
COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention



Abstract
1. Introduction
2. Evolution of the Coronavirus
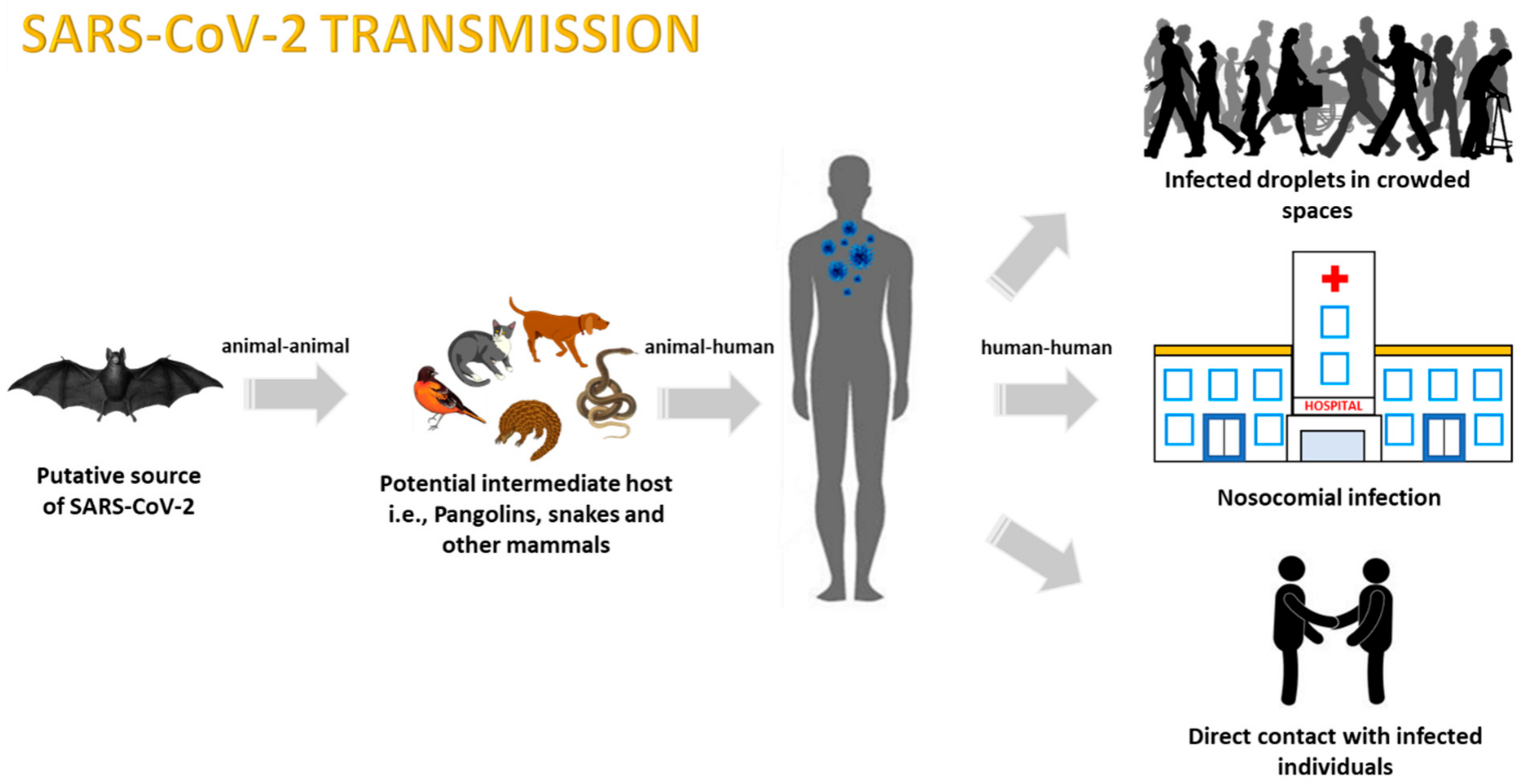
3. COVID-19 Transmission
3.1. Animal-to-Human Transmission
3.2. Human-to-Human Transmission
3.2.1. Transmission via Aerosols
3.2.2. Nosocomial-Related Infections
3.2.3. Maternal Transmission
4. COVID-19 Modes of Detection
4.1. Reverse Transcription Polymerase Chain Reaction (RT-PCR)-Based Testing
4.2. Radiological Testing
4.3. Serological and Immunological Assays
4.3.1. COVID-19 Testing Kits
4.3.2. CRISPR-Based Detection Techniques
5. COVID-19 Control Measures
5.1. Antiviral Drug Therapeutics
5.1.1. Repositioning Antiviral Drugs as Therapy for SARS-CoV-2
5.1.2. Clinical Trials for Drugs against COVID-19
5.1.3. Repositioning Hydroxychloroquine as a Drug Therapy for SARS-CoV-2
5.1.4. Host–Virus Interaction Studies to Identify Antiviral Molecules against SARS-CoV-2
5.2. Immunotherapy
5.3. Development of Vaccines
5.3.1. Clinical Trials for Vaccines against COVID-19
5.3.2. Peptide Vaccine
5.3.3. Challenges in Vaccine Development
5.4. Nosocomial Infection-Related Control Measures
5.5. Population Outbreak Predictions Using Computational Tools
6. Preventative Strategies
6.1. Daily Safety Guidelines
6.2. Preventative Measures Adoption According to Age Group
6.3. Travel and Airport Screenings
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- De Wit, E.; Van Doremalen, N.; Falzarano, D.; Munster, V.J. SARS and MERS: Recent insights into emerging coronaviruses. Nat. Rev. Microbiol. 2016, 14, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Gong, S.R.; Bao, L.L. The battle against SARS and MERS coronaviruses: Reservoirs and Animal Models. Anim. Model. Exp. Med. 2018, 1, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Fehr, A.R.; Perlman, S. Coronaviruses: An overview of their replication and pathogenesis. Methods Mol. Biol. 2015, 1282, 1–23. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Teleman, M.D.; Heng, B.H.; Earnest, A.; Ling, A.E.; Leo, Y.S. Asymptomatic SARS coronavirus infection among healthcare workers, Singapore. Emerg. Infect. Dis. 2005, 11, 1142–1145. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Jartti, L.; Langen, H.; Söderlund-Venermo, M.; Vuorinen, T.; Ruuskanen, O.; Jartti, T. New respiratory viruses and the elderly. Open Respir. Med. J. 2011, 5, 61–69. [Google Scholar] [CrossRef] [PubMed]
- The New York Times. Coronavirus Updates: The Illness Now Has a Name, COVID-19. Available online: https://www.nytimes.com/2020/02/11/world/asia/coronavirus-china.html (accessed on 17 May 2020).
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020. [Google Scholar] [CrossRef]
- World Health Organization. International Health Regulations Emergency Committee on Novel Coronavirus in China. Available online: https://www.who.int/news-room/events/detail/2020/01/30/default-calendar/international-health-regulations-emergency-committee-on-novel-coronavirus-in-china (accessed on 17 May 2020).
- Business Insider. The Coronavirus Has Pandemic ‘Potential’ as it Spreads in South Korea, Italy, and Iran, According to WHO. Available online: https://www.businessinsider.com/covid-19-coronavirus-has-pandemic-potential-says-who-2020-2?IR=T (accessed on 7 April 2020).
- NewScientist. The WHO Still isn’t Describing Covid-19 as a Pandemic. Available online: https://www.newscientist.com/article/2235095-the-who-still-isnt-describing-covid-19-as-a-pandemic/#ixzz6F2fq8ncn (accessed on 17 May 2020).
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19–11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 17 May 2020).
- Pyrc, K.; Berkhout, B.; Van der Hoek, L. The novel human coronaviruses NL63 and HKU1. J. Virol. 2007, 81, 3051–3057. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, S.G.; Sawicki, D.L.; Siddell, S.G. A contemporary view of coronavirus transcription. J. Virol. 2007, 81, 20–29. [Google Scholar] [CrossRef]
- Smith, E.C.; Denison, M.R. Coronaviruses as DNA wannabes: A new model for the regulation of RNA virus replication fidelity. PLoS Pathog. 2013, 9. [Google Scholar] [CrossRef]
- Wang, L.; Byrum, B.; Zhang, Y. Detection and genetic characterization of deltacoronavirus in pigs, Ohio, USA, 2014. Emerg. Infect. Dis. 2014, 20, 1227–1230. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Zhang, D. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Wu, Q.; Zhang, Z. Pangolin Homology Associated with 2019-nCoV. bioRxiv 2020. Available online: https://www.biorxiv.org/content/10.1101/2020.02.19.950253v1 (accessed on 17 May 2020).
