Cirrhotic Cardiomyopathy



Abstract
1. Introduction
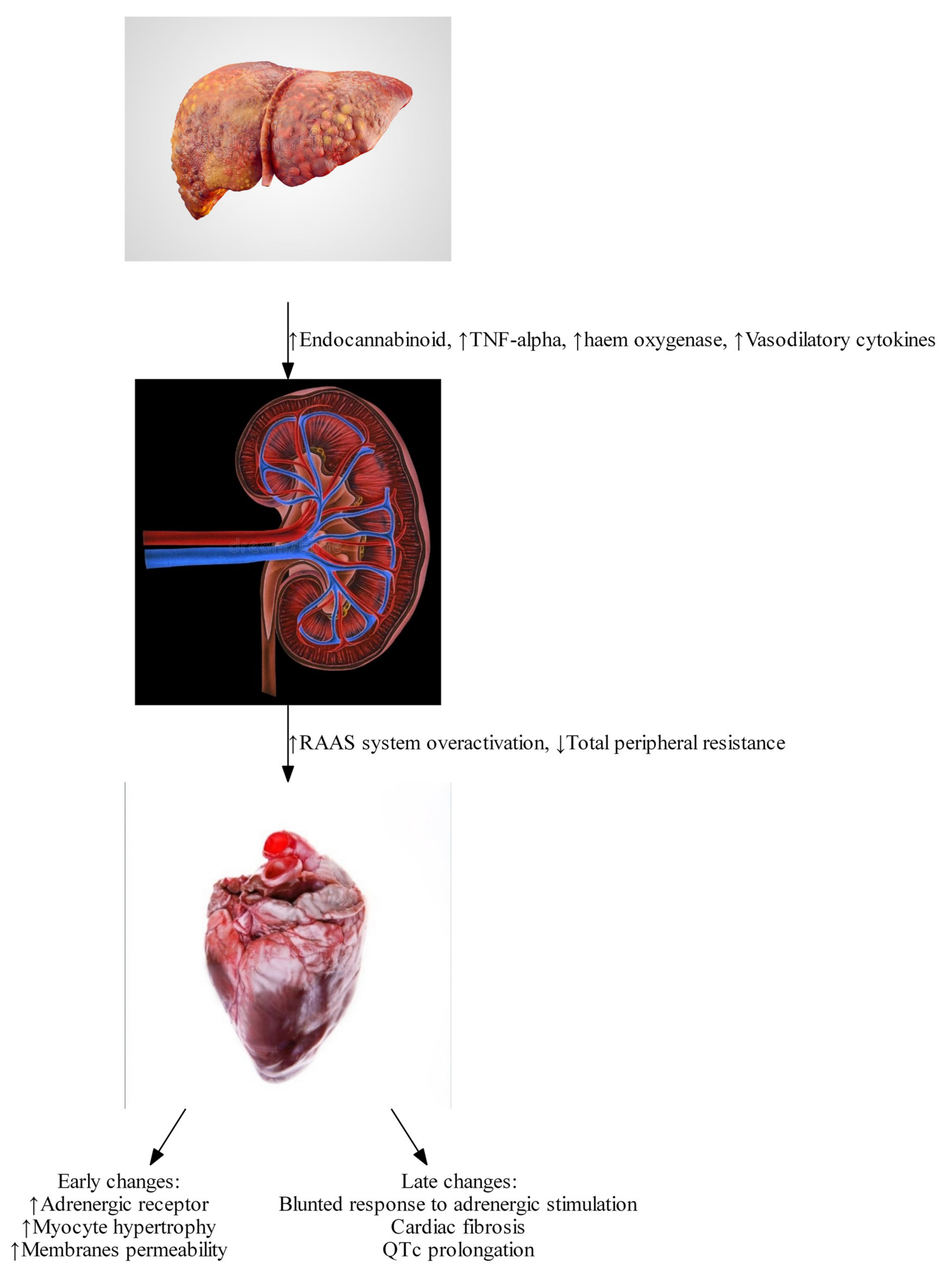
2. Pathophysiology
2.1. Endocannabinoids
2.2. Tumor Necrosis Factor
2.3. Haem Oxygenase
2.4. Bile Acid
2.5. β Adrenergic Responsiveness
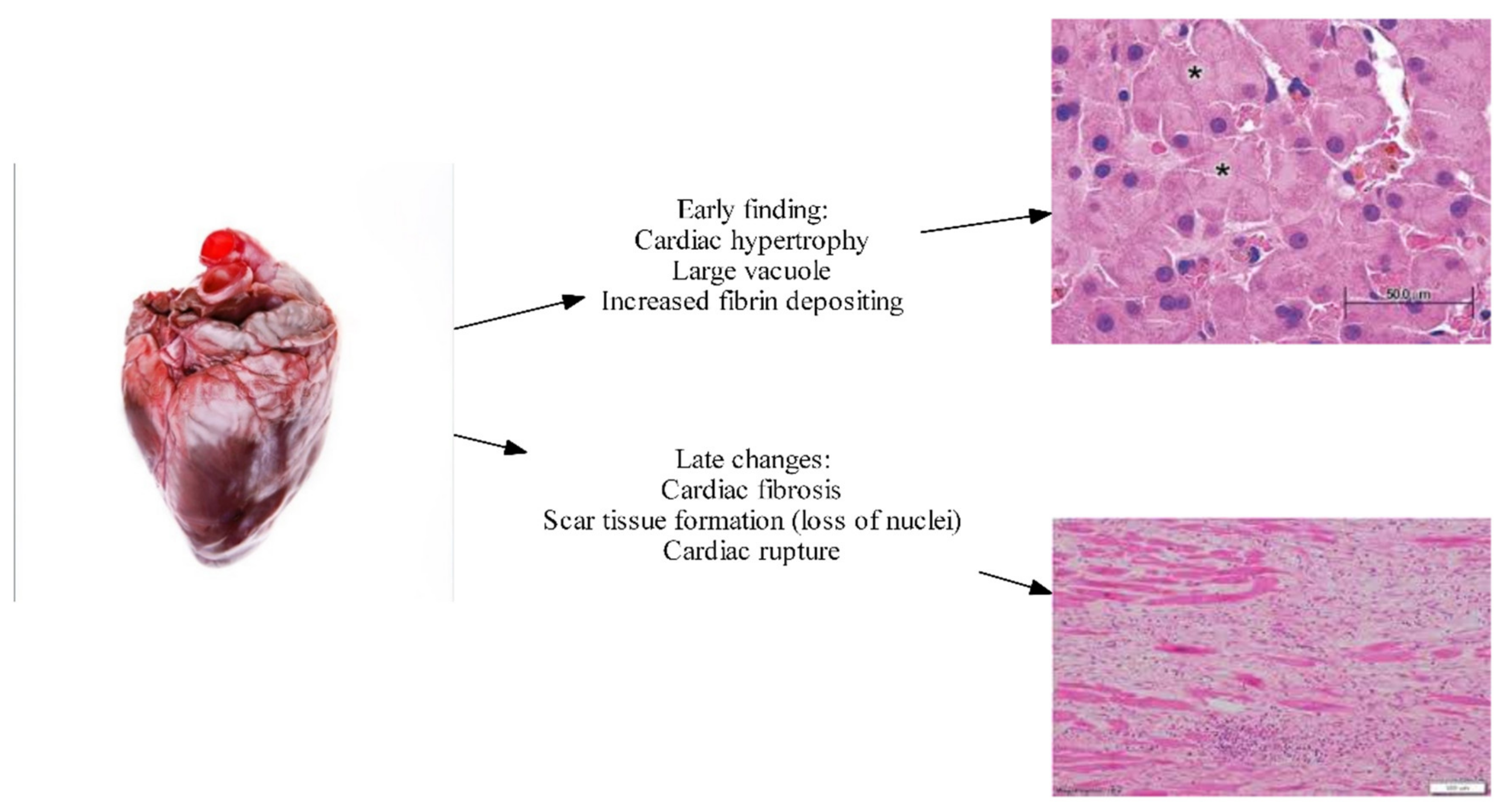
2.6. Myocardial Fibrosis and Myocyte Hypertrophy
2.7. Altered Cardiomyocyte Membrane Fluidity and Ion Channel Defects
3. Investigations
3.1. Electrocardiogram
3.2. Echocardiography
3.3. Diastolic Dysfunction
3.3.1. E/A Ratio
3.3.2. e′
3.3.3. E/e′
3.4. Systolic Dysfunction
Global Longitudinal Strain
3.5. Cardiac MRI
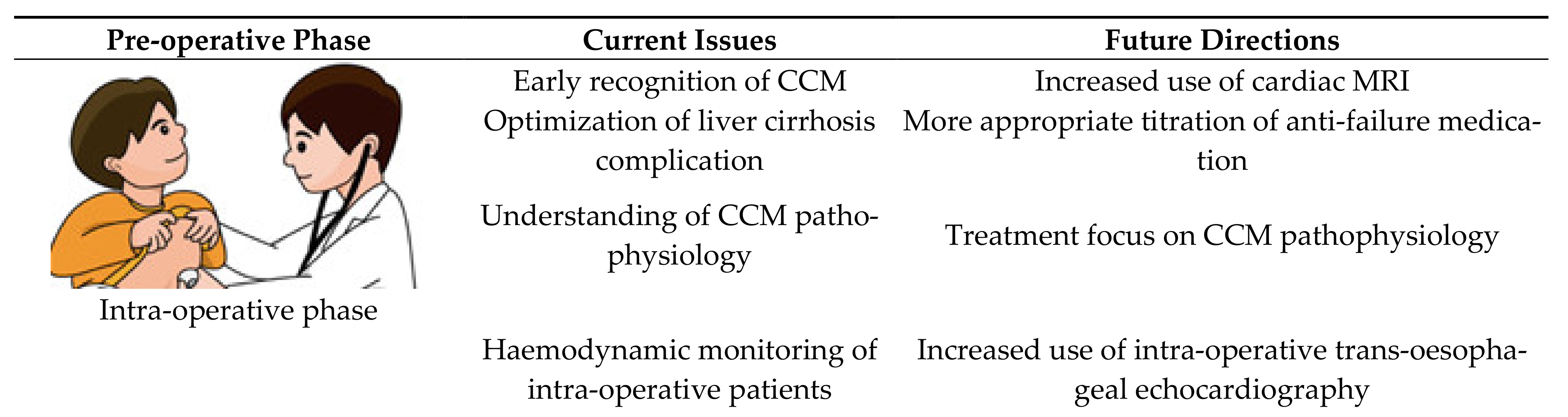
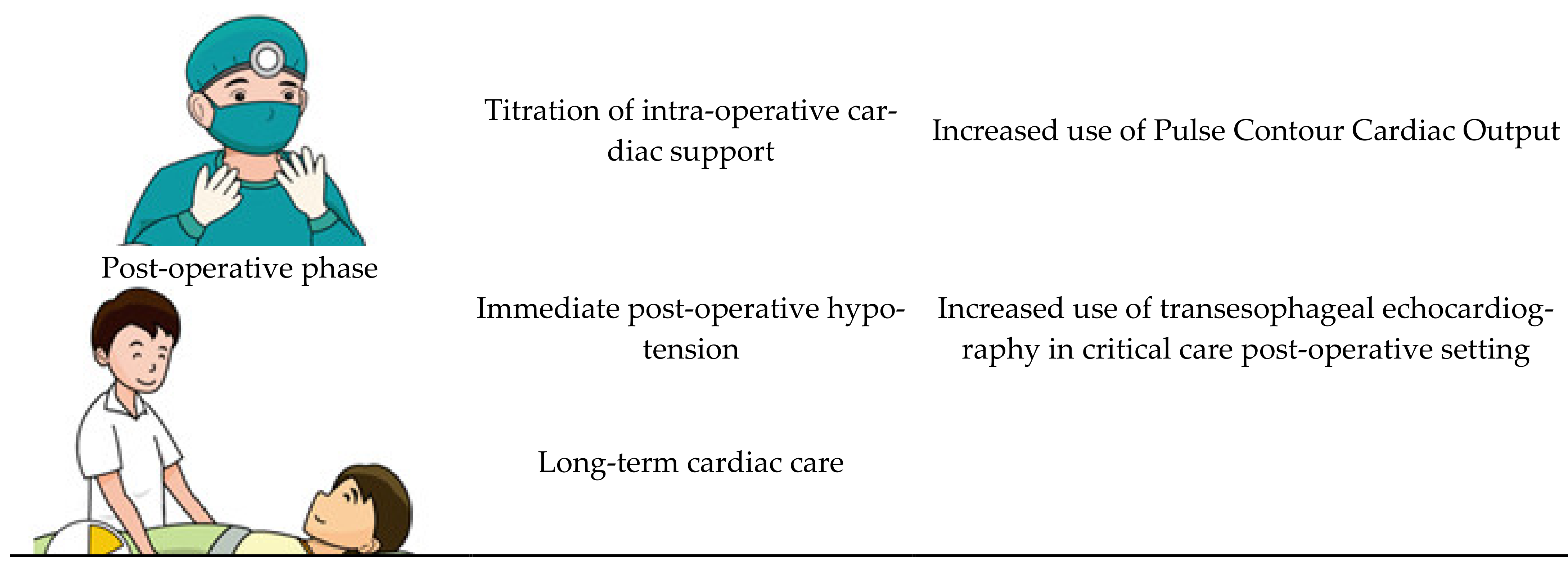
4. Treatment of CCM
4.1. β Blockade
4.2. Ivabradine
4.3. Liver Transplantation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Razpotnik, M.; Bota, S.; Wimmer, P.; Hackl, M.; Lesnik, G.; Alber, H.; Peck-Radosavljevic, M. The prevalence of cirrhotic cardiomyopathy according to different diagnostic criteria. Liver Int. 2020. [Google Scholar] [CrossRef]
- Desai, M.S.; Penny, D.J. Bile acids induce arrhythmias: Old metabolite, new tricks. Heart 2013, 99, 1629–1630. [Google Scholar] [CrossRef] [PubMed]
- Hamoudi, W.A.; Lee, S.S. Cirrhotic cardiomyopathy. Ann. Hepatol. 2006, 5, 132–139. [Google Scholar] [CrossRef]
- Møller, S.; Danielsen, K.V.; Wiese, S.; Hove, J.D.; Bendtsen, F. An update on cirrhotic cardiomyopathy. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Møller, S.; Henriksen, J.H. Cardiovascular complications of cirrhosis. Gut 2008, 57, 268–278. [Google Scholar] [CrossRef] [PubMed]
- Izzy, M.; VanWagner, L.B.; Lin, G.; Altieri, M.; Findlay, J.Y.; Oh, J.K.; Watt, K.D.; Lee, S.S. Redefining cirrhotic cardiomyopathy for the modern era. Hepatology 2020, 71, 334–345. [Google Scholar] [CrossRef] [PubMed]
- Glenn, T.K.; Honar, H.; Liu, H.; ter Keurs, H.E.; Lee, S.S. Role of cardiac myofilament proteins titin and collagen in the pathogenesis of diastolic dysfunction in cirrhotic rats. J. Hepatol. 2011, 55, 1249–1255. [Google Scholar] [CrossRef]
