U.S. and U.S.-comparable urban settings. Several of the studies included here also illuminate barriers that youth face to healthy eating, especially in urban environments with limited affordable, fresh food options and an abundance of inexpensive, high-calorie processed foods. In middle school, youth have increasing, though not complete, agency over their food choices, and conversation about the food environment at home, at school, and in the broader community should be included in nutrition education interventions, as should devising strategies to navigate those food environments in healthy ways. One of the limitations of this review was the lack of consistent methods for evaluating youth receptivity of the intervention. Further research should include more measures of engagement and youth feedback, not only immediately post-intervention, but also after several months post intervention to determine whether messages have stayed with the youth and continue to motivate healthy behavior change.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/nu13082749/s1. Figure S1: Electronic search strategy for PubMed/Medline Database.
Author Contributions
Conceptualization, C.S.P., W.G., J.M. and J.M.S.; methodology, C.S.P.; article review and data extraction, L.B., G.D., A.M. and S.G.; writing—original draft preparation, C.S.P.; writing—review and editing, W.G., J.M., J.M.S.; All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the U.S. Department of Health and Human Services Office of Minority Health, grant number CPIMP191186.
Acknowledgments
The 2020–2021 New Orleans-based Up2 Us Coaches; Up2Us staff—including Jerita Mitchell, Katie Rawlings, and the entire training team; and physical activity training partner Natasha Cruz were all instrumental in developing and delivering the trainings that came from the application of these review findings.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Herman, K.M.; Craig, C.L.; Gauvin, L.; Katzmarzyk, P.T. Tracking of obesity and physical activity from childhood to adulthood: The Physical Activity Longitudinal Study. Int. J. Pediatr. Obes. 2009, 4, 281–288. [Google Scholar] [CrossRef]
- Megari, K. Quality of life in chronic disease patients. Health Psychol. Res. 2013, 1, e27. [Google Scholar] [CrossRef]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity Among Adults and Youth: United States, 2015–2016. NCHS Data Brief, No. 288; National Center for Health Statistics: Hyattsville, MD, USA, 2017. [Google Scholar]
- Ogden, C.L.; Carroll, M.D.; Fakhouri, T.H.; Hales, C.; Fryar, C.D.; Li, X.; Freedman, D.S. Prevalence of Obesity among Youths by Household Income and Education Level of Head of Household—United States 2011–2014. MMWR Morb. Mortal Wkly. Rep. 2018, 67, 186–189. [Google Scholar] [CrossRef]
- National Survey of Children’s Health Interactive Data Query: 2018–2019 National Survey of Children’s Health. Baltimore, MD: Data Resource Center for Child and Adolescent Health. Available online: https://www.childhealthdata.org/browse/survey/results?q=7620&r=1 (accessed on 10 March 2021).
- Kim, S.A.; Moore, L.V.; Galuska, D. Vital Signs: Fruit and vegetable intake among children—United States, 2003–2010. MMWR 2014, 63, 671–676. [Google Scholar] [PubMed]
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among children age 4–13 years in the United States: Analyses of 2005–2010 NHANES data. Nutr. J. 2013, 12, 85. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rodrigo, C.; Wind, M.; Hildonen, C.; Bjelland, M.; Aranceta, J.; Klepp, K.-I.; Brug, J. The Pro Children Intervention: Applying the Intervention Mapping Protocol to Develop a School-Based Fruit and Vegetable Promotion Programme. Ann. Nutr. Metab. 2005, 49, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Langford, R.; Bonell, C.; Jones, H.; Campbell, R. Obesity prevention and the Health promoting Schools framework: Essential components and barriers to success. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–17. [Google Scholar] [CrossRef]
