Abstract
Background: Aging populations make expanded workforce participation among older adults an economic and public health priority. The COVID-19 pandemic accelerated the growth of virtual work, providing new opportunities for healthy aging in the workplace through increased flexibility and less physical strain. However, digital exclusion, ergonomically challenging tasks, and social isolation can limit these opportunities for older populations. Objective: This scoping review aimed to synthesize interdisciplinary research on the relationship between remote work and labor force participation among adults aged 45 years and older, focusing on health-related outcomes, barriers, and facilitators. Methods: Following the JBI Manual for Evidence Synthesis and PRISMA-ScR guidelines, we conducted a comprehensive search across seven databases for peer-reviewed and gray literature published between 2000 and 2025. Of 2108 records screened, 33 studies met the inclusion criteria. Data were extracted using a standardized charting tool and analyzed thematically. Results: Most studies were published after 2020 and originated in North America (45%) and Europe (40%). Core barriers included digital exclusion, ageism, and adverse ergonomic environments. Facilitators involved flexible working hours, a supportive organizational environment, and digital skills. Health-related outcomes such as stress reduction and improved well-being were commonly reported. However, only 18% of studies assessed policy effects, and very few examined intersectionality (e.g., gender, socioeconomic status). Conclusions: Remote and flexible work options can improve the health and participation of older adults in the workforce, but technology, infrastructure, and social barriers remain. Age-inclusive policies, digital equity efforts, and inclusive workplace practices are necessary to maximize the benefits of remote arrangements for aging populations.
1. Introduction
1.1. Background
The global population aged 60 and older is projected to double by 2050, reaching 2.1 billion [1,2]. This increasing demographic presents significant opportunities for the world’s public health system, labor market, and social policies. Encouraging active workforce participation among older adults has become a strategic goal in many countries, aiming to reduce pension burdens, address workforce shortages caused by aging, and prevent social exclusion later in life.
Meanwhile, flexible and remote work arrangements, driven by the COVID-19 pandemic, have changed how work is organized, especially in healthcare, education, and government administration. Older workers can benefit greatly from these setups, as they decrease physical stress, provide more independence, and help them manage illness or caregiving responsibilities. However, remote work can also worsen issues such as digital exclusion, reduced social interaction, and age-based discrimination in workplace technology and culture [3,4,5,6].
These complex dynamics are not well studied, especially among adults aged 45 and older. Although the World Health Organization defines older adults as those 60 or 65 years and above, we use a broader age range (45+) to include transitional midlife periods that are most relevant when examining detachment from the labor market, emerging chronic diseases, and retirement planning. This expanded age group allows for a more comprehensive analysis of the effects of remote work on populations entering or in older adulthood—key groups for preventive labor and health strategies.
Working remotely is also a new factor influencing health. Telework affects physical activity, ergonomic risks, stress, and social opportunities [7,8]. These aspects directly impact health outcomes and future functional abilities. In line with the Ottawa Charter for Health Promotion, creating supportive environments, improving health literacy, and implementing system-level policy changes are vital for advancing well-being throughout life [9]. When poorly executed, remote work can harm health and participation; when well-supported, it can enhance autonomy and resilience. Telework affects physical activity, ergonomic risks, stress, and social opportunities [7,8]. These aspects directly impact health outcomes and future functional abilities. In line with the Ottawa Charter for Health Promotion, creating supportive environments, improving health literacy, and implementing system-level policy changes are vital for advancing well-being throughout life [9]. When poorly executed, remote work can harm health and participation; when well-supported, it can enhance autonomy and resilience.
Furthermore, the United Nations Decade of Healthy Ageing (2021–2030) encourages the development of age-inclusive work practices that enhance both the quality and duration of life [10]. In this context, it is crucial to understand how remote work arrangements impact older adults’ engagement, health, and equity outcomes as we pursue the objectives of public health and labor policy.
To inform our synthesis, we created a conceptual framework (Figure 1) based on established models and existing literature in aging, digital equity, workforce flexibility, and workplace health [11,12,13]. The framework emphasizes barriers (e.g., digital exclusion, ergonomic limitations, ageism) and facilitators (e.g., flexible schedules, access to training, supportive managers) that affect older adults’ experiences with remote work. These elements influence both individual well-being and broader workforce retention trends. To promote healthy and sustainable aging in remote work settings, policy changes, workplace designs, and digital inclusion initiatives are essential tools.