- Møller, S.; Bendtsen, F. The pathophysiology of arterial vasodilatation and hyperdynamic circulation in cirrhosis. Liver Int. 2018, 38, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Mallat, A.; Teixeira-Clerc, F.; Lotersztajn, S. Cannabinoid signaling and liver therapeutics. J. Hepatol. 2013, 59, 891–896. [Google Scholar] [CrossRef]
- Yang, Y.-Y.; Liu, H.; Nam, S.W.; Kunos, G.; Lee, S.S. Mechanisms of tnfα-induced cardiac dysfunction in cholestatic bile duct-ligated mice: Interaction between tnfα and endocannabinoids. J. Hepatol. 2010, 53, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Caraceni, P.; Domenicali, M.; Giannone, F.; Bernardi, M. The role of the endocannabinoid system in liver diseases. Best Pract. Res. Clin. Endocrinol. Metab. 2009, 23, 65–77. [Google Scholar] [CrossRef]
- Toshikuni, N.; Ozaki, K.; George, J.; Tsutsumi, M. Serum endocan as a survival predictor for patients with liver cirrhosis. Can. J. Gastroenterol. Hepatol. 2015, 29, 427–430. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Ma, Z.; Lee, S.S. Contribution of nitric oxide to the pathogenesis of cirrhotic cardiomyopathy in bile duct-ligated rats. Gastroenterology 2000, 118, 937–944. [Google Scholar] [CrossRef]
- Maines, M.D. The heme oxygenase system:A regulator of second messenger gases. Annu. Rev. Pharmacol. Toxicol. 1997, 37, 517–554. [Google Scholar] [CrossRef]
- Liu, H.; Song, D.; Lee, S.S. Role of heme oxygenase-carbon monoxide pathway in pathogenesis of cirrhotic cardiomyopathy in the rat. Am. J. Physiol.-Gastrointest. Liver Physiol. 2001, 280, G68–G74. [Google Scholar] [CrossRef] [PubMed]
- Bessa, S.S.E.-D.; Ali, E.M.M.; El-Wahab, A.E.-S.A.; El-Din, S.A.E.-M.N. Heme oxygenase-1 mrna expression in egyptian patients with chronic liver disease. Hepat. Mon. 2012, 12, 278–285. [Google Scholar] [CrossRef]
