
Assessment of Risk Factors Associated with Cardiovascular Diseases in Overweight Women

 ,
,  , ,
, ,
Abstract
:1. Introduction
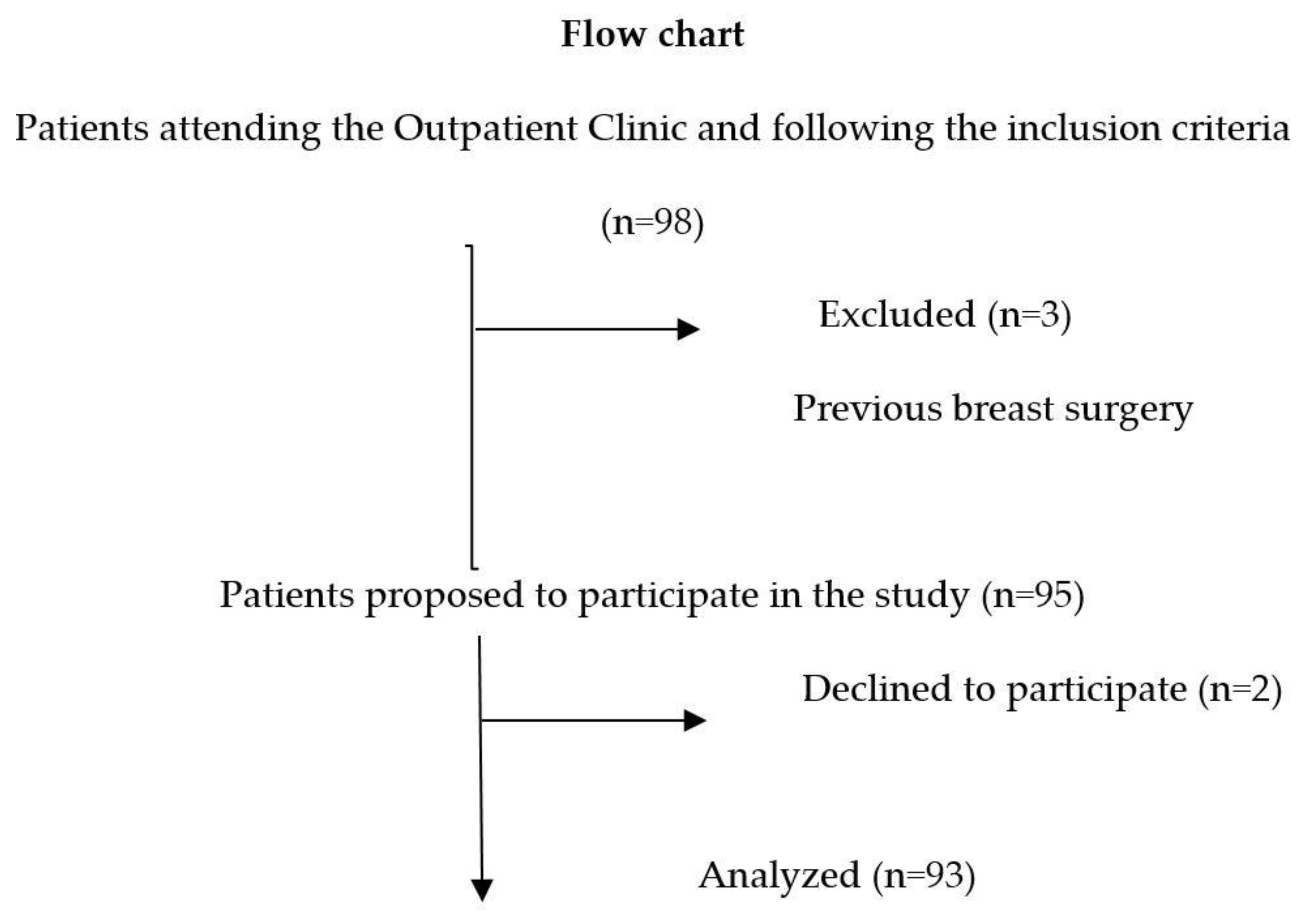
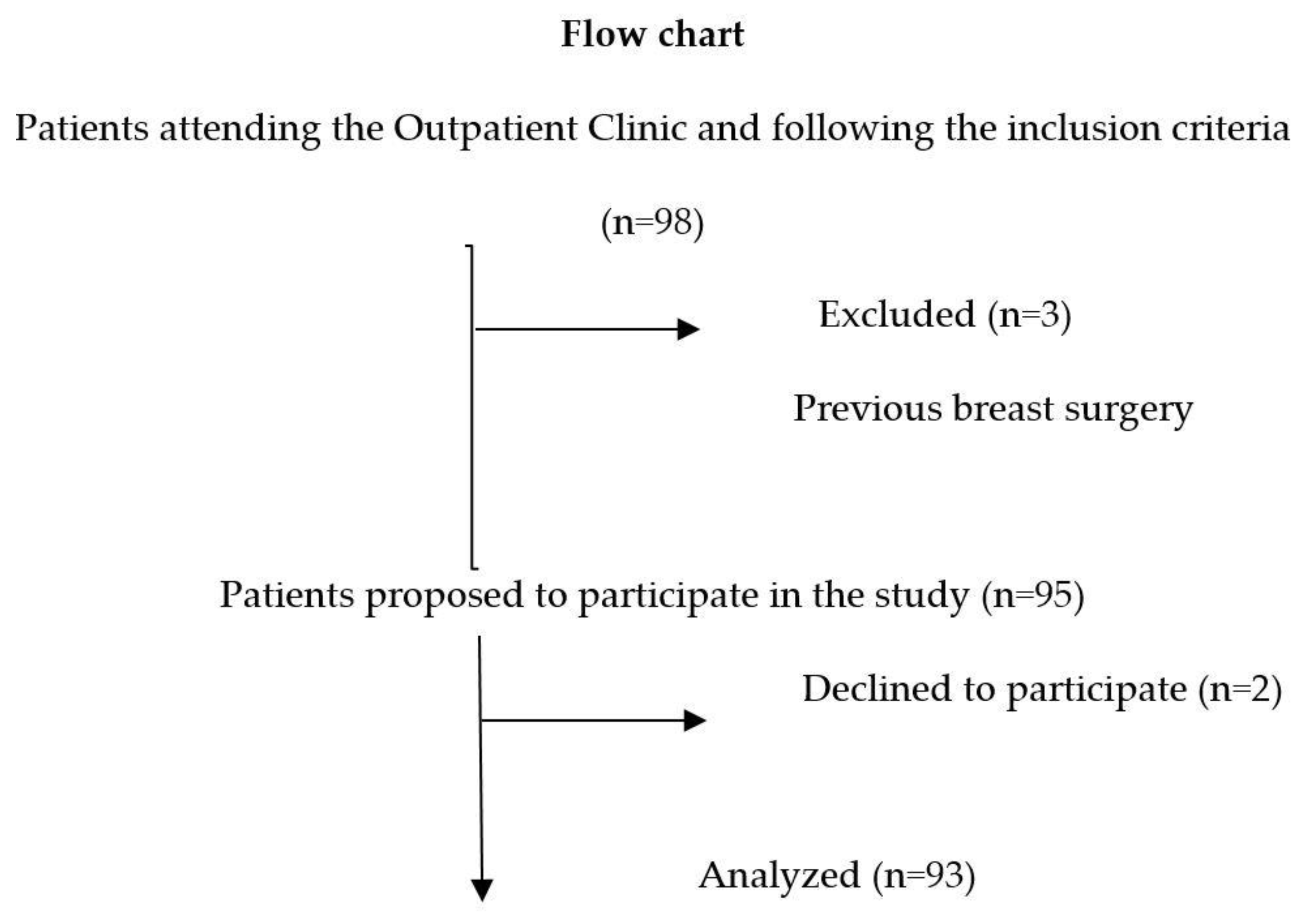
2. Materials and Methods
2.1. Definitions
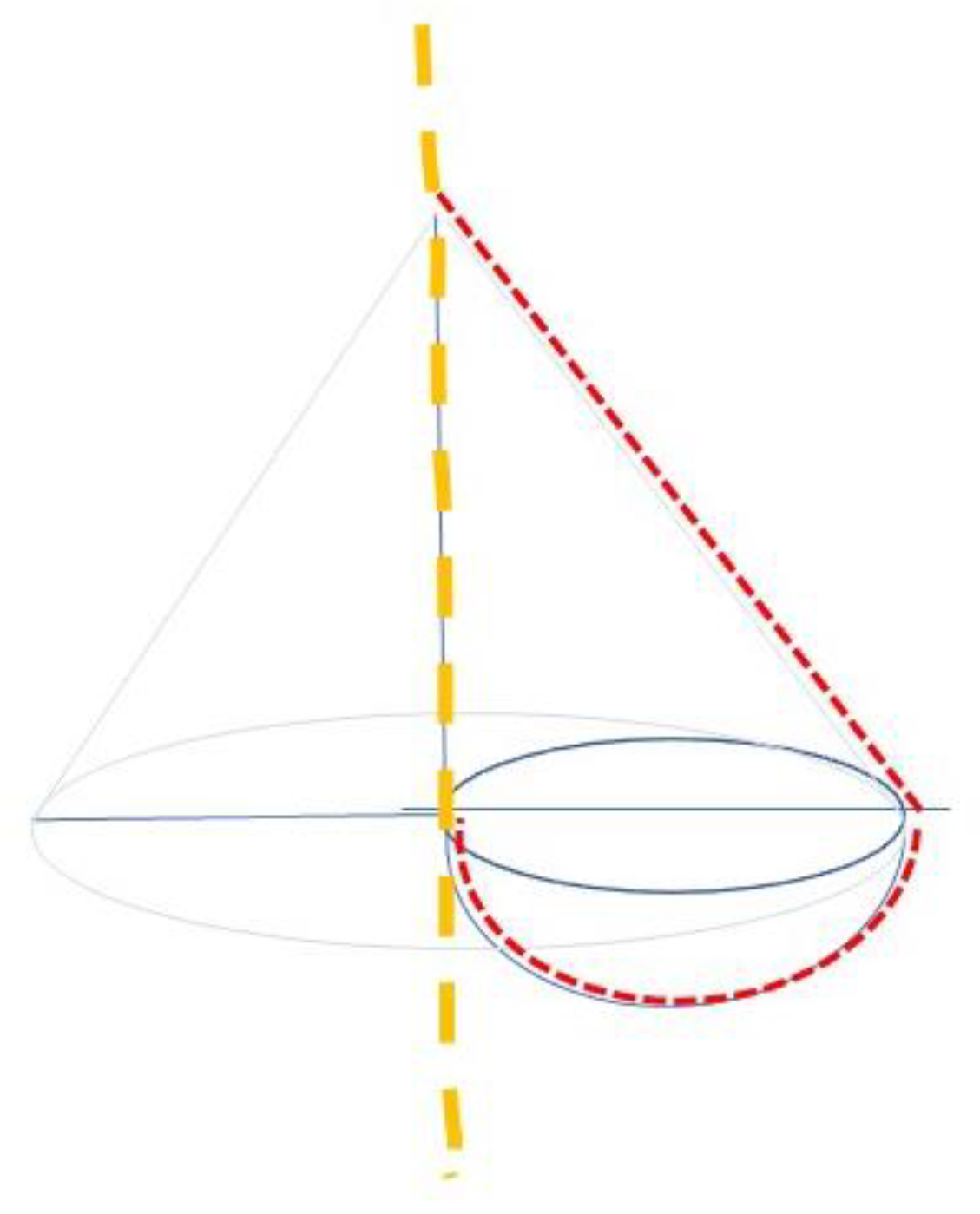
2.2. Analysis of Body Composition
2.3. Variables
2.4. Statistical Analysis
3. Results
3.1. Bioimpedance Analysis
3.2. Cardiovascular Risk Factors Assessment
3.3. Correlation between MV-BMI and Cardiovascular Risk Factors
3.4. Evaluation of MV-BMI or Waist-To-Hip Ratio as Best Anthropometric Predictor of FRS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- González-Muniesa, P.; Mártinez-González, M.A.; Hu, F.B.; Després, J.P.; Matsuzawa, Y.; Loos, R.J.F.; Moreno, L.A.; Bray, G.A.; Martinez, J.A. Obesity. Nat. Rev. Dis. Primers 2017, 3, 17034. [Google Scholar] [CrossRef] [PubMed]
