Current Data on Dietary Sodium, Arterial Structure and Function in Humans: A Systematic Review

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Selection of Studies and Data Extraction
3. Results
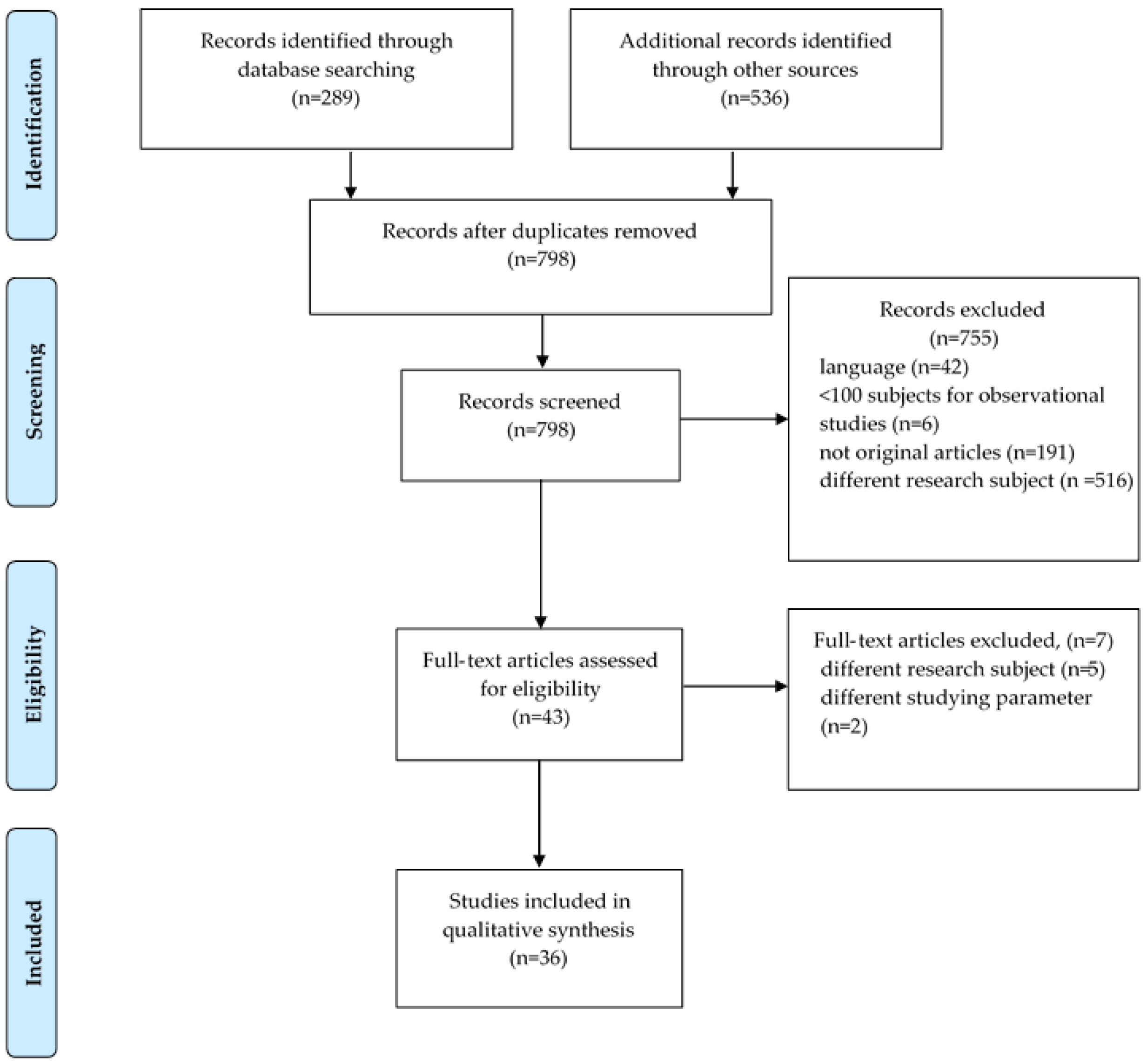
3.1. Number of Studies Screened and Selected
3.2. Description of Studies
3.2.1. Studies Investigating Arteriosclerosis (Arterial Stiffness)
Observational Studies
Interventional Studies
3.2.2. Studies Investigating Arterial Remodeling
Observational Studies
Interventional Studies
3.2.3. Studies Investigating Atheromatosis
4. Discussion
4.1. Na and Arteriosclerosis
4.2. Na and Arterial Remodeling
4.3. Na and Atheromatosis
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. PRISMA Checklist
| TITLE | |||
| Title | 1 | Identify the report as a systematic review, meta-analysis, or both. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. | 1,2 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). | 1,2 |
| METHODS | |||
| Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (e.g., web address), and, if available, provide registration information including registration number. | Not applicable |
| Eligibility criteria | 6 | Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale. | 2 |
| Information sources | 7 | Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. | 2 |
| Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | 2,3 |
| Study selection | 9 | State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis). | 3 |
| Data collection process | 10 | Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators. | 2 |
| Data items | 11 | List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made. | 2 |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis. | Not applicable |
| Summary measures | 13 | State the principal summary measures (e.g., risk ratio, difference in means). | - |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. | Not applicable |
| Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies). | Not applicable |
| Additional analyses | 16 | Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified. | Not applicable |
| RESULTS | |||
| Study selection | 17 | Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram. | 3 |
| Study characteristics | 18 | For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. | 4–15 |
| Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). | Not applicable |
| Results of individual studies | 20 | For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot. | Not applicable |
| Synthesis of results | 21 | Present results of each meta-analysis done, including confidence intervals and measures of consistency. | Not applicable |
| Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see Item 15). | Not applicable |
| Additional analysis | 23 | Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]). | Not applicable |
| DISCUSSION | |||
| Summary of evidence | 24 | Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers). | 15,16 |
| Limitations | 25 | Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias). | 18,19 |
| Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence, and implications for future research. | 18,19 |
| FUNDING | |||
| Funding | 27 | Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review. | 19 |
Appendix B. Population Description and Exclusion Criteria of Selected Studies
| Arteriosclerosis—Observational Studies | ||
| cfPWV | ||
| 1. Observational Cross-Sectional Studies | ||
| Author (year) | Population Description | Exclusion Criteria |
| Polónia, J. (2006) | essential hypertensives, recent stroke or healthy university students | urine sample not meeting the required quality criteria |
| García-Ortiz, L. (2012) | primary care patients aged 30–80 | cardiovascular and/or cerebrovascular disease |
| Kotliar, C. (2014) | essential hypertensives, aged 30 to 70 | abnormal renal function; volume or electrolyte alterations; diabetes mellitus; history of renal disease, ischemic heart disease, stroke; loss of data; counter indication for the drug washout; use of corticoids or nonsteroidal anti-inflammatory drugs during the study |
| Polonia, J. (2016) | hypertensive adults | secondary hypertension, previous cardiovascular events history; estimated glomerular filtration rate >50 mL/min/1.73 |
| Strauss, M. (2018) | normotensive adults | previously diagnosed chronic illness (self-reported); use of anti-hypertensive drugs or other chronic diseases; diabetes mellitus; HIV infected; microalbuminuria>30 mg/mL; pregnancy or lactation |
| Triantafyllou, A. (2018) | newly diagnosed & never-treated hypertensives—healthy individuals admitted for regular check-up | previously treated with anti-hypertensive drugs; use of any kind of drugs; other known health problems; secondary causes of hypertension; other comorbidities (e.g., diabetes mellitus, CVD) |
| 2. Observational Studies with Follow up (>1 Time Points) | ||
| Nerbass, F.B. (2015) | adults in CKD stage 3 | solid organ transplant or terminally illness |
| Aortic PWV Other Than cfPWV | ||
| Siriopol, D. (2018) | hypertensive & normotensive Romanian adults | use of diuretic treatment; CKD; missing values for the variables of interest |
| baPWV | ||
| 1. Observational Cross-Sectional Studies | ||
| Sonoda, H. (2012) | healthy subjects | heart failure; valvular heart disease; atrial fibrillation; peripheral artery disease |
| Lee, S.K. (2015) | non-hypertensive subjects, with no use of anti-hypertensive drugs | age >70 years; preexisting CVD including significant valvular heart diseases and arrhythmia; chronic renal disease or a serum creatinine level >1.5 mg/dL; unavailable urinary Na data, inadequate data of tissue Doppler echocardiography, carotid ultrasound, or baPWV; ejection fraction of <55% after echocardiography |
