
Laboratory Findings in Patients with Probable Dengue Diagnosis from an Endemic Area in Colombia in 2018



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Human Sample Collection, Blood Testing and Dengue Diagnosis
2.3. Statistical Analysis
3. Results
3.1. Children under 15 Represent the Higher Number of Dengue Positive Cases by RDT
3.2. Days of Symptoms Do Not Have a Significant Effect on RDT Results
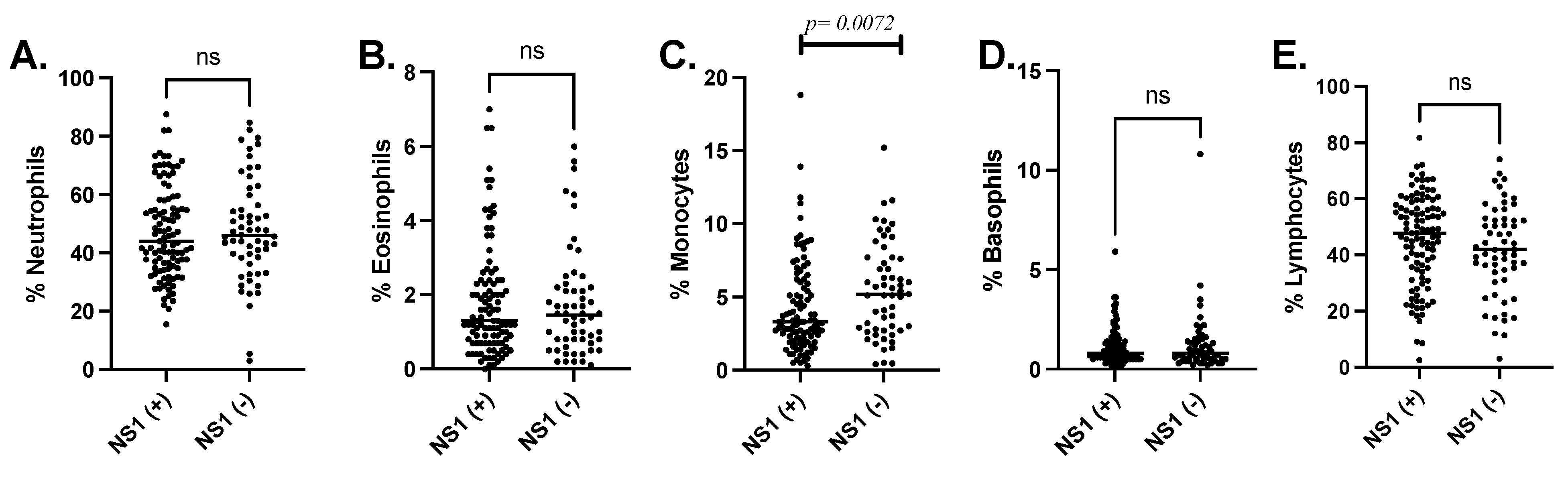
3.3. NS1-Ag Positive Patients Present Lower Leukocyte Count Represented with a Significant Decrease in Monocytes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- WHO. Dengue and Severe Dengue Fact Sheet; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Tapia-Conyer, R.; Betancourt-Cravioto, M.; Méndez-Galván, J. Dengue: An escalating public health problem in Latin America. Paediatr. Int. Child Health 2012, 32, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Guzman, M.G.; Halstead, S.B.; Artsob, H.; Buchy, P.; Farrar, J.; Gubler, D.J.; Hunsperger, E.; Kroeger, A.; Margolis, H.S.; Martínez, E.; et al. Dengue: A continuing global threat. Nat. Rev. Genet. 2010, 8, S7–S16. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.J.; Chan, K.S.; Chang, J.-S.; Chang, K.; Lin, C.C.; Huang, J.H.; Lin, W.R.; Chen, T.C.; Hsieh, H.C.; Lin, S.H.; et al. Effect of serotypes on clinical manifestations of dengue fever in adults. J. Microbiol. Immunol. Infect. 2009, 42, 471–478. [Google Scholar]
- Suppiah, J.; Ching, S.M.; Amin-Nordin, S.A.; Mat-Nor, L.-A.; Ahmad-Najimudin, N.-A.; Low, G.K.K.; Abdul-Wahid, M.-Z.; Thayan, R.; Chee, H.-Y. Clinical manifestations of dengue in relation to dengue serotype and genotype in Malaysia: A retrospective observational study. PLOS Negl. Trop. Dis. 2018, 12, e0006817. [Google Scholar] [CrossRef]
- Ten Bosch, Q.A.T.; Clapham, H.E.; Lambrechts, L.; Duong, V.; Buchy, P.; Althouse, B.M.; Lloyd, A.L.; Waller, L.A.; Morrison, A.C.; Kitron, U.; et al. Contributions from the silent majority dominate dengue virus transmission. PLOS Pathog. 2018, 14, e1006965. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.; Sammon, M.; Garg, M. Dengue, Zika and Chikungunya: Emerging Arboviruses in the New World. West. J. Emerg. Med. 2016, 17, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Khan, W.; Zakai, H.A.; Khan, K.; Kausar, S.; Aqeel, S. Discriminating Clinical and Biological Features in Malaria and Dengue Patients. J. Arthropod-Borne Dis. 2018, 12, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Chong, H.Y.; Leow, C.Y.; Abdul Majeed, A.B.; Leow, C.H.A. Flavivirus infection—A review of immunopathogenesis, immunological response, and immunodiagnosis. Virus Res. 2019, 274, 197770. [Google Scholar] [CrossRef]
- Leach, C.B.; Hoeting, J.A.; Pepin, K.M.; Eiras, A.E.; Hooten, M.B.; Webb, C.T. Linking mosquito surveillance to dengue fever through Bayesian mechanistic modeling. PLOS Neglected Trop. Dis. 2020, 14, e0008868. [Google Scholar] [CrossRef]
- Quintero, J.; Ronderos Pulido, N.R.; Logan, J.; Ant, T.; Bruce, J.; Carrasquilla, G. Effectiveness of an intervention for Aedes aegypti control scaled-up under an inter-sectoral approach in a Colombian city hyper-endemic for dengue virus. PLoS ONE 2020, 15, e0230486. [Google Scholar] [CrossRef]
- Gómez-Palacio, A.; Suaza-Vasco, J.; Castaño, S.; Triana, O.; Uribe, S. Aedes albopictus (Skuse, 1894) infected with the American-Asian genotype of dengue type 2 virus in Medellín suggests its possible role as vector of dengue fever in Colombia. Biomédica 2017, 37, 135–142. [Google Scholar] [CrossRef]
- Lim, J.K.; Carabali, M.; Camacho, E.; Velez, D.C.; Trujillo, A.; Egurrola, J.; Lee, K.-S.; Velez, I.D.; Osorio, J.E. Epidemiology and genetic diversity of circulating dengue viruses in Medellin, Colombia: A fever surveillance study. BMC Infect. Dis. 2020, 20, 466. [Google Scholar] [CrossRef]
- Pan American Health Organization. Epidemiological Update: Dengue 7 February 2020. Available online: https://www.paho.org/en/documents/epidemiological-update-dengue-7-february-2020.
- Raafat, N.; Blacksell, S.D.; Maude, R.J. A review of dengue diagnostics and implications for surveillance and control. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization. Reported Cases of Dengue Fever in the Americas, by Country or Territory. Available online: https://www.paho.org/data/index.php/en/mnu-topics/indicadores-dengue-en/dengue-nacional-en/252-dengue-pais-ano-en.html (accessed on 14 December 2020).