- Van Jaarsveld, C.H.; Gulliford, M.C. Childhood obesity trends from primary care electronic health records in England between 1994 and 2013: Population-based cohort study. Arch. Dis. Child. 2015, 100, 214–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, J.V.S.; Dias, M.M.G.; Brilhante, A.; Terra, M.F.; García-Arévalo, M.; Figueira, A.C.M. Multifactorial Basis and Therapeutic Strategies in Metabolism-Related Diseases. Nutrients 2021, 13, 2830. [Google Scholar] [CrossRef] [PubMed]
- Koliaki, C.; Liatis, S.; Kokkinos, A. Obesity and cardiovascular disease: Revisiting an old relationship. Metabolism 2019, 92, 98–107. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaziano, J.M.; Hennekens, C.H.; O’Donnell, C.J.; Breslow, J.L.; Buring, J.E. Fasting triglycerides, high-density lipoprotein, and risk of myocardial infarction. Circulation 1997, 96, 2520–2525. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Tovar, J.; Oller, I.; Galindo, I.; Llavero, C.; Arroyo, A.; Calero, A.; Diez, M.; Zubiaga, L.; Calpena, R. Change in levels of C-reactive protein (CRP) and serum cortisol in morbidly obese patients after laparoscopic sleeve gastrectomy. Obes. Surg. 2013, 23, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Medina-Inojosa, J.R.; Batsis, J.A.; Supervia, M.; Somers, V.K.; Thomas, R.J.; Jenkins, S.; Grimes, C.; Lopez-Jimenez, F. Relation of Waist-Hip Ratio to Long-Term Cardiovascular Events in Patients With Coronary Artery Disease. Am. J. Cardiol. 2018, 121, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Amirabdollahian, F.; Haghighatdoost, F. Anthropometric Indicators of Adiposity Related to Body Weight and Body Shape as Cardiometabolic Risk Predictors in British Young Adults: Superiority of Waist-to-Height Ratio. J. Obes. 2018, 2018, 