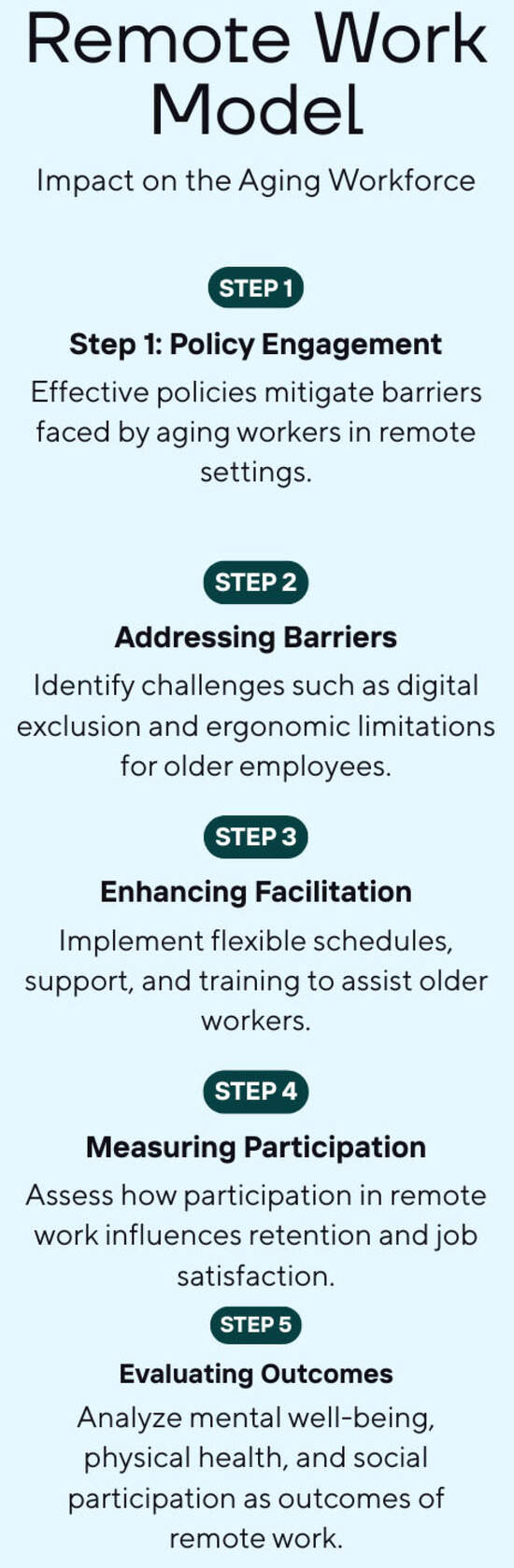
Figure 1.
Conceptual framework illustrating the relationship between remote work and labor force participation among older adults.
The five-step model illustrates theoretical and empirical links discussed in early aging and occupational health literature [3,5,6]. Created using Canva 2.335.1 (Canva Pty Ltd.,110 Kippax Street, Surry Hills, NSW 2010, Australia), the model shows how policy engagement, digital barriers, facilitation, and outcome evaluation interact in remote work settings for adults aged 45 and older.
1.2. Rationale and Research Objectives
Although some research has been carried out on older adults’ experiences with telework, there is no comprehensive evidence that identifies all the barriers, facilitators, and health effects of working from home for this group. Varying definitions, sector differences, and cross-country variations further complicate the evidence base.
To address these gaps, the current scoping review aims to systematically map and synthesize the interdisciplinary literature on the relationship between remote work and labor force participation among adults aged 45 and older. Specifically, it seeks to:
- Identify the main barriers and supports that affect older adults’ participation in remote work and their related well-being outcomes.
- Consider the health promotion opportunities of working remotely in later life, particularly concerning autonomy, ergonomically safe work environments, and social inclusion.
- Develop workplace policies and public programs that promote diverse, inclusive, and age-inclusive virtual work environments.
Addressing the links between public health, labor economics, and gerontology, this review provides new insights for researchers, practitioners, and policymakers aiming to promote healthy aging through fair workforce participation.
