
Identifying High-Risk Events for COVID-19 Transmission: Estimating the Risk of Clustering Using Nationwide Data


Abstract
:1. Introduction
2. Materials and Methods
2.1. Cluster Surveillance Data
2.2. Event Frequency and Users
2.3. Estimating the Risk of Clustering
2.4. Sensitivity Analysis on the Estimates
2.5. Simulation-Based Bias Assessment
2.6. Evaluation on the Consistency of Reporting througout the Study Period
3. Results
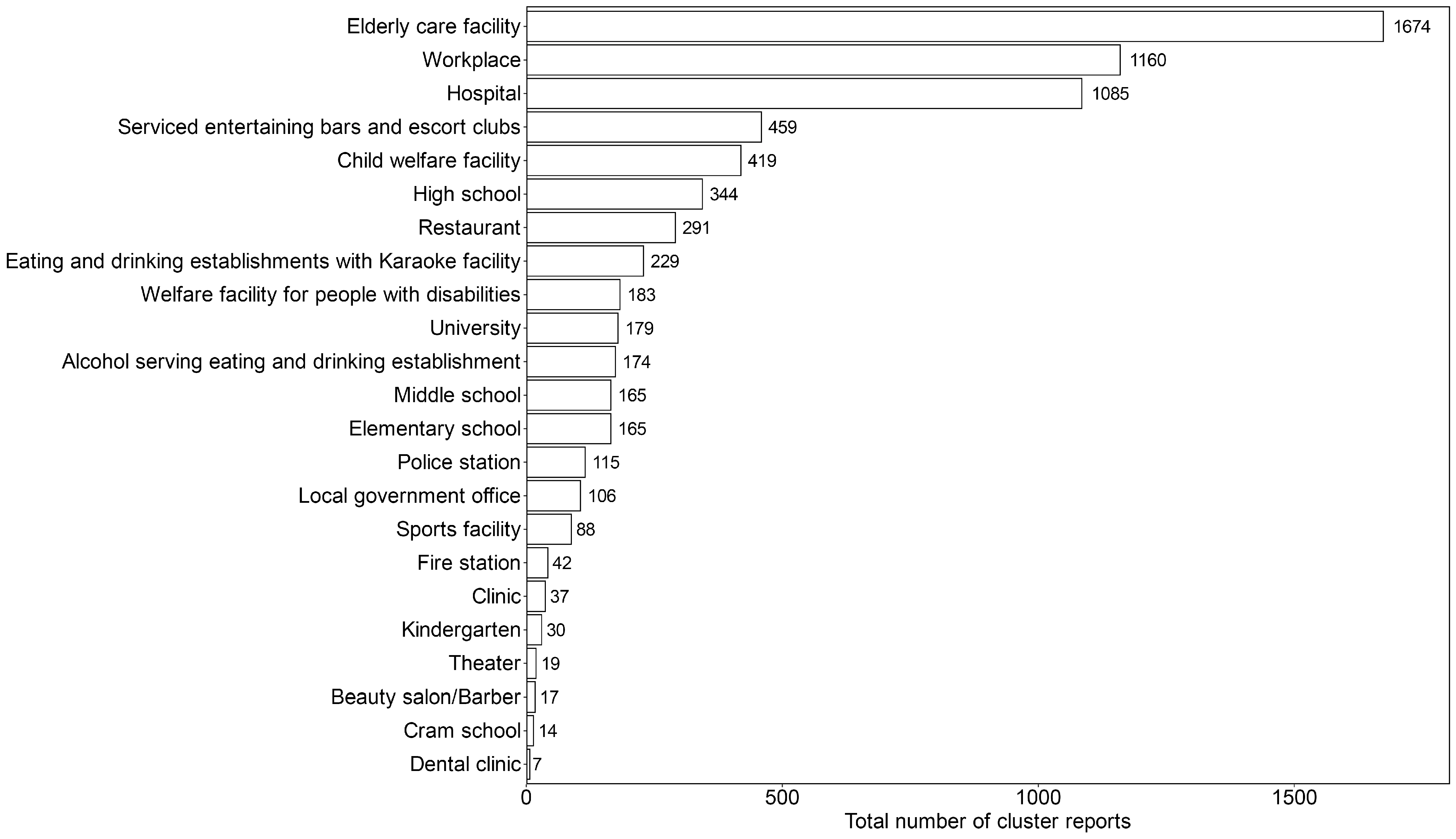
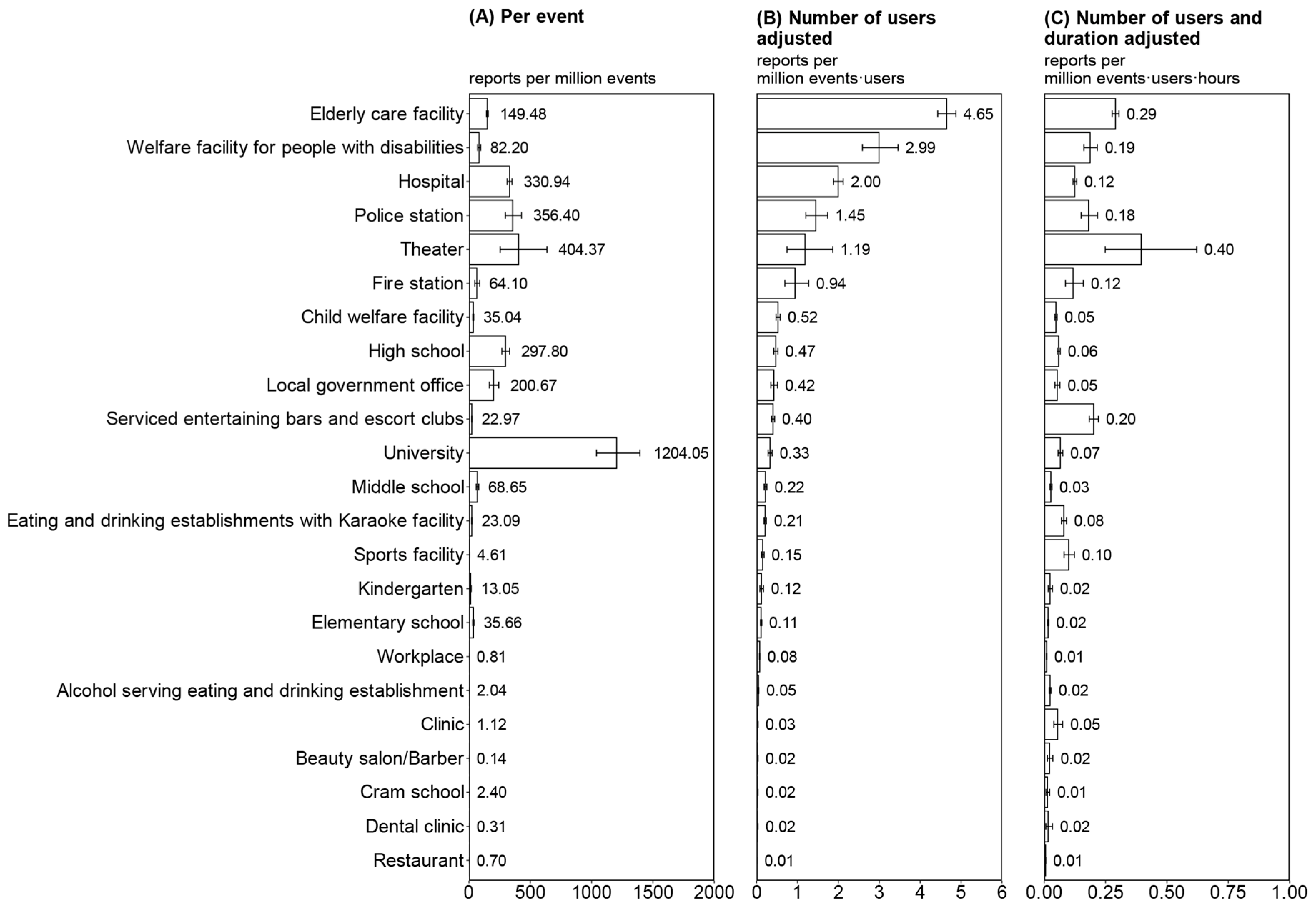
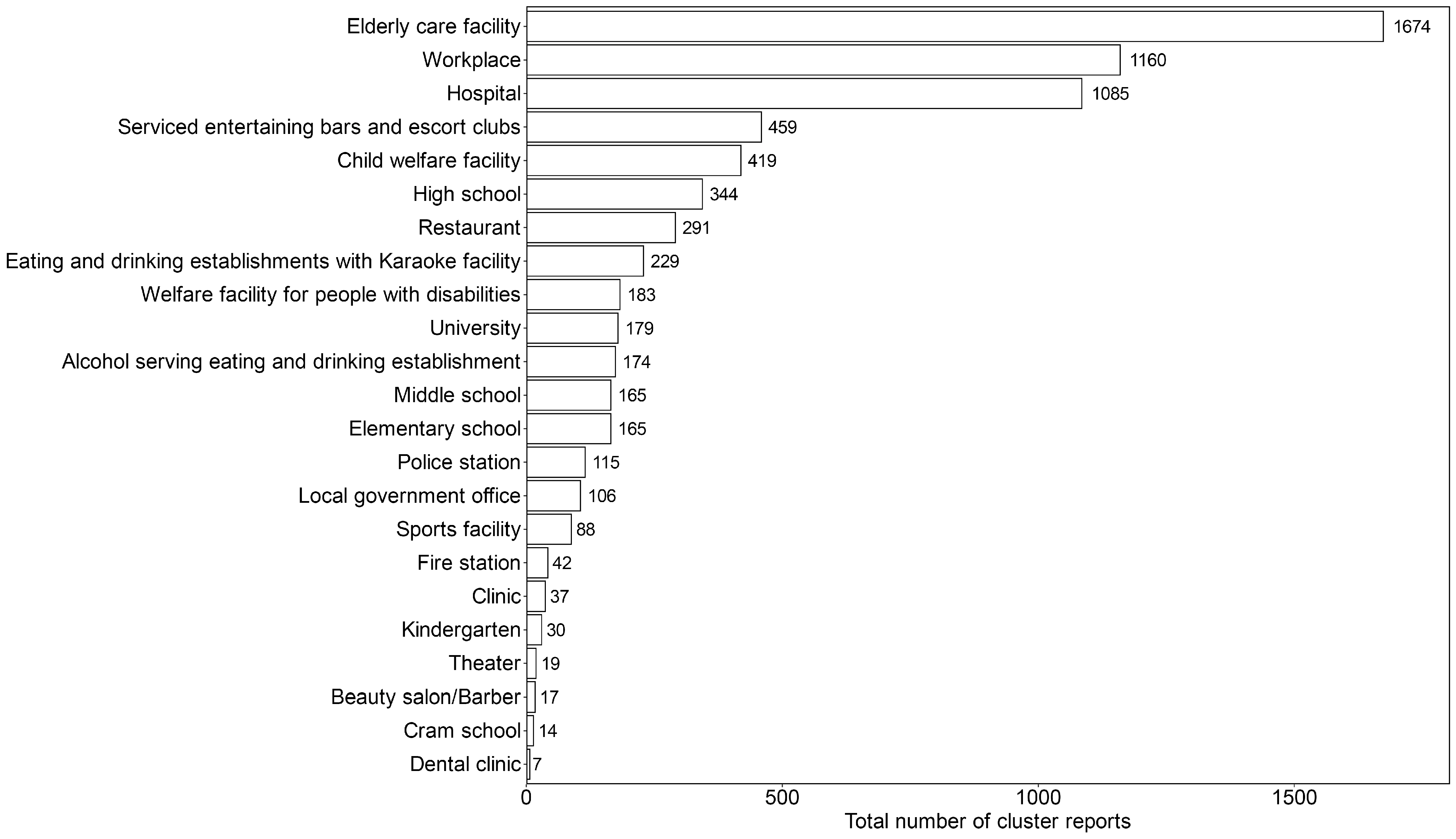
