1. Introduction
Intrauterine growth retardation (IUGR) and small for gestational age (SGA) are associated with intrauterine foetal death [
1], cerebral palsy [
2], perinatal acidosis, hypoglycaemia, hypothermia, and coagulation abnormalities [
3]. Later in life, SGA born children are at higher risk of short stature, cognitive delays, diabetes and cardiovascular disease [
3,
4,
5,
6]. Some risk factors for having a baby born SGA, such as maternal smoking, maternal weight (very low and also increased body mass index) and primiparity, have been identified [
7,
8,
9,
10]. In addition, a number of dietary factors have been associated with SGA, such as diet quality/unhealthy dietary patterns [
11,
12,
13], high sugar consumption in pregnancy [
14], low consumption of seafood [
15,
16], low iodine intake [
17], and caffeine consumption [
18,
19]. A review on the impact of maternal diet during pregnancy on infant birth weight found that consumption of whole foods such as fruit, vegetables, low-fat dairy, and lean meats throughout pregnancy may be beneficial for appropriate birth weight in relation to gestational age [
20]. Studies examining associations between maternal/neonatal trace element concentrations during pregnancy and SGA status found selenium concentration, but not iron, zinc, copper, cadmium or lead, to be significantly associated with the risk of being born SGA [
21,
22,
23].
Selenium is a trace element which is incorporated into selenoproteins. Examples of important selenoproteins are the key antioxidative enzyme glutathione peroxidase and the iodothyronine deiodinases D1, D2, and D3, each containing selenium at their active sites [
24]. Glutathione peroxidase has a major impact on redox status and regulates oxidative stress, while the iodothyronine deiodinases have key roles in regulating circulating and intracellular levels of thyroid hormones [
25]. We have previously reported that maternal dietary selenium intake is associated with a small but significant decrease in the risk of preterm delivery and an increase in gestational duration [
26]. There are also studies suggesting that maternal blood selenium status before or during pregnancy correlates positively with birth weight [
23,
27].
The aim of this study was to examine whether maternal intake of selenium and maternal whole blood selenium concentration in mid-pregnancy are associated with birth weight and SGA in a large Norwegian pregnancy cohort.
4. Discussion
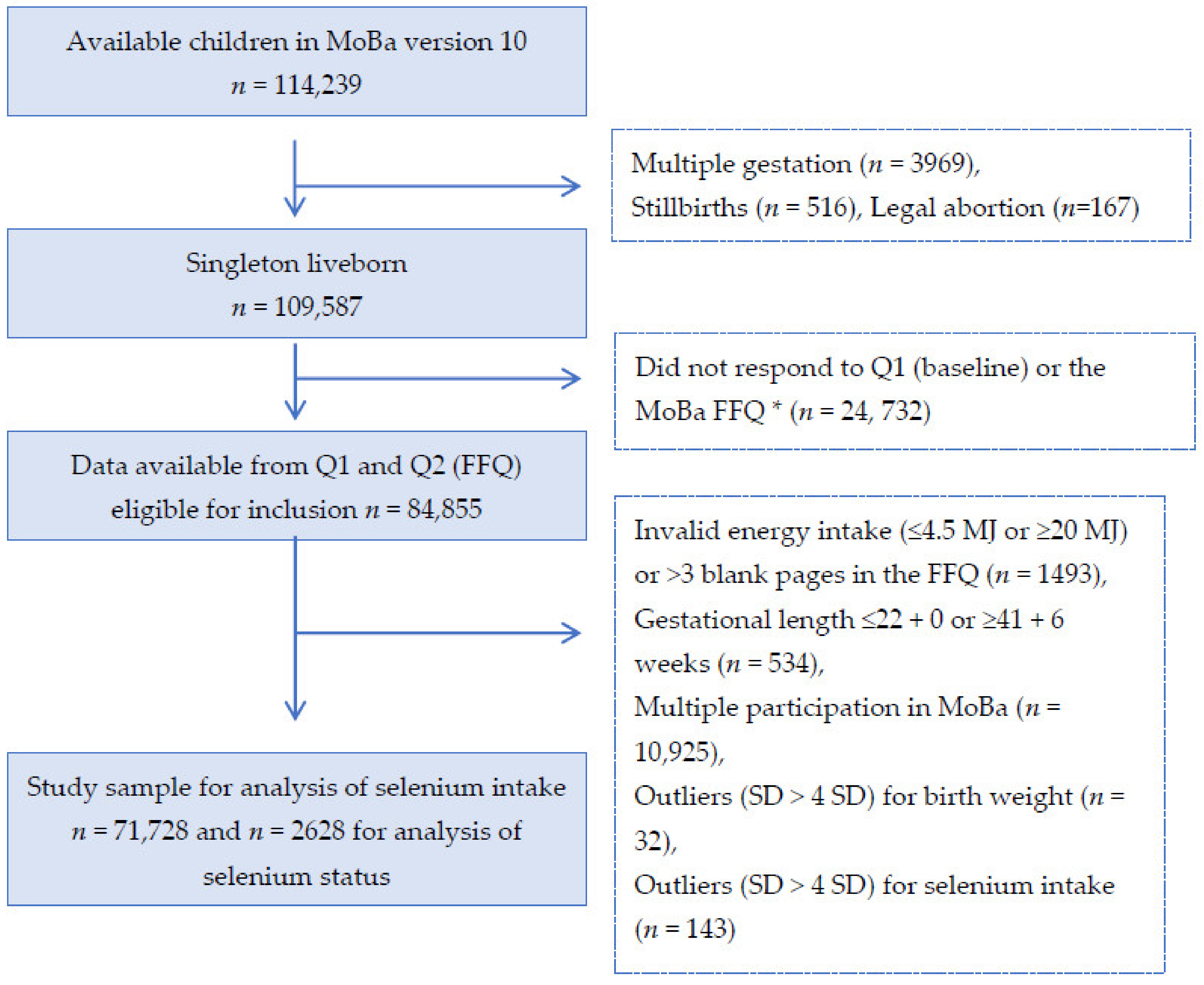
In this study including 71,728 pregnant women, maternal dietary intake of selenium during the first half of pregnancy was weakly associated with increased birth weight (12 g per SD of selenium intake in the adjusted models) and with decreased risk of the child being born SGA (9% decrease per SD of selenium intake). However, maternal selenium intake from supplements in 71,728 mothers and whole blood selenium in 2628 mothers were not associated with birth weight or with SGA.
Foetal growth is dependent on nutrients transported from the maternal to the foetal circulation across the placenta. The transport of small membrane permeable molecules such as oxygen and carbon dioxide is influenced mainly by umbilical blood flow and placental structure, while larger molecules such as amino acids, fatty acids and glucose are dependent on nutrient transport proteins [
47]. The nutrient transport capacity of the placenta is influenced by numerous factors, including hormones, nutrient levels and placental function [
48]. Furthermore, oxidative stress in the placenta has been shown to influence the transport of nutrients through altering the gene expression of different nutrient transporters (e.g., glucose and amino acid) [