- Gazawi, H.; Ljubuncic, P.; Cogan, U.; Hochgraff, E.; Ben-Shachar, D.; Bomzon, A. The effects of bile acids on beta-adrenoceptors, fluidity, and the extent of lipid peroxidation in rat cardiac membranes. Biochem. Pharmacol. 2000, 59, 1623–1628. [Google Scholar] [CrossRef]
- Desai, M.S.; Zainuer, S.; Kennedy, C.; Kearney, D.; Goss, J.; Karpen, S.J. Cardiac structural and functional alterations in infants and children with biliary atresia, listed for liver transplantation. Gastroenterology 2011, 141, 1264–1272.e1–4. [Google Scholar] [CrossRef]
- Rainer, P.P.; Primessnig, U.; Harenkamp, S.; Doleschal, B.; Wallner, M.; Fauler, G.; Stojakovic, T.; Wachter, R.; Yates, A.; Groschner, K.; et al. Bile acids induce arrhythmias in human atrial myocardium--implications for altered serum bile acid composition in patients with atrial fibrillation. Heart 2013, 99, 1685–1692. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Marty, J.; Mantz, J.; Samain, E.; Braillon, A.; Lebrec, D. Desensitization of myocardial β-adrenergic receptors in cirrhotic rats. Hepatology 1990, 12, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Wiese, S.; Hove, J.D.; Bendtsen, F.; Møller, S. Cirrhotic cardiomyopathy: Pathogenesis and clinical relevance. Nat. Rev. Gastroenterol. Hepatol. 2013, 11, 177–186. [Google Scholar] [CrossRef]
- Lunseth, J.H.; Olmstead, E.G.; Forks, G.; Abboud, F. A study of heart disease in one hundred eight hospitalized patients dying with portal cirrhosis. Arch. Intern. Med. 1958, 102, 405–413. [Google Scholar] [CrossRef]
- Jellis, C.L.; Kwon, D.H. Myocardial t1 mapping: Modalities and clinical applications. Cardiovasc. Diagn. Ther. 2014, 4, 126–137. [Google Scholar] [PubMed]