| Sun, N. (2015) | newly diagnosed hypertensives, untreated hypertensives or patients with a 1 to 5 year history of hypertensives who had stopped taking anti-hypertensive drugs for 1 month | use of anti-hypertensive drugs; secondary hypertension; hypertensive emergency; hypertensive urgency; acute coronary syndrome; severe arrhythmias; DM; stroke; CKD |
| Han, W. (2017) | hypertensive adults | any secondary cause of hypertension; hypertension emergencies; serious arrhythmia; peripheral arterial disease; heart failure; impaired renal function with plasma creatinine ≥150 μmol/L; rheumatic & autoimmune diseases; malignancies |
| 2. Observational Studies with Follow up (>1 Time Points) | ||
| Jung, S. (2019) | adults aged >40 | history of heart disease, stroke, and/or cancer; anti-hypertensive drugs; diabetes mellitus; dyslipidemia; implausible dietary intake reported (< 500 or > 4000 kcal/day); missing general characteristic data from the baseline visit |
| Common Carotid Arterial Elasticity (Young’s Elastic Modulus, Stiffness Index, Arterial Compliance) | ||
| Ferreira-Sae, M.C. (2011) | hypertensive adults | age <18 years; neoplastic disease; secondary hypertension |
| Arteriosclerosis—Interventional studies | ||
| cfPWV | ||
| Seals, D.R. (2001) | postmenopausal women, ≥50 years, high normal SBP or Stage 1 hypertension | anti-hypertensive drugs; other chronic disease; low-Na diet or regular exercise during the preceding 2 years; smoking |
| Dickinson, K.M. (2009) | overweight/obese, mild hypertensive adults | metabolic disease; CVD; SBP >160 mm Hg at screening; significant weight loss in the preceding 6 months (>2 kg); BMI < 27 or > 40; use of anti-hypertensive drugs |
| He, F.J. (2009) | hypertensive adults | anti-hypertensive drugs; secondary cause of hypertension; impaired renal function; previous stroke; ischemic heart disease; heart failure; diabetes mellitus; malignancy; liver disease; pregnancy or lactation or on oral contraceptive pills |
| Pimenta, E. (2009) | resistant hypertensive adults on stable anti-hypertensive drugs | history of atherosclerotic disease (in the previous 6 months); congestive heart failure; diabetes mellitus on insulin treatment; office blood pressure > 160/100 mm Hg |
| Todd, A.S. (2010) | Pre-hypertensive or hypertensive, non-obese adults or in anti-hypertensive drugs | age >65; smoking; history of CVD or diabetes mellitus or renal disease |
| Todd, A.S. (2012) | normotensives, non-obese adults | age >65; antihypertensive medication; smoking; history of cardiovascular disease or diabetes mellitus or renal disease |
| McMahon, E.J. (2013) | hypertensive adult patients with stage 3 or 4 CKD (GFR 15–59 mL/min per 1.73 m2), non-dialyzed, non-transplanted | salt-wasting CKD, pregnant or breastfeeding, current prescription of medications providing 0.20 mmol sodium per day, life expectancy,6 months, current involvement in another intervention study, or insufficient mental or physical capacity to adhere to the study protocol. |
| Dickinson, K.M. (2014) | overweight or obese subjects | diabetes mellitus; dyslipidemia; inflammatory bowel disease; pulmonary disease or vasculitis |
| Gijsbers, L. (2015) | untreated prehypertensives, aged 40–80 | smoking; diabetes mellitus, CVD; gastrointestinal, liver or renal diseases; BMI > 40; use of drugs known to affect the cardiovascular system; use of nutritional supplements, an energy-restricted or medically prescribed diet; unstable body weight in past 2 months; alcohol use over 21 (women) or 28 (men) consumptions/week; pregnancy or lactation |
| Suckling, F.J. (2016) | untreated hypertensive adults with diet-controlled type 2 diabetes mellitus or impaired glucose tolerance | any secondary causes of hypertension, impaired renal function (plasma creatinine >150 μmol), uncontrolled heart failure, ischemic heart disease, previous stroke, active malignancy or liver disease, pregnancy, breast feeding, or oral contraceptive drugs |
| van der Graaf, A.M. (2016) | women with history of preeclampsia or history of healthy former pregnancy | renal disease; diabetes mellitus or a history of gestational diabetes; obesity; use of anti-hypertensive drugs; pregnancy; lactation; postmenopausal status; use of oral contraceptives |
| Muth, B.J. (2017) | healthy, normotensive adults | history of hypertension; CVD; malignancy; diabetes mellitus; renal impairment; obesity; smoking |
| Aortic PWV (Other than cfPWV) | ||
| Avolio, A.P. (1986) | healthy normotensive adults & children | N/AV |
| hfPWV | ||
| Rhee, M.Y. (2016) | normotensive & hypertensive adults | stage 2 and 3 hypertension; secondary hypertension; angina pectoris; myocardial infarction; congestive cardiac failure; stroke; diabetes mellitus; CKD |
| baPWV | ||
| Wang, Y. (2015) | mild hypertensive adults | stage 2 hypertension; history of clinical CVD; CKD; diabetes mellitus; use of anti-hypertensive drugs; high alcohol intake |
| Arterial Elasticity (Arterial Compliance) | ||
| Creager, M.A. (1991) | normotensive men | hematologic, renal, or hepatic dysfunction |
| Gates, P.E. (2004) | hypertensive adults (stage 1), older than 50 | use of anti-hypertensive drugs; abnormal blood chemistry; positive ECG-monitored exercise test; ankle–brachial index > 0.9; presence of plaque on ultrasound interrogation of the carotid and femoral arteries; smoking for previous 2 years; BMI < 35; consumption of a low-Na diet; not in postmenopausal if female (amenorrheic for at least 2 years) |
| Arterial Remodeling—Observational Studies | ||
| cIMT | ||
| 1. Observational Cross-Sectional Studies | ||
| Ferreira-Sae, M.C. (2011) | hypertensive adults | age <18 years; neoplastic disease; secondary hypertension |
| Njoroge, J.N. (2011) | overweight or obese, physically inactive adults | diabetes mellitus; anti-hypertensive drugs or average baseline SBP of ≥140 or DBP ≥ 90 mmHg; cholesterol lowering or anti-psychotic or vasoactive drugs; use of vasoactive devices; pregnancy or lactation |
| García-Ortiz, L. (2012) | primary care patients aged 30–80 | cardiovascular and/or cerebrovascular disease |