- Kamath, C.C.; Vickers, K.S.; Ehrlich, A.; McGovern, L.; Johnson, J.; Singhal, V.; Paulo, R.; Hettinger, A.; Erwin, P.J.; Montori, V.M. Behavioral Interventions to Prevent Childhood Obesity: A Systematic Review and Metaanalyses of Randomized Trials. J. Clin. Endocrinol. Metab. 2008, 93, 4606–4615. [Google Scholar] [CrossRef] [PubMed]
- Meiklejohn, S.; Ryan, L.; Palermo, C. A Systematic Review of the Impact of Multi-Strategy Nutrition Education Programs on Health and Nutrition of Adolescents. J. Nutr. Educ. Behav. 2016, 48, 631–646.e1. [Google Scholar] [CrossRef]
- Murimi, M.W.; Moyeda-Carabaza, A.F.; Nguyen, B.; Saha, S.; Amin, R.; Njike, V. Factors that contribute to effective nutrition education interventions in children: A systematic review. Nutr. Rev. 2018, 76, 553–580. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Cherry, M.G.; Smith, H.; Perkins, E.; Boland, A. Reviewing Qualitative Evidence. In Doing a Systematic Review: A Student’s Guide, 2nd ed.; Boland, A., Cherry, M.G., Dicksson, R., Eds.; Sage Publications: London, UK, 2017; Chapter 11; pp. 193–222. [Google Scholar]
- Oliver, S.R.; Rees, R.; Clarke-Jones, L.; Milne, R.; Oakley, A.R.; Gabbay, J.; Stein, K.; Buchanan, P.; Gyte, G. A multidimensional conceptual framework for analysing public involvement in health services research. Health Expect. 2008, 11, 72–84. [Google Scholar] [CrossRef]
- Oliver, S.; Clarke-Jones, L.; Rees, R.; Milne, R.; Buchanan, P.; Gabbay, J.; Gyte, G.; Oakley, A.; Stein, K. Involving consumers in research and development agenda setting for the NHS: Developing an evidence-based approach. Health Technol. Assess. 2004, 8, 1–148. [Google Scholar] [CrossRef]
- Brunton, G.; Oliver, S.; Thomas, J. Innovations in framework synthesis as a systematic review method. Res. Synth. Methods 2020, 11, 316–330. [Google Scholar] [CrossRef] [PubMed]
- Noyes, J.; Booth, A.; Cargo, M. Qualitative evidence. In Cochrane Handbook for Systematic Reviews of Interventions, Version 6.2; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2021; Chapter 21; updated on February 2021; Available online: www.training.cochrane.org/handbook (accessed on 23 July 2021).
- Critical Appraisal Skills Programme. CASP Qualitative Checklist. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf (accessed on 23 July 2021).
- Carroll, C.; Booth, A.; Lloyd-Jones, M. Should We Exclude Inadequately Reported Studies from Qualitative Systematic Reviews? An Evaluation of Sensitivity Analyses in Two Case Study Reviews. Qual. Health Res. 2012, 22, 1425–1434. [Google Scholar] [CrossRef] [PubMed]
- Arlinghaus, K.R.; Moreno, J.; Reesor, L.; Hernandez, D.C.; Johnston, C.A. Compañeros: High School Students Mentor Middle School Students to Address Obesity Among Hispanic Adolescents. Prev. Chronic Dis. 2017, 14, E92. [Google Scholar] [CrossRef]
- Baskin, M.L.; Zunker, C.; Worley, C.B.; Dial, B.; Kimbrough, L. Design and implementation of a pilot obesity prevention program in a low-resource school. Health Educ. 2008, 109, 66–85. [Google Scholar] [CrossRef]
- Bell, S.L.; Audrey, S.; Cooper, A.; Noble, S.; Campbell, R. Lessons from a peer-led obesity prevention programme in English schools. Health Promot. Int. 2017, 32, 250–259. [Google Scholar] [CrossRef]
- Bogart, L.M.; Elliott, M.N.; Cowgill, B.O.; Klein, D.J.; Hawes-Dawson, J.; Uyeda, K.; Schuster, M.A. Two-Year BMI Outcomes From a School-Based Intervention for Nutrition and Exercise: A Randomized Trial. Pediatrics 2016, 137, e20152493. [Google Scholar] [CrossRef]