- Wiese, S.; Voiosu, A.; Hove, J.D.; Danielsen, K.V.; Voiosu, T.; Grønbaek, H.; Møller, H.J.; Genovese, F.; Reese-Petersen, A.L.; Mookerjee, R.P.; et al. Fibrogenesis and inflammation contribute to the pathogenesis of cirrhotic cardiomyopathy. Aliment. Pharmacol. Ther. 2020, 52, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Marian, A.J.; Braunwald, E. Hypertrophic Cardiomyopathy: Genetics, Pathogenesis, Clinical Manifestations, Diagnosis, and Therapy. Circ. Res. 2017, 121, 749–770. [Google Scholar] [CrossRef]
- Bernardi, M.; Calandra, S.; Colantoni, A.; Trevisani, F.; Raimondo, M.L.; Sica, G.; Schepis, F.; Mandini, M.; Simoni, P.; Contin, M.; et al. Q-t interval prolongation in cirrhosis: Prevalence, relationship with severity, and etiology of the disease and possible pathogenetic factors. Hepatology 1998, 27, 28–34. [Google Scholar] [CrossRef]
- Ruíz-del-Árbol, L.; Serradilla, R. Cirrhotic cardiomyopathy. World J. Gastroenterol. 2015, 21, 11502. [Google Scholar] [CrossRef] [PubMed]
- Ward, C.A.; Liu, H.; Lee, S.S. Altered cellular calcium regulatory systems in a rat model of cirrhotic cardiomyopathy. Gastroenterology 2001, 121, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
- Jaue, D.; Ma, Z.; Lee, S. Cardiac muscarinic receptor function in rats with cirrhotic cardiomyopathy. Hepatology 1997, 25, 1361–1365. [Google Scholar] [CrossRef]
- Oh, J.K.; Hatle, L.; Tajik, A.J.; Little, W.C. Diastolic heart failure can be diagnosed by comprehensive two-dimensional and doppler echocardiography. J. Am. Coll. Cardiol. 2006, 47, 500–506. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the american society of echocardiography and the european association of cardiovascular imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Farr, M.; Schulze, P.C. Recent advances in the diagnosis and management of cirrhosis-associated cardiomyopathy in liver transplant candidates: Advanced echo imaging, cardiac biomarkers, and advanced heart failure therapies. Clin. Med. Insights Cardiol. 2014, 8, CMC-S15722. [Google Scholar] [CrossRef] [PubMed]