- Weiss, S.R.; Navas-Martin, S. Coronavirus pathogenesis and the emerging pathogen severe acute respiratory syndrome coronavirus. Microbiol. Mol. Biol. Rev. 2005, 69, 635–664. [Google Scholar] [CrossRef]
- Van der Hoek, L.; Pyrc, K.; Jebbink, M.F.; Vermeulen-Oost, W.; Berkhout, R.J.M.; Wolthers, K.C.; Wertheim-van Dillen, P.; Kaandorp, J.; Spaargaren, J.; Berkhout, B. Identification of a new human coronavirus. Nat. Med. 2004, 10, 368–373. [Google Scholar] [CrossRef]
- Azhar, E.I.; El-Kafrawy, S.A.; Farraj, S.A.; Hassan, A.M.; Al-Saeed, M.S.; Hashem, A.M.; Hashem, A.; Madani, T. Evidence for camel-to-human transmission of MERS coronavirus. N. Engl. J. Med. 2014, 370, 2499–2505. [Google Scholar] [CrossRef]
- Sharma, A.; Lal, S.K. Zika virus: Transmission, detection, control, and prevention. Front. Microbiol. 2017. [Google Scholar] [CrossRef]
- Sui, J.; Aird, D.R.; Tamin, A.; Murakami, A.; Yan, M.; Yammanuru, A.; Jing, H.; Kan, B.; Liu, X.; Zhu, Q.; et al. Broadening of neutralization activity to directly block a dominant antibody-driven SARS-coronavirus evolution pathway. PLoS Pathog. 2008, 4. [Google Scholar] [CrossRef]
- Kahn, J.S.; McIntosh, K. History and recent advances in coronavirus discovery. Pediatr. Infect. Dis. J. 2005, 24, S223–S227. [Google Scholar] [CrossRef]
- Zeng, Z.Q.; Chen, D.H.; Tan, W.P.; Qiu, S.Y.; Xu, D.; Liang, H.X.; Che, M.; Li, X.; Lin, Z.; Liu, W.; et al. Epidemiology and clinical characteristics of human coronaviruses OC43, 229E, NL63, and HKU1: A study of hospitalized children with acute respiratory tract infection in Guangzhou, China. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 363–369. [Google Scholar] [CrossRef]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Bo, Y.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020. [Google Scholar] [CrossRef]
- To, K.K.; Hung, I.F.; Chan, J.F.; Yuen, K.Y. From SARS coronavirus to novel animal and human coronaviruses. J. Thorac. Dis. 2013, 3, S103–S108. [Google Scholar] [CrossRef]
- Gralinski, L.E.; Menachery, V.D. Return of the coronavirus: 2019-nCoV. Viruses 2020, 12, 135. [Google Scholar] [CrossRef] [PubMed]
- Chowell, G.; Blumberg, S.; Simonsen, L.; Miller, M.A.; Viboud, C. Synthesizing data and models for the spread of MERS-CoV, 2013: Key role of index cases and hospital transmission. Epidemics 2014, 9, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Al Awaidy, S.T.; Khamis, F. Middle East Respiratory Syndrome Coronavirus (MERS-CoV) in Oman: Current Situation and Going Forward. Oman Med. J. 2019, 34, 181–183. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. MERS Global Summary and Assessment of Risk. Available online: https://www.who.int/emergencies/mers-cov/en/ (accessed on 17 May 2020).
- Lam, T.T.Y.; Shum, M.H.H.; Zhu, H.C.; Tong, Y.G.; Ni, X.B.; Liao, Y.S.; Li, W.; Jiang, B.; Wei, W.; Yuan, T.; et al. Identification of 2019-nCoV related coronaviruses in Malayan pangolins in southern China. bioRxiv 2020. [Google Scholar] [CrossRef]
- Soucheray, S. Scientists Warn nCoV More Infectious than SARS, but Experts Have Doubts. Available online: http://www.cidrap.umn.edu/news-perspective/2020/01/scientists-warn-ncov-more-infectious-sars-experts-have-doubts (accessed on 17 May 2020).
- Worldometer. Wuhan Coronavirus Outbreak. Available online: https://www.worldometers.info/coronavirus/ (accessed on 8 October 2020).
- Elena, S.F.; Sanjuán, R. Adaptive value of high mutation rates of RNA viruses: Separating causes from consequences. J. Virol. 2005, 79, 11555–11558. [Google Scholar] [CrossRef]
- Sharma, A.; Lal, S.K. Is tetherin a true antiviral: The influenza a virus controversy. Rev. Med. Virol. 2019, 29. [Google Scholar] [CrossRef]
- Duffy, S. Why are RNA virus mutation rates so damn high? PLoS Biol. 2018, 16, 8. [Google Scholar] [CrossRef]
- Perlman, S.; Netland, J. Coronaviruses post-SARS: Update on replication and pathogenesis. Nat. Rev. Microbiol. 2009, 7, 439–450. [Google Scholar] [CrossRef]
- Anand, K.B.; Karade, S.; Sen, S.; Gupta, R.M. SARS-CoV-2: Camazotz’s Curse. Med. J. Armed Forces India 2020, 76. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Peng, W.; Zhu, Y.; Lu, S.; Zhou, M.; Lin, W.; Wu, W.; Huang, S.; Jiang, L.; Luo, X.; et al. Recent Progress in understanding 2019 novel coronavirus associated with human respiratory disease: Detection, mechanism and treatment. Int. J. Antimicrob. Agentsp. 2020. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Wu, C.; Li, X.; Song, Y.; Yao, X.; Wu, X.; Duan, Y.; Zhang, H.; Wang, Y.; Qian, Z.; et al. On the origin and continuing evolution of SARS-CoV-2. Natl. Sci. Rev. 2020. [Google Scholar] [CrossRef]
- Li, F. Structure, function, and evolution of coronavirus spike proteins. Annu. Rev. Virol. 2016, 3, 237–261. [Google Scholar] [CrossRef]
- Qing, E.; Gallagher, T. SARS coronavirus redux. Trends Immunol. 2020. [Google Scholar] [CrossRef] [PubMed]
- De Haan, C.A.; Te Lintelo, E.; Li, Z.; Raaben, M.; Wurdinger, T.; Bosch, B.J.; Rottier, P.J. Cooperative involvement of the S1 and S2 subunits of the murine coronavirus spike protein in receptor binding and extended host range. J. Virol. 2006, 80, 10909–10918. [Google Scholar] [CrossRef]
- Saputri, D.S.; Li, S.; Van Eerden, F.J.; Rozewicki, J.; Xu, Z.; Ismanto, H.S.; Davila, A.; Teraguchi, S.; Katoh, K.; Standley, D.M. Flexible, Functional, and Familiar: Characteristics of SARS-CoV-2 Spike Protein Evolution. Front. Microbiol. 2020, 11, 2112. [Google Scholar] [CrossRef]
- Zhang, L.; Jackson, C.; Mou, H.; Ojha, A.; Rangarajan, E.; Izard, T.; Farzan, M.; Choe, H. The D614G mutation in the SARS-CoV-2 spike protein reduces S1 shedding and increases infectivity. bioRxiv 2020. [Google Scholar] [CrossRef]
- Chan, J.F.W.; Yuan, S.; Kok, K.H.; To, K.K.W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.; Poon, R.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020. [Google Scholar] [CrossRef]
- Xiao, K.; Zhai, J.; Feng, Y.; Xhou, N.; Zhang, X.; Zou, J.J.; Na, L.; Yaqiong, G.; Xiaobing, L.; Xuejuan, S.; et al. Isolation and characterization of 2019-nCoV-like coronavirus from Malayan Pangolins. bioRxiv 2020. [Google Scholar] [CrossRef]
- Zaki, A.M.; Van Boheemen, S.; Bestebroer, T.M.; Osterhaus, A.D.; Fouchier, R.A. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- Durai, P.; Batool, M.; Shah, M.; Choi, S. Middle East respiratory syndrome coronavirus: Transmission, virology and therapeutic targeting to aid in outbreak control. Exp. Mol. Med. 2015, 47. [Google Scholar] [CrossRef] [PubMed]
- Carlos, W.G.; Crus, C.; Cao, B.; Pasnick, S.; Jamil, S. Novel Wuhan (2019-nCoV) coronavirus. Am. J. Respir. Crit. Care Med. 2020, 201, 7–8. [Google Scholar] [CrossRef] [PubMed]
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus disease 19 (COVID-19): Implications for clinical dental care. J. Endod. 2020, 45, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Sun, W.; Huang, J.; Gamber, M.; Wu, J.; He, G. Indirect Virus Transmission in Cluster of COVID-19 Cases, Wenzhou, China, 2020. Emerg. Infect. Dis. 2020, 26. [Google Scholar] [CrossRef]