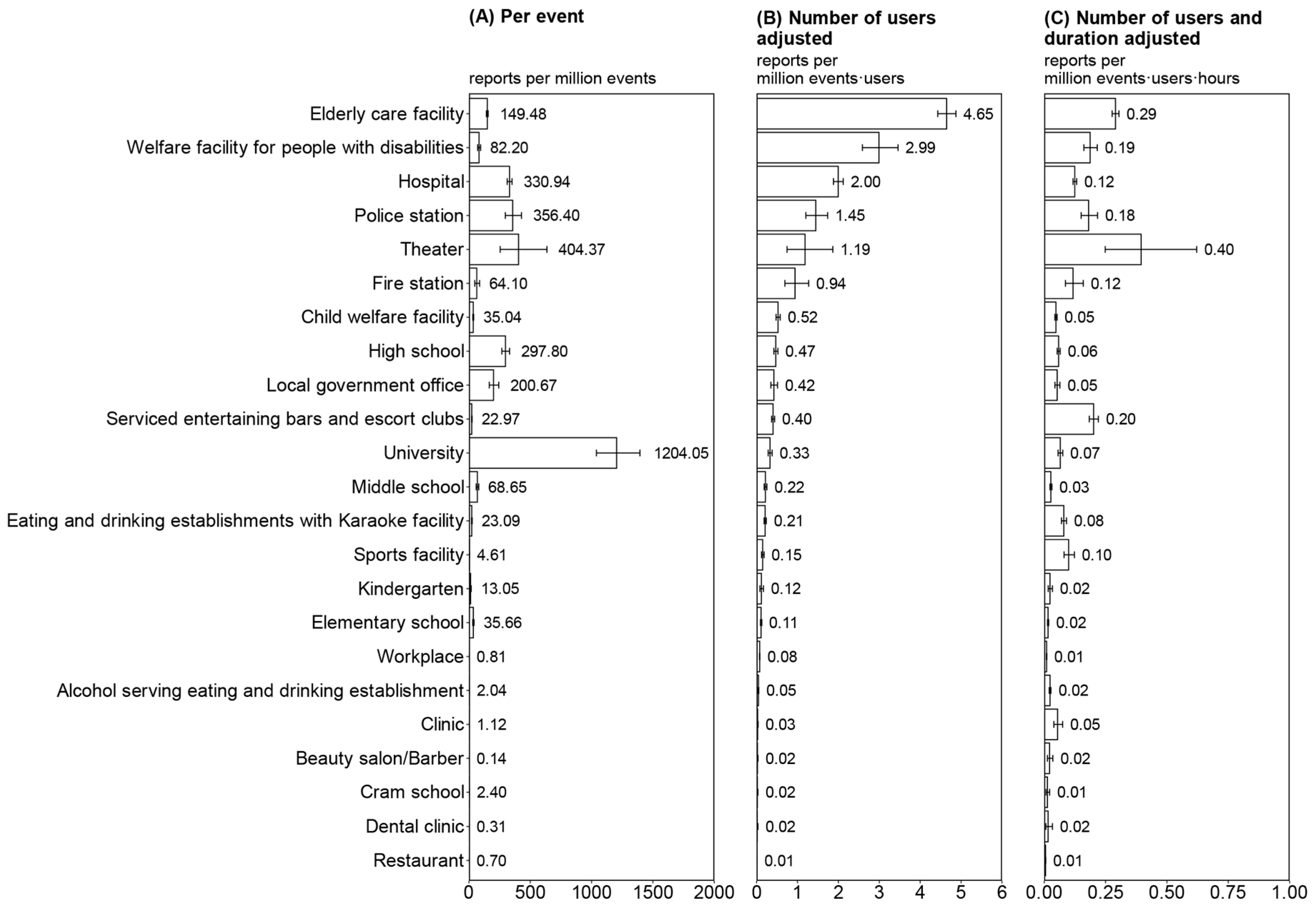
3.1. Activity-Dependent Cluster Infection Risk Index
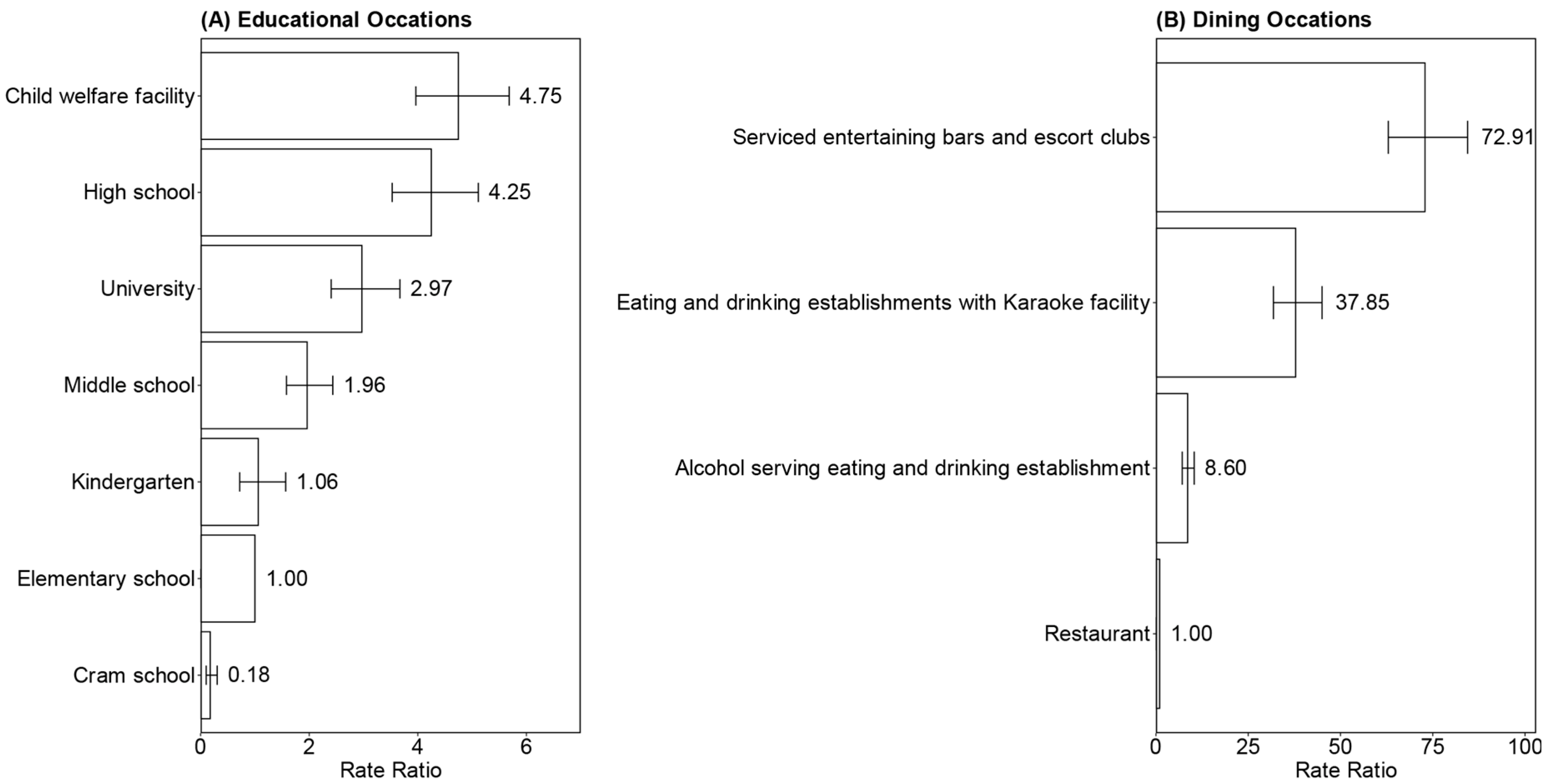
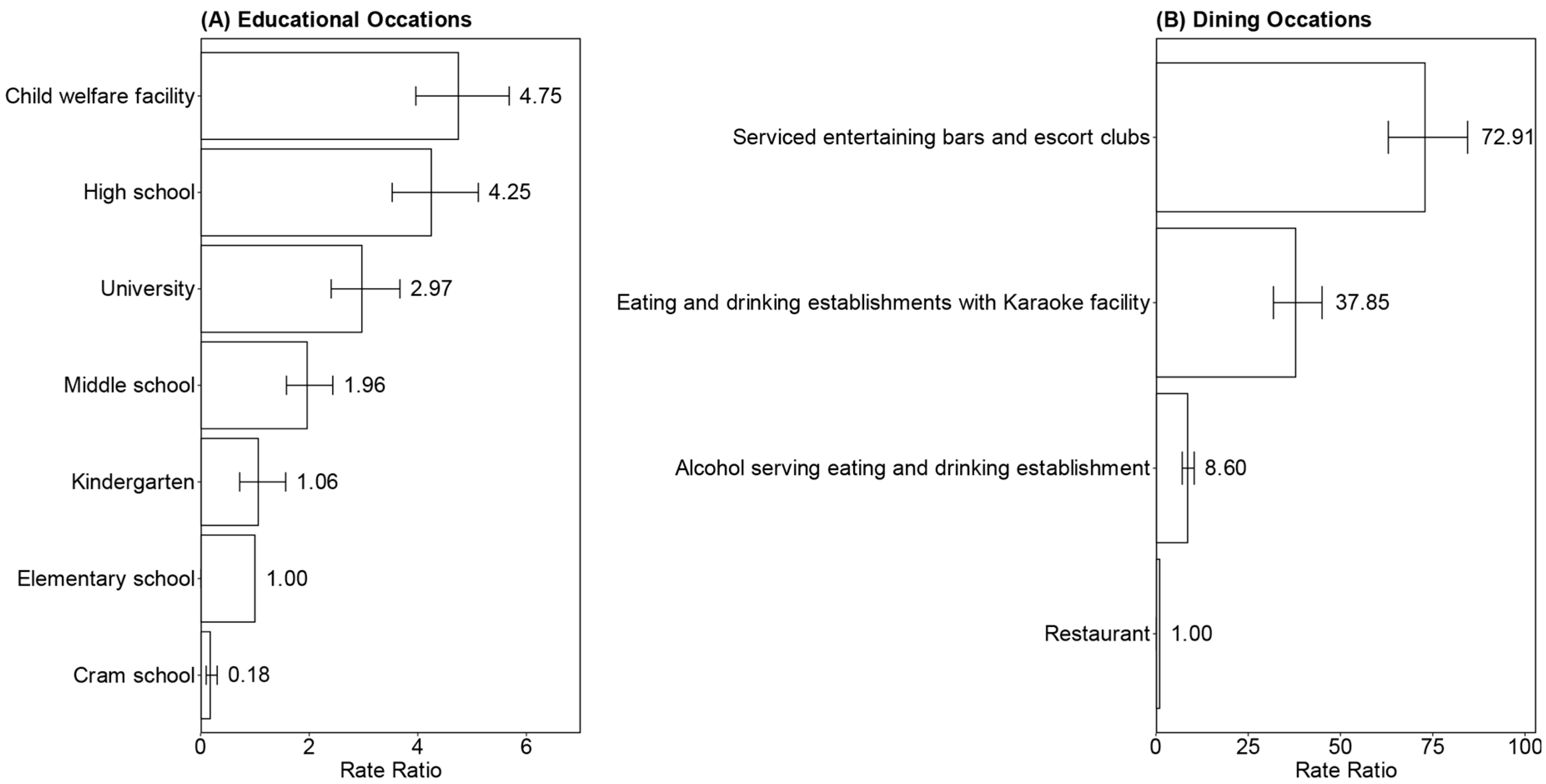
3.2. Rate Ratios of Activity-Dependent Risk
3.3. Sensitivity Analysis of the Risk Index and RR