- Timoh, T.; Protano, M.; Wagman, G.; Bloom, M.; Vittorio, T. A perspective on cirrhotic cardiomyopathy. Transplant. Proc. 2011, 43, 1649–1653. [Google Scholar] [CrossRef] [PubMed]
- Buggey, J.; Alenezi, F.; Yoon, H.J.; Phelan, M.; DeVore, A.D.; Khouri, M.G.; Schulte, P.J.; Velazquez, E.J. Left ventricular global longitudinal strain in patients with heart failure with preserved ejection fraction: Outcomes following an acute heart failure hospitalization. ESC Heart Fail. 2017, 4, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Mechelinck, M.; Hartmann, B.; Hamada, S.; Becker, M.; Andert, A.; Ulmer, T.F.; Neumann, U.P.; Wirtz, T.H.; Koch, A.; Trautwein, C.; et al. Global longitudinal strain at rest as an independent predictor of mortality in liver transplant candidates: A retrospective clinical study. J. Clin. Med. 2020, 9, 2616. [Google Scholar] [CrossRef] [PubMed]
- Isaak, A.; Praktiknjo, M.; Jansen, C.; Faron, A.; Sprinkart, A.M.; Pieper, C.C.; Chang, J.; Fimmers, R.; Meyer, C.; Dabir, D.; et al. Myocardial fibrosis and inflammation in liver cirrhosis: Mri study of the liver-heart axis. Radiology 2020, 297, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Silvestre, O.M.; Farias, A.Q.; Ramos, D.S.; Furtado, M.S.; Rodrigues, A.C.; Ximenes, R.O.; de Campos Mazo, D.F.; Yoshimura Zitelli, P.M.; Diniz, M.A.; Andrade, J.L.; et al. β-blocker therapy for cirrhotic cardiomyopathy: A randomized-controlled trial. Eur. J. Gastroenterol. Hepatol. 2018, 30, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Zardi, E.M.; Zardi, D.M.; Chin, D.; Sonnino, C.; Dobrina, A.; Abbate, A. Cirrhotic cardiomyopathy in the pre- and post-liver transplantation phase. J. Cardiol. 2016, 67, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Nanashima, A.; Pillay, P.; Crawford, M.; Nakasuji, M.; Verran, D.J.; Painter, D. Analysis of postrevascularization syndrome after orthotopic liver transplantation: The experience of an Australian liver transplantation center. J. Hepatobiliary Pancreat. Surg. 2001, 8, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Premkumar, M.; Rangegowda, D.; Vyas, T.; Khumuckham, J.S.; Shasthry, S.M.; Thomas, S.S.; Goyal, R.; Kumar, G.; Sarin, S.K. Carvedilol combined with ivabradine improves left ventricular diastolic dysfunction, clinical progression, and survival in cirrhosis. J. Clin. Gastroenterol. 2019, 54, 561–568. [Google Scholar] [CrossRef]
- Merit-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL randomised intervention trial in-congestive heart failure (MERIT-HF). Lancet 1999, 353, 2001–2007. [Google Scholar] [CrossRef]
- Swedberg, K.; Komajda, M.; Böhm, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L.; SHIFT Investigators. Ivabradine and outcomes in chronic heart failure (shift): A randomised placebo-controlled study. Lancet 2010, 376, 875–885. [Google Scholar] [CrossRef]
- Liu, H.; Jayakumar, S.; Traboulsi, M.; Lee, S.S. Cirrhotic cardiomyopathy: Implications for liver transplantation. Liver Transplant. 2017, 23, 826–835. [Google Scholar] [CrossRef]
- Carvalho, M.; Kroll, P.; Kroll, R.; Carvalho, V. Cirrhotic cardiomyopathy: The liver affects the heart. Braz. J. Med. Biol. Res. 2019, 52. [Google Scholar] [CrossRef] [PubMed]
- Gorgis, N.M.; Kennedy, C.; Lam, F.; Thompson, K.; Coss-Bu, J.; Akcan Arikan, A.; Nguyen, T.; Hosek, K.; Miloh, T.; Karpen, S.J.; et al. Clinical Consequences of Cardiomyopathy in Children With Biliary Atresia Requiring Liver Transplantation. Hepatology 2019, 69, 1206–1218. [Google Scholar] [CrossRef]
- Junge, N.; Junge, C.; Schröder, J.; Pfister, E.D.; Leiskau, C.; Hohmann, D.; Beerbaum, P.; Baumann, U. Pediatric cirrhotic cardiomyopathy: Impact on liver transplant outcomes. Liver Transpl. 2018, 24, 820–830. [Google Scholar] [CrossRef] [PubMed]
- Pietri, L.D.; Mocchegiani, F.; Leuzzi, C.; Montalti, R.; Vivarelli, M.; Agnoletti, V. Transoesophageal echocardiography during liver transplantation. World J. Hepatol. 2015, 7, 2432. [Google Scholar] [CrossRef]