2. Methods
This scoping review adhered to the methodological guidelines in the Joanna Briggs Institute (JBI) Manual for Evidence Synthesis [11]. The report was organized according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews, (PRISMA-ScR) [12]. Additionally, we incorporated methodological improvements from Levac et al. [13].
The search was performed in close collaboration with librarians at New York Medical College, who scoped the project, developed and optimized database-specific search strategies, executed and documented searches, and supported reproducibility. The screening and data management process was supported by Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia), enabling independent screening, conflict resolution, and data extraction. Completed PRISMA-ScR Checklist attached (File S4).
2.1. Eligibility Criteria
Eligibility criteria were developed using the Population–Concept–Context (PCC) framework, as recommended for scoping reviews [11].
- Population: Individuals aged 45 and older. The cutoff at 45 years was chosen to reflect midlife changes relevant to workforce engagement and aligns with life-course perspectives in the literature on labor and aging.
- Concept: Flexible, hybrid, or remote work options such as telework, virtual work, working from home, or telecommuting.
- Context: Throughout the world, across all occupations, sectors, and income levels.
- Inclusion Criteria: Studies were eligible if they:
- Were published between January 2000 and May 2025.
- Included peer-reviewed or gray literature (e.g., government reports, dissertations).
- Employed any study design (qualitative, quantitative, or mixed methods).
- Reported among adults aged 45 and older on at least one of the following:
- o
- Labor force participation;
- o
- Employment or retirement outcomes;
- o
- Job satisfaction;
- o
- Physical or mental health;
- o
- Inclusion or exclusion from workplace practices.
- Exclusion Criteria: Studies were excluded if they:
- Did not report age-specific findings.
- Did not specify remote or flexible work contexts.
- Focused exclusively on interventions unrelated to labor force participation or work settings.
2.2. Search Strategy
The databases searched were the seven largest academic databases:
- MEDLINE (Ovid).
- EMBASE.
- Scopus.
- CINAHL (EBSCOHost).
- AgeLine (EBSCOHost).
- PsycINFO (EBSCOHost).
- EconLit.
Combined searches of MeSH, Emtree, and keyword terms such as aging, older workers, working remotely, flexible schedules, and labor participation. Boolean operators (AND, OR), truncation (*), and proximity operators (e.g., NEAR, adj, PRE/W) were used together to enhance both precision and sensitivity. Full search strategies are available in Supplementary File S1.
The searches were limited to English-language publications and supplemented with citation chaining and targeted gray literature searches.
2.3. Search Results
A total of 2108 records were identified: 2098 through databases and 10 through citation searching. After removing 369 duplicates, 1739 unique records were screened based on titles and abstracts; 1646 were excluded, and 93 were assessed in full. Sixty studies were excluded for reasons such as wrong indication (n = 49), intervention (n = 8), setting (n = 1), population (n = 1), or research question misalignment (n = 1). The remaining 33 studies met all inclusion criteria and were included in the final synthesis.
The selection process is illustrated in Figure 2 (PRISMA 2020 flow diagram).
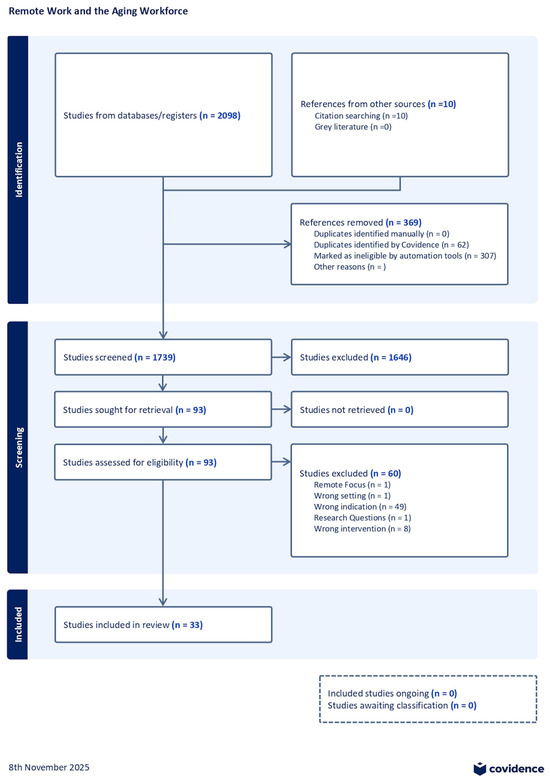
Figure 2.