8370304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Tovar, J.; Zubiaga, L.; Llavero, C. Mammary Volume-to-Body Mass Index Ratio: Preoperative Predictor of Cardiovascular Risk Factor and Indicator of Long-term Postoperative Remission of Comorbidities in Premenopausal Women Undergoing Sleeve Gastrectomy. Obes. Surg. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Copcu, E. A versatile breast reduction technique: Conical plicated central U shaped (COPCUs) mammaplasty. Ann. Surg. Innov. Res. 2009, 3, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syed-Abdul, M.M.; Soni, D.S.; Barnes, J.T.; Wagganer, J.D. Comparative analysis of BIA, IBC and DXA for determining body fat in American Football players. J. Sports Med. Phys. Fit. 2021, 61, 687–692. [Google Scholar] [CrossRef]
- Brown, N.; White, J.; Milligan, A.; Risius, D.; Ayres, B.; Hedger, W.; Scurr, J. The relationship between breast size and anthropometric characteristics. Am. J. Hum. Biol. 2012, 24, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Coltman, C.E.; Steele, J.R.; McGhee, D.E. Breast volume is affected by body mass index but not age. Ergonomics 2017, 60, 1576–1585. [Google Scholar] [CrossRef] [PubMed]
- Brisken, C.; O’Malley, B. Hormone action in the mammary gland. Cold Spring Harb. Perspect. Biol. 2010, 2, a003178. [Google Scholar] [CrossRef] [PubMed]
- Gierach, G.L.; Patel, D.A.; Falk, R.T.; Pfeiffer, R.M.; Geller, B.M.; Vacek, P.M.; Weaver, D.L.; Chicoine, R.E.; Shepherd, J.A.; Mahmoudzadeh, A.P.; et al. Relationship of serum estrogens and metabolites with area and volume mammographic densities. Horm. Cancer 2015, 6, 107–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iversen, A.; Frydenberg, H.; Furberg, A.S.; Flote, V.G.; Finstad, S.E.; McTiernan, A.; Ursin, G.; Wilsgaard, T.; Ellison, P.T.; Jasienska, G.; et