- Drosten, C.; Meyer, B.; Müller, M.A.; Corman, V.M.; Al-Masri, M.; Hossain, R.; Madani, H.; Sieber, A.; Bosch, B.; Lattwein, E.; et al. Transmission of MERS-coronavirus in household contacts. N. Engl. J. Med. 2014, 371, 828–835. [Google Scholar] [CrossRef]
- Santarpia, J.L.; Rivera, D.N.; Herrera, V.; Morwitzer, M.J.; Creager, H.; Santarpia, G.W.; Crown, K.; Brett-Major, D.; Schnaubelt, E.; Broadhurst, M.J.; et al. Transmission potential of SARS-CoV-2 in viral shedding observed at the University of Nebraska Medical Center. MedrXiv 2020. [Google Scholar] [CrossRef]
- Soetikno, R.; Teoh, A.Y.; Kaltenbach, T.; Lau, J.Y.; Asokkumar, R.; Cabral-Prodigalidad, P.; Shergill, A. Considerations in performing endoscopy during the COVID-19 pandemic. Gastrointest. Endosc. 2020. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, S.; Xue, Y. Fecal specimen diagnosis 2019 novel coronavirus–infected pneumonia. J. Med. Virol. 2020, 92, 680–682. [Google Scholar] [CrossRef]
- Chen, L.; Lou, J.; Bai, Y.; Wang, M. COVID-19 disease with positive fecal and negative pharyngeal and sputum viral tests. Am. J. Gastroenterol. 2020, 115. [Google Scholar] [CrossRef]
- Xiao, F.; Sun, J.; Xu, Y.; Li, F.; Huang, X.; Li, H.; Zhao, J.; Huang, J.; Zhao, J. Infectious SARS-CoV-2 in feces of patient with severe COVID-19. Emerg. Infect. Dis. 2020, 26, 1920. [Google Scholar] [CrossRef]
- Cheung, K.S.; Hung, I.F.; Chan, P.P.; Lung, K.C.; Tso, E.; Liu, R.; Ng, Y.Y.; Chu, M.Y.; Chung, T.W.; Tam, A.R.; et al. Gastrointestinal manifestations of SARS-CoV-2 infection and virus load in fecal samples from the Hong Kong cohort and systematic review and meta-analysis. Gastroenterology 2020. [Google Scholar] [CrossRef]
- Phua, J.; Weng, L.; Ling, L.; Egi, M.; Lim, C.M.; Divatia, J.V.; Shrestha, B.; Arabi, Y.; Ng, J.; Gomersall, C.; et al. Intensive care management of coronavirus disease 2019 (COVID-19): Challenges and recommendations. Lancet Respir. Med. 2020, 8, 506–517. [Google Scholar] [CrossRef]
- Chen, H.; Guo, J.; Wang, C.; Luo, X.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef]
- Cevik, M.; Bamford, C.; Ho, A. COVID-19 pandemic—A focused review for clinicians. Clin. Microbiol. Infect. 2020, 26, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.; Alqusairi, R.; Adams, A.; Paul, M.; Kothari, N.; Peters, S.; DeBenedet, A. SARS-CoV-2 gastrointestinal infection causing hemorrhagic colitis: Implications for detection and transmission of COVID-19 disease. Am. J. Gastroenterol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.K.; Peng, S.; Li, L.Q.; Wang, Q.; Ping, W.; Zhang, N.; Fu, X.N. Clinical and transmission characteristics of Covid-19—a retrospective study of 25 cases from a single thoracic surgery department. Curr. Med. Sci. 2020, 40, 295–300. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Laboratory Testing of Human Suspected Cases of Novel Coronavirus (nCoV) Infection. Available online: https://apps.who.int/iris/bitstream/handle/10665/330374/WHO-2019-nCoV-laboratory-2020.1-eng.pdf (accessed on 17 May 2020).
- World Health Organization. Laboratory Testing for 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases. Available online: https://apps.who.int/iris/bitstream/handle/10665/330676/9789240000971-eng.pdf?sequence=1&isAllowed=y (accessed on 17 May 2020).
- Corman, V.; Bleicker, T.; Brünink, S.; Drosten, C.; Olfert, L.; Koopmans, M.; Zambon, M. Diagnostic Detection of Wuhan Coronavirus 2019 by Real-Time RT-PCR. Available online: https://www.who.int/docs/default-source/coronaviruse/wuhan-virus-assay-v1991527e5122341d99287a1b17c111902.pdf?sfvrsn=d381fc88_2 (accessed on 27 March 2020).
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.; Bleicker, T.; Brunink, S.; Schneider, J.; Schmidt, M.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurvelliance 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Vogels, C.; Brackney, D.; Wang, J.; Kalinich, C.; Ott, I.; Kudo, E.; Lu, P.; Venkataraman, A.; Tokuyama, M.; Moore, A.; et al. SalivaDirect: Simple and sensitive molecular diagnostic test for SARS-CoV-2 surveillance. medRxiv 2020. [Google Scholar] [CrossRef]
- Lei, J.; Li, J.; Li, X.; Qi, X. CT Imaging of the 2019 Novel Coronavirus (2019-nCoV) Pneumonia. Radiology 2020. [Google Scholar] [CrossRef]
- Kanne, J.P. Chest CT Findings in 2019 novel coronavirus (2019-nCoV) infections from Wuhan, China: Key points for the radiologist. Radiology 2020. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wong, A. COVID-Net: A Tailored Deep Convolutional Neural Network Design for Detection of COVID-19 Cases from Chest Radiography Images. arXiv 2020. Available online: https://arxiv.org/abs/2003.09871 (accessed on 17 May 2020). [CrossRef] [PubMed]
- Li, L.; Qin, L.; Xu, Z.; Yin, Y.; Wang, X.; Kong, B.; Bai, J.; Lu, Y.; Fang, Z.; Song, Q.; et al. Artificial intelligence distinguishes COVID-19 from community acquired pneumonia on chest CT. Radiology 2020. [Google Scholar] [CrossRef] [PubMed]
- Zumla, A.; Hui, D.S.; Azhar, E.I.; Memish, Z.A.; Maeurer, M. Reducing mortality from 2019-nCoV: Host-directed therapies should be an option. Lancet 2020. [Google Scholar] [CrossRef]
- World Health Organization. Novel Coronavirus (2019-nCoV) Advice for the Public: Myth Busters. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/myth-busters (accessed on 17 May 2020).
- AYTU Bioscience. COVID-19 IgG/IgM Rapid Test. Available online: https://aytubio.com/covid-19/ (accessed on 17 May 2020).
- Nordic Biosite. SARS-CoV-2 Ab Rapid Test. Available online: https://www.nordicbiosite.com/product/256-WJ-2750-50/SARSCoV2-Ab-Rapid-Test (accessed on 17 May 2020).
- Biolidics. Coronavirus (COVID-19) Diagnostic Solutions. Available online: https://www.biolidics.com/ (accessed on 17 May 2020).
- Snibe Diagnostic. The World’s First 2019-nCoV (SARS-CoV-2) CLIA Kits Received CE Mark. Available online: http://www.snibe.com/zh_en/en_newsView.aspx?id=576 (accessed on 17 May 2020).
- 360Dx. Snibe Diagnostic Receives CE Mark for SARS-CoV-2 Kits, Immunoassay System. Available online: https://www.360dx.com/regulatory-news-fda-approvals/snibe-diagnostic-receives-ce-mark-sars-cov-2-kits-immunoassay-system#.XsGDYWgzZPY (accessed on 17 May 2020).
- BioSpectrum. Abbott Launches COVID-19 Antibody Test. Available online: https://www.biospectrumasia.com/news/26/15926/abbott-launches-covid-19-antibody-test.html (accessed on 17 May 2020).
- Sona Nanotech. Sona Nanotech Provides a Progress Update on its Covid-19 Antigen Test. 2020. Available online: https://sonanano.com/sona-nanotech-provides-a-progress-update-on-its-covid-19-antigen-test/ (accessed on 17 May 2020).
- Coris BioConcept. COVID-19 Ag Respi-Strip. 2020. Available online: https://www.corisbio.com/Products/Human-Field/Covid-19.php (accessed on 17 May 2020).
- Mertens, P.; De Vos, N.; Martiny, D.; Jassoy, C.; Mirazimi, A.; Cuypers, L.; Wijngaert, S.; Monteil, V.; Melin, P.; Stoffels, K.; et al. Development and Potential Usefulness of the COVID-19 Ag Respi-Strip Diagnostic Assay in a Pandemic Context. Front. Med. 2020, 7, 225. [Google Scholar] [CrossRef]
- Sugentech. COVID-19 IgM/IgG. Available online: https://sugentech.com/products/products-view.php?ct=7&target=32 (accessed on 17 May 2020).