- Della Rocca, G.; Costa, M.G.; Pompei, L.; Chiarandini, P. The liver transplant recipient with cardiac disease. Transplant. Proc. 2008, 40, 1172–1174. [Google Scholar] [CrossRef]
- Oxorn, D.C. Intraoperative echocardiography. Heart 2008, 94, 1236–1243. [Google Scholar] [CrossRef]
- Gaskari, S.A.; Honar, H.; Lee, S.S. Therapy insight: Cirrhotic cardiomyopathy. Nat. Clin. Pract. Gastroenterol. Hepatol. 2006, 3, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Voiosu, A.M.; Bălănescu, P.; Daha, I.; Smarandache, B.; Rădoi, A.; Mateescu, R.B.; Băicuş, C.R.; Voiosu, T.A. The diagnostic and prognostic value of serum endocan in patients with cirrhotic cardiomyopathy. Rom. J. Intern. Med. 2018, 56, 182–192. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Systolic Dysfunction | Diastolic Dysfunction | Supportive Criteria |
|---|---|---|
| Blunted increase in cardiac output on exercise, volume challenge or pharmacological stimuli | E/A ratio <1.0 (age-corrected) | Prolonged Q-Tc interval |
| Resting ejection fraction <55% | Prolonged deceleration time (<200 ms) | Enlarged left atrium |
| Prolonged isovolumetric relaxation time (<80 ms) | Increased myocardial mass | |
| Electrophysiological abnormalities | Increased BNP and pro-BNP | |
| Abnormal chronotropic response | Increased troponin I | |
| Electromechanical uncoupling/dys-synchrony |
| Systolic Dysfunction | Advanced Diastolic Dysfunction | Areas for Future Research Which Require Further Validation |
|---|---|---|
| Any of the following LV ejection fraction ≤50 % | ≥3 of the following | Abnormal chronotropic or inotropic response |
| Absolute GLS <18% or >22% | Septal é velocity <7 cm/s | Electrocardiographic changes |
| E/é ratio ≥15 | Electromechanical uncoupling | |
| LAVI >34 mL/m2 | Myocardial mass change | |
| TR velocity >2.8 m/s | Serum biomarkers | |
| Chamber enlargement | ||
| CMRI |