- Abbas, M.; Aloudat, T.; Bartolomei, J.; Carballo, M.; Durieux-Paillard, S.; Gabus, L.; Jablonka, A.; Jackson, Y.; Kaojaroen, K.; Koch, D.; et al. Migrant and refugee populations: A public health and policy perspective on a continuing global crisis. Antimicrob. Resist. Infect. Control. 2018, 7, 113. [Google Scholar] [CrossRef] [PubMed]
- Napoli, C.; Salcuni, P.; Pompa, M.G.; Declich, S.; Rizzo, C. Estimated Imported Infections of Chikungunya and Dengue in Italy, 2008 to 2011. J. Travel Med. 2012, 19, 294–297. [Google Scholar] [CrossRef]
- Beatty, M.E.; Stone, A.; Fitzsimons, D.W.; Hanna, J.N.; Lam, S.K.; Vong, S.; Guzman, M.G.; Mendez-Galvan, J.F.; Halstead, S.B.; Letson, G.W.; et al. Best Practices in Dengue Surveillance: A Report from the Asia-Pacific and Americas Dengue Prevention Boards. PLOS Neglected Trop. Dis. 2010, 4, e890. [Google Scholar] [CrossRef] [PubMed]
- Hunsperger, E.A.; Sharp, T.M.; Lalita, P.; Tikomaidraubuta, K.; Cardoso, Y.R.; Naivalu, T.; Khan, A.S.; Marfel, M.; Hancock, W.T.; Tomashek, K.M.; et al. Use of a Rapid Test for Diagnosis of Dengue during Suspected Dengue Outbreaks in Resource-Limited Regions. J. Clin. Microbiol. 2016, 54, 2090–2095. [Google Scholar] [CrossRef] [PubMed]
- Sa-Ngamuang, C.; Haddawy, P.; Luvira, V.; Piyaphanee, W.; Iamsirithaworn, S.; Lawpoolsri, S. Accuracy of dengue clinical diagnosis with and without NS1 antigen rapid test: Comparison between human and Bayesian network model decision. PLOS Neglected Trop. Dis. 2018, 12, e0006573. [Google Scholar] [CrossRef] [PubMed]
- Andreata-Santos, R.; Pereira, S.S.; Pereira, L.R.; Félix, A.C.; Romano, C.M.; Ferreira, L.C.D.S. Specificity of NS1-based immunochromatographic tests for dengue virus with regard to the Zika virus protein. Int. J. Infect. Dis. 2020, 95, 276–278. [Google Scholar] [CrossRef] [PubMed]
- Mora-Cárdenas, E.; Aloise, C.; Faoro, V.; Knap Gašper, N.K.; Korva, M.; Caracciolo, I.; D’Agaro, P.; Avšič-Županc, T.; Marcello, A. Comparative specificity and sensitivity of NS1-based serological assays for the detection of flavivirus immune response. PLOS Neglected Trop. Dis. 2020, 14, e0008039. [Google Scholar] [CrossRef] [PubMed]
- Alcon, S.; Talarmin, A.; Debruyne, M.; Falconar, A.; Deubel, V.; Flamand, M. Enzyme-Linked Immunosorbent Assay Specific to Dengue Virus Type 1 Nonstructural Protein NS1 Reveals Circulation of the Antigen in the Blood during the Acute Phase of Disease in Patients Experiencing Primary or Secondary Infections. J. Clin. Microbiol. 2002, 40, 376–381. [Google Scholar] [CrossRef]
- Young, P.R.; Hilditch, P.A.; Bletchly, C.; Halloran, W. An Antigen Capture Enzyme-Linked Immunosorbent Assay Reveals High Levels of the Dengue Virus Protein NS1 in the Sera of Infected Patients. J. Clin. Microbiol. 2000, 38, 1053–1057. [Google Scholar] [CrossRef] [PubMed]
- Redoni, M.; Yacoub, S.; Rivino, L.; Giacobbe, D.R.; Luzzati, R.; Di Bella, S. Dengue: Status of current and under-development vaccines. Rev. Med Virol. 2020, 30, e2101. [Google Scholar] [CrossRef] [PubMed]
- Shukla, R.; Ramasamy, V.; Shanmugam, R.K.; Ahuja, R.; Khanna, N. Antibody-Dependent Enhancement: A Challenge for Developing a Safe Dengue Vaccine. Front. Cell. Infect. Microbiol. 2020, 10, 572681. [Google Scholar] [CrossRef]