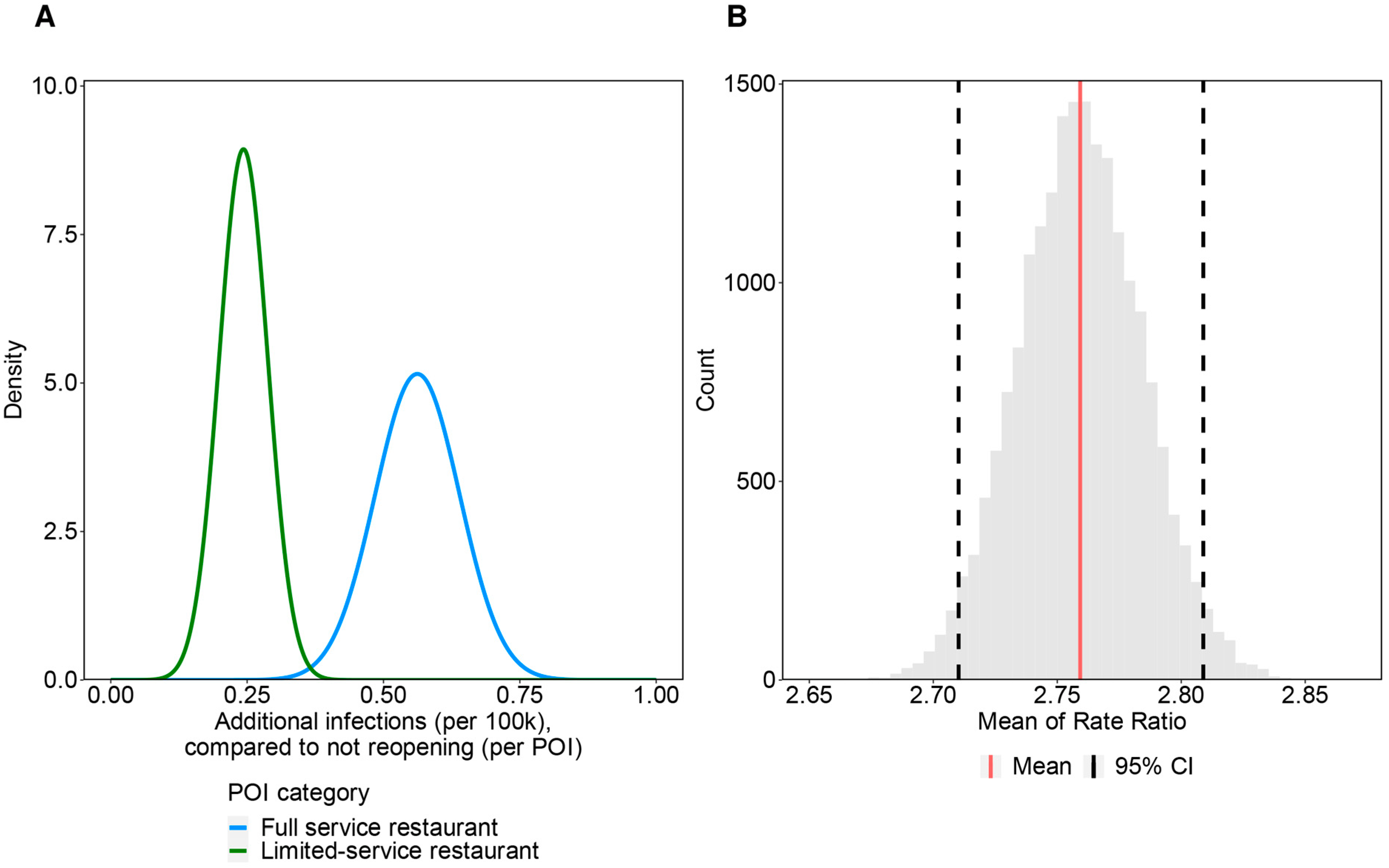
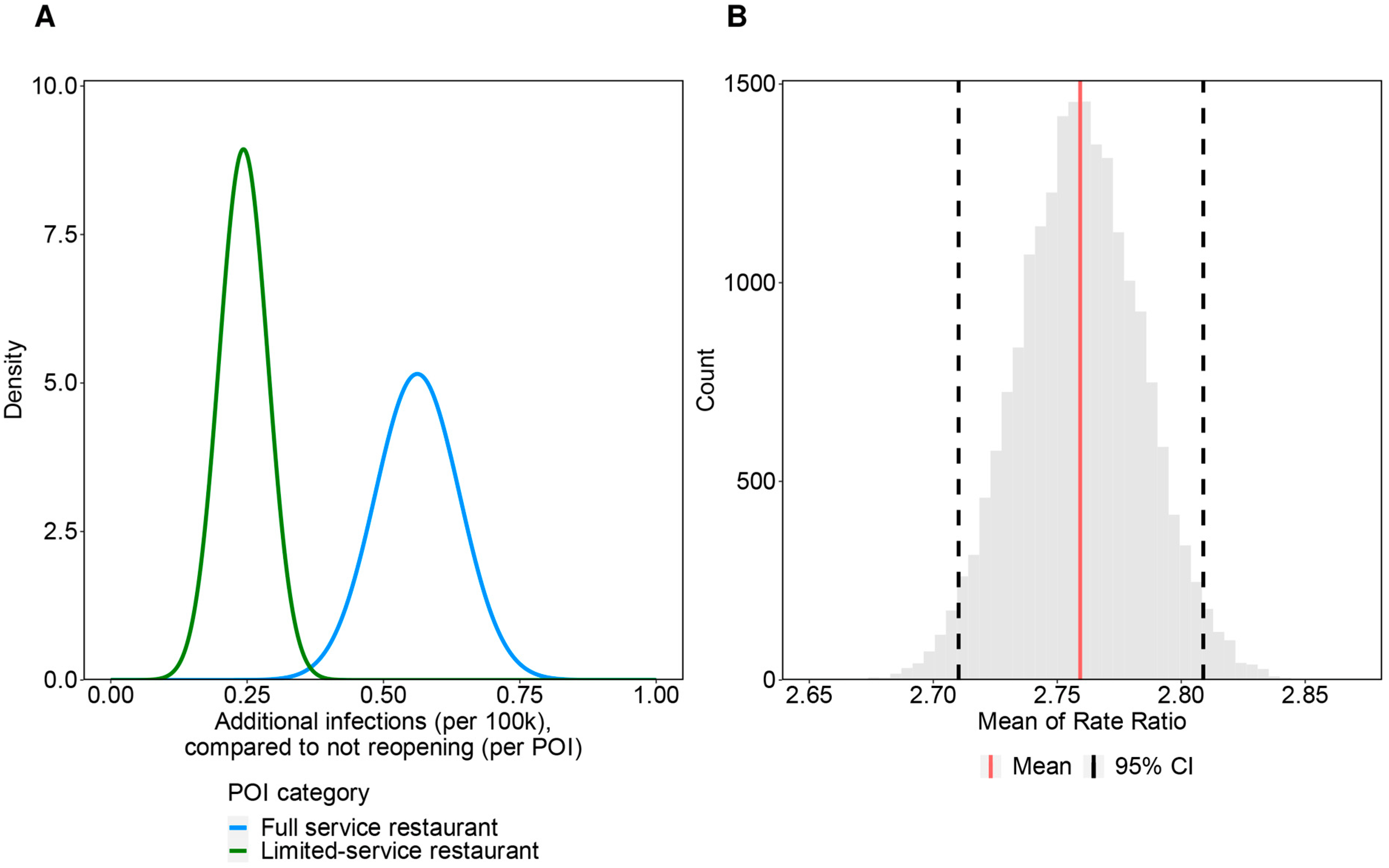
3.4. Simulation-Based Bias Assessment
3.5. Evaluation on the Consistency of Reporting throughout the Study Period
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 23 March 2022).