- Food and Drug Administration. FDA Advisory No. 2020-483 || FDA Approves Rapid Antibody Test Kits for COVID-19. Available online: https://www.fda.gov.ph/fda-advisory-no-2020-483-fda-approves-rapid-antibody-test-kits-for-covid-19/ (accessed on 17 May 2020).
- Veredus. Singapore HSA issued Veredus Laboratories with Provisional Authorisation for LIONRUN Diagnostic Kit for Antibody IgM/IgG of Novel Coronavirus COVID-19 for In vitro Diagnostic (IVD) Use. Available online: https://vereduslabs.com/category/news-and-updates/ (accessed on 17 May 2020).
- Grit Overseas. Diagnosure COVID-19 IgG/IgM Rapid Test Cassette. Available online: https://gritoverseas.com/glukrylate-2/ (accessed on 17 May 2020).
- Ortho Clinical Diagnostics. Ortho’s Total Antibody Test for COVID-19 Receives Emergency Use Authorization from FDA. Available online: https://www.orthoclinicaldiagnostics.com/en-us/home/ortho-total-antibody-test-for-covid-19-receives-emergency-use-authorization-from-fda (accessed on 17 May 2020).
- MP Biomedicals Asia Pacific. MP Diagnostics ASSURE® SARS-CoV-2 IgG/IgM Rapid Test. Available online: https://www.hsa.gov.sg/docs/default-source/hprg-mdb/mp-biomedicals_provisional-authorisation-for-covid-19-tests_12052020.pdf (accessed on 17 May 2020).
- Health Science Authority. HSA Expedites Approval of COVID-19 Diagnostic Tests in Singapore via Provisional Authorisation. Available online: https://www.hsa.gov.sg/announcements/regulatory-updates/hsa-expedites-approval-of-covid-19-diagnostic-tests-in-singapore-via-provisional-authorisation (accessed on 17 May 2020).
- Roche. Elecsys® Anti-SARS-CoV-2. Available online: https://diagnostics.roche.com/global/en/products/params/elecsys-anti-sars-cov-2.html#selectProfile (accessed on 17 May 2020).
- Carter, L.J.; Garner, L.V.; Smoot, J.W.; Li, Y.; Zhou, Q.; Saveson, C.J.; Sasso, J.; Gregg, A.; Soares, D.; Beskid, T.; et al. Assay Techniques and Test Development for COVID-19 Diagnosis. ACS Cent. Sci. 2020, 6, 591–605. [Google Scholar] [CrossRef]
- Broughton, J.P.; Deng, X.; Yu, G.; Fasching, C.L.; Servellita, V.; Singh, J.; Miao, X.; Streithorst, J.; Granados, A.; Sotomayor-Gonzalez, A.; et al. CRISPR–Cas12-based detection of SARS-CoV-2. Nat. Biotechnol. 2020. [Google Scholar] [CrossRef]
- Financial Express. Available online: https://www.financialexpress.com/lifestyle/health/covid-19-test-result-in-minutes-feluda-indias-first-paper-strip-test-check-details/1949771/ (accessed on 17 May 2020).
- The Economic Times. Available online: https://economictimes.indiatimes.com/magazines/panache/feluda-provides-a-ray-of-hope-in-coronavirus-vaccine/articleshow/75749518.cms (accessed on 17 May 2020).
- Peeri, N.C.; Shrestha, N.; Rahman, M.S.; Zaki, R.; Tan, Z.; Bibi, S.; Bahgbanzadeh, M.; Aghamohammadi, N.; Zhang, W.; Haque, U. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: What lessons have we learned? Int. J. Epidemiol. 2020. [Google Scholar] [CrossRef]
- Kock, R.A.; Karesh, W.B.; Veas, F.; Velavan, T.P.; Simons, D.; Mboera, L.; Dar, O.; Arruda, L.; Zumla, A. 2019-nCoV in context: Lessons learned? Lancet Planet. Health 2020. [Google Scholar] [CrossRef]
- Smith, N.; Fraser, M. Straining the system: Novel coronavirus (COVID-19) and preparedness for concomitant disasters. Am. J. Public Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Heymann, D.L.; Shindo, N. COVID-19: What is next for public health? Lancet 2020. [Google Scholar] [CrossRef]
- Lu, H. Drug treatment options for the 2019-new coronavirus (2019-nCoV). Biosci. Trends 2020. [Google Scholar] [CrossRef]
- Wang, F.S.; Zhang, C. What to do next to control the 2019-nCoV epidemic? Lancet 2020. [Google Scholar] [CrossRef]
- New Straits Times. Thailand Sees Apparent Success Treating Coronavirus with HIV Drug. Available online: https://www.nst.com.my/world/world/2020/02/562079/thailand-sees-apparent-success-treating-coronavirus-hiv-drug (accessed on 17 May 2020).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Guohui, F.; Jiuyang, X.; Xiaoying, G.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020. [Google Scholar] [CrossRef]
- Cao, Y.C.; Deng, Q.X.; Dai, S.X. Remdesivir for severe acute respiratory syndrome coronavirus 2 causing COVID-19: An evaluation of the evidence. Travel Med. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Stebbing, J.; Phelan, A.; Griffin, I.; Tucker, C.; Oechsle, O.; Smith, D.; Richardson, P. COVID-19: Combining antiviral and anti-inflammatory treatments. Lancet Infect. Dis. 2020, 20, 400–402. [Google Scholar] [CrossRef]
- National Institutes of Health. NIH Clinical Trial Testing Antiviral Remdesivir Plus Anti-Inflammatory Drug Baricitinib for COVID-19 Begins. Available online: https://www.nih.gov/news-events/news-releases/nih-clinical-trial-testing-antiviral-remdesivir-plus-anti-inflammatory-drug-baricitinib-covid-19-begins (accessed on 10 May 2020).
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y.; et al. Experimental treatment with favipiravir for COVID-19: An open-label control study. Engineering 2020. [Google Scholar] [CrossRef]
- Hornyak, T. Japan Sending Fujifilm’s Flu Drug Favipiravir to Over 40 Countries for Covid-19 Trials. Available online: https://www.cnbc.com/2020/05/04/fujifilms-flu-drug-favipiravir-sent-to-43-nations-for-covid-19-trials.html (accessed on 10 May 2020).
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell. Res. 2020, 30, 269–271. [Google Scholar] [CrossRef]
- Cortegiani, A.; Ingoglia, G.; Ippolito, M.; Giarratano, A.; Einav, S. A systematic review on the efficacy and safety of chloroquine for the treatment of COVID-19. J. Crit. Care 2020. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Maddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Viera, V.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020. [Google Scholar] [CrossRef] [PubMed]
- Geleris, J.; Sun, Y.; Platt, J.; Zucker, J.; Baldwin, M.; Hripcsak, G.; Labella, A.; Manson, D.; Kubin, C.; Barr, R.G.; et al. Observational study of hydroxychloroquine in hospitalized patients with Covid-19. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kupferschmidt, K.; Cohen, J. Race to find COVID-19 treatments accelerates. Science 2020, 367, 1412–1413. [Google Scholar] [CrossRef] [PubMed]
- Rosa, S.; Santos, W.C. Clinical trials on drug repositioning for COVID-19 treatment. Rev. Panam. Salud Publica 2020, 44. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Hou, Y.; Shen, J.; Huang, Y.; Marin, W.; Cheng, F. Network-based Drug Repurposing for Novel Coronavirus 2019-nCoV/SARS-CoV-2. Cell. Discov. 2020. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Liu, G.; Mellacheruvu, D.; Tyers, M.; Gingras, A.; Nesvizhskii, A. Analyzing protein-protein interactions from affinity purification-mass spectrometry data with SAINT. Curr. Protoc. Bioinform. 2012, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Gordon, D.E.; Jang, G.M.; Bouhaddou, M.; Xu, J.; Obernier, K.; O’Meara, M.; Rezelj, V.; Guo, J.; Swaney, D.; Tummino, T.; et al. A SARS-CoV-2-human protein-protein interaction map reveals drug targets and potential drug-repurposing. bioRxiv 2020. [Google Scholar] [CrossRef]
- Surjit, M.; Liu, B.; Jameel, S.; Chow, V.; Lal, S. The SARS coronavirus nucleocapsid protein induces actin reorganization and apoptosis in COS-1 cells in the absence of growth factors. Biochem. J. 2004, 383, 13–18. [Google Scholar] [CrossRef]
- Casella, J.F.; Flanagan, M.D.; Lin, S. Cytochalasin D inhibits actin polymerization and induces depolymerization of actin filaments formed during platelet shape change. Nature 1981, 293, 302–305. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. PubChem Database, Cytochalasin D. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Cytochalasin-D (accessed on 3 April 2020).