- Bogart, L.M.; Cowgill, B.O.; Elliott, M.N.; Klein, D.J.; Hawes-Dawson, J.; Uyeda, K.; Elijah, J.; Binkle, D.G.; Schuster, M.A. A Randomized Controlled Trial of Students for Nutrition and eXercise: A Community-Based Participatory Research Study. J. Adolesc. Health 2014, 55, 415–422. [Google Scholar] [CrossRef]
- Bogart, L.M.; Elliott, M.N.; Uyeda, K.; Hawes-Dawson, J.; Klein, D.J.; Schuster, M.A. Preliminary Healthy Eating Outcomes of SNaX, a Pilot Community-Based Intervention for Adolescents. J. Adolesc. Health 2011, 48, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, A.; Fredericks, L.; Wylie-Rosett, J. Strategies to Promote High School Students’ Healthful Food Choices. J. Nutr. Educ. Behav. 2011, 43, 414–418. [Google Scholar] [CrossRef]
- Contento, I.R.; Koch, P.A.; Lee, H.; Calabrese-Barton, A. Adolescents Demonstrate Improvement in Obesity Risk Behaviors after Completion of Choice, Control & Change, a Curriculum Addressing Personal Agency and Autonomous Motivation. J. Am. Diet. Assoc. 2010, 110, 1830–1839. [Google Scholar] [CrossRef] [PubMed]
- Contento, I.R.; Koch, P.A.; Lee, H.; Sauberli, W.; Calabrese-Barton, A. Enhancing Personal Agency and Competence in Eating and Moving: Formative Evaluation of a Middle School Curriculum—Choice, Control, and Change. J. Nutr. Educ. Behav. 2007, 39, S179–S186. [Google Scholar] [CrossRef]
- Gray, H.L.; Contento, I.R.; Koch, P.A.; Di Noia, J. Mediating Mechanisms of Theory-Based Psychosocial Determinants on Behavioral Changes in a Middle School Obesity Risk Reduction Curriculum Intervention, Choice, Control, and Change. Child Obes. 2016, 12, 348–359. [Google Scholar] [CrossRef]
- Gray, H.L.; Contento, I.R.; Koch, P.A. Linking implementation process to intervention outcomes in a middle school obesity prevention curriculum, ‘Choice, Control and Change’. Health Educ. Res. 2015, 30, 248–261. [Google Scholar] [CrossRef]
- Lee, H.; Contento, I.R.; Koch, P. Using a Systematic Conceptual Model for a Process Evaluation of a Middle School Obesity Risk-Reduction Nutrition Curriculum Intervention: Choice, Control & Change. J. Nutr. Educ. Behav. 2013, 45, 126–136. [Google Scholar] [CrossRef]
- Dubuy, V.; De Cocker, K.; De Bourdeaudhuij, I.; Maes, L.; Seghers, J.; Lefevre, J.; De Martelaer, K.; Brooke, H.; Cardon, G. Evaluation of a real world intervention using professional football players to promote a healthy diet and physical activity in children and adolescents from a lower socio-economic background: A controlled pretest-posttest design. BMC Public Health 2014, 14, 457. [Google Scholar] [CrossRef]
- Duncan, S.; Stewart, T.; McPhee, J.; Borotkanics, R.; Prendergast, K.; Zinn, C.; Meredith-Jones, K.; Taylor, R.; McLachlan, C.; Schofield, G. Efficacy of a compulsory homework programme for increasing physical activity and improving nutrition in children: A cluster randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 1–12. [Google Scholar] [CrossRef]
- El Rayess, F.; Gandhi, M.; Mennillo, H. Mark, Set, Go! School-Based Nutrition and Physical Activity Program: A Five-Year Evaluation. Rhode Isl. Med. J. 2017, 100, 39–44. [Google Scholar]
- Fahlman, M.M.; Dake, J.A.; McCaughtry, N.; Martin, J. A Pilot Study to Examine the Effects of a Nutrition Intervention on Nutrition Knowledge, Behaviors, and Efficacy Expectations in Middle School Children. J. Sch. Health 2008, 78, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Hackett, A.F.; Davies, I.G.; Gobbi, R.; Mackintosh, K.A.; Warburton, G.L.; Stratton, G.; Van Sluijs, E.M.; Boddy, L.M. Promoting healthy weight in primary school children through physical activity and nutrition education: A pragmatic evaluation of the CHANGE! Randomised intervention study. BMC Public Health 2013, 13, 626. [Google Scholar] [CrossRef]