- Luo, R.; Fongwen, N.; Kelly-Cirino, C.; Harris, E.; Wilder-Smith, A.; Peeling, R.W. Rapid diagnostic tests for determining dengue serostatus: A systematic review and key informant interviews. Clin. Microbiol. Infect. 2019, 25, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Simmons, C.P.; Farrar, J.J.; Nguyen, vV.; Wills, B. Dengue. N. Engl. J. Med. 2012, 366, 1423–1432. [Google Scholar] [CrossRef]
- Londono-Renteria, B.; Cardenas, J.C.; Giovanni, J.E.; Cardenas, L.; Villamizar, P.; Rolon, J.; Chisenhall, D.M.; Carvajal, D.J.; Pérez, O.G.; Wesson, D.M.; et al. Concentración de los anticuerpos en contra de proteínas de las glándulas salivares de Aedes aegypti e historia de la exposición al virus del dengue en residentes de una zona endémica colombiana. Biomédica 2015, 35, 572–581. [Google Scholar] [CrossRef]
- Jiménez-Silva, C.L.; Carreño, M.F.; Ortiz-Baez, A.S.; Rey, L.A.; Villabona-Arenas, C.J.; Ocazionez, R.E. Evolutionary history and spatio-temporal dynamics of dengue virus serotypes in an endemic region of Colombia. PLoS ONE 2018, 13, e0203090. [Google Scholar] [CrossRef]
- Caicedo-Borrero, D.M.; Tovar, J.R.; Méndez, A.; Parra, B.; Bonelo, A.; Celis, J.; Villegas, L.; Collazos, C.; Osorio, L. Development and Performance of Dengue Diagnostic Clinical Algorithms in Colombia. Am. J. Trop. Med. Hyg. 2020, 102, 1226–1236. [Google Scholar] [CrossRef]
- Lin, S.F.; Liu, H.W.; Chang, C.S.; Yen, J.-H.; Chen, T.P. Hematological aspects of dengue fever. Kaohsiung J. Med Sci. 1989, 5, 12–16. [Google Scholar]
- Durbin, A.P.; Vargas, M.J.; Wanionek, K.; Hammond, S.N.; Gordon, A.; Rocha, C.; Balmaseda, A.; Harris, E. Phenotyping of peripheral blood mononuclear cells during acute dengue illness demonstrates infection and increased activation of monocytes in severe cases compared to classic dengue fever. Virology. 2008, 376, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Castillo, J.A.; Naranjo, J.S.; Rojas, M.; Castaño, D.; Velilla, P.A. Role of Monocytes in the Pathogenesis of Dengue. Arch. Immunol. Et. Ther. Exp. 2019, 67, 27–40. [Google Scholar] [CrossRef]
- Torrentes-Carvalho, A.; Azeredo, E.L.; Reis, S.R.; Miranda, A.S.; Gandini, M.; Barbosa, L.S.; Kubelka, C.F. Dengue-2 infection and the induction of apoptosis in human primary monocytes. Memórias Inst. Oswaldo Cruz 2009, 104, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Castillo, J.A.; Urcuqui-Inchima, S. Mechanisms of monocyte cell death triggered by dengue virus infection. Apoptosis 2018, 23, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.-J.; Chang, J.-S.; Chang, K.; Chen, P.-C.; Liu, L.-T.; Ho, T.-C.; Tan, S.S.; Chien, Y.-W.; Lo, Y.-C.; Perng, G.C. Transient Monocytosis Subjugates Low Platelet Count in Adult Dengue Patients. Biomed. Hub 2017, 2, 1–16. [Google Scholar] [CrossRef]