- Surjit, M.; Liu, B.; Chow, V.; Lal, S. The nucleocapsid protein of severe acute respiratory syndrome-coronavirus inhibits the activity of cyclin-cyclin-dependent kinase complex and blocks S phase progression in mammalian cells. J. Biol. Chem. 2006, 81, 10669–10681. [Google Scholar] [CrossRef]
- Susman, E. Novel Agent Extends Breast Cancer Time to Progression. Available online: https://www.medpagetoday.com/MeetingCoverage/SABCS/36306 (accessed on 17 May 2020).
- Lu, J. Palbociclib: A first-in-class CDK4/CDK6 inhibitor for the treatment of hormone-receptor positive advanced breast cancer. J. Hematol. Oncol. 2015, 8. [Google Scholar] [CrossRef] [PubMed]
- Surjit, M.; Kumar, R.; Mishra, N.; Reddy, K.; Chow, V.; Lal, S. The severe acute respiratory syndrome coronavirus nucleocapsid protein is phosphorylated and localizes in the cytoplasm by 14-3-3-mediated translocation. J. Virol. 2005, 79, 11476–11486. [Google Scholar] [CrossRef] [PubMed]
- R&D Systems. R18. Available online: https://www.rndsystems.com/products/r18_2144 (accessed on 17 May 2020).
- DrugBank. Phenethyl Isothiocynate. Available online: https://www.drugbank.ca/drugs/DB12695 (accessed on 17 May 2020).
- Sharma, K.; Åkerström, S.; Sharma, A.K.; Chow, V.; Teow, S.; Abrenica, B.; Booth, S.; Mirazimi, A.; Lal, S. SARS-CoV 9b protein diffuses into nucleus, undergoes active Crm1 mediated nucleocytoplasmic export and triggers apoptosis when retained in the nucleus. PLoS ONE 2011, 6. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. FDA Grants Accelerated Approval to Selinexor for Multiple Myeloma. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-selinexor-multiple-myeloma (accessed on 17 May 2020).
- U.S Food and Drug Administration. Drugs@FDA Isoniazid. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=008678 (accessed on 8 April 2020).
- Varshney, B.; Lal, S. SARS-CoV accessory protein 3b induces AP-1 transcriptional activity through activation of JNK and ERK pathways. Biochemistry 2011, 50, 5419–5425. [Google Scholar] [CrossRef]
- U.S Food and Drug Administration. Drugs@FDA Trisenox. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&varApplNo=021248 (accessed on 8 April 2020).
- Cao, W.; Liu, X.; Bai, T.; Fan, H.; Hong, K.; Song, H.; Han, Y.; Lin, L.; Ruan, L.; Li, T. High-dose intravenous immunoglobulin as a therapeutic option for deteriorating patients with coronavirus disease 2019. Open Forum Infect. Dis. 2020, 7. [Google Scholar] [CrossRef]
- National Institutes of Health. The Efficacy of Intravenous Immunoglobulin Therapy for Severe 2019-nCoV Infected Pneumonia. Available online: https://clinicaltrials.gov/ct2/show/NCT04261426 (accessed on 10 May 2020).
- Businesswire. New COVID-19 clinical trial supported by Octapharma USA. Available online: https://www.eurekalert.org/pub_releases/2020-04/ypr-ncc041520.php (accessed on 25 April 2020).
- Shen, C.; Wang, Z.; Zhao, F.; Yang, Y.; Li, J.; Yuan, J.; Wang, F.; Li, D.; Yang, M.; Xing, L. Treatment of 5 critically ill patients with COVID-19 with convalescent plasma. JAMA 2020, 323, 1582–1589. [Google Scholar] [CrossRef]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc. Natl. Acad. Sci. USA 2020. [Google Scholar] [CrossRef]
- Guaraldi, G.; Meschiari, M.; Cozzi-Lepri, A.; Milic, J.; Tonelli, R.; Menozzi, M.; Franceschini, E.; Cuomo, G.; Orlando, G.; Borghi, V.; et al. Tocilizumab in patients with severe COVID-19: A retrospective cohort study. Lancet Rheumatol. 2020, 2, 474–484. [Google Scholar] [CrossRef]
- Liu, C.; Zhou, Q.; Li, Y.; Garner, L.V.; Watkins, S.P.; Carter, L.J.; Smoot, J.; Gregg, A.; Daniels, A.; Jervey, S.; et al. Research and development on therapeutic agents and vaccines for COVID-19 and related human coronavirus diseases. ACS Cen. Sci. 2020, 6, 315–331. [Google Scholar] [CrossRef]
- Regulatory Affairs Professionals Society. Available online: https://www.raps.org/news-and-articles/news-articles/2020/3/covid-19-vaccine-tracker (accessed on 5 September 2020).
- Carlson, R. mRNA-1273 SARS-CoV-2 Vaccine. Available online: https://www.precisionvaccinations.com/vaccines/mrna-1273-sars-cov-2-vaccine (accessed on 17 May 2020).
- Taylor, P.N. Moderna Eyes ‘Early Summer’ Start for Phase 3 COVID-19 Vaccine Trial. FierceBiotech. Available online: https://www.fiercebiotech.com/biotech/moderna-eyes-early-summer-start-for-phase-3-covid-19-vaccine-trial (accessed on 17 May 2020).
- National Institutes of Health. NIH Clinical Trial of Investigational Vaccine for COVID-19 Begins. Available online: https://www.nih.gov/news-events/news-releases/nih-clinical-trial-investigational-vaccine-covid-19-begins (accessed on 17 May 2020).
- DrugBank. mRNA-1273. Available online: https://www.drugbank.ca/drugs/DB15654 (accessed on 17 May 2020).
- U.S. National Library of Medicine. Phase I Clinical Trial of a COVID-19 Vaccine in 18-60 Healthy Adults (CTCOVID-19). Available online: https://clinicaltrials.gov/ct2/show/record/NCT04313127?view=record (accessed on 17 May 2020).
- Carlson, R. Ad5-nCoV COVID-19 Vaccine. Available online: https://www.precisionvaccinations.com/vaccines/ad5-ncov-covid-19-vaccine (accessed on 17 May 2020).
- CanSino Biologics. China’s COVID-19 Vaccine Called Ad5-nCoV Moves into Phase II Clinical Trial, 500 Volunteers Sought. Available online: https://www.trialsitenews.com/chinas-covid-19-vaccine-called-ad5-ncov-moves-into-phase-ii-clinical-trial-500-volunteers-sought/ (accessed on 17 May 2020).
- DrugBank. Ad5-nCoV. Available online: https://www.drugbank.ca/drugs/DB15655 (accessed on 17 May 2020).
- U.S. National Library of Medicine. Phase III Trial of A COVID-19 Vaccine of Adenovirus Vector in Adults 18 Years Old and Above. Available online: https://clinicaltrials.gov/ct2/show/NCT04526990 (accessed on 5 September 2020).
- U.S. National Library of Medicine. A Study of a Candidate COVID-19 Vaccine (COV001). Available online: https://clinicaltrials.gov/ct2/show/NCT04324606?term=vaccine&cond=covid-19&draw=2 (accessed on 17 May 2020).
- Sanal, M.G.; Dubey, R.C. An Oral Live Attenuated Vaccine Strategy against Severe Acute Respiratory Syndrome Coronavirus 2 (2019-nCoV). Available online: https://www.preprints.org/manuscript/202004.0153/v1 (accessed on 17 May 2020).
- Van Doremalen, N.; Lambe, T.; Spencer, A.; Belij-Rammerstorfer, S.; Purushotham, J.N.; Port, J.R.; Avanzato, V.; Bushmaker, T.; Flaxman, A.; Ulaszewska, M.; et al. ChAdOx1 nCoV-19 vaccination prevents SARS-CoV-2 pneumonia in rhesus macaques. Nature 2020. [Google Scholar] [CrossRef]
- U.S. National Library of Medicine. Phase III Double-blind, Placebo-controlled Study of AZD1222 for the Prevention of COVID-19 in Adults. Available online: https://clinicaltrials.gov/ct2/show/NCT04516746 (accessed on 5 September 2020).
- Carlson, R. AZD1222 SARS-CoV-2 Vaccine. Available online: https://www.precisionvaccinations.com/vaccines/azd1222-sars-cov-2-vaccine (accessed on 5 September 2020).
- Redelman-Sidi, G. Could BCG be used to protect against COVID-19? Nat. Rev. Urol. 2020. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. Application of BCG Vaccine for Immune-Prophylaxis among Egyptian Healthcare Workers during the Pandemic of COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04350931?term=vaccine&cond=COVID-19&draw=2&rank=1 (accessed on 17 May 2020).