A PRISMA flow diagram presents the screening process and the number of studies included/excluded at each stage (Supplementary File S1).
2.4. Study Selection Process
Extraction was carried out using [K.A.] and [T.K.], and manually checked by [M.S.] for consistency.
Study selection was performed using the Covidence software in a three-step screening process:
- Title and Abstract Screening: Carried out by three reviewers individually.
- Full-Text Review: Full-text articles that satisfied the initial inclusion criteria were reviewed against the full criteria.
- Discrepancy Resolution: Differences were settled by discussion or by a third reviewer.
Reviewer Agreement and Discrepancies Resolution
- 116/1739 records (6.7%) needed reconciliation at the title/abstract level.
- 12/93 articles (12.9%) needed discussion at full-text review to reach consensus.
Inter-rater reliability was assessed for both the title/abstract and full-text screening. Agreement was high, with Cohen’s κ = 0.82 for title/abstract screening and κ = 0.79 for full-text screening, indicating substantial reliability between reviewers.
All disagreements were resolved through reviewer deliberation and, when an initial agreement was not reached, by consensus or referral to a third reviewer. These results indicate strong consensus, enhancing the reliability and transparency of the reviews.
2.5. Data Extraction and Charting
A standardized form for charting the data (see Supplementary Files S2 and S3) was created to abstract the following variables:
- Bibliographic details (author, year, country).
- Study design and method.
- Participant characteristics (age range, gender, job type).
- Remote work arrangement (telework, hybrid, flexible, etc.).
- Health or labor outcomes (e.g., well-being, inclusion, job satisfaction, retirement intentions).
- Identified barriers and facilitators.
- Policy or practice implications.
Data extraction was performed independently by several reviewers to establish reliability (Table 1 and Table 2). Descriptive statistics (e.g., frequencies and proportions of theme extraction) were generated in Stata 18 (StataCorp LLC, College Station, TX, USA) to assess thematic patterns across the included studies. These findings are tabulated (Figure 3).

Table 1.
Summary of extraction.
Table 2.
Geographic distribution of included studies (n = 33).
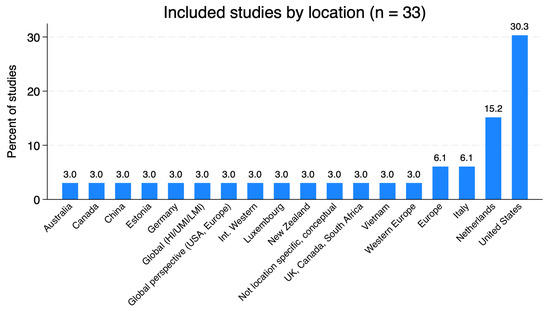
Figure 3.
Geographic distribution of studies included in the review. Geographic distribution of included studies (n = 33) was generated using Stata 18 (StataCorp LLC, College Station, TX, USA). Bars show the percentage of included studies conducted in each country or region. “Global (HI/UMI/LMI)” denotes a multi-country study across high-, upper-middle- and lower-middle-income settings; “International Western” and “Western Europe” denote multi-country studies focused on Western, high-income contexts; “UK, Canada, South Africa” represents a single multi-country study; “Not location specific, conceptual” refers to a conceptual paper without a defined empirical setting. See Table 2 for underlying counts and percentages by country/region.
2.6. Data Synthesis
The synthesis used a descriptive and thematic approach:
- Quantitative summary: The studies were summarized according to year, country, sector, design, and type of remote work.
- Thematic analysis: Key themes were derived related to:
- Barriers (e.g., digital exclusion, ageism, ergonomic risks);
- Facilitators (e.g., autonomy, training support, flexibility);
- Health promotion outcomes (e.g., mental health, well-being, and social participation).
Themes were organized in alignment with health promotion frameworks such as the Ottawa Charter for Health Promotion [9], which guided the interpretation of findings in terms of enabling environments, personal skills development, and supportive policies.
3. Results
3.1. Study Selection
A total of 2108 records were identified through database searches and citation chaining. Of these, 369 duplicates were removed. Then, 1739 records were screened based on title and abstract, and 93 were reviewed in full. Ultimately, 33 studies met the inclusion criteria (Figure 2).