| Lee, S.K. (2015) | non-hypertensive individuals, with no use of anti-hypertensive drugs | age >70 years; preexisting CVD including significant valvular heart diseases and arrhythmia; chronic renal disease or a serum creatinine level > 1.5 mg/dL; unavailable urinary Na data, inadequate data of tissue Doppler echocardiography, carotid ultrasound, or baPWV; ejection fraction of <55% after echocardiography |
| Ustundag, S. (2015) | ambulatory adult patients, in stage 2–4 CKD | BMI < 35 kg/m2; diabetes mellitus; salt-losing nephropathy or history of malignancy or cardio-cerebrovascular disease or any acute disease |
| Dai, X.W. (2016) | Asian adults, via subject referral and community advertisement | hospital-confirmed diabetes mellitus; CVD; renal failure; CKD; cancer |
| Mazza, E. (2018) | adults aged ≥65, not suffering from any debilitating diseases | history of CVD or thyroid dysfunction or excessive alcohol consumption; use of dietary supplements & psychotropic drugs |
| 2. Observational studies with follow up (>1 time points) | ||
| Jung, S. (2019) | adults aged >40 | history of heart disease, stroke, and/or cancer; anti-hypertensive drugs; diabetes mellitus; dyslipidemia; implausible dietary intake reported (< 500 or > 4000 kcal/day); missing general characteristic data from the baseline visit |
| Arterial Remodeling—Interventional Studies | ||
| Right Branchial Artery & Common Carotid Artery Diameter | ||
| Benetos, A. (1992) | actively working, mild to moderate hypertensive adults | cardiac, neurologic or renal involvement or arteriosclerosis obliterans of the lower limbs |
| Atheromatosis—Observational Studies | ||
| Carotid Plaques | ||
| Dai, X.W. (2016) | Asian adults, via subject referral and community advertisement | hospital-confirmed diabetes mellitus; CVD; renal failure; CKD; cancer |
| Mazza, E. (2018) | adults aged ≥65, not suffering from any debilitating diseases | history of CVD or thyroid dysfunction or excessive alcohol consumption; use of dietary supplements & psychotropic drugs |
| Abbreviations: CKD: chronic kidney disease; CVD: cardiovascular disease; BMI: body mass index; Na: Sodium; N/AV: not available. | ||
References
- Lorenz, M.W.; Sitzer, M.; Markus, H.S.; Bots, M.L.; Rosvall, M. Prediction of clinical cardiovascular events with carotid intima-media thickness: A systematic review and meta-analysis. Circulation 2007, 115, 459–467. [Google Scholar] [CrossRef]
- Nambi, V.; Chambless, L.; He, M.; Folsom, A.R.; Mosley, T.; Boerwinkle, E.; Ballantyne, C.M. Common carotid artery intima-media thickness is as good as carotid intima-media thickness of all carotid artery segments in improving prediction of coronary heart disease risk in the Atherosclerosis Risk in Communities (ARIC) study. Eur. Heart J. 2012, 33, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Vlachopoulos, C.; Xaplanteris, P.; Aboyans, V.; Brodmann, M.; Cífková, R.; Cosentino, F.; De Carlo, M.; Gallino, A.; Landmesser, U.; Laurent, S.; et al. The role of vascular biomarkers for primary and secondary prevention. A position paper from the European Society of Cardiology Working Group on peripheral circulation: Endorsed by the Association for Research into Arterial Structure and Physiology (ARTERY) Society. Atherosclerosis 2015, 241, 507–532. [Google Scholar] [PubMed]
- Powles, J.; Fahimi, S.; Micha, R.; Khatibzadeh, S.; Shi, P.; Ezzati, M.; Engell, R.E.; Lim, S.S.; Danaei, G.; Mozaffarian, D.; et al. Global, regional and national sodium intakes in 1990 and 2010, a systematic analysis of 24h urinary sodium excretion and dietary surveys worldwide. BMJ Open 2013, 3, e003733. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guideline: Sodium Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2012. [Google Scholar]
- Mozaffarian, D.; Singh, G.M.; Powles, J. Sodium and cardiovascular disease. N. Engl. J. Med. 2014, 371, 2138–2139. [Google Scholar]
- Strazzullo, P.; D’Elia, L.; Kandala, N.B.; Cappuccio, F.P. Salt intake, stroke, and cardiovascular disease: Meta-Analysis of prospective studies. BMJ 2009, 339, b4567. [Google Scholar] [CrossRef]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analyses. BMJ 2013, 346, f1326. [Google Scholar] [CrossRef]
- Mente, A.; O’Donnell, M.; Rangarajan, S.; Dagenais, G.; Lear, S.; McQueen, M.; Diaz, R.; Avezum, A.; Lopez-Jaramillo, P.; Lanas, F.; et al. Associations of urinary sodium excretion with cardiovascular events in individuals with and without hypertension: A pooled analysis of data from four studies. Lancet 2016, 388, 465–475. [Google Scholar] [CrossRef]
- Graudal, N.; Jürgens, G.; Baslund, B.; Alderman, M.H. Compared with usual sodium intake, low- and excessive-sodium diets are associated with increased mortality: A meta-analysis. Am. J. Hypertens. 2014, 27, 1129–1137. [Google Scholar] [CrossRef]
- Saulnier, P.J.; Gand, E.; Hadjadj, S.; Surdiagene Study Group. Sodium and cardiovascular disease. N. Engl. J. Med. 2014, 371, 2135–2136. [Google Scholar]
- O’Donnell, M.J.; Yusuf, S.; Mente, A.; Gao, P.; Mann, J.F.; Teo, K.; McQueen, M.; Sleight, P.; Sharma, A.M.; Dans, A.; et al. Urinary sodium and potassium excretion and risk of cardiovascular events. JAMA 2011, 306, 2229–2238. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.; Mente, A.; Rangarajan, S.; McQueen, M.J.; Wang, X.; Liu, L.; Yan, H.; Lee, S.F.; Mony, P.; Devanath, A.; et al. Urinary Sodium and Potassium Excretion, Mortality, and Cardiovascular Events. N. Engl. J. Med. 2014, 371, 612–623. [Google Scholar] [CrossRef] [PubMed]
- Alderman, M.H.; Cohen, H.W. Dietary sodium intake and cardiovascular mortality: Controversy resolved? Am. J. Hypertens. 2012, 25, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Kim, M.K.; Shin, J.; Choi, B.Y.; Lee, Y.H.; Shin, D.H.; Shin, M.H. High sodium intake and sodium to potassium ratio may be linked to subsequent increase in vascular damage in adults aged 40 years and older: The Korean multi-rural communities cohort (MRCohort). Eur. J. Nutr. 2019, 58, 1659–1671. [Google Scholar] [CrossRef]