- Foley, B.C.; Shrewsbury, V.A.; Hardy, L.L.; Flood, V.M.; Byth, K.; Shah, S. Evaluation of a peer education program on student leaders’ energy balance-related behaviors. BMC Public Health 2017, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- Franken, S.C.M.; Smit, C.R.; Buijzen, M. Promoting Water Consumption on a Caribbean Island: An Intervention Using Children’s Social Networks at Schools. Int. J. Environ. Res. Public Health 2018, 15, 713. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Dennisuk, L.A.; Christiansen, K.; Bhimani, R.; Johnson, A.; Alexander, E.; Lee, M.; Lee, S.H.; Rowan, M.; Coutinho, A.J. Development and implementation of Baltimore Healthy Eating Zones: A youth-targeted intervention to improve the urban food environment. Health Educ. Res. 2013, 28, 732–744. [Google Scholar] [CrossRef]
- Gittelsohn, J.; Steeves, E.A.; Mui, Y.; Kharmats, A.Y.; Hopkins, L.C.; Dennis, D. B’More Healthy Communities for Kids: Design of a multi-level intervention for obesity prevention for low-income African American children. BMC Public Health 2014, 14, 942. [Google Scholar] [CrossRef] [PubMed]
- Sato, P.M.; Steeves, E.A.; Carnell, S.; Cheskin, L.J.; Trude, A.C.; Shipley, C.; Ruiz, M.J.M.; Gittelsohn, J. A youth mentor-led nutritional intervention in urban recreation centers: A promising strategy for childhood obesity prevention in low-income neighborhoods. Health Educ. Res. 2016, 31, 195–206. [Google Scholar] [CrossRef]
- Trude, A.C.B.; Steeves, E.A.; Shipley, C.; Surkan, P.J.; Sato, P.D.M.; Estep, T.; Clanton, S.; Lachenmayr, L.; Gittelsohn, J. A Youth-Leader Program in Baltimore City Recreation Centers: Lessons Learned and Applications. Health Promot. Pract. 2018, 19, 75–85. [Google Scholar] [CrossRef]
- Steeves, E.A.; Trude, A.C.B.; Ruggiero, C.F.; Ruiz, M.J.M.; Jones-Smith, J.; Porter, K.P.; Cheskin, L.; Hurley, K.; Hopkins, L.; Gittelsohn, J. Perceptions and Impact of a Youth-led Childhood Obesity Prevention Intervention among Youth-leaders. J. Hunger. Environ. Nutr. 2019, 16, 213–234. [Google Scholar] [CrossRef]
- Heo, M.; Jimenez, C.C.; Lim, J.; Isasi, C.R.; Blank, A.E.; Lounsbury, D.W.; Fredericks, L.; Bouchard, M.; Faith, M.S.; Wylie-Rosett, J.; et al. Effective nationwide school-based participatory extramural program on adolescent body mass index, health knowledge and behaviors. BMC Pediatr. 2018, 18, 7. [Google Scholar] [CrossRef]
- Irwin, C.; Irwin, R.; Richey, P.; Miller, M.; Boddie, J.; Dickerson, T. Get fit with the Grizzlies: A community-school-home initiative to fight childhood obesity led by a professional sports organization. Stud. Health Technol. Inform. 2012, 172, 163–167. [Google Scholar]
- Irwin, C.C.; Miller, M.E.; Somes, G.W.; Richey, P.A.; Irwin, R.L. Get Fit with the Grizzlies: A Community-School-Home Initiative to Fight Childhood Obesity. J. Sch. Health 2010, 80, 333–339. [Google Scholar] [CrossRef]
- Jackson, C.J.; Mullis, R.M.; Hughes, M. Development of a theater-based nutrition and physical activity intervention for low-income, urban, African American adolescents. Prog. Community Health Partnersh. Res. Educ. Action 2010, 4, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Kipping, R.R.; Howe, L.; Jago, R.; Campbell, R.; Wells, S.; Chittleborough, C.; Mytton, J.; Noble, S.M.; Peters, T.; Lawlor, D.A. Effect of intervention aimed at increasing physical activity, reducing sedentary behaviour, and increasing fruit and vegetable consumption in children: Active for Life Year 5 (AFLY5) school based cluster randomised controlled trial. BMJ 2014, 348, g3256. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Jago, R.; Noble, S.M.; Chittleborough, C.R.; Campbell, R.; Mytton, J.; Howe, L.D.; Peters, T.J.; Kipping, R.R. The Active for Life Year 5 (AFLY5) school based cluster randomised controlled trial: Study protocol for a randomized controlled trial. Trials 2011, 12, 181. [Google Scholar] [CrossRef]