- U.S. National Library of Medicine. Reducing Health Care Workers Absenteeism in Covid-19 Pandemic through BCG Vaccine (BCG-CORONA). Available online: https://clinicaltrials.gov/ct2/show/NCT04328441?term=vaccine&cond=COVID-19&draw=2&rank=2 (accessed on 17 May 2020).
- U.S. National Library of Medicine. Measles Vaccine in HCW (MV-COVID19). Available online: https://clinicaltrials.gov/ct2/show/NCT04357028?term=Measles-Mumps-Rubella&cond=COVID&draw=2&rank=1 (accessed on 17 May 2020).
- U.S. National Library of Medicine. Study to Describe the Safety, Tolerability, Immunogenicity, and Potential Efficacy of RNA Vaccine Candidates against COVID-19 in Healthy Adults. Available online: https://clinicaltrials.gov/ct2/show/NCT04368728?term=vaccine&type=Intr&cond=COVID-19&draw=3&rank=15 (accessed on 17 May 2020).
- Carlson, R. INO-4800 DNA Coronavirus Vaccine. Available online: https://www.precisionvaccinations.com/vaccines/ino-4800-dna-coronavirus-vaccine (accessed on 17 May 2020).
- U.S. National Library of Medicine. Safety, Tolerability and Immunogenicity of INO-4800 for COVID-19 in Healthy Volunteers. Available online: https://clinicaltrials.gov/ct2/show/NCT04336410?term=INO-4800&cond=COVID&draw=2&rank=1 (accessed on 17 May 2020).
- U.S. National Library of Medicine. Safety, Tolerability and Immunogenicity of INO-4800 Followed by Electroporation in Healthy Volunteers for COVID19. Available online: https://clinicaltrials.gov/ct2/show/NCT04447781 (accessed on 5 September 2020).
- U.S. National Library of Medicine. Safety and Immunity of Covid-19 aAPC Vaccine. Available online: https://clinicaltrials.gov/ct2/show/NCT04299724?term=vaccine&type=Intr&cond=COVID-19&draw=2&rank=5 (accessed on 17 May 2020).
- U.S. National Library of Medicine. Immunity and Safety of Covid-19 Synthetic Minigene Vaccine. Available online: https://clinicaltrials.gov/ct2/show/NCT04276896?term=vaccine&type=Intr&cond=COVID-19&draw=2&rank=7 (accessed on 17 May 2020).
- U.S. National Library of Medicine. Tableted COVID-19 Therapeutic Vaccine (COVID-19). Available online: https://clinicaltrials.gov/ct2/show/NCT04380532?term=vaccine&type=Intr&cond=COVID-19&draw=3&rank=14 (accessed on 17 May 2020).
- Silin, D.S.; Lyubomska, O.V.; Jirathitikal, V.; Bourinbaiar, A.S. Oral vaccination: Where we are? Expert Opin. Drug Deliv. 2007, 4, 323–340. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. Phase Ib-II Trial of Dendritic Cell Vaccine to Prevent COVID-19 in Frontline Healthcare Workers and First Responders. Available online: https://clinicaltrials.gov/ct2/show/NCT04386252?term=AV-COVID-19&cond=COVID&draw=2&rank=1 (accessed on 17 May 2020).
- U.S. National Library of Medicine. Safety and Immunogenicity Study of Inactivated Vaccine for Prophylaxis of SARS CoV-2 Infection (COVID-19). Available online: https://clinicaltrials.gov/ct2/show/NCT04352608?term=vaccine&cond=COVID&strd_s=04%2F01%2F2020&strd_e=05%2F15%2F2020&draw=2&rank=2 (accessed on 17 May 2020).
- U.S. National Library of Medicine. Safety and Immunogenicity Study of GX-19, a COVID-19 Preventive DNA Vaccine in Healthy Adults. Available online: https://clinicaltrials.gov/ct2/show/NCT04445389 (accessed on 5 September 2020).
- U.S. National Library of Medicine. Evaluation of the Safety and Immunogenicity of a SARS-CoV-2 rS (COVID-19) Nanoparticle Vaccine With/Without Matrix-M Adjuvant. Available online: https://clinicaltrials.gov/ct2/show/NCT04368988?term=vaccine&cond=COVID&strd_s=04%2F01%2F2020&strd_e=05%2F15%2F2020&draw=2&rank=8 (accessed on 17 May 2020).
- Carlson, R. NVX-CoV2373 SARS-CoV-2 Vaccine. Available online: https://www.precisionvaccinations.com/vaccines/nvx-cov2373-sars-cov-2-vaccine (accessed on 17 May 2020).
- U.S. National Library of Medicine. Evaluating the Safety, Tolerability and Immunogenicity of bacTRL-Spike Vaccine for Prevention of COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04334980?term=vaccine&cond=COVID&strd_s=04%2F01%2F2020&strd_e=05%2F15%2F2020&draw=2&rank=9 (accessed on 17 May 2020).
- U.S. National Library of Medicine. Available online: https://clinicaltrials.gov/ (accessed on 5 September 2020).
- Precision Vaccinations. SCB-2019 SARS-CoV-2 Vaccine. Available online: https://www.precisionvaccinations.com/vaccines/scb-2019-sars-cov-2-vaccine (accessed on 5 September 2020).
- Gao, Q.; Bao, L.; Mao, H.; Wang, L.; Xu, K.; Yang, M.; Li, Y.; Zhu, L.; Wang, N.; Lv, Z.; et al. Development of an inactivated vaccine candidate for SARS-CoV-2. Science 2020. [Google Scholar] [CrossRef] [PubMed]
- Nandy, A.; Basak, S.C. The Wuhan Epidemic 2019- a commentary. Rapid Response Emerg. Epidemics 2020. [Google Scholar] [CrossRef]
- Söllner, J.; Heinzel, A.; Summer, G.; Fechete, R.; Stipkovits, L.; Szathmary, S.; Mayer, B. Concept and application of a computational vaccinology workflow. Immun. Res. 2010, 6. [Google Scholar] [CrossRef] [PubMed]
- Basak, S.C.; Majumdar, S.; Nandy, A.; Roy, P.; Dutta, T.; Vracko, M.; Bhattacharjee, A. Computer-assisted and data driven approaches for surveillance, drug discovery, and vaccine design for the Zika virus. Pharmaceuticals 2019, 12, 157. [Google Scholar] [CrossRef]
- Anwar, S.; Mourosi, J.T.; Khan, M.F.; Hosen, M.J. Prediction of epitope-based peptide vaccine against the Chikungunya virus by immune-informatics approach. Curr. Pharm. Biotechnol. 2019. [Google Scholar] [CrossRef]
- Chakraborty, S.; Barman, A.; Deb, B. Japanese encephalitis virus: A multi-epitope loaded peptide vaccine formulation using reverse vaccinology approach. Infect. Genet. Evol. 2020, 78, 104106. [Google Scholar] [CrossRef]
- Ahmed, S.F.; Quadeer, A.A.; McKay, M.R. Preliminary identification of potential vaccine targets for 2019-nCoV based on SARS-CoV immunological studies. bioRxiv 2020. [Google Scholar] [CrossRef]
- Joob, B.; Wiwanitkit, V. Epitope finding in 2019 novel coronavirus (2019-nCoV): The first world report. Asian Pac. J. Trop. Med. 2020. [Google Scholar] [CrossRef]
- Chen, W.H.; Strych, U.; Hotez, P.J.; Bottazzi, M.E. The SARS-CoV-2 vaccine pipeline: An overview. Curr. Trop. Med. Rep. 2020. [Google Scholar] [CrossRef] [PubMed]
- Brightling, C.E.; Symon, F.A.; Birring, S.S.; Bradding, P.; Wardlaw, A.J.; Pavord, I.D. Comparison of airway immunopathology of eosinophilic bronchitis and asthma. Thorax 2003, 58, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Simon, H.U.; Karaulov, A.V.; Bachmann, M.F. Strategies to Prevent SARS-CoV-2-Mediated Eosinophilic Disease in Association with COVID-19 Vaccination and Infection. Int. Arch. Allergy Immunol. 2020, 181, 624–628. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Coordinated Global Research Roadmap–12 March 2020. Available online: https://www.who.int/who-documents-detail/a-coordinated-global-research-roadmap (accessed on 17 May 2020).
- Carvalho, V.; Hansen, S.; Ortiz, G.; Rodrigo, T.; Mora, S.; Ruiz, J. DP14642 Tracking the COVID-19 Crisis with High-Resolution Transaction Data. Available online: https://cepr.org/active/publications/discussion_papers/dp.php?dpno=14642 (accessed on 15 August 2020).