- Lee, S.K.; Kim, J.S.; Kim, S.H.; Kim, Y.H.; Lim, H.E.; Kim, E.J.; Park, C.G.; Cho, G.Y.; Kim, J.; Baik, I.; et al. Sodium Excretion and Cardiovascular Structure and Function in the Nonhypertensive Population: The Korean Genome and Epidemiology Study. Am. J. Hypertens. 2015, 28, 1010–1016. [Google Scholar] [CrossRef]
- Pimenta, E.; Gaddam, K.K.; Oparil, S.; Aban, I.; Husain, S.; Dell’Italia, L.J.; Calhoun, D.A. Effects of dietary sodium reduction on blood pressure in subjects with resistant hypertension: Results from a randomized trial. Hypertension 2009, 54, 475–481. [Google Scholar] [CrossRef]
- Todd, A.S.; Macginley, R.J.; Schollum, J.B.; Williams, S.M.; Sutherland, W.H.; Mann, J.I.; Walker, R.J. Dietary sodium loading in normotensive healthy volunteers does not increase arterial vascular reactivity or blood pressure. Nephrology 2012, 17, 249–256. [Google Scholar] [CrossRef]
- Dai, X.W.; Wang, C.; Xu, Y.; Guan, K.; Su, Y.X.; Chen, Y.M. Urinary Sodium and Potassium Excretion and Carotid Atherosclerosis in Chinese Men and Women. Nutrients 2016, 8, 612. [Google Scholar] [CrossRef]
- Mazza, E.; Ferro, Y.; Lamprinoudi, T.; Gazzaruso, C.; Doldo, P.; Pujia, A.; Montalcini, T. Relationship between high sodium and low PUFA intake and carotid atherosclerosis in elderly women. Exp. Gerontol. 2018, 108, 256–261. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Polonia, J.; Maldonado, J.; Ramos, R.; Bertoquini, S.; Duro, M.; Almeida, C.; Ferreira, J.; Barbosa, L.; Silva, J.A.; Martins, L. Estimation of salt intake by urinary sodium excretion in a Portuguese adult population and its relationship to arterial stiffness. Rev. Port. Cardiol. 2006, 25, 801–817. [Google Scholar] [PubMed]
- García-Ortiz, L.; Recio-Rodríguez, J.I.; Rodríguez-Sánchez, E.; Patino-Alonso, M.C.; Agudo-Conde, C.; Rodríguez-Martín, C.; Castaño-Sánchez, C.; Runkle, I.; Gómez-Marcos, M.A. Sodium and potassium intake present a J-shaped relationship with arterial stiffness and carotid intima-media thickness. Atherosclerosis 2012, 225, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Kotliar, C.; Kempny, P.; Gonzalez, S.; Castellaro, C.; Forcada, P.; Obregon, S.; Cavanagh, E.; Chiabaut Svane, J.; Casarini, M.J.; Rojas, M.; et al. Lack of RAAS inhibition by high-salt intake is associated with arterial stiffness in hypertensive patients. J. Renin Angiotensin Aldosterone Syst. 2014, 15, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Polonia, J.; Monteiro, J.; Almeida, J.; Silva, J.A.; Bertoquini, S. High salt intake is associated with a higher risk of cardiovascular events: A 7.2-year evaluation of a cohort of hypertensive patients. Blood Press Monit. 2016, 21, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Strauss, M.; Smith, W.; Kruger, R.; Van der Westhuizen, B.; Schutte, A.E. Large artery stiffness is associated with salt intake in young healthy black but not white adults: The African-PREDICT study. Eur. J. Nutr. 2018, 57, 2649–2656. [Google Scholar] [CrossRef] [PubMed]
- Triantafyllou, A.; Anyfanti, P.; Gkaliagkousi, E.; Zabulis, X.; Vamvakis, A.; Gkolias, V.; Petidis, K.; Aslanidis, S.; Douma, S. Association of Urinary Sodium Excretion with Vascular Damage: A Local Kidney Effect, Rather Than a Marker of Generalized Vascular Impairment. Int. J. Hypertens. 2018, 2018, 7620563. [Google Scholar] [CrossRef] [PubMed]
- Nerbass, F.B.; Pecoits-Filho, R.; McIntyre, N.J.; Shardlow, A.; McIntyre, C.W.; Taal, M.W. Reduction in sodium intake is independently associated with improved blood pressure control in people with chronic kidney disease in primary care. Br. J. Nutr. 2015, 114, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Siriopol, D.; Covic, A.; Iliescu, R.; Kanbay, M.; Tautu, O.; Radulescu, L.; Mitu, O.; Salaru, D.; Dorobantu, M. Arterial stiffness mediates the effect of salt intake on systolic blood pressure. J. Clin. Hypertens. (Greenwich) 2018, 20, 1587–1594. [Google Scholar] [CrossRef]
- Sonoda, H.; Takase, H.; Dohi, Y.; Kimura, G. Factors associated with brachial-ankle pulse wave velocity in the general population. J. Hum. Hypertens. 2012, 26, 701–705. [Google Scholar] [CrossRef][Green Version]
- Sun, N. Relationship of 24-h urinary sodium excretion with blood pressure, arterial distensibility, and urine albumin in Chinese hypertensive patients. Eur. Heart J. Suppl. 2015, 17, F37–F43. [Google Scholar] [CrossRef]
- Han, W.; Han, X.; Sun, N.; Chen, Y.; Jiang, S.; Li, M. Relationships between urinary electrolytes excretion and central hemodynamics, and arterial stiffness in hypertensive patients. Hypertens. Res. 2017, 40, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Sae, M.C.; Cipolli, J.A.; Cornélio, M.E.; Matos-Souza, J.R.; Fernandes, M.N.; Schreiber, R.; Costa, F.O.; Franchini, K.G.; Rodrigues, R.C.; Gallani, M.C.; et al. Sodium intake is associated with carotid artery structure alterations and plasma matrix metalloproteinase-9 upregulation in hypertensive adults. J. Nutr. 2011, 141, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Seals, D.R.; Tanaka, H.; Clevenger, C.M.; Monahan, K.D.; Reiling, M.J.; Hiatt, W.R.; Davy, K.P.; DeSouza, C.A. Blood pressure reductions with exercise and sodium restriction in postmenopausal women with elevated systolic pressure: Role of arterial stiffness. J. Am. Coll. Cardiol. 2001, 38, 506–513. [Google Scholar] [CrossRef]
- Dickinson, K.M.; Keogh, J.B.; Clifton, P.M. Effects of a low-salt diet on flow-mediated dilatation in humans. Am. J. Clin. Nutr. 2009, 89, 485–490. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Marciniak, M.; Visagie, E.; Markandu, N.D.; Anand, V.; Dalton, R.N.; MacGregor, G.A. Effect of modest salt reduction on blood pressure, urinary albumin, and pulse wave velocity in white, black, and Asian mild hypertensives. Hypertension 2009, 54, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Todd, A.S.; MacGinley, R.J.; Schollum, J.B.; Johnson, R.J.; Williams, S.M.; Sutherland, W.H.; Mann, J.I.; Walker, R.J. Dietary salt loading impairs arterial vascular reactivity. Am. J. Clin. Nutr. 2010, 91, 557–564. [Google Scholar] [CrossRef] [PubMed]