- Koch, P.A.; Contento, I.R.; Gray, H.L.; Burgermaster, M.; Bandelli, L.; Abrams, E.; Di Noia, J. Food, Health, & Choices: Curriculum and Wellness Interventions to Decrease Childhood Obesity in Fifth-Graders. J. Nutr. Educ. Behav. 2019, 51, 440–455. [Google Scholar] [CrossRef]
- Kohlstadt, I.; Gittelsohn, J.; Fang, Y. NutriBee Intervention Improves Diet and Psychosocial Outcomes by Engaging Early Adolescents from Diverse and Disadvantaged Communities. J. Am. Coll. Nutr. 2016, 35, 1–9. [Google Scholar] [CrossRef]
- Kohlstadt, I.C.; Steeves, E.T.A.; Rice, K.; Gittelsohn, J.; Summerfield, L.M.; Gadhoke, P. Youth peers put the “invent” into NutriBee’s online intervention. Nutr. J. 2015, 14, 1–8. [Google Scholar] [CrossRef]
- Lepe, S.; Goodwin, J.; Mulligan, K.T.; Balestracci, K.; Sebelia, L.; Greene, G. Process Evaluation of a Policy, Systems, and Environmental Change Intervention in an Urban School District. J. Nutr. Educ. Behav. 2019, 51, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Leung, M.M.; Agaronov, A.; Entwistle, T.; Harry, L.; Sharkey-Buckley, J.; Freudenberg, N. Voices through Cameras. Health Promot. Pract. 2016, 18, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hu, X.; Zhang, Q.; Liu, A.; Fang, H.; Hao, L.; Duan, Y.; Xu, H.; Shang, X.; Ma, J.; et al. The nutrition-based comprehensive intervention study on childhood obesity in China (NISCOC): A randomised cluster controlled trial. BMC Public Health 2010, 10, 229. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Li, Y.; Zhang, Q.; Hu, X.L.; Liu, A.; Du, S.; Li, T.; Guo, H.; Li, Y.; Xu, G.; et al. Comprehensive school-based intervention to control overweight and obesity in China: A cluster randomized controlled trial. Asia Pac. J. Clin. Nutr. 2017, 26, 1139–1151. [Google Scholar]
- Linton, L.S.; Edwards, C.C.; Woodruff, S.I.; Millstein, R.A.; Moder, C. Youth Advocacy as a Tool for Environmental and Policy Changes That Support Physical Activity and Nutrition: An Evaluation Study in San Diego County. Prev. Chronic Dis. 2014, 11, E46. [Google Scholar] [CrossRef]
- Lo, E.; Coles, R.; Humbert, M.L.; Polowski, J.; Henry, C.J.; Whiting, S.J. Beverage intake improvement by high school students in Saskatchewan, Canada. Nutr. Res. 2008, 28, 144–150. [Google Scholar] [CrossRef]
- Luesse, H.B.; Luesse, J.E.; Lawson, J.; Koch, P.A.; Contento, I.R. In Defense of Food Curriculum: A Mixed Methods Outcome Evaluation in Afterschool. Health Educ. Behav. 2019, 46, 612–625. [Google Scholar] [CrossRef] [PubMed]
- Mihas, C.; Mariolis, A.; Manios, Y.; Naska, A.; Arapaki, A.; Mariolis-Sapsakos, T.; Tountas, Y. Evaluation of a nutrition intervention in adolescents of an urban area in Greece: Short- and long-term effects of the VYRONAS study. Public Health Nutr. 2009, 13, 712–719. [Google Scholar] [CrossRef]
- Molaison, E.F.; Connell, C.L.; Stuff, J.E.; Yadrick, M.K.; Bogle, M. Influences on Fruit and Vegetable Consumption by Low-Income Black American Adolescents. J. Nutr. Educ. Behav. 2005, 37, 246–251. [Google Scholar] [CrossRef]
- Necheles, J.W.; Chung, E.Q.; Hawes-Dawson, J.; Ryan, G.W.; Williams, S.B.; Holmes, H.N.; Wells, K.B.; Vaiana, M.E.; Schuster, M.A.; Williams, L.B. The Teen Photovoice Project: A Pilot Study to Promote Health Through Advocacy. Prog. Community Health Partnersh. Res. Educ. Action 2007, 1, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Olivares, S.; Zacarías, I.; Andrade, M.; Kain, J.; Lera, L.; Vio, F.; Morón, C. Nutrition Education in Chilean Primary Schools. Food Nutr. Bull. 2005, 26, S179–S185. [Google Scholar] [CrossRef]
- Saez, L.; Legrand, K.; Alleyrat, C.; Ramisasoa, S.; Langlois, J.; Muller, L.; Omorou, A.Y.; De Lavenne, R.; Kivits, J.; LeComte, E.; et al. Using facilitator—Receiver peer dyads matched according to socioeconomic status to promote behaviour change in overweight adolescents: A feasibility study. BMJ Open 2018, 8, e019731. [Google Scholar] [CrossRef] [PubMed]