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The Positive Impact of Lockdown in Wuhan on Containing the COVID-19 Outbreak in China. J. Travel Med. 2020, 27, taaa037. [Google Scholar] [CrossRef] [PubMed]
- International Monetary Fund. World Economic Outlook, April 2020: The Great Lockdown. Available online: https://www.imf.org/en/Publications/WEO/Issues/2020/04/14/weo-april-2020 (accessed on 28 December 2021).
- Sibley, C.G.; Greaves, L.M.; Satherley, N.; Wilson, M.S.; Overall, N.C.; Lee, C.H.J.; Milojev, P.; Bulbulia, J.; Osborne, D.; Milfont, T.L.; et al. Effects of the COVID-19 Pandemic and Nationwide Lockdown on Trust, Attitudes Toward Government, and Well-Being. Am. Psychol. 2020, 75, 618–630. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Infectious Diseases, Japan. Guideline for Execution of Active Epidemiological Investigation on Patients Infected to COVID-19 (Edition as of 12 March 2020). Available online: https://www.niid.go.jp/niid/images/epi/corona/2019nCoV-02-200312.pdf (accessed on 20 December 2021).
- Endo, A.; Abbott, S.; Kucharski, A.J.; Funk, S. Estimating the Overdispersion in COVID-19 Transmission Using Outbreak Sizes Outside China [Version 3; Peer Review: 2 Approved]. Wellcome Open Res. 2020, 5, 67. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Han, C.; Jung, J.; Lee, S. Analysis of Superspreading Potential from Transmission Clusters of COVID-19 in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 12893. [Google Scholar] [CrossRef]
- Tariq, A.; Lee, Y.; Roosa, K.; Blumberg, S.; Yan, P.; Ma, S.; Chowell, G. Real-Time Monitoring the Transmission Potential of COVID-19 in Singapore, March 2020. BMC Med. 2020, 18, 166. [Google Scholar] [CrossRef]
- Wang, L.; Didelot, X.; Yang, J.; Wong, G.; Shi, Y.; Liu, W.; Gao, G.F.; Bi, Y. Inference of Person-to-Person Transmission of COVID-19 Reveals Hidden Super-Spreading Events during the Early Outbreak Phase. Nat. Commun. 2020, 11, 5006. [Google Scholar] [CrossRef]
- Nakajo, K.; Nishiura, H. Transmissibility of Asymptomatic COVID-19: Data from Japanese Clusters. Int. J. Infect. Dis. 2021, 105, 236–238. [Google Scholar] [CrossRef]
- Adam, D.C.; Wu, P.; Wong, J.Y.; Lau, E.H.Y.; Tsang, T.K.; Cauchemez, S.; Leung, G.M.; Cowling, B.J. Clustering and Superspreading Potential of SARS-CoV-2 Infections in Hong Kong. Nat. Med. 2020, 26, 1714–1719. [Google Scholar] [CrossRef]
- Kwok, K.O.; Chan, H.H.H.; Huang, Y.; Hui, D.S.C.; Tambyah, P.A.; Wei, W.I.; Chau, P.Y.K.; Wong, S.Y.S.; Tang, J.W.T. Inferring Super-Spreading from Transmission Clusters of COVID-19 in Hong Kong, Japan, and Singapore. J. Hosp. Infect. 2020, 105, 682–685. [Google Scholar] [CrossRef]
- Endo, A.; Centre for the Mathematical Modelling of Infectious Diseases COVID-19 Working Group; Leclerc, Q.J.; Knight, G.M.; Medley, G.F.; Atkins, K.E.; Funk, S.; Kucharski, A.J. Implication of Backward Contact Tracing in the Presence of Overdispersed Transmission in COVID-19 Outbreaks [Version 3; Peer Review: 2 Approved]. Wellcome Open Res. 2021, 5, 239. [Google Scholar] [CrossRef]
- Expert Meeting on COVID-19 Prevention, Japan. Opinion on COVID-19 Prevention. Available online: https://www.mhlw.go.jp/content/10900000/000606000.pdf (accessed on 20 December 2021).
- Hayashi, K.; Kayano, T.; Anzai, A.; Fujimoto, M.; Linton, N.; Sasanami, M.; Suzuki, A.; Kobayashi, T.; Otani, K.; Yamauchi, M.; et al. Assessing Public Health and Social Measures against COVID-19 in Japan From March to June 2021. Front. Med. 2022, 9, 937732. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Scientific Brief: SARS-CoV-2 Transmission. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/sars-cov-2-transmission.html (accessed on 3 December 2021).
- Setti, L.; Passarini, F.; De Gennaro, G.; Barbieri, P.; Perrone, M.G.; Borelli, M.; Palmisani, J.; Di Gilio, A.; Piscitelli, P.; Miani, A. Airborne Transmission Route of COVID-19: Why 2 Meters/6 Feet of Inter-Personal Distance Could Not Be Enough. Int. J. Env. Res. Public Health 2020, 17, 2932. [Google Scholar] [CrossRef]
- Stadnytskyi, V.; Bax, C.E.; Bax, A.; Anfinrud, P. The Airborne Lifetime of Small Speech Droplets and Their Potential Importance in SARS-CoV-2 Transmission. Proc. Natl. Acad. Sci. USA 2020, 117, 11875–11877. [Google Scholar] [CrossRef]
- Department for Digital, Culture, Media & Sport. Science Note-Emerging Findings from Studies of Indicators of SARS-CoV-2 Transmission Risk at the Events Research Programme: Environment, Crowd Densities and Attendee Behaviour. Available online: https://www.gov.uk/government/publications/events-research-programme-phase-ii-and-iii-findings/science-note-emerging-findings-from-studies-of-indicators-of-sars-cov-2-transmission-risk-at-the-events-research-programme-environment-crowd-densi (accessed on 22 December 2021).
- Leclerc, Q.J.; Fuller, N.M.; Knight, L.E.; Group, C.C.W.; Funk, S.; Knight, G.M. What Settings Have Been Linked to SARS-CoV-2 Transmission Clusters? [Version 2; Peer Review: 2 Approved]. Wellcome Open Res. 2020, 5, 83. [Google Scholar] [CrossRef]
- Nishiura, H.; Oshitani, H.; Kobayashi, T.; Saito, T.; Sunagawa, T.; Matsui, T.; Wakita, T.; MHLW COVID-19 Response Team; Suzuki, M. Closed Environments Facilitate Secondary Transmission of Coronavirus Disease 2019 (COVID-19). Available online: http://medrxiv.org/lookup/doi/10.1101/2020.02.28.20029272 (accessed on 6 December 2021).