al. Cyclic endogenous estrogen and progesterone vary by mammographic density phenotypes in premenopausal women. Eur. J. Cancer Prev. 2016, 25, 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattioli, A.V.; Sciomer, S.; Moscucci, F.; Maiello, M.; Cugusi, L.; Gallina, S.; Dei Cas, A.; Lombardi, C.; Pengo, M.; Parati, G.; et al. Cardiovascular prevention in women: A narrative review from the Italian Society of Cardiology working groups on ‘Cardiovascular Prevention, Hypertension and peripheral circulation’ and on ‘Women Disease’. J. Cardiovasc. Med. 2019, 20, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Janiszewski, P.M.; Saunders, T.J.; Ross, R. Breast volume is an independent predictor of visceral and ectopic fat in premenopausal women. Obesity 2010, 18, 1183–1187. [Google Scholar] [CrossRef] [PubMed]
- Steele, J.R.; Coltman, C.E.; McGhee, D.E. Effects of obesity on breast size, thoracic spine structure and function, upper torso musculoskeletal pain and physical activity in women. J. Sport Health Sci. 2020, 9, 140–148. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Waist circumference (cm) | 80.6 ± 9.6 |
| Hip circumference (cm) | 101.7 ± 10.2 |
| Waist-to-hip ratio | 0.8 ± 0.07 |
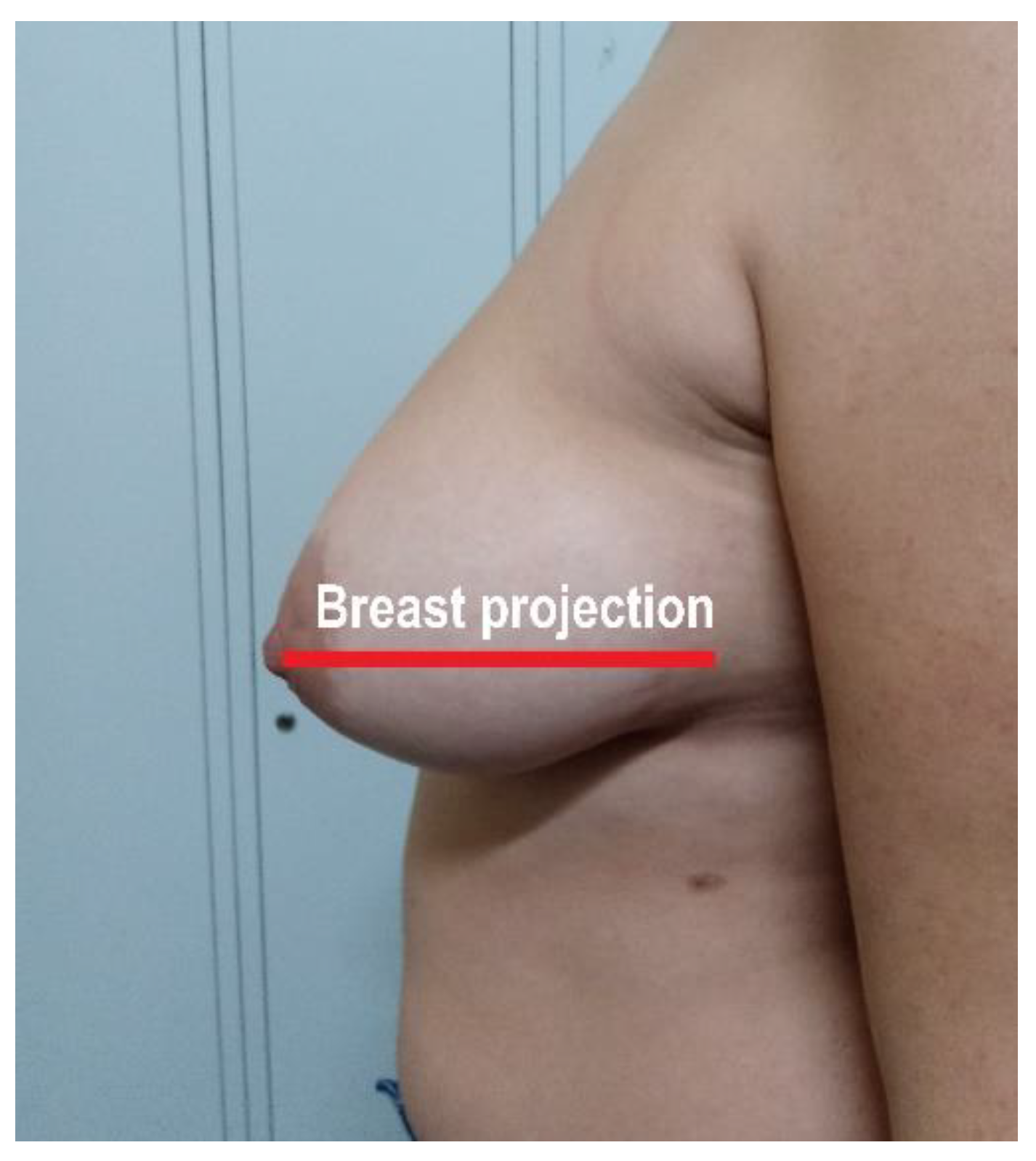
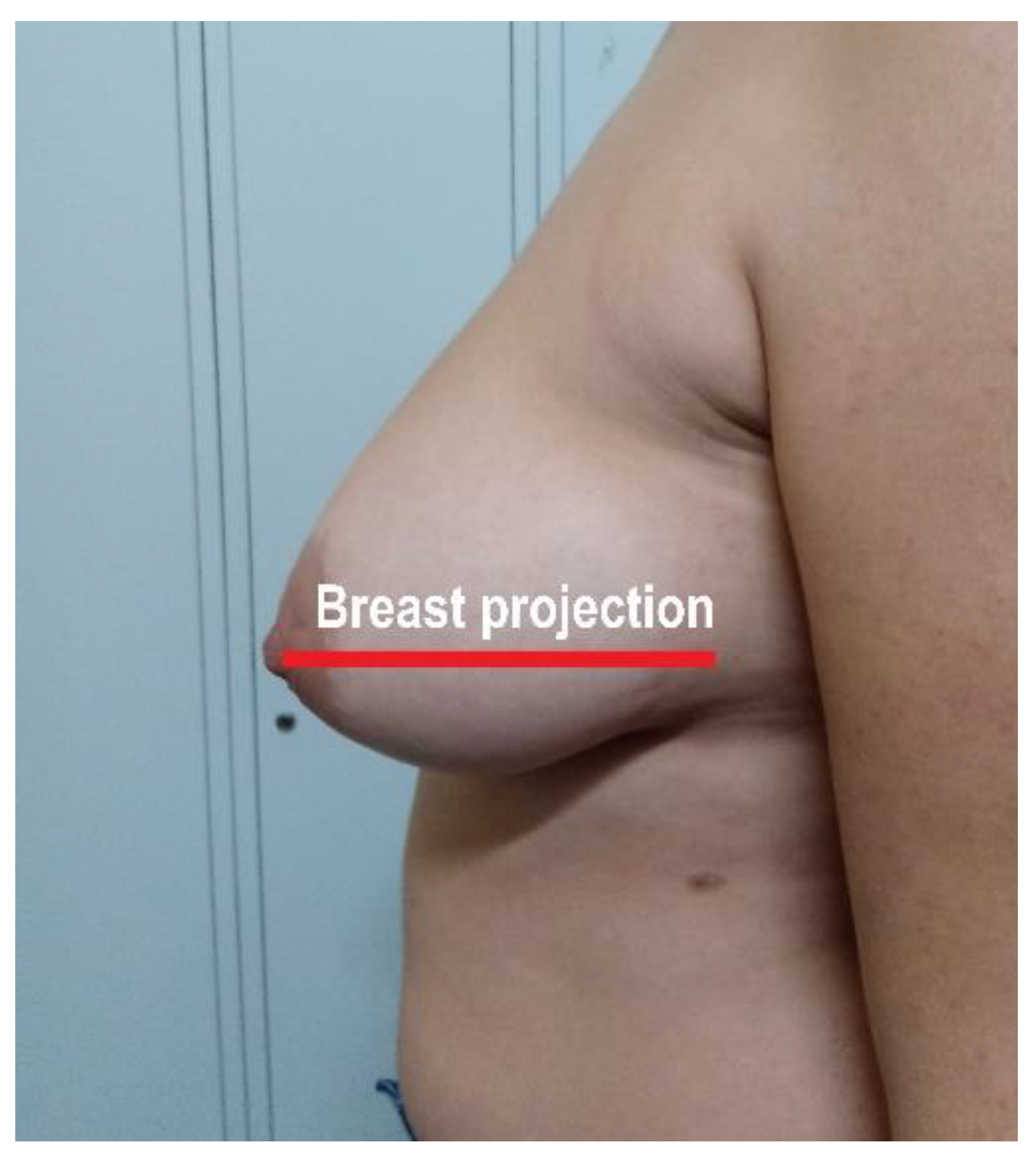
| Mammary projection (cm) | 18.8 ± 3.6 |
| Ptosis (cm) | 17.1 ± 7.3 |
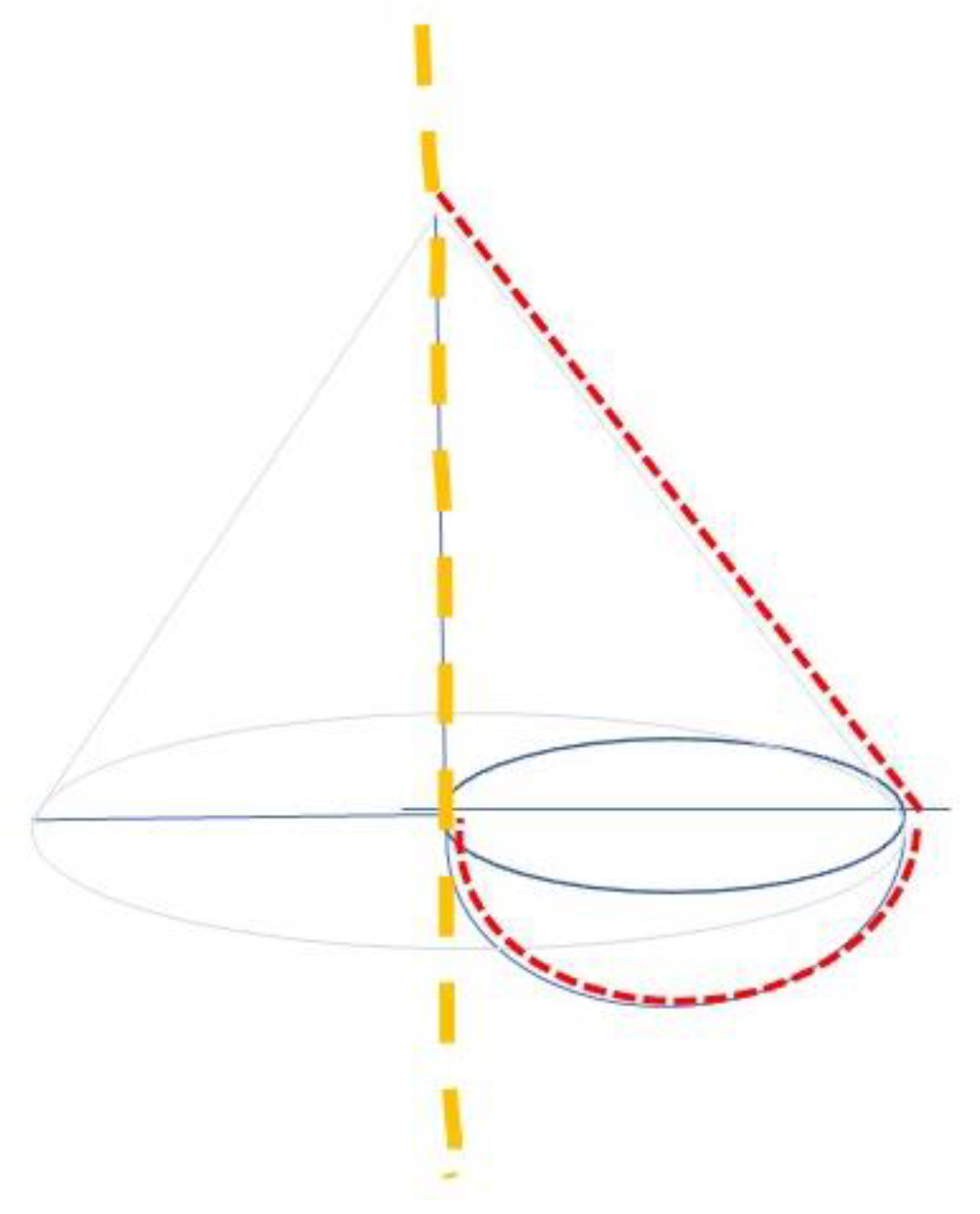
| Mammary volume (cm3) | 1045 ± 657.4 |
| Mammary volume/BMI ratio (cm3/(kg/m2) | 38.4 ± 24.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro, M.-J.; Jiménez, J.-M.; López, M.; Cao, M.-J.; Durán, M.; Albertos, I.; García, S.; Ruiz-Tovar, J. Assessment of Risk Factors Associated with Cardiovascular Diseases in Overweight Women. Nutrients 2021, 13, 3658. https://doi.org/10.3390/nu13103658
Castro M-J, Jiménez J-M, López M, Cao M-J, Durán M, Albertos I, García S, Ruiz-Tovar J. Assessment of Risk Factors Associated with Cardiovascular Diseases in Overweight Women. Nutrients. 2021; 13(10):3658. https://doi.org/10.3390/nu13103658
Chicago/Turabian StyleCastro, María-José, José-María Jiménez, María López, María-José Cao, Manuel Durán, Irene Albertos, Sara García, and Jaime Ruiz-Tovar. 2021. "Assessment of Risk Factors Associated with Cardiovascular Diseases in Overweight Women" Nutrients 13, no. 10: 3658. https://doi.org/10.3390/nu13103658
APA StyleCastro, M.-J., Jiménez, J.-M., López, M., Cao, M.-J., Durán, M., Albertos, I., García, S., & Ruiz-Tovar, J. (2021). Assessment of Risk Factors Associated with Cardiovascular Diseases in Overweight Women. Nutrients, 13(10), 3658. https://doi.org/10.3390/nu13103658