3.2. Characteristics of Included Studies
The 33 studies, conducted between 2002 and 2025, covered diverse regions and research methods, focusing on remote or flexible work among adults aged 45 and older. Most took place in high-income countries such as the United States, Canada, and European nations, while one study in Vietnam provided an LMIC perspective. Methodologically, 15 studies were quantitative, 11 qualitative, 3 used mixed methods, 3 were conceptual reviews, and 1 was a systematic review. The populations studied varied, including contract workers [14], healthcare workers, teachers, and government employees, with focuses ranging from job performance to health and retirement transitions. European studies highlighted policy frameworks and digital infrastructure, whereas U.S. studies more often emphasized individual liberty and caregiving conflicts. A summary of the study designs and settings is available in Table 2 and Supplementary File S3.
Table 3 summarizes the characteristics, contexts, and findings of the 33 reviewed studies. An abridged version is shown for illustration; the whole table is available in Supplementary File S4 via OSF at https://doi.org/10.17605/OSF.IO/B6H7C. https://osf.io/tdgsv (accessed on 23 September 2025).
Table 3.
Summary of Reviewed Studies on Remote Work and Older Adults.
This methodological diversity reflects a balanced representation of empirical, theoretical, and policy-oriented perspectives on remote work and aging.
The population samples primarily comprised individuals aged 45 years and above, with subgroups including caregivers, teaching and healthcare professionals, government servants, and those based in specific geographic areas (Figure 3). The remote work arrangements explored included fully remote, hybrid, and flexible options.
Figure 3: This pie chart displays the geographic distribution of the 33 included studies. The United States accounts for the largest share, followed by Europe, North America, and a mix of global or unspecified locations.
3.3. Theme Coverage Across Studies
The coder coded studies for four major thematic areas: facilitators, barriers, policy implications, and health and labor outcomes. Text-based records were coded, and any incidence of descriptive data in the theme column was treated as a mention. The blank rows were assumed to indicate a lack of thematic discourse. Table 3 presents a quantitative summary.
Table 4: This table shows the percentage of studies (out of 33) that addressed each central theme. Barriers and facilitators were the most reported, followed closely by outcomes and policy implications.
Table 4.
Prevalence of Themes Among the 33 Included Studies.
Interpretation
Barriers and facilitators were the most consistently prominent themes, appearing in more than 90% of studies. This suggests a strong orientation toward identifying the structure and individual-level challenges and enablers in remote work for older adults. While the results and policymaking implications were also quite common (approximately 85% of the studies), a small proportion of studies were conceptual or theoretical and did not yield actionable results or policy implications.
3.4. Barriers
Barriers to remote work were multidisciplinary, covering digital, organizational, and psychosocial areas. Precarious contract workers experienced greater insecurity and fewer benefits than regular employees [14]. Psychological distress from sudden telework changes during the COVID-19 lockdown was common among older adults [15]. Inadequate ergonomics and technical issues limited satisfaction and well-being [16], while unclear expectations and increased workload reduced productivity [17].
Inflexible HR practices and a lack of personalized accommodations restricted older workers’ flexibility [18]. Organized workplace support was not always transformed into well-being, especially when relational bonds were weak [19]. Cognitive decline, digital gaps, and systemic discrimination were identified as overlooked aging factors in telework in broader reviews [20]. Gender disparities in workplace flexibility persisted, putting older women at a disadvantage [21]. Digital and social exclusion created compounded risks for individuals with limited networks or digital exposure [22].
Low digital confidence and technology anxiety limited participation, highlighting the need for formal digital training [23]. Blended or hybrid models were not always beneficial—older adults struggled with transitioning from in-person to remote roles [24]. In Germany, health-related employment restrictions reduced participation in flexible work arrangements [25]. Cross-age comparisons revealed that satisfaction with remote work heavily depended on trust in the employer and clear role definitions [26,27]. Systematic reviews found that poor workplace control and social isolation negatively affected mental and physical health [28,29]: limited digital skills and inconsistent managerial communication contributed to long-term inequalities [30,31].
Below is a cross-study comparison (Table 5) that summarizes the significant barriers and facilitators reported across the 33 included studies. Each category was derived by grouping similar themes from the extraction data; the “Number of studies” column indicates how many studies mentioned each category (out of 33).
Table 5.
Barriers to Remote Work Among Older Adults.