- Smit, C.R.; de Leeuw, R.N.; Bevelander, K.E.; Burk, W.J.; Buijzen, M. A social network-based intervention stimulating peer influence on children’s self-reported water consumption: A randomized control trial. Appetite 2016, 103, 294–301. [Google Scholar] [CrossRef]
- Stock, S.; Miranda, C.; Evans, S.; Plessis, S.; Ridley, J.; Yeh, S.; Chanoine, J.-P. Healthy Buddies: A Novel, Peer-Led Health Promotion Program for the Prevention of Obesity and Eating Disorders in Children in Elementary School. Pediatrics 2007, 120, e1059–e1068. [Google Scholar] [CrossRef]
- Tamiru, D.; Argaw, A.; Gerbaba, M.; Ayana, G.; Nigussie, A.; Belachew, T. Effect of integrated school-based nutrition education on optimal dietary practices and nutritional status of school adolescents in Southwest of Ethiopia: A quasi-experimental study. Int. J. Adolesc. Med. Health 2016, 29, 20160015. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.-Y.; Boonpleng, W.; McElmurry, B.J.; Park, C.G.; McCreary, L. Lessons Learned in Using TAKE 10! With Hispanic Children. J. Sch. Nurs. 2009, 25, 163–172. [Google Scholar] [CrossRef]
- Tucker, S.; Lanningham-Foster, L.M. Nurse-Led School-Based Child Obesity Prevention. J. Sch. Nurs. 2015, 31, 450–466. [Google Scholar] [CrossRef]
- Wright, K.; Norris, K.; Giger, J.N.; Suro, Z. Improving Healthy Dietary Behaviors, Nutrition Knowledge, and Self-Efficacy among Underserved School Children with Parent and Community Involvement. Child. Obes. 2012, 8, 347–356. [Google Scholar] [CrossRef]
- Zhou, Z.; Li, S.; Yin, J.; Fu, Q.; Ren, H.; Jin, T.; Zhu, J.; Howard, J.; Lan, T.; Yin, Z.; et al. Impact on Physical Fitness of the Chinese CHAMPS: A Clustered Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 4412. [Google Scholar] [CrossRef]
- Zhou, Z.; Dong, S.; Yin, J.; Fu, Q.; Ren, H.; Yin, Z. Improving Physical Fitness and Cognitive Functions in Middle School Students: Study Protocol for the Chinese Childhood Health, Activity and Motor Performance Study (Chinese CHAMPS). Int. J. Environ. Res. Public Health 2018, 15, 976. [Google Scholar] [CrossRef]
- Black, M.M.; Hager, E.R.; Le, K.; Anliker, J.; Arteaga, S.S.; DiClemente, C.; Gittelsohn, J.; Magder, L.; Papas, M.; Snitker, S.; et al. Challenge! Health Promotion/Obesity Prevention Mentorship Model Among Urban, Black Adolescents. Pediatrics 2010, 126, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Dzewaltowski, D.A.; Estabrooks, P.A.; Welk, G.; Hill, J.; Milliken, G.; Karteroliotis, K.; Johnston, J.A. Healthy Youth Places: A Randomized Controlled Trial to Determine the Effectiveness of Facilitating Adult and Youth Leaders to Promote Physical Activity and Fruit and Vegetable Consumption in Middle Schools. Health Educ. Behav. 2008, 36, 583–600. [Google Scholar] [CrossRef]
- Institute of Medicine. Fitness Measures and Health Outcomes in Youth; National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- Birch, L.; Perry, R.; Hunt, L.P.; Matson, R.; Chong, A.; Beynon, R.; Hamilton-Shield, J. What change in body mass index is associated with improvement in percentage body fat in childhood obesity? A meta-regression. BMJ Open 2019, 9, e028231. [Google Scholar] [CrossRef] [PubMed]
- Tugault-Lafleur, C.N.; Black, J.L.; IBarr, S. A Systematic Review of Methods to Assess Children’s Diets in the School Context. Adv. Nutr. 2017, 8, 63–79. [Google Scholar] [CrossRef] [PubMed]
- Mangieri, H. Fueling Young Athletes; Human Kinetics: Champaign, IL, USA, 2016. [Google Scholar]
- Seebohar, B. Sports Nutrition for Youth Athletes. USA Triathlon. 25 July 2019. Available online: https://www.teamusa.org/USA-Triathlon/News/Blogs/Multisport-Lab/2019/July/25/Sports-Nutrition-for-Youth-Athletes (accessed on 22 September 2020).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).