- Lu, J.; Gu, J.; Li, K.; Xu, C.; Su, W.; Lai, Z.; Zhou, D.; Yu, C.; Xu, B.; Yang, Z. COVID-19 Outbreak Associated with Air Conditioning in Restaurant, Guangzhou, China, 2020. Emerg. Infect. Dis. 2020, 26, 1628–1631. [Google Scholar] [CrossRef]
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic Analysis of SARS-CoV-2 in Two Wuhan Hospitals. Nature 2020, 582, 557–560. [Google Scholar] [CrossRef]
- Furuse, Y.; Sando, E.; Tsuchiya, N.; Miyahara, R.; Yasuda, I.; Ko, Y.K.; Saito, M.; Morimoto, K.; Imamura, T.; Shobugawa, Y.; et al. Clusters of Coronavirus Disease in Communities, Japan, January 2020. Emerg. Infect. Dis. 2020, 26, 2176–2179. [Google Scholar] [CrossRef]
- Hamner, L. High SARS-CoV-2 Attack Rate Following Exposure at a Choir Practice Skagit County, Washington, March 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 606–610. [Google Scholar] [CrossRef]
- Atrubin, D. An Outbreak of COVID-19 Associated with a Recreational Hockey Game Florida, June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1492–1493. [Google Scholar] [CrossRef]
- Atherstone, C. SARS-CoV-2 Transmission Associated with High School Wrestling Tournaments Florida, December 2020—January 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 141–143. [Google Scholar] [CrossRef]
- Jang, S.; Han, S.H.; Rhee, J.-Y. Cluster of Coronavirus Disease Associated with Fitness Dance Classes, South Korea. Emerg. Infect. Dis. 2020, 26, 1917–1920. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.; Kim, H.; Jung, T.-Y.; Lim, J.-A.; Jo, D.-H.; Kang, G.-S.; Jeong, S.-H.; Choi, D.-K.; Kim, H.-J.; Cheon, Y.H.; et al. Epidemiological Characteristics of COVID-19 Outbreak at Fitness Centers in Cheonan, Korea. J. Korean Med. Sci. 2020, 35, e288. [Google Scholar] [CrossRef] [PubMed]
- Alsved, M.; Matamis, A.; Bohlin, R.; Richter, M.; Bengtsson, P.-E.; Fraenkel, C.-J.; Medstrand, P.; Löndahl, J. Exhaled Respiratory Particles during Singing and Talking. Aerosol. Sci. Technol. 2020, 54, 1245–1248. [Google Scholar] [CrossRef]
- Dougherty, K. SARS-CoV-2 B.1.617.2 (Delta) Variant COVID-19 Outbreak Associated with a Gymnastics Facility Oklahoma, April 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1004–1007. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.A. Community and Close Contact Exposures Associated with COVID-19 among Symptomatic Adults ≥ 18 Years in 11 Outpatient Health Care Facilities United States, July 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1258–1264. [Google Scholar] [CrossRef]
- Ge, Y.; Martinez, L.; Sun, S.; Chen, Z.; Zhang, F.; Li, F.; Sun, W.; Chen, E.; Pan, J.; Li, C.; et al. COVID-19 Transmission Dynamics among Close Contacts of Index Patients with COVID-19: A Population-Based Cohort Study in Zhejiang Province, China. JAMA Intern. Med. 2021, 181, 1343–1350. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among Front-Line Health-Care Workers and the General Community: A Prospective Cohort Study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Hiironen, I.; Saavedra-Campos, M.; Panitz, J.; Ma, T.; Nsonwu, O.; Charlett, A.; Hughes, G.; Oliver, I. Occupational Exposures Associated with Being a COVID-19 Case; Evidence from Three Case-Controls Studies. Available online: https://www.medrxiv.org/content/10.1101/2020.12.21.20248161v1 (accessed on 2 December 2021).
- European Centre for Disease Prevention and Control. COVID-19 Clusters and Outbreaks in Occupational Settings in the EU/EEA and the UK. Available online: https://www.ecdc.europa.eu/en/publications-data/covid-19-clusters-and-outbreaks-occupational-settings-eueea-and-uk (accessed on 2 December 2021).
- Pray, I.W.; Kocharian, A.; Mason, J.; Westergaard, R.; Meiman, J. Trends in Outbreak-Associated Cases of COVID-19 Wisconsin, March 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 114–117. [Google Scholar] [CrossRef]
- Environmental Modelling Group Transmission Group. Insights on Transmission of COVID-19 with a Focus on the Hospitality, Retail and Leisure Sector. Available online: https://www.gov.uk/government/publications/emg-transmission-group-insights-on-transmission-of-covid-19-with-a-focus-on-the-hospitality-retail-and-leisure-sector-8-april-2021 (accessed on 20 December 2021).
- National Institute of Infectious Diseases, Japan. Case-Control Study of the Social Activity and Behavioral Risks of COVID-19 Infection in Unvaccinated Individuals (Provisional Report). Available online: https://www.niid.go.jp/niid/ja/2019-ncov/2484-idsc/10692-covid19-59.html (accessed on 20 December 2021).
- Chang, S.; Pierson, E.; Koh, P.W.; Gerardin, J.; Redbird, B.; Grusky, D.; Leskovec, J. Mobility Network Models of COVID-19 Explain Inequities and Inform Reopening. Nature 2021, 589, 82–87. [Google Scholar] [CrossRef]
- Wong, N.S.; Lee, S.S.; Kwan, T.H.; Yeoh, E.-K. Settings of Virus Exposure and Their Implications in the Propagation of Transmission Networks in a COVID-19 Outbreak. Lancet Reg. Health West. Pac. 2020, 4, 100052. [Google Scholar] [CrossRef]
- Infectious Disease Society of America. What the Experts Say about COVID-19 Risks. Available online: https://www.idsociety.org/globalassets/idsa/public-health/covid-19/activity-risk.pdf (accessed on 20 December 2021).
- Fontanet, A.; Tondeur, L.; Grant, R.; Temmam, S.; Madec, Y.; Bigot, T.; Grzelak, L.; Cailleau, I.; Besombes, C.; Ungeheuer, M.-N.; et al. SARS-CoV-2 Infection in Schools in a Northern French City: A Retrospective Serological Cohort Study in an Area of High Transmission, France, January to April 2020. Euro Surveill. 2021, 26, 2001695. [Google Scholar] [CrossRef]
- Swedish National Board of Health. Prevalence of COVID-19 in Different Occupational Groups. Available online: https://www.folkhalsomyndigheten.se/publicerat-material/publikationsarkiv/f/forekomst-av-covid-19-i-olika-yrkesgrupper/ (accessed on 20 December 2021).
- National Institute of Infectious Diseases, Japan. Guideline for Execution of Active Epidemiological Investigation on Patients Infected to COVID-19 (Edition as of 29 November 2021). Available online: https://www.niid.go.jp/niid/ja/2019-ncov/2559-cfeir/10800-covid19-02.html (accessed on 20 December 2021).
- Ministry of Health, Labor, and Welfare, Japan. Prevention of the Spread of Infection and Preparation of Medical Care Provision System. Available online: https://www.mhlw.go.jp/stf/covid-19/kansenkakudaiboushi-iryouteikyou.html (accessed on 20 December 2021).
- Ministry of Health, Labor, and Welfare, Japan. Testing of COVID-19. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000121431_00132.html (accessed on 20 December 2021).
- Agresti, A.; Coull, B.A. Approximate Is Better Than “Exact” for Interval Estimation of Binomial Proportions. Am. Stat. 1998, 52, 119–126. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Rohatgi, A. Webplotdigitizer: Version 4.6. Available online: https://automeris.io/WebPlotDigitizer (accessed on 10 October 2022).