49,
50]. In vitro studies have shown that selenium supplementation protects placental cells from oxidative stress through increased expression of selenium-containing antioxidants, such as glutathione and thioredoxin reductase [
51]. Hence, one of the leading hypotheses regarding how selenium may affect foetal growth is through the selenium-dependent antioxidative defence system [
49,
50,
51,
52].
Other selenium-dependent proteins are the iodothyronine deiodinase (DIOs) that are involved in thyroid hormones metabolism [
53]. Thyroid hormones are essential in regulating placental nutrient transport, for example, hyperthyroidism is known to reduce circulating glucose in foetal tissues [
54]. Hence, another hypothesis on how selenium may influence foetal growth is through regulating the levels of thyroid hormones. In line with this, mice fed a diet low in selenium had increased levels of both maternal and foetal plasma levels of the thyroid hormones triiodothyronine (T3) and tetraiodothyronine (T4) [
49]. In humans, studies have found lipid peroxidation and oxidative stress to be associated with children being born SGA [
55,
56]. In one of the studies, SGA born children had lower levels of reduced glutathione (indicating deficient antioxidant defence mechanisms) but higher concentration of the lipid peroxidation malondialdehyde [
56].
Previous observational studies analysing the association between selenium status and birth weight or SGA births have mainly focused on selenium concentration in maternal serum, plasma or blood samples, collected either before or during pregnancy [
22,
23,
27] or at delivery [
57,
58,
59,
60,
61]. To the best of our knowledge, no study has investigated the association between maternal dietary intake of selenium and birth weight. Previous studies have suggested that maternal selenium status during pregnancy, but not at delivery, correlates positively with birth weight. A nested case-control study within the US Camden Study, with preterm delivery as the main outcome, found selenium status at around 16 weeks of gestation to be positively associated with birth weight in infants born at term (
n = 126), but not in infants born preterm (
n = 107) [
27]. Another study performed in Japan on 44 newborn infants, including maternal serum samples collected around entry to antenatal care, found maternal selenium status during pregnancy to be positively associated with higher birth weight [
23]. A UK study on 126 adolescent pregnancies found selenium concentration in plasma collected at around 30 weeks of gestation to be associated with higher birth weight scores and with a lower risk of SGA [
22]. These suggested positive associations between maternal selenium status and birth weight were not supported in the sub-sample in the current study, where selenium status was not associated with birth weight or SGA. We had information about selenium status in a fairly small subgroup of the women (3.7%). Still, the current study is far larger than previous studies. One obvious difference between our study and the previous studies is that we used selenium analysed in whole blood, while the three other studies used selenium analysed in serum or plasma. Whole blood selenium concentration reflects both status and uptake while plasma/serum selenium only reflects short-term status [
46]. Hence, the difference in specimen used for selenium analyses may be one explanation for the different results between the current and previous studies. In the current study, median selenium status was close to the reference level of 100 µg/L [
46,
62].