- Yen, M.Y.; Schwartz, J.; Chen, S.Y.; King, C.C.; Yang, G.Y.; Hsueh, P.R. Interrupting COVID-19 transmission by implementing enhanced traffic control bundling: Implications for global prevention and control efforts. J. Microbiol. Immunol. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kucharski, A.J.; Russell, T.W.; Diamond, C.; Liu, Y.; Edmunds, J.; Funk, S.; Eggo, R. Early dynamics of transmission and control of COVID-19: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 553–558. [Google Scholar] [CrossRef]
- Yang, Z.; Zeng, Z.; Wang, K.; Wong, S.S.; Liang, W.; Zanin, M.; Liu, P.; Cao, X.; Gao, Z.; Mai, Z.; et al. Modified SEIR and AI prediction of the epidemics trend of COVID-19 in China under public health interventions. J. Thorac. Dis. 2020, 12, 165–174. [Google Scholar] [CrossRef]
- Chenar, S.S.; Deng, Z. Development of artificial intelligence approach to forecasting oyster norovirus outbreaks along Gulf of Mexico coast. Environ. Int. 2018, 111, 212–223. [Google Scholar] [CrossRef]
- Shi, Y.; Liu, X.; Kok, S.Y.; Rajarethinam, J.; Liang, S.; Yap, G.; Chong, C.S.; Lee, K.S.; Tan, S.S.; Chin, C.K.Y.; et al. Three-month real-time dengue forecast models: An early warning system for outbreak alerts and policy decision support in Singapore. Environ. Health Perspect. 2016, 124, 1369–1375. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. 2019 Novel Coronavirus Prevention & Treatment. Available online: https://www.cdc.gov/coronavirus/2019-nCoV/about/prevention-treatment.html (accessed on 20 April 2020).
- World Health Organization. Coronavirus. Available online: https://www.who.int/health-topics/coronavirus (accessed on 17 May 2020).
- Daoust, J.F. Elderly people and responses to COVID-19 in 27 Countries. PLoS ONE 2020. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Older Adults. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/older-adults.html (accessed on 9 November 2020).
- Le, H.T.; Nguyen, L.V.; Tran, D.M.; Do, H.T.; Tran, H.T.; Le, Y.T.; Phan, P.H. The first infant case of COVID-19 acquired from a secondary transmission in Vietnam. Lancet Child Adolesc. 2020, 4, 405–406. [Google Scholar] [CrossRef]
- Zeng, L.K.; Tao, X.W.; Yuan, W.H.; Wang, J.; Liu, X.; Liu, Z.S. First case of neonate infected with novel coronavirus pneumonia in China. Zhonghua Er Ke Za Zhi 2020, 58. [Google Scholar] [CrossRef]
- Chen, Y.; Peng, H.; Wang, L.; Zhao, Y.; Zeng, L.; Gao, H.; Liu, Y. Infants born to mothers with a new coronavirus (COVID-19). Front. Pediatr. 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Wang, J.; Mo, Y.; Duan, W.; Xiang, G.; Yi, M.; Bo, L.; Sh, Y. Unlikely SARS-CoV-2 vertical transmission from mother to child: A case report. J. Inf. Public Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Mayo Clinic. COVID-19 (Coronavirus) in Babies and Children. Available online: https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/coronavirus-in-babies-and-children/art-20484405 (accessed on 11 November 2020).
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; Eggo, R.M.; CMMID COVID-19 working group. Age-dependent effects in the transmission and control of COVID-19 epidemics. MedRxiv 2020, 26, 1205–1211. [Google Scholar]
- Guardian Staff and Agencies. Coronavirus: What Airport Measures are in Place to Detect Sick Passengers? Available online: https://www.theguardian.com/world/2020/jan/18/coronavirus-what-airport-measures-are-in-place-to-detect-for-sick-passengers (accessed on 17 May 2020).
- The Japan Times. Countries around World Gear up Response to New Coronavirus. 2020. Available online: https://www.japantimes.co.jp/news/2020/01/22/asia-pacific/science-health-asia-pacific/countries-around-world-gear-response-new-coronavirus/#.XkPgsTEzY2x (accessed on 17 March 2020).
- China Airlines. Novel Coronavirus Service Information. Available online: https://news.china-airlines.com/emer_area/info_en.aspx (accessed on 20 April 2020).
- Malaysia Airlines. 2019-Novel Coronavirus (2019-nCov). Available online: https://www.malaysiaairlines.com/au/en/advisory/china-coronavirus.html (accessed on 17 May 2020).
- Quilty, J.B.; Clifford, S.; CMMID nCoV Working Group; Flasche, S.; Eggo, R.M. Effectiveness of airport screening at detecting travellers infected with novel coronavirus (2019-nCoV) separator commenting unavailable. Eurosurvelliance 2020, 25. [Google Scholar] [CrossRef]
- New Straits Times. Covid-19: Nearly One Billion under Lockdown Worldwide. Available online: https://www.nst.com.my/world/world/2020/03/576869/covid-19-nearly-one-billion-under-lockdown-worldwide (accessed on 17 May 2020).


{kind=link}
| SARS-CoV-2 * | MERS-CoV | SARS-CoV | |
|---|---|---|---|
| Outbreak Date | December 2019 | April 2012 | November 2002 |
| Epicenter of Disease Outbreak | Wuhan, China | Jeddah, Saudi Arabia | Guangdong, China |
| Original/Intermediate Animal Reservoir | Bats, Pangolins and potentially other mammals | Bats/Camels | Bats/Masked palm civets |
| Number of Cases | 36,401,583 | 2494 | 8096 |
| Number of Deaths | 1,060,567 | 858 | 744 |
| Transmission Rate | 3–4 | <1 | 3 |
| Fatality Rate | 1.4% | 37% | 10% |
| Countries/Territories affected | 214 | 27 | 26 |
| Coronavirus Strain | Genomic Sequence Similarity to SARS-CoV-2 | Reference |
|---|---|---|
| SARS-like coronavirus bat-RaTG13 | 96.2% | [21] |
| SARS-like coronavirus bat-SL-CoVZC45 | 88% | [21] |
| SARS-like coronavirus bat-SL-CoVZXC21 | 88% | [21] |
| SARS-CoV | 79% | [39] |
| MERS-CoV | 51.8% | [40] |
| Name | Company | Date of Release | Sample Type | Target Antigen | Duration of Test | Country of Validation | References |
|---|---|---|---|---|---|---|---|
| COVID-19 IgG/IgM Point of Care Rapid test | Aytu Biosciences | March 2020 | Whole blood/serum/plasma | IgG/IgM | 2–10 min | China and United States | [80] |
| Wantai SARS-CoV-2 Ab Rapid Test | Beijing Wantai Biological Pharmacy Enterprise | March 2020 | Whole blood/serum/plasma | IgG/IgM | 15 min | China and Australia | [81] |
| Biolidics 2019-nCoV IgG/IgM Detection Ki | Biolidics Limited | March 2020 | Whole blood/serum/plasma | IgG/IgM | <10 min | Singapore | [82] |
| MAGLUMI IgG de 2019-nCoV | Snibe Diagnostic | March 2020 | Whole blood | IgG | 600 tests per hour | Brazil, China and United States | [83,84] |
| m2000 SARS-CoV-2 assay | Abbott Core Laboratory | April 2020 | Whole blood/serum/plasma | IgG | 100–200 tests per hour | United States | [85] |
| Rapid SARS-CoV-2 antigen detection test | Sona Nanotech | April 2020 | nasal or oropharyngeal swabs | S1 subunit | - | Canada and United States | [86] |
| COVID-19 Ag Respi-Strip | Coris Bioconcept | April 2020 | Nasopharyngeal secretions | N protein | <15 min | Belgium | [79,87] |
| SGTi-flex COVID-19 IgM/IgG | Sugentech | April 2020 | Whole blood/serum/plasma | IgG/IgM | 10–15 min | South Korea and United States | [88] |
| INNOVITA 2019-nCoV Ab Test (Colloidal Gold) | Bioforge Solutions Pte Ltd. | April 2020 | Whole blood/serum/plasma | IgG/IgM | <15 min | China, Singapore and United States | [89] |
| Shanghai LiangRun LionRun Diagnostic Kit for Antibody IgM-IgG of Novel Coronavirus COVID-19 | Veredus Laboratories Pte Ltd. | April 2020 | Whole blood/serum/plasma | IgG/IgM | <10 min | China and Singapore | [90] |
| DiagnoSure COVID-19 IgG/IgM Rapid Test Cassette | Grit Overseas Pte Ltd. | April 2020 | Whole blood/serum/plasma | IgG/IgM | <10 min | China, Singapore and Netherlands | [91] |