- McMahon, E.J.; Bauer, J.D.; Hawley, C.M.; Isbel, N.M.; Stowasser, M.; Johnson, D.W.; Campbell, K.L. A randomized trial of dietary sodium restriction in CKD. J. Am. Soc. Nephrol. 2013, 24, 2096–2103. [Google Scholar] [CrossRef]
- Dickinson, K.M.; Clifton, P.M.; Keogh, J.B. A reduction of 3 g/day from a usual 9 g/day salt diet improves endothelial function and decreases endothelin-1 in a randomised cross_over study in normotensive overweight and obese subjects. Atherosclerosis 2014, 233, 32–38. [Google Scholar] [CrossRef]
- Gijsbers, L.; Dower, J.I.; Mensink, M.; Siebelink, E.; Bakker, S.J.; Geleijnse, J.M. Effects of sodium and potassium supplementation on blood pressure and arterial stiffness: A fully controlled dietary intervention study. J. Hum. Hypertens. 2015, 29, 592–598. [Google Scholar] [CrossRef]
- Suckling, R.J.; He, F.J.; Markandu, N.D.; MacGregor, G.A. Modest Salt Reduction Lowers Blood Pressure and Albumin Excretion in Impaired Glucose Tolerance and Type 2 Diabetes Mellitus: A Randomized Double-Blind Trial. Hypertension 2016, 67, 1189–1195. [Google Scholar] [CrossRef]
- van der Graaf, A.M.; Paauw, N.D.; Toering, T.J.; Feelisch, M.; Faas, M.M.; Sutton, T.R.; Minnion, M.; Lefrandt, J.D.; Scherjon, S.A.; Franx, A.; et al. Impaired sodium-dependent adaptation of arterial stiffness in formerly preeclamptic women: The RETAP-vascular study. Am. J. Physiol. Heart Circ. Physiol. 2016, 310, H1827–H1833. [Google Scholar] [CrossRef] [PubMed]
- Muth, B.J.; Brian, M.S.; Chirinos, J.A.; Lennon, S.L.; Farquhar, W.B.; Edwards, D.G. Central systolic blood pressure and aortic stiffness response to dietary sodium in young and middle-aged adults. J. Am. Soc. Hypertens. 2017, 11, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Avolio, A.P.; Clyde, K.M.; Beard, T.C.; Cooke, H.M.; Ho, K.K.; O’Rourke, M.F. Improved arterial distensibility in normotensive subjects on a low salt diet. Arteriosclerosis 1986, 6, 166–169. [Google Scholar] [CrossRef] [PubMed]
- Rhee, M.Y.; Kim, J.H.; Na, S.H.; Chung, J.W.; Bae, J.H.; Nah, D.Y.; Gu, N.; Kim, H.Y. Elevation of heart-femoral pulse wave velocity by short-term low sodium diet followed by high sodium diet in hypertensive patients with sodium sensitivity. Nutr. Res. Pract. 2016, 10, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Mu, J.J.; Geng, L.K.; Wang, D.; Ren, K.Y.; Guo, T.S.; Chu, C.; Xie, B.Q.; Liu, F.Q.; Yuan, Z.Y. Effect of salt intake and potassium supplementation on brachial-ankle pulse wave velocity in Chinese subjects: An interventional study. Braz. J. Med. Biol. Res. 2015, 48, 83–90. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Creager, M.A.; Roddy, M.A.; Holland, K.M.; Hirsch, A.T.; Dzau, V.J. Sodium depresses arterial baroreceptor reflex function in normotensive humans. Hypertension 1991, 17, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Gates, P.E.; Tanaka, H.; Hiatt, W.R.; Seals, D.R. Dietary sodium restriction rapidly improves large elastic artery compliance in older adults with systolic hypertension. Hypertension 2004, 44, 35–41. [Google Scholar] [CrossRef]
- Njoroge, J.N.; Khoudary, S.R.; Fried, L.F.; Barinas-Mitchell, E.; Sutton-Tyrrell, K. High urinary sodium is associated with increased carotid intima-media thickness in normotensive overweight and obese adults. Am. J. Hypertens. 2011, 24, 70–76. [Google Scholar] [CrossRef]
- Ustundag, S.; Yilmaz, G.; Sevinc, C.; Akpinar, S.; Temizoz, O.; Sut, N.; Ustundag, A. Carotid intima media thickness is independently associated with urinary sodium excretion in patients with chronic kidney disease. Ren. Fail. 2015, 37, 1285–1292. [Google Scholar] [CrossRef]
- Benetos, A.; Xiao, Y.Y.; Cuche, J.L.; Hannaert, P.; Safar, M. Arterial effects of salt restriction in hypertensive patients. A 9-week, randomized, double-blind, crossover study. J. Hypertens. 1992, 10, 355–360. [Google Scholar] [CrossRef]
- Felder, R.A.; White, M.J.; Williams, S.M.; Jose, P.A. Diagnostic tools for hypertension and salt sensitivity testing. Curr. Opin. Nephrol. Hypertens. 2013, 22, 65–76. [Google Scholar] [CrossRef] [PubMed]
- D’Elia, L.; Galletti, F.; La Fata, E.; Sabino, P.; Strazzullo, P. Effect of dietary sodium restriction on arterial stiffness: Systematic review and meta-analysis of the randomized controlled trials. J. Hypertens. 2018, 36, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.G.; Farquhar, W.B. Vascular effects of dietary salt. Curr. Opin. Nephrol. Hypertens. 2015, 24, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Simon, G. Experimental evidence for blood pressure-independent vascular effects of high sodium diet. Am. J. Hypertens. 2003, 16, 1074–1078. [Google Scholar] [CrossRef] [PubMed]
- Elijovich, F.; Weinberger, M.H.; Anderson, C.A.; Appel, L.J.; Bursztyn, M.; Cook, N.R.; Dart, R.A.; Newton-Cheh, C.H.; Sacks, F.M.; Laffer, C.L. Salt Sensitivity of Blood Pressure: A Scientific Statement from the American Heart Association. Hypertension 2016, 68, e7–e46. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ARTERIOSCLEROSIS | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| cfPWV | |||||||||||||
| 1. Observational Cross-Sectional Studies | |||||||||||||
| Author (Year) | Country | Study Design | Population Description | FU (Years) | Sex | Race | N | Age (Years, Mean ± SD) | Na Estimation Method | Na Intake/Excretion (mg/d) | Vascular Assessment | Results | |
| Polónia, J. (2006) [22] | Portugal | c-sect | essential HT, recent stroke or healthy university students | - | M/F | Mixed | 426 | 50 ± 22 | 24hU | Total: 4646 ± 1472 | tonometry | + ** | |