Possible reasons for why only selenium intake from diet but not from supplements was associated with birth weight and SGA in this study can only be speculated on. One reason may be that the women in this cohort have intake levels from diet close to the level associated with optimal selenoprotein expression and adding further selenium intake from supplements does not give further improvement in selenoprotein expression. Another reason might be related to the difficulty in accurately measuring the intake of nutrients contributed from dietary supplements. Dietary intakes are often more stable over time while intake from supplements may vary more, especially during pregnancy when many women care more about their nutritional intake [
63,
64]. One additional explanation is that dietary selenium intake may serve as a proxy for a high quality diet containing other factors that have a beneficial effect on birth weight. As we state in the introduction, for example, high sugar consumption [
14], low fish intake [
15,
16], low iodine intake [
17], and high caffeine consumption [
18,
19] have previously been associated with the risk of being born SGA. However, we adjusted our models for fibre intake as a proxy for an overall healthy diet, iodine intake, protein intake and n-3 intake from diet. After adjusting for these and other factors, the effect size was somewhat reduced for selenium intake association with birth weight but not for SGA. Hence, even if we cannot rule out that dietary intake of selenium is a proxy for another dietary factor that correlates with the intake of selenium, we believe that the size of our study, allowing us to adjust for very many factors including markers for overall food quality, strengthens the validity of our results. A possible explanation for the lack of association between blood selenium and birth weight may be that the sub-population with available blood selenium was rather homogenous and had fairly good selenium status.
The main strength of this study is its large sample size. The study is by far the largest examining selenium intake from both diet and supplements and whole blood selenium concentration in relation to birth weight and SGA. Another strength of the current study is its prospective design with selenium intake assessment during the first half of pregnancy and with maternal blood collected in mid-pregnancy, since previous studies suggest that maternal selenium status during pregnancy, but not at delivery, is associated with birth weight [
22,
23,
27,
57,
58,
59,
60,
61].
Another strength is the population-based study design, including women from all over Norway representing women living in different areas and regions, from different socioeconomic groups and women with diverse dietary habits. Another strength is the extensive data from questionnaires and the linkage to MBRN allowing us to control for important covariates.
Still, our study is limited by the observational design and the inherent risk of residual confounding. There is also a potential influence of self-selection bias as for all cohort studies. The participation rate in MoBa was 41%; women participating in MoBa are generally healthier and better educated than the general population of pregnant Norwegian women [
28].
In the main analyses, we used the birth weight z-score variable that was extracted directly from MBRN. To make the results more comparable to those from other parts of the world, we analysed z-scores of birth weight and SGA according to different growth standards. The findings for the association between maternal dietary selenium intake during pregnancy and higher birth weight and lower risk for SGA were consistent and of similar size when using the different growth standards as shown in the(
Supplementary Files).
The subgroup of women with data on selenium concentration in whole blood was included in the Norwegian Environmental Biobank Study, where two of the inclusion criteria for participation was to have answered the first six MoBa questionnaires and to have provided biological samples. Hence, this subgroup with selenium measurements does not represent the whole MoBa population, but a highly selected group. The women in this subgroup included a higher proportion of non-smokers and highly educated compared with those in the whole MoBa [
34]. Thus, a limitation with the current study is that the generalizability of the selenium blood status may be compromised due to selection bias. In addition, while we did not identify any association between whole blood selenium and birth weight or SGA, we cannot rule out that smaller effect estimates might be detected if a larger and more varied study population with broader variation in selenium concentration was available.
The dietary intake of selenium was estimated during pregnancy using an FFQ specifically developed and validated for use in the MoBa cohort [
29,
31]. All dietary assessment methods have errors. The use of an FFQ to assess diet has limitations since it is imprecise and prone to misreporting. Since the selenium content varies according to the selenium concentration of the soil where crops are grown or the animals graze, it is especially difficult to assess selenium intake from food composition databases. This difficulty is reflected in the low correlation between selenium intake from diet and selenium concentration in blood reported previously (Spearman rho: 0.135 95% CI: 0.10, 0.17) [
26]. However, blood selenium concentration is influenced by homeostatic regulation and by individual differences in absorption, metabolism and body composition. In the validation study, selenium intake estimated with the FFQ was significantly correlated with selenium intake estimated using a 4-day food diary, but the correlation coefficient was low (Spearman’s rho 0.33 (95%CI: 0.16, 0.48)) [
32].


 ,
, 


{kind=link}
{kind=link}