Table 4: The most frequently reported barrier was digital exclusion, reflecting inadequate access to technology and skills among older adults. Ageism and employer bias were also common, indicating persistent stereotypes about older workers’ adaptability and a lack of supportive HR practices. Health limitations, cognitive strain, and structural and policy constraints further restricted older workers’ ability to engage in remote work.
3.5. Facilitators
Facilitators of autonomy, trust, and organizational culture include flexible schedules and phased retirements, which enabled older adults to continue participating [32]. Early research showed that telework could extend employability when supported by psychological and ergonomic measures [33]. Later studies found that formal digital onboarding increased satisfaction and inclusion among new and returning employees [34].
Federal agency telework programs showed increased retention when combined with flexible management and ergonomically designed tools [35]. The Vietnam case revealed that telework eased the decline in employment for some, while for others it worsened inequality based on connectivity levels and education [36]. Age-based boundary management tactics, such as separating work and home, were linked to productivity gains and better work–life balance [37].
Employer discretion in responding to aging workforces, such as through mentoring and flexible pensions plans, boosts retention and reduces turnover [38]. Infrastructure gaps in digital technology, especially in the public sector, restrict fair and equal opportunities for remote work [39]. Research linking flexibility to health shows improved well-being when organizational environments are supportive [40]. Smart use of intelligent technology decreased fatigue and increased satisfaction among older teleworkers [41].
Technology-supported ergonomic settings, such as ambient-assisted working systems, and augmented functional independence [42]. Positive attitudes toward technology and age-related cognitive adaptability help overcome age-based barriers to remote work [43]. Flexible work arrangements and organizational climates that foster trust improve health and productivity outcomes [44]. Virtual workplaces that emphasize self-efficacy and mentoring support “successful aging at work” [45]. Finally, integrating international HR standards and ethical considerations in technology enhances the long-term sustainability of an aging workforce [46].
Below is a cross-study comparison (Table 4) summarizing the significant barriers and facilitators reported across the 33 included studies. Each category was created by grouping similar themes from the extracted data; the “Number of studies” column shows how many studies mentioned each category (out of 33).
Table 6: The most common facilitators were flexible scheduling and a strong sense of community at work, both of which help older workers balance personal needs with professional demands. Digital upskilling programs and personalized job arrangements (Ideals) assist older adults in overcoming technology barriers and staying engaged [18]. Supportive organizational and policy environments, including phased retirement options, ergonomic adjustments, and inclusive leadership, also foster healthy and sustained participation in remote work.
Table 6.
Facilitators of Remote Work Among Older Adults.
3.6. Health and Labor Force Participation Outcomes
Health effects varied depending on the environment. Flexible and hybrid setups reduced commuting stress and enhanced mental health [14,16,19,25]. Conversely, technostress, social isolation, and boundary blurring increased cognitive fatigue and loneliness [15,22,27,29]. Workplace health benefits were most significant when both ergonomics and psychosocial supports were in place [40,41].
Labor participation trends showed delayed retirement and increased staying in caregiving and knowledge jobs [24,31,32]. Meanwhile, informal workers and women faced layered exclusion due to caregiving responsibilities and digital gaps [21,36]. Research reaffirmed the link between supportive policies, mentoring, and digital upskilling to support longer, healthier working lives [18,23,34,45].
3.7. Policy and Practice Implications
The evidence from the 33 studies shows that the success of remote work among older adults depends on equitable design. Organizations should provide personalized flexibility (“i-deals”) [18,32], digital training [23,30], ergonomic support [16,25], and age-inclusive mentoring [34,37]. Policymakers must expand digital infrastructure, protect informal workers, and redesign pension systems to support hybrid models [36,38,44]. Including international HR standards and responsible AI practices offers a way to sustain aging workforces in the long term [42,46].
These strategies encompassed the five areas of action outlined in the Ottawa Charter (Figure 4).