| Parameter | Units | Normal Range | Cirrhotic Cardiomyopathy | Definition |
|---|---|---|---|---|
| Cardiac Index | L/min/m2 | 2.9 | 3.7 | Cardiac output per surface area. Elevated in CCM due to hyperdynamic circulation |
| Left atrial volume | mL/m2 | 34 | 53 | End-diastolic left atrial volume. Increased in CCM and is load independent |
| Late Gadolinium Enhancement | No enhancement | Enhancement present | Gadolinium deposition within areas of myocardium disruption | |
| Longitudinal Strain | % | −22.5 | −18.5 | Reduced in CCM due to reduced deformation of the LV during systole |
| T1 Relaxation time | msecond | 958 | 1008 | Indicator of ventricle tissue integrity |
| T2 Relaxation time | msecond | 53 | 59 | Indicator of oedema within ventricular tissue |
| Extracellular volume fraction | % | 23 | 34 | Measurement of the extracellular volume within the myocardium. Marker of peri-cellular oedema |
| Parameters | Child-Pugh A | Child-Pugh B | Child-Pugh C |
|---|---|---|---|
| Late gadolinium enhancement | 1.6% | 4.3% | 13.1% |
| Amount of gadolinium deposited in extracellular space | |||
| Control (0%) | |||
| T1 relaxation time | 978 ms | 1006 ms | 1044 ms |
| Colored mapping during T1 phase, | |||
| Indicator of ventricle tissue integrity | |||
| Control (958 ms) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longley, K.; Tran, T.; Ho, V. Cirrhotic Cardiomyopathy. Gastroenterol. Insights 2021, 12, 76-88. https://doi.org/10.3390/gastroent12010008
Longley K, Tran T, Ho V. Cirrhotic Cardiomyopathy. Gastroenterology Insights. 2021; 12(1):76-88. https://doi.org/10.3390/gastroent12010008
Chicago/Turabian StyleLongley, Kieran, Tuan Tran, and Vincent Ho. 2021. "Cirrhotic Cardiomyopathy" Gastroenterology Insights 12, no. 1: 76-88. https://doi.org/10.3390/gastroent12010008
APA StyleLongley, K., Tran, T., & Ho, V. (2021). Cirrhotic Cardiomyopathy. Gastroenterology Insights, 12(1), 76-88. https://doi.org/10.3390/gastroent12010008