- Kalayanarooj, S.; Vaughn, D.W.; Nimmannitya, S.; Green, S.; Suntayakorn, S.; Kunentrasai, N.; Viramitrachai, W.; Ratanachu-Eke, S.; Kiatpolpoj, S.; Innis, B.L.; et al. Early Clinical and Laboratory Indicators of Acute Dengue Illness. J. Infect. Dis. 1997, 176, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Chaloemwong, J.; Tantiworawit, A.; Rattanathammethee, T.; Hantrakool, S.; Chai-Adisaksopha, C.; Rattarittamrong, E.; Norasetthada, L. Useful clinical features and hematological parameters for the diagnosis of dengue infection in patients with acute febrile illness: A retrospective study. BMC Hematol. 2018, 18, 20. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.A.; U, R.R.; Gosavi, S.; Menon, S. Dengue Fever: Prognostic Insights From a Complete Blood Count. Cureus 2020, 12, e11594. [Google Scholar] [CrossRef]
- Thomas, L.; Césaire, R.; Martial, J.; Najioullah, F.; Verlaeten, O.; Kaidomar, J.S.; Cabié, A.; Brichler, S.; Moravie, V. Relationship between Nonstructural Protein 1 Detection and Plasma Virus Load in Dengue Patients. Am. J. Trop. Med. Hyg. 2010, 83, 696–699. [Google Scholar] [CrossRef]
- Garg, A.; Garg, J.; Singh, D.V.; Dhole, T.N. Can rapid dengue diagnostic kits be trusted? A comparative study of commercially available rapid kits for serodiagnosis of dengue fever. J. Lab. Physicians 2019, 11, 63–67. [Google Scholar] [CrossRef]
- Tang, K.F.; Ooi, E.E. Diagnosis of dengue: An update. Expert Rev. Anti Infective Ther. 2012, 10, 895–907. [Google Scholar] [CrossRef]
- Wright, W.F.; Pritt, B.S. Update: The diagnosis and management of dengue virus infection in North America. Diagn. Microbiol. Infect. Dis. 2012, 73, 215–220. [Google Scholar] [CrossRef]
- Villar, L.A.; Rojas, D.P.; Besada-Lombana, S.; Sarti, E. Epidemiological Trends of Dengue Disease in Colombia (2000–2011): A Systematic Review. PLOS Negl. Trop. Dis. 2015, 9, e0003499. [Google Scholar] [CrossRef] [PubMed]
- Anker, M.; Arima, Y. Male-female differences in the number of reported incident dengue fever cases in six Asian countries. West. Pac. Surveill. Response J. 2011, 2, e17–e23. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, J.E.; Eliason, D.A.; Moore, M.; Sather, G.E.; Schonberger, L.B.; Cabrera-Coello, L.; Fernandez De Castro, J.F. Epidemiologic investigations of dengue infection in Mexico, 1980. Am. J. Epidemiol. 1983, 117, 335–343. [Google Scholar] [CrossRef]
- Trravassos Da Rosa, A.P.T.; Vasconcelos, P.F.; Trravassos Da Rosa, E.S.T.; Rodrigues, S.G.; Mondet, B.; Cruz, A.C.; Sousa, M.R.; Trravassos Da Rosa, J.F.T. Dengue Epidemic in Belem, Para, Brazil, 1996–1997. Emerg. Infect. Dis. 2000, 6, 298–301. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | N | % | NS1-Ag Positive | NS1-Ag Negative | Mann-Whitney Test | ||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | Median | n | % | Median | p-Value | |||
| Age (in years old) | 161 | 100% | 103 | 64% | 8.8 ± 10.5 | 58 | 36% | 20.7 ± 20.5 | <0.0001 * |
| Female Age | 92 | 57% | 55 | 60% | 9.9 ± 13.5 | 37 | 40% | 22.4 ± 22.4 | 0.0016 * |
| Male Age | 69 | 43% | 48 | 70% | 7.52 ± 5.0 | 21 | 30% | 17.7 ± 17.0 | 0.0041 * |
| Children ≤ 15 years | 126 | 78% | 93 | 74% | 6.2 ± 3.7 | 33 | 26% | 6.9 ± 3.7 | 0.2972 |
| Adults ≥ 15 years | 35 | 22% | 10 | 29% | 32.2 ± 20.8 | 25 | 71% | 38.8 ± 19.6 | 0.3158 |
| Days of symptoms | 161 | 100% | 103 | 64% | 4.9 ± 1.2 | 58 | 36% | 4.7 ± 1.5 | 0.2458 |
| NS1-Ag | PCR | Total | |
|---|---|---|---|
| Positive | Negative | ||
| Positive | 67 | 24 | 91 |