| VITROS Immunodiagnostic Products Anti-SARSCoV-2 Total Reagent Pack | Ortho Clinical Diagnostics | May 2020 | Serum/plasma | IgG/IgM/IgA | 150 tests per hour | Singapore and United States | [92] |
| MP Diagnostics ASSURE® SARS-CoV-2 IgG/IgM Rapid Test | MP Biomedicals Asia Pacific Pte Ltd. | May 2020 | Whole blood/serum/plasma | IgG/IgM | <25 min | Singapore | [93,94] |
| Roche Elecsys Anti-SARS-CoV-2 | Roche Diagnostics Asia Pacific Pte Ltd. | May 2020 | Serum/plasma | N protein/IgG | 18 min | Singapore | [95] |
| Host Protein | Viral Protein | Effect of Host–Virus Interaction | Antiviral Property of Host Protein | Inhibitors of Host Proteins | References |
|---|---|---|---|---|---|
| Actin | Nucleocapsid (N) | Viral N protein recognizes host actin and induces apoptosis in COS-1 cells | Data not available | Cytochalasin D * | [121,122,123] |
| cyclin-cyclin-dependent kinase complex | Nucleocapsid (N) | N protein inhibits S-phase progression in mammalian cells | Pro-viral - | Palbociclib ^ Abemaciclib * Ribociclib * | [124,125,126] |
| 14-3-3 | Nucleocapsid (N) | Nucleocytoplasmic shuttling of the N protein is mediated by 14-3-3 | Pro-viral - | R18 # Fusicoccin + Phenethyl isothiocyanate + | [127,128,129] |
| CRM1 | 9b accessory protein (9b) | Nuclear shuttling of 9b is dependent on CRM1 | Pro-viral - | Selinexor * Isoniazid * | [130,131,132] |
| AP-1 | 3b accessory protein | 3b protein induces the transcriptional activity of AP-1 | Pro-viral - | Arsenic trioxide * | [133,134] |
| Vaccine Name | Company | Clinical Trial Phase/Identifier | Number of Participants Enrolled in Trial | Vaccine Dosage Received | Vaccine Type | Target/Mode of Action | Reported Adverse Effects | References |
|---|---|---|---|---|---|---|---|---|
| mRNA-1273 | National Institute of Allergy and Infectious Diseases (NIAID) and Moderna | Phase III (NCT04470427) Phase I/II (NCT04283461) | 30,000/600 | 100 μg (intramuscular)/50 μg or 250 μg (intramuscular) | Novel mRNA vaccine encapsulated in lipid nanoparticle for delivery | Encodes for a full-length stabilized form of the S protein | No obvious side effects | [144,145,146,147] |
| Ad5-nCoV | CanSino Biologics Inc and collaboration with National Research Council of Canada and Beijing institute of Biotechnology | Phase III (NCT04526990) Phase II (NCT04341389) | 40,000/500 | Low: 5 × 1010 vp Middle: 1 × 1011 vp High: 1.5 × 1011 vp (intramuscular) | Recombinant adenovirus type-5 vector to express spike protein | Adenovirus vector express SARS-CoV-2 spike protein | High dosage group experienced higher fever within 24 h of administration | [148,149,150,151,152] |
| AZD1222 (Formerly known as: ChAdOx1 nCoV-19) | Oxford University | Phase III (NCT04516746) Phase I/II (NCT04324606) | 30,000/1090 | Single dose of 5 × 1010 vp (intramuscular) Booster dose: 2.5 × 1010 vp | Chimpanzee adenovirus vector encoding spike protein of SARS-CoV-2 | Elicits humoral and cell-mediated response against spike protein | Mild increase in temperature, headache, or sore arm. | [153,154,155,156,157] |
| Bacille Calmette-Guerin (BCG) | Multiple companies | Phase III (NCT04350931) (NCT04328441) | Variable | 0.1 mL intradermal | Attenuated Mycobacterium bovis | Hypothesized that trained immunity would develop and may aid in immunity against COVID-19 | To be assessed | [158,159,160] |
| Measels-Mumps-Rubella vaccine (MMR) | Kasr El Aini Hospital | Phase III (NCT04357028) | 200 | 0.5 mL subcutaneous | Attenuated virus vaccine | Hypothesized that MMR may lower serological incidence caused by SARS-CoV-2 as neutralizing antibodies will be produced | To be assessed | [161] |
| BNT162 (a1, b1, b2, c2) | Biontech RNA Pharmaceuticals GmbH, Pfizer | Phase I/II (NCT04380701) Approaching phase III | 7600 | 0.5 mL (intramuscular) | mRNA and lipid nanoparticle | mRNA encoding spike protein and receptor-binding domain gets delivered via lipid nanoparticles into host cells activating immunity against SARS-CoV-2 | Fever, fatigue, vomiting, diarrhea, or worsened muscle pain | [162] |
| INO-4800 | Inovio Pharmaceuticals Inc. | Phase I/II (NCT04447781) Phase I (NCT04336410) | 160/40 | Two doses of 1 mg each | Plasmid DNA that encodes spike protein | Host cells translate spike protein encoded by plasmid eliciting immune response against spike protein | To be assessed | [163,164,165] |
| COVID-19/aAPC | Shenzhen Geno-Immune Medical Institute | Phase I (NCT04299724) | 100 | Thee injections 5 × 106 each (Subcutaneous) | Modified Lentivirus | Lentivirus vector presents modulatory and viral genes to artificial antigen presenting cells (aAPCs) | To be assessed | [166] |
| LV-SMENP-DC | Shenzhen Geno-Immune Medical Institute | Phase I/II (NCT04276896) | 100 | 5 × 106 (subcutaneous) | Modified Dendritic cells (DC) with Lentivirus | Modified DC with Lentivirus vector carries SMENP minigenes to express COVID-19 antigens to | To be assessed | [167] |
| V-SARS | Immunitor LLC | Phase I/II (NCT04380532) | 20 | Vaccine formulated as oral pill, one pill-per-day for 1 month | Heat-inactivated plasma from COVID-19 patients | Host immunity development against COVID-19. Exact mechanism to be determined. | To be assessed | [168,169] |
| AV-COVID-19 | Aivita Biomedical, Inc | Phase I/II (NCT04386252) | 180 | Variable | Autologous DC loaded with SARS-CoV-2 antigens | Host immunity development against COVID-19. Exact mechanism to be determined | To be assessed | [170] |
| Inactivated SARS-CoV-2 | Sinovac Research and Development Co., Ltd. | Phase I/II (NCT04352608) | 744 | Medium dose: 600 SU/0.5 mL High Dose: 1200 SU/0.5 mL | Inactivated SARS-CoV-2 virus | Inactivated whole virus yields immunization through producing IgG against viral spike–receptor binding domain | To be assessed | [171] |
| GX-19 | Genexine, Inc. | Phase I/II (NCT04445389) | 210 | Not revealed. (Intramusculary) | DNA vaccine | DNA vaccine which expresses SARS-CoV-2 Spike protein antigen | To be assessed | [172] |
| SARS-CoV-2 rS or NVX-CoV2373 | Novavax | Phase I (NCT04368988) | 131 | 25 μg without Matrix-M, 5 μg with 50 μg Matrix-M | Nanoparticle vaccine with/without Matrix-M adjuvant | Efficient binding with viral targeted receptors. Adjuvant stimulates high levels of neutralizing antibodies | To be assessed | [173,174] |
| bacTRL-Spike | Symvivo Corporation | Phase I (NCT04334980) | 84 | Vaccine formulated as oral pill. Dosage variable | Bacterial vaccine | Bifidobacterium longum delivers synthetic plasmid DNA containing spike protein of SARS-CoV-2 | To be assessed | [175] |
| SCB-2019 | Clover Biopharmaceuticals AUS Pty Ltd. | Phase I (NCT04405908) | 150 | 3–30 μg twice daily (intramuscular) | Recombinant subunit vaccine | Synthesized subunit that resembles viral spike protein induces immunity against spike protein of SARS-CoV-2 | To be assessed | [176,177] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharma, A.; Ahmad Farouk, I.; Lal, S.K. COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention. Viruses 2021, 13, 202. https://doi.org/10.3390/v13020202
Sharma A, Ahmad Farouk I, Lal SK. COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention. Viruses. 2021; 13(2):202. https://doi.org/10.3390/v13020202
Chicago/Turabian StyleSharma, Anshika, Isra Ahmad Farouk, and Sunil Kumar Lal. 2021. "COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention" Viruses 13, no. 2: 202. https://doi.org/10.3390/v13020202
APA StyleSharma, A., Ahmad Farouk, I., & Lal, S. K. (2021). COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention. Viruses, 13(2), 202. https://doi.org/10.3390/v13020202