- Sasanami, M.; Kayano, T.; Nishiura, H. The Number of COVID-19 Clusters in Healthcare and Elderly Care Facilities Averted by Vaccination of Healthcare Workers in Japan, February 2021. MBE 2022, 19, 2762–2773. [Google Scholar] [CrossRef]
- Goldstein, E.; Lipsitch, M.; Cevik, M. On the Effect of Age on the Transmission of SARS-CoV-2 in Households, Schools, and the Community. J. Infect. Dis. 2021, 223, 362–369. [Google Scholar] [CrossRef]
- Bi, Q.; Wu, Y.; Mei, S.; Ye, C.; Zou, X.; Zhang, Z.; Liu, X.; Wei, L.; Truelove, S.A.; Zhang, T.; et al. Epidemiology and Transmission of COVID-19 in 391 Cases and 1286 of Their Close Contacts in Shenzhen, China: A Retrospective Cohort Study. Lancet Infect. Dis. 2020, 20, 911–919. [Google Scholar] [CrossRef]
- Jones, B.; Phillips, G.; Kemp, S.; Payne, B.; Hart, B.; Cross, M.; Stokes, K.A. SARS-CoV-2 Transmission during Rugby League Matches: Do Players Become Infected after Participating with SARS-CoV-2 Positive Players? Br. J. Sport. Med. 2021, 55, 807–813. [Google Scholar] [CrossRef]
- National Institute of Infectious Diseases, Japan. Investigation Research on the Infection Risk of COVID-19 in So-Called “Serviced Eating and Drinking Establishments” in the Downtown of Shinjuku-Ward (Interim Report). Available online: https://www.niid.go.jp/niid/ja/diseases/ka/corona-virus/2019-ncov/2488-idsc/iasr-news/10081-491p04.html (accessed on 5 January 2022).
- Echternach, M.; Gantner, S.; Peters, G.; Westphalen, C.; Benthaus, T.; Jakubaß, B.; Kuranova, L.; Döllinger, M.; Kniesburges, S. Impulse Dispersion of Aerosols during Singing and Speaking: A Potential COVID-19 Transmission Pathway. Am. J. Respir. Crit. Care. Med. 2020, 202, 1584–1587. [Google Scholar] [CrossRef]
- Asadi, S.; Wexler, A.S.; Cappa, C.D.; Barreda, S.; Bouvier, N.M.; Ristenpart, W.D. Aerosol Emission and Superemission during Human Speech Increase with Voice Loudness. Sci. Rep. 2019, 9, 2348. [Google Scholar] [CrossRef]
- Shimizu, K.; Tokuda, Y.; Shibuya, K. Japan Should Aim to Eliminate COVID-19. BMJ 2021, 372, n294. [Google Scholar] [CrossRef]
- Sanada, T.; Honda, T.; Yasui, F.; Yamaji, K.; Munakata, T.; Yamamoto, N.; Kurano, M.; Matsumoto, Y.; Kohno, R.; Toyama, S.; et al. Serologic Survey of IgG against SARS-CoV-2 among Hospital Visitors without a History of SARS-CoV-2 Infection in Tokyo, 2020. J. Epidemiol. 2022, 32, 105–111. [Google Scholar] [CrossRef]
- Live and Entertainment Investigation Committee. White Paper on Live and Entertainment 2021. Available online: https://live-entertainment-whitepaper.jp/pdf/summary2021.pdf (accessed on 28 December 2021).
- Japan Karaoke Industrialist Association. White Paper on Karaoke 2021; Japan Karaoke Industrialist Association: Tokyo, Japan, 2021. [Google Scholar]
- Ministry of Economy, Trade, and Industry, Japan. Current Survey of Selected Service Industries, Long-Term Data. Available online: https://www.meti.go.jp/statistics/tyo/tokusabido/result/result_1.html (accessed on 5 January 2022).
- Ministry of Economy, Trade, and Industry, Japan. Indices of Tertiary Industry Activity. Available online: https://www.meti.go.jp/statistics/tyo/sanzi/result-2.html (accessed on 5 January 2022).
- Ministry of Education, Culture, Sports, Science and Technology, Japan. Social Education Survey 2018, Survey on Physical Exercise Facilities. Table 207. Number of Users of Public Physical Exercise Facilities. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00400004&tstat=000001017254&cycle=0&tclass1=000001138486&tclass2=000001138488&tclass3=000001138498&stat_infid=000031924537&tclass4val=0 (accessed on 5 January 2022).
- Ministry of Education, Culture, Sports, Science and Technology, Japan. Social Education Survey 2018, Survey on Physical Exercise Facilities. Table 221. Number of Users of Private Physical Exercise Facilities. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00400004&tstat=000001017254&cycle=0&tclass1=000001138486&tclass2=000001138488&tclass3=000001138499&stat_infid=000031924551&tclass4val=0 (accessed on 5 January 2022).
- Ministry of Health, Labor, and Welfare, Japan. Fact-Finding Survey on Economic Conditions of Environmental Health Industry 2015. Hair-Dressing and Beauty Salons. Available online: https://www.mhlw.go.jp/content/10900000/000501315.pdf (accessed on 4 January 2022).
- Ministry of Health, Labor, and Welfare, Japan. Fact-Finding Survey on Economic Conditions of Environmental Health Industry 2015. Barbershops. Available online: https://www.mhlw.go.jp/content/10900000/000501312.pdf (accessed on 4 January 2022).
- Ministry of Health, Labor, and Welfare, Japan. Survey of Social Welfare Institutions. 2019. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/fukushi/19/dl/tyosa.pdf (accessed on 5 January 2022).
- Senior Housing Association. Registration Status of Residences with Health and Welfare Services for the Elderly (as of the End of August 2021). Available online: https://www.satsuki-jutaku.jp/doc/system_registration_01.pdf (accessed on 10 October 2021).
- Ministry of Health, Labor, and Welfare, Japan. Overview of Survey of Medical Institutions 2019. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/iryosd/19/dl/02sisetu01.pdf (accessed on 28 December 2021).
- Ministry of Health, Labor, and Welfare, Japan. Overview of Patient Survey 2017. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/kanja/17/index.html (accessed on 4 January 2022).
- Ministry of Health, Labor, and Welfare, Japan. Fact-Finding Survey on Economic Conditions of Environmental Health Industry 2013. Restaurant Business (Eating Places). Survey A. Table 13. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/0000169420.xls (accessed on 5 January 2022).
- Ministry of Health, Labor, and Welfare, Japan. Fact-Finding Survey on Economic Conditions of Environmental Health Industry 2013. Coffee Shop Business. Survey A. Table 13. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/0000171258.xls (accessed on 5 January 2022).
- National Police Agency, Japan. White Paper on Police 2020. Chapter 7, Section 1, Item1. Figure 7-1. Available online: https://www.npa.go.jp/hakusyo/r02/honbun/html/w7711000.html (accessed on 4 January 2022).
- Fire and Disaster Management Agency. 2020 White Paper on Fire Service. Available online: https://www.fdma.go.jp/publication/hakusho/r2/56707.html (accessed on 4 January 2022).
- Ministry of Internal Affairs and Communications, Japan. Survey on the Total Number Management of Civil Servants in Local Governments. 2021. Available online: https://www.soumu.go.jp/main_sosiki/jichi_gyousei/c-gyousei/teiin/ (accessed on 4 January 2022).
- Ministry of Economy, Trade, and Industry, Japan. Economy Census 2016, Cross-Industrial Survey on Office. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00200553&tstat=000001095895&cycle=0&tclass1=000001106235&tclass2=000001106275&tclass3=000001114495&stat_infid=000031724997&tclass4val=0 (accessed on 4 January 2022).