| Negative | 11 | 9 | 20 |
| Total | 78 | 33 | 111 |
| ≤5 Days | PCR | >6 Days | PCR | ||||
|---|---|---|---|---|---|---|---|
| NS1-Ag | Positive | Negative | Total | NS1-Ag | Positive | Negative | Total |
| Positive | 54 | 21 | 75 | Positive | 13 | 3 | 18 |
| Negative | 8 | 8 | 16 | Negative | 3 | 1 | 4 |
| Total | 62 | 29 | 91 | Total | 18 | 4 | 22 |
| Days of Symptoms | NS1-Ag (+) | NS1-Ag (−) | n | RT-PCR (+) | RT-PCR (−) | n |
|---|---|---|---|---|---|---|
| 3 | 16 | 7 | 23 | 13 | 6 | 19 |
| 4 | 31 | 14 | 45 | 24 | 8 | 32 |
| 5 | 36 | 22 | 58 | 25 | 15 | 40 |
| 6 | 11 | 10 | 21 | 10 | 3 | 13 |
| 7 | 6 | 3 | 9 | 6 | 1 | 7 |
| 8 | 1 | 1 | 2 | 0 | 0 | 0 |
| 9 | 1 | 1 | 2 | 1 | 0 | 1 |
| 15 | 1 | 0 | 1 | 1 | 0 | 1 |
| Total | 103 | 58 | 161 | 80 | 33 | 113 |
| Parameter | NS1-Ag Positive (n = 103) | NS1-Ag Negative (n = 58) | Mann-Whitney Test |
|---|---|---|---|
| Median (IQR) | Median (IQR) | p Value | |
| Hemoglobin (g/dL) | 12.9 (1.4) | 13 (1.3) | 0.6147 |
| Hematocrit | 39.0 (4.1) | 39.9 (3.9) | 0.3513 |
| Platelet count (×109/L) | 113 (30.6) | 108 (28.3) | 0.4302 |
| RBC (×1012/L) | 4.5 (0.4) | 4.59 (0.5) | 0.2091 |
| WBC (×109/L) | 3.26 (2.0) | 4.52 (2.6) | 0.0008 * |
| MCH (pg) | 28.8 (2.7) | 28.3 (2.7) | 0.4452 |
| MCV (ft) | 85.8 (9.4) | 84.8 (13.0) | 0.4109 |
| RDW CV% | 12.8 (0.9) | 12.8 (1.0) | 0.1374 |
| RDW-SD (fL) | 46.4 (3.2) | 45.8 (3.4) | 0.7207 |
| Parameters | NS1-Ag Positive (n = 103) | NS1-Ag Negative (n = 58) | ||
|---|---|---|---|---|
| Leukopenia (≤4.0 cells × 103/μL) | 67 | 65% | 23 | 40% |
| Leukocytes (4.1–10 cells × 103/μL) | 35 | 34% | 32 | 55% |
| Leukocytosis (>10 cells × 103/μL) | 1 | 1% | 3 | 5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardenas, J.C.; Giraldo-Parra, S.Y.; Gonzalez, M.U.; Gutierrez-Silva, L.Y.; Jaimes-Villamizar, L.; Roa-Parra, A.L.; Carvajal, D.J.; Valdivia, H.O.; Sanchez, J.F.; Colpitts, T.M.; et al. Laboratory Findings in Patients with Probable Dengue Diagnosis from an Endemic Area in Colombia in 2018. Viruses 2021, 13, 1401. https://doi.org/10.3390/v13071401
Cardenas JC, Giraldo-Parra SY, Gonzalez MU, Gutierrez-Silva LY, Jaimes-Villamizar L, Roa-Parra AL, Carvajal DJ, Valdivia HO, Sanchez JF, Colpitts TM, et al. Laboratory Findings in Patients with Probable Dengue Diagnosis from an Endemic Area in Colombia in 2018. Viruses. 2021; 13(7):1401. https://doi.org/10.3390/v13071401
Chicago/Turabian StyleCardenas, Jenny C., Sandra Y. Giraldo-Parra, Maria U. Gonzalez, Lady Y. Gutierrez-Silva, Lucy Jaimes-Villamizar, Alba L. Roa-Parra, Daisy J. Carvajal, Hugo O. Valdivia, Juan F. Sanchez, Tonya M. Colpitts, and et al. 2021. "Laboratory Findings in Patients with Probable Dengue Diagnosis from an Endemic Area in Colombia in 2018" Viruses 13, no. 7: 1401. https://doi.org/10.3390/v13071401
APA StyleCardenas, J. C., Giraldo-Parra, S. Y., Gonzalez, M. U., Gutierrez-Silva, L. Y., Jaimes-Villamizar, L., Roa-Parra, A. L., Carvajal, D. J., Valdivia, H. O., Sanchez, J. F., Colpitts, T. M., & Londono-Renteria, B. (2021). Laboratory Findings in Patients with Probable Dengue Diagnosis from an Endemic Area in Colombia in 2018. Viruses, 13(7), 1401. https://doi.org/10.3390/v13071401