| García-Ortiz, L. (2012) [23] | Spain | c-sect | primary care patients aged 30–80 | - | M/F | N/AV | 351 | 54.8 ± 11.7 | FFQ | Total: 3180 ± 1250 Q1:1800 ± 390 Q2: 2650 ± 200 Q3: 3440 ± 270 | tonometry | J-shaped curve | |
| Kotliar, C. (2014) [24] | Argentina | c-sect | essential HT, aged 30 to 70 | - | M/F | N/AV | 300 | 48.7 ± 14.6 | 24hU | (a) low Na-low RAAS: 913.1 (747.5–1035) | tonometry | ≠ | |
| (b) low Na-high RAAS: 690 (602.6–740.6) | ≠ | ||||||||||||
| (c) High-Na-low RAAS: 2610.5 (1745.7–3604.1) | ≠ | ||||||||||||
| (d) high-Na-high RAAS: 2898 (2035.5–3588) | + * | ||||||||||||
| Polonia, J. (2016) [25] | Portugal | retrosp | HT adults | 7.2 (0.5–11.1) | M/F | White | 608 | 54.1 ± 14.3 | 24hU | 4793.2 ± 1821.6 | tonometry | + * | |
| Strauss, M. (2018) [26] | South Africa | prosp | NT adults | - | M/F | Mixed | 693 | 24.8 ± 3.01 | 24hU | 2967 (984.4–7613) | tonometry | total | + ** |
| black | + * | ||||||||||||
| white | ≠ | ||||||||||||
| Triantafyllou, A. (2018) [27] | Greece | c-sect | untreated HT—healthy individuals | - | M/F | White | 197 | 43.7 ± 12.1 | 24hU | True HT: 3348.8 (2251.7–4595.4) Intermediated HT phenotypes: 3128 (1902.1–4312.5) NT: 2732.4 (1630.7–4312.5) | tonometry | ≠ | |
| 2. Observational Studies with Follow Up (>1 Time Points) | |||||||||||||
| Author (Year) | Country | Study Design | Population Description | FU (Years) | Sex | Race | N | Age (Years, Mean ± SD) | Na Estimation Method | Na Intake/Excretion (mg/d) | Vascular Assessment | Results | |
| Nerbass, F.B. (2015) [28] | UK | prosp | adults in CKD stage 3 | 1 | M/F | N/AV | 1607 | 72.6 ± 9.0 | Spot urine collections and Nerbass equation to estimate 24h Na excretion | baseline: 2599 ± 782 follow-up: 2576 ± 782 | oscillometry | cfPWV (at both time points) | |
| Na <2300 mg | + ** | ||||||||||||
| Na >2300 mg | ≠ | ||||||||||||
| ΔcfPWV | |||||||||||||
| Unchanged Na | ≠ | ||||||||||||
| Decreased Na | ≠ | ||||||||||||
| Increased Na | + * | ||||||||||||
| Aortic PWV Other than cfPWV | |||||||||||||
| Siriopol, D. (2018) [29] | Romania | prosp | HT and NT Romanian adults | - | M/F | White | 1599 | 47.3 ± 17.1 | Morning spot urine sample + Kawasaki equation | 4816.2 ± 1550.2 | oscillometry | NT | + ** |
| HT | + ** | ||||||||||||
| baPWV | |||||||||||||
| 1. Observational Cross-Sectional Studies | |||||||||||||
| Sonoda, H. (2012) [30] | Japan | c-sect | healthy subjects | - | M/F | Asian | 911 | 61.3 ± 8.5 | 24hU | 720 ± 200 (mg /day/10 kg) | oscillometry | + ** | |
| Lee, S.K. (2015) [16] | Korea | c-sect | non-HT subjects, with no use of anti-HT drugs | - | M/F | Asian | 1586 | tertile 1: 52.1 ± 5.5 tertile 2: 53.0 ± 6.0 tertile 3: 52.6 ± 5.5 | Second morning void and Tanaka’s equation to convert to 24hU | 3588 ± 782 | plethysmography | − ** | |
| Sun, N. (2015) [31] | China | c-sect | newly diagnosed HT, untreated HT or patients with a 1 to 5 year history of HT who had stopped taking anti-HT drugs for 1 month | - | M/F | N/AV | 341 | Group A: 59.3 + 13.4 Group B: 56.1 + 15.5 Group C: 57.6 + 14.2 | 24hU | Total: 3507.5 ± 1577.8 Group A: 1807.8 ± 411.7 Group B: 3374.1 ± 618.7 Group C: 5858.1 ± 961.4 | oscillometry | + * | |
| Author (year) | Country | Study Design | Population Description | FU (years) | Sex | Race | N | Ag (Years, Mean ± SD) | Na Estimation Method | Na Intake/Excretion (mg/d) | Vascular Assessment | Results | |
| Han, W. (2017) [32] | China | c-sect | HT adults | - | M/F | N/AV | 431 | Group A: 54.5 ± 12.9 Group B: 52.9 ± 12.6 Group C: 50.9 ± 11.4 | 24hU | Total: 3831.8 ± 1.610, Group A: 1768.7 ± 464.6 Group B: 3371.8 ± 650.9 Group C: 5947.8 ± 1069.5 | oscillometry | + * | |
| 2. Observational Studies with Follow Up (>1 Time Points) | |||||||||||||
| Jung, S. (2019) [15] | South Korea | prosp | adults aged >40 | 5.3±1.0 | M/F | Mixed | 2145 | 59.9 ± 9.1 | FFQ and 3 day diet record | 2538 ± 1416 | oscillometry | baPWV | |
| Na baseline | + ** | ||||||||||||
| Na average of three visits | + ** | ||||||||||||
| ΔbaPWV | |||||||||||||
| Na baseline | + ** | ||||||||||||
| Na average of three visits | + ** | ||||||||||||
| Common Carotid Arterial Elasticity (Young’s Elastic Modulus, Stiffness Index, and Arterial Compliance) | |||||||||||||
| Ferreira-Sae, M.C. (2011) [33] | Brazil | c-sect | HT adults | - | M/F | N/AV | 134 | 58 ± 1 | 1. FFQ 2. 24h recall 3. discretionary Na intake 1 | Na intake/d: 5520 ± 290 FFQ: 1450 ± 180 24h recall: 940 ± 70 Discretionary Na: 3130 ± 190 | B-mode US | Young’s elastic modulus | + ** |
| stiffness index | ≠ | ||||||||||||
| arterial compliance | ≠ | ||||||||||||
| ARTERIOSCLEROSIS | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| cfPWV | |||||||||||||||
| Author | Country | Study Design | Population Description | Sex | Race | N | Age (Years, Mean ± SD) | Intervention Duration (Weeks) | Type of Diet | Na Estimation Method | Na Intake/Excretion (mg/d) | Vascular Assessment | Results | ||
| Intervention Groups | cfPWV Change (m/s) | ||||||||||||||
| Seals, D.R. (2001) [34] | USA | RCT | postmenopausal women, ≥50 years, high normal SBP or Stage 1 HTN | F | Mixed | 17 | 65 ± 10 | 13 | LS < 2400 mg | 24hU & food records | Urinary Na excretion Preint_restr: 2852 ± 1058 Postintn_restr:1978 ± 736 Dietary Na intake Preint_restr: 2685 ± 559 Postint_restr:1421 ± 512 | US | LS vs. baseline | −0.24 * | |
| Dickinson, K.M. (2009) [35] | Australia | cross-over RCT | OW/OB, mild HT adults | M/F | N/AV | 29 | 52.7 ± 6.0 | 4 (2 weeks × two diets) | Usual Na diet: 3450 mg Na/d vs. LS diet: 1150 mg Na/d | Three-day weighed food records & 24hU | Urinary method | oscillometry | LS vs. Usual Na | ≠ | |
| Baseline | 3553.5 ± 1568.6 | ||||||||||||||
| Usual Na | 3594.9 ± 1304.1 | ||||||||||||||
| LS | 1474.3 ± 949.9 | ||||||||||||||
| He, F.J. (2009) [36] | UK | cross-over dbRCT | HT adults | M/F | Mixed | 169 | All: 50 ± 11 Blacks: 50 ± 9 Whites: 52 ± 12 Asians: 47 ± 10 | 12 | 9 Na tablets (×230 mg)/d & 9 placebo tablets/d. (remained on LS diet: 2000 mg Na/d) | 24hU | Total | 3013 ± 1150 | tonometry | From Na to placebo | |