- Ministry of Education, Culture, Sports, Science and Technology, Japan. School Basic Survey 2020. Elementary, Secondary Educational Institutions; Specialized Training College; Miscellaneous Schools. School Survey. Summary. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00400001&tstat=000001011528&cycle=0&year=20200&tclass1=000001148386&tclass2=000001148404&tclass3=000001148405&tclass4=000001148406&stat_infid=000032040244&tclass5val=0 (accessed on 4 January 2022).
- Ministry of Education, Culture, Sports, Science and Technology, Japan. School Basic Survey 2020. Higher Education Institutions. School Survey. Summary. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00400001&tstat=000001011528&cycle=0&year=20200&tclass1=000001148386&tclass2=000001148387&tclass3=000001148388&tclass4=000001148389&stat_infid=000032040259&tclass5val=0 (accessed on 4 January 2022).
- National Institute for Educational Policy Research. National Survey on Academic Abilities and Learning Conditions 2017, Questionnaire Survey. Available online: https://www.nier.go.jp/17chousakekkahoukoku/report/data/17qn_05.pdf (accessed on 4 January 2022).
- Benesse Educational Research and Development Institute. Report on 5th Basic Survey of Learning. Chapter 3. Learning Opportunities Outside School. Available online: https://berd.benesse.jp/up_images/research/3_chp3.pdf (accessed on 4 January 2022).
- Japan Karaoke Industrialist Association. White Paper on Karaoke 2020; Japan Karaoke Industrialist Association: Tokyo, Japan, 2020. [Google Scholar]
- Ministry of Education, Culture, Sports, Science and Technology, Japan. Overview of the Result of Survey on Physical Education and Sports Facilities. 2018. Available online: https://www.mext.go.jp/sports/content/20200422-spt_stiiki-1368165.pdf (accessed on 28 December 2021).
- Yano Research Institute. Execution of Survey on Fitness Facilities (2020). Available online: https://www.yano.co.jp/press-release/show/press_id/2657 (accessed on 28 December 2021).
- Ministry of Health, Labor, and Welfare, Japan. Report on Public Health Administration and Services. 2019. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/eisei_houkoku/19/dl/gaikyo.pdf (accessed on 28 December 2021).
- National Police Agency, Japan. White Paper on Police 2021. Chapter 2. Figure 2-54. Available online: https://www.npa.go.jp/hakusyo/r03/honbun/html/x2217000.html (accessed on 5 January 2022).
- National Police Agency, Japan. Current Status of Amusement Businesses and Crackdown on Crimes Related to Amusement Business in 2020. Available online: https://www.npa.go.jp/hakusyo/r03/pdf/09_dai2sho.pdf (accessed on 28 December 2021).
- Ministry of Economy, Trade, and Industry, Japan. Current Survey of Selected Service Industries. 2018. Available online: https://www.meti.go.jp/statistics/tyo/tokusabizi/result-2/h30/pdf/h30outline.pdf (accessed on 4 January 2022).
- National Police Agency, Japan. Overview of National Police Agency. Available online: https://www.npa.go.jp/about/overview/index.html (accessed on 4 January 2022).
- Japan Geographic Data Center. National Database of Prefecture and Local Govenment Office. Available online: https://www.kokudo.or.jp/database/007.html (accessed on 4 January 2022).
- Ministry of Health, Labor, and Welfare, Japan. Summary of Statistical Surveys. D: Working Time. Table 1: Actual Working Hours. Available online: https://www.mhlw.go.jp/toukei/youran/indexyr_d.html (accessed on 4 January 2022).
- Benesse Educational Research and Development Institute. Report on Survey of Learning and Living Conditions of College Students. Chapter 2, Section 2. Living Conditions of College Students. Available online: https://berd.benesse.jp/berd/center/open/report/daigaku_jittai/hon/daigaku_jittai_2_2_1.html (accessed on 4 January 2022).
- Cabinet Office, Government of Japan. Ordinance for Enforcement of Child and Child Care Support Act. Available online: https://elaws.e-gov.go.jp/document?lawid=426M60000002044 (accessed on 4 January 2022).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Establishment Type | Definition of an Event | Type of Users | [Users] | [Days] | [Facilities] | [Hours] |
|---|---|---|---|---|---|---|---|
| Recreational facilities | Theater | Attend a performance | Audiences | 341.2 | 46,986 | 3.0 | |
| Eating and drinking establishments with Karaoke facility | Visit stores/facilities | Users | 110.4 | 395.0 | 25,108 | 2.6 | |
| Sports facility | 30.8 | 268.0 | 71,271 | 1.5 | |||
| Beauty salon/Barber | 6.4 | 327.0 | 371,688 | 1.0 | |||
| Welfare facility | Welfare facility for persons with disabilities | Stay for a night | Residents, Users | 27.5 | 395.0 | 5636 | 16.0 |
| Elderly care facility | 32.2 | 395.0 | 28,352 | 16.0 | |||
| Child welfare facility | 66.8 | 268.0 | 44,616 | 11.0 | |||
| Health institute | Hospital | Stay for a night | Inpatients | 165.8 | 395.0 | 8300 | 16.0 |
| Clinic | Visit a doctor | Outpatients | 41.1 | 323.0 | 102,616 | 0.5 | |
| Dental clinic | 19.7 | 326.0 | 68,500 | 1.0 | |||
| Eating and drinking establishment | Restaurant | Visit stores | Users | 127.4 | 323.0 | 1,279,784 | 1.0 |
| Alcohol serving eating and drinking establishment | 42.9 | 323.0 | 264,359 | 2.0 | |||
| Serviced entertaining bars and escort clubs | 57.0 | 323.0 | 61,857 | 2.0 | |||
| Educational institution | University | Attend for a day | Students | 3667.4 | 187.0 | 795 | 5.0 |
| High school | 634.4 | 237.0 | 4874 | 8.0 | |||
| Middle school | 316.6 | 237.0 | 10,142 | 8.0 | |||
| Elementary school | 322.7 | 237.0 | 19,525 | 7.0 | |||
| Kindergarten | 111.2 | 237.0 | 9698 | 5.0 | |||
| Cram school | 122.8 | 124.7 | 46,734 | 1.5 | |||
| Public office and enterprises | Police station | Work for a day | Staffs | 246.2 | 268.0 | 1204 | 8.0 |
| Local government office | 474.1 | 268.0 | 1971 | 8.0 | |||
| Fire station | 68.2 | 268.0 | 2445 | 8.0 | |||
| Workplace | 10.6 | 268.0 | 5,340,783 | 7.8 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ueda, M.; Hayashi, K.; Nishiura, H. Identifying High-Risk Events for COVID-19 Transmission: Estimating the Risk of Clustering Using Nationwide Data. Viruses 2023, 15, 456. https://doi.org/10.3390/v15020456
Ueda M, Hayashi K, Nishiura H. Identifying High-Risk Events for COVID-19 Transmission: Estimating the Risk of Clustering Using Nationwide Data. Viruses. 2023; 15(2):456. https://doi.org/10.3390/v15020456
Chicago/Turabian StyleUeda, Minami, Katsuma Hayashi, and Hiroshi Nishiura. 2023. "Identifying High-Risk Events for COVID-19 Transmission: Estimating the Risk of Clustering Using Nationwide Data" Viruses 15, no. 2: 456. https://doi.org/10.3390/v15020456
APA StyleUeda, M., Hayashi, K., & Nishiura, H. (2023). Identifying High-Risk Events for COVID-19 Transmission: Estimating the Risk of Clustering Using Nationwide Data. Viruses, 15(2), 456. https://doi.org/10.3390/v15020456