| Total | −0.40 ** | ||||||||||||||
| Blacks | 3036 ± 1058 | Blacks | −0.50 ** | ||||||||||||
| Whites | 2921 ± 1173 | Whites | ≠ | ||||||||||||
| Asians | 3174 ± 1311 | Asians | ≠ | ||||||||||||
| Pimenta, E. (2009) [17] | USA | cross-over RCT | resistant HT adults on a stable anti-HT drug | M/F | Mixed | 12 | 55.5 ± 9.4 | 2 (1 week × two diets) | LS diet: 1495 mg Na/d vs. HS diet: suppl. >5750 mg Na/d | 24hU | Baseline: 4478.1 ± 1577.8 LS diet: 1060.3 ± 616.4 vs. HS diet: 5800.6 ± 1485.8 | tonometry | From HS to LS ≠ | ||
| Todd, A.S. (2010) [37] | New Zealand | cross-over sbRCT | PHT or HT, NOB adults or on anti-HT drugs | M/F | Mixed | 33 | 51.8 ± 7.6 | 12 | (500 mL tomato juice + LS diet/day) (A) 0 + 1380 mg (B) 2070 + 1380 mg (C) 3220 + 1380 mg | Morning spot urine samples & dietary recalls | Na intake | tonometry | B vs. A | + 0.39 ** | |
| Usual diet | 2607 ± 1289 | C vs. A | + 0.35 ** | ||||||||||||
| A | 1254 ± 397 | B vs. C | ≠ | ||||||||||||
| B | 1357 ± 486 | ||||||||||||||
| C | 1306 ± 335 | ||||||||||||||
| Todd, A.S. (2012) [18] | New Zealand/Australia | cross-over sbRCT | NT, NOB adults | M/F | N/AV | 23 | 43.7 (24–61) | 12 | (500 mL tomato juice + LS diet/day) (A) 0 + 1380 mg (B) 2070 + 1380 mg (C) 3220 + 1380 mg | Morning spot urine samples & dietary recalls | Pre-baseline: | 2410.4 | tonometry | B vs. A | ≠ |
| After intervention (Na intake + Na tomato juice) | C vs. A | ≠ | |||||||||||||
| A | 0 + 1232.8 | ||||||||||||||
| B | 2070 + 1207.5 | B vs. C | ≠ | ||||||||||||
| C | 3220 + 1140.8 | ||||||||||||||
| McMahon, E.J. (2013) [38] | Australia | cross-over dbRCT | HT adults, with stage 3 or 4 CKD | M/F | N/AV | 20 | 68.5 ± 11 | 4 (2 weeks × two diets) | HS diet: 4140–4600 mg Na/d vs. LS diet: 1380–1840 mg Na/d | 24hU | LS: 1725 (1334–2576) vs. HS: 3864 (3358–5037) | tonometry | LS vs. HS | ≠ | |
| Dickinson, K.M. (2014) [39] | Australia | cross-over sbRCT | OW or OB subjects | M/F | N/AV | 25 | N/AV | 6 | LS diet: 2400 mg/d vs. Usual Na diet: 3600 mg/d | 24hU | baseline: 2761 ± 1031 Usual Na diet: 1729 ± 627 LS diet: 1799 ± 497 | tonometry | LS vs. US | ≠ | |
| Gijsbers, L. (2015) [40] | the Netherlands | cross-over RCT | untreated (P)HT, aged 40–80 | M/F | White | 36 | 65.8 (47–80) | 4 | Na suppl: 3000 mg/d vs. placebo | 24hU | Baseline: 3535.1 Na suppl.: 4666.7 ± 1260.4 vs. Placebo: 2417.3 ± 913.1 | tonometry | Na suppl. vs. placebo | ≠ | |
| Suckling, F.J. (2016) [41] | United Kingdom | Cross-over dbRCT | untreated HT adults | M/F | Mixed | 46 | 58 ± 1 | 12 (6 weeks × two diets) | 9 Na tablets (×230 mg)/d vs. 9 placebo tablets/d. | 24hU | Na diet: 3797.3 ± 207 vs. Placebo: 2681.8 ± 218.5 | tonometry | Na diet vs. placebo | ≠ | |
| van der Graaf, A.M. (2016) [42] | the Netherlands | cross-over RCT | women with history of preeclampsia or history of healthy former pregnancy | F | N/AV | 36 | 36 ± 5 | 2 | LS diet: 1150 mg/d vs. HS diet: 4600 mg/d | 24hU | NT pregnancy history group: LS: 897 ± 322 HS: 5083 ± 1472 Preeclamptic pregnancy history group: LS: 1035 ± 529 HS: 5934 ± 1978 | tonometry | LS vs. HS (in either group) | ≠ | |
| Muth, B.J. (2017) [43] | USA | cross-over RCT | healthy, NT adults | M/F | N/AV | 85 | Young: 27 ± 1 Middle-aged: 52 ± 1 | 2 | LS diet: 460 mg/d vs. HS diet:6900 mg/d | 24hU | * LS diet (young & middle aged): 690 HS diet (young & middle-aged): 5405 * Approximately from diagram | tonometry | middle aged | +0.60 ** | |
| young | ≠ | ||||||||||||||
| Aortic PWV (Other than cfPWV) | |||||||||||||||
| Author | Country | Study Design | Population Description | Sex | Race | N | Age(Years, Mean ± SD) | Intervention Duration | Type of Diet | Na Estimation Method | Na Intake/Excretion (mg/d) | Vascular Assessment | Results | ||
| Intervention groups | PWV Change (%) | ||||||||||||||
| Avolio AP. (1986) [44] | Australia | RCT | healthy NT adults and children | M/F | N/AV | 114 | Group 1: Control: 10.8 ± 1.9 LS: 10.4 ± 2.5 Group 2: Control: 39.4 ± 1.7 LS: 39.8 ± 1.6 Group 3: Control: 52.2 ± 3.5 LS: 54.5 ± 4.2 | 24.8±2.5 months (8 months to 5 years) | N/AV | 24hU & diet questionnaire | Na excretion: Control group: N/AV Group 1: 1564 Group 2: 943 Group 3: 506 | oscillometry | Group 1 leg | −11.2 * | |
| Group 2 aortic arm leg | −21.8 ** −10.7 * −13.3 * | ||||||||||||||
| Group 3 aortic leg | −22.7 * −22.3 * | ||||||||||||||
| hfPWV | |||||||||||||||
| Rhee MY. (2016) [45] | Korea | RCT | NT and HT adults | M/F | N/AV | 101 | 46.0 ± 16.6 | 2 | LS DASH diet: 2320 mg Na/d vs. HS DASH diet: 7000 mg Na/d | N/AV | LS diet: 2320 vs. HS diet: 7000 | US | HS vs. LS | ||
| SS | +4% * | ||||||||||||||
| SR | ≠ | ||||||||||||||
| HT | ≠ | ||||||||||||||
| NT | ≠ | ||||||||||||||
| baPWV | |||||||||||||||
| Wang Y. (2015) [46] | China | dietary intervention study | mild HT adults | M/F | N/AV | 49 | 49.0 ± 7.9 | 3 (1 week × three diets) | LS diet: 1179.9 mg/d & HS diet: 7079.4 mg/d | 24hU | 3999.7 ± 1543.3 | plethysmography | LS vs. HS | ≠ | |
| SS vs. SR | |||||||||||||||
| Baseline | +2.3 * | ||||||||||||||
| After LS | +1.5 * | ||||||||||||||
| After HS | +2.0 * | ||||||||||||||
| Arterial Elasticity (Arterial Compliance) | |||||||||||||||
| Author | Country | Study Design | Population Description | Sex | Race | N | Age (Years, Mean ± SD) | Intervention Duration | Type of Diet | Na Estimation Method | Na Intake/Excretion (mg/d) | Vascular Assessment | Results | ||
| Intervention Groups | Vascular Change (mm/mmHg) | ||||||||||||||
| Creager MA. (1991) [47] | USA | cross-over RCT | NT men | M | N/AV | 17 | 30 ± 2 years | 10 days | LS diet: 230 mg Na/d vs. HS diet: 4600 mg Na/d | 24hU | LS: 253 ± 46 vs. HS: 4117 ± 207 | diastolic blood pressure time decay method | LS vs. HS | ≠ | |
| Gates PE. (2004) [48] | USA | cross-over dbRCT | stage 1 HT adults, older than 50 | M/F | White | 12 | men: 63 ± 1 women: 64 ± 4 | 8 weeks | LS diet: 1196 ± 92 & Normal Na diet: 1311 ± 23 | 3 day dietary records & 24hU | Na excretion Baseline: 3105 LS: 1380 Normal Na: 3450 | B-mode US | LS | +0.04 * | |
| Normal | ≠ | ||||||||||||||
| Arterial Remodeling | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| cIMT | |||||||||||||
| 1. Observational Cross-Sectional Studies | |||||||||||||
| Author (Year) | Country | Study Design | Population Description | FU (Years) | Sex | Race | N | Age (Years, Mean ± SD) | Na Estimation Method | Na Intake/Excretion (mg/d) | Vascular Assessment | Results | |
| Ferreira-Sae, M.C. (2011) [33] | Brazil | c-sect | HT adults | - | M/F | N/AV | 134 | 58 ± 1 | 1. FFQ 2. 24h recall 3. discretionary Na intake 1 | Na intake/d: 5520 ± 290 FFQ: 1450 ± 180 24h recall: 940 ± 70 Discretionary Na: 3130 ± 190 | B-mode US | + * | |
| Njoroge, J.N. (2011) [49] | USA | c-sect | OW or OB, physically inactive adults | - | M/F | Mixed | 258 | Total: 38.5 ± 5.8 Q1: 39.3 ± 5.6 Q2: 38.7 ± 5.2 Q3: 37.6 ± 6.2 Q4: 38.2 ± 6 | 24hU | Total:1104–9545 Q1: 1104–3289 Q2: 3312–4117 Q3: 4140–5152 Q4: 5175–9545 | B-mode US | + * | |
| García-Ortiz, L. (2012) [23] | Spain | c-sect | primary care patients aged 30–80 | - | M/F | N/AV | 351 | Total: 54.8 ± 11.7 Q1: 57.6 ± 12.1 Q2: 55.9 ± 11.3 Q3: 54.7 ± 10.5 | FFQ | Total: 3180 ± 1250 Q1:1800 ± 390 Q2: 2650 ± 200 Q3: 3440 ± 270 | B-mode US | J-shaped | |
| Lee SK. (2015) [16] | Korea | c-sect | non-HT subjects, with no use of anti-HT drugs | - | M/F | Asian | 1586 | tertile 1: 52.1 ± 5.5 tertile 2: 53.0 ± 6.0 tertile 3: 52.6 ± 5.5 | second morning void & Tanaka’s equation | 3588 ± 782 | B-mode US | − ** | |
| Ustundag, S. (2015) [50] | Turkey | c-sect | ambulatory adult patients, in stage 2–4 CKD | - | M/F | N/AV | 193 | Na excretion <1955 mg/day: 47.7 ± 10.6 ≥1955 mg/day: 49.7 ± 11.0 Mean IMT <0.750 mm: 45.1 ± 12.2 ≥0.750 mm: 52.3 ± 8.3 | 24hU | <1955 mg/day: 3220 ± 69 ≥1955 mg/day: 3220 ± 69 Mean IMT < 0.750 mm: 3220 ± 46 Mean IMT ≥ 0.750 mm: 3220 ± 69 | B-mode US | + ** | |
| Dai, X.W. (2016) [19] | China | c-sect | Asian adults, via subject referral and community advertisement | - | M/F | Asian | 3290 | M: 62.1 ± 6.7 F: 59.4 ± 5.5 | FFQ | Dietary Na intake: Q1: 833 ± 394 Q2: 864 ± 507 Q3: 825 ± 41 Q4: 828 ± 395 | B-mode US | common cIMT | ≠ |
| carotid bifurcation IMT | + * | ||||||||||||
| Mazza, E. (2018) [20] | Italy | c-sect | adults aged ≥65, not suffering from any debilitating diseases | - | F | White | 108 | 70 ± 4 | 24h dietary recall + 7 day food record | 1476 ± 618 | B-mode US | + * | |
| 2. Observational Studies with Follow up (>1 Time Points) | |||||||||||||
| Jung, S. (2019) [15] | South Korea | prosp | adults aged >40 | 5.4 ± 1.0 | M/F | Mixed | 2494 | 60.2 ± 9.0 | FFQ + 3 day diet record | 2644 ± 1573 | B-mode US | cIMT | |
| Na baseline | ≠ | ||||||||||||
| Na average of three visits | + ** | ||||||||||||
| ΔcIMT | |||||||||||||
| Na baseline | ≠ | ||||||||||||
| Na average of three visits | − * | ||||||||||||
| Arterial Remodeling | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Right Branchial Artery and Common Carotid Artery Diameter | ||||||||||||||
| Author | Country | Study Design | Population Description | Sex | Race | N | Age (Years, Mean ± SD) | Intervention Duration (Weeks) | Type of Diet | Na Estimation Method | Na Intake/Excretion (mg/d) | Vascular Assessment | Results | |
| Benetos, A. (1992) [51] | France | cross-over dbRCT | actively working, mild to moderate HT adults | M/F | N/AV | 20 | 41.5 ± 2.4 | 8 | Group 1 and Group 2: Normal Na diet (NS diet, Na capsules): 1400 mg and low-Na diet (LS diet), lactose capsules | 24hU | Baseline: 3979 ± 299 LS diet: 1955 ± 220.8 NS diet: 3749 ± 305.9 | B-mode US | LS diet vs. NS diet | |
| Brachial artery diameter | +0.67m ** | |||||||||||||
| common carotid diameter | ≠ | |||||||||||||
| Atheromatosis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Carotid Plaques | ||||||||||||
| Author (Year) | Country | Study Design | Population Description | FU (Years) | Sex | Race | N | Age (Years, Mean ± SD) | Na Estimation Method | Na Intake/Excretion (mg/d) | Vascular Assessment | Results |
| Dai, X.W. (2016) [19] | China | c-sect | Asian adults, via subject referral and community advertisement | - | M/F | Asian | 3290 | M: 62.1 ± 6.7 F: 59.4 ± 5.5 | FFQ | Dietary Na intake: Q1: 833 ± 394 Q2: 864 ± 507 Q3: 825 ± 41 Q4: 828 ± 395 | B-mode US | ≠ |
| Mazza, E. (2018) [20] | Italy | c-sect | Adults aged ≥65, not suffering from any debilitating diseases | - | F | White | 108 | 70 ± 4 | 24h dietary recall + 7 day food record | 1476 ± 618 Tertile I: 780–900 Tertile II: 1330–1430 Tertile III: 2050–2330 | B-mode US | Tertile III vs. Tertile I + * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsirimiagkou, C.; Basdeki, E.D.; Argyris, A.; Manios, Y.; Yannakoulia, M.; Protogerou, A.D.; Karatzi, K. Current Data on Dietary Sodium, Arterial Structure and Function in Humans: A Systematic Review. Nutrients 2020, 12, 5. https://doi.org/10.3390/nu12010005
Tsirimiagkou C, Basdeki ED, Argyris A, Manios Y, Yannakoulia M, Protogerou AD, Karatzi K. Current Data on Dietary Sodium, Arterial Structure and Function in Humans: A Systematic Review. Nutrients. 2020; 12(1):5. https://doi.org/10.3390/nu12010005
Chicago/Turabian StyleTsirimiagkou, Christiana, Eirini D. Basdeki, Antonios Argyris, Yannis Manios, Maria Yannakoulia, Athanase D. Protogerou, and Kalliopi Karatzi. 2020. "Current Data on Dietary Sodium, Arterial Structure and Function in Humans: A Systematic Review" Nutrients 12, no. 1: 5. https://doi.org/10.3390/nu12010005
APA StyleTsirimiagkou, C., Basdeki, E. D., Argyris, A., Manios, Y., Yannakoulia, M., Protogerou, A. D., & Karatzi, K. (2020). Current Data on Dietary Sodium, Arterial Structure and Function in Humans: A Systematic Review. Nutrients, 12(1), 5. https://doi.org/10.3390/nu12010005