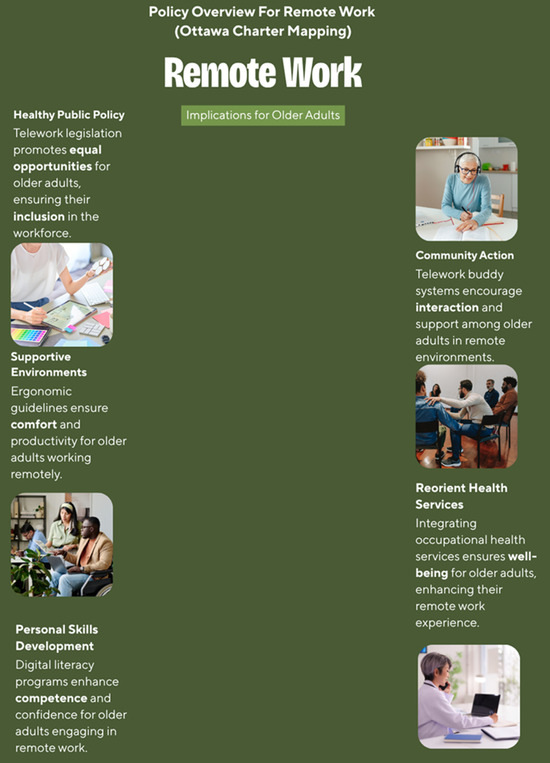
Figure 4.
Policy Implications for Remote Work (Ottawa Charter Mapping), Infographic created using Canva (Canva Pty Ltd., 110 Kippax St, Surry Hills, NSW 2010, Australia).
This diagram places “Remote Work for Older Adults” at the center and illustrates how recommended interventions align with the Charter’s action areas: building healthy public policy (telework legislation, age-sensitive incentives, digital equity); creating supportive environments (ergonomic guidelines, inclusive leadership, work–life boundaries); strengthening community action (telework buddy systems, peer and mentoring support, cross-generational learning); developing personal skills (digital literacy/upskilling, health programs, chronic-disease management); and reorienting health services (integration of occupational and mental health, telehealth and screenings, social insurance and counseling). The improved layout and consistent colors aim to present these relationships more clearly and professionally.
4. Discussion
4.1. Summary of Evidence
This review concludes that home-based work offers both structural potential and psychosocial risks for older workers. While flexible arrangements can support health and workforce retention, the distribution of benefits is uneven. Without strong policies and digital infrastructure, home-based work may lead to exclusion that worsens with age, especially among older workers with caregiving duties, chronic illnesses, or limited digital access [14,15,16,17,47]. Results should be viewed in light of the changing nature of home-based work. Studies from the early 2000s saw telework as the exception [18,20], whereas research after 2020 reflects more normalized arrangements, often imposed by regimes [48,49].
Telecommuting encourages continuous participation by reducing physical stress and helping older workers stay productive [14,17,47]. Despite these benefits, digital divides, limited institutional support, and ongoing ageism can weaken these advantages [16,22,48]. Organizational preparedness and inclusive HR practices, such as personalized flexibility agreements (i-deals) [18], technical assistance, ergonomic solutions [23], and age-inclusive management, are crucial to ensure remote work is empowering rather than exclusionary [19,21,45]. Without these support mechanisms, telecommuting may reinforce exclusion through information gaps, fewer mentorship opportunities, and technology-related disparities [22,48,50]. When executed well, remote work can enhance workforce participation, reduce healthcare costs, and increase economic productivity [17,24,49].
Older workers have stability, experience, and mentoring in increasingly fluid labor markets. They benefit GDP growth, reduce the pension burden, and promote intergenerational equity in the labor force.
4.2. Health Promotion Implications
The review highlights a gendered pattern. Working remotely can support older workers’ caregiving expectations, especially among older women, as working from home often overlaps with family caregiving, increasing unpaid labor and reinforcing traditional gender roles [47,51,52]. The combined influence of age, gender, and caregiving expectations underscores an urgent need for future research in occupational health. Remote work’s potential to reduce stress and enhance autonomy aligns with the Ottawa Charter’s emphasis on creating a supportive environment for stress reduction [9]. Flexible work options decrease commuting-related stress and improve work–life balance [19,24,27]. However, autonomy in remote work depends on proper ergonomics, digital literacy, and flexible management. Without these, telework can cause psychosocial stress instead of fostering empowerment [29,30,41]. Low-quality home environments and digital eye strain contribute to cognitive overload, while reduced social contact increases loneliness risk [22,29,52]. Therefore, the health benefits of telework depend on an individual’s capabilities and the adequacy of workplace infrastructure.
When properly supported, telework can extend working life, improve mental health, and enhance inclusion [14,19,27]. These benefits align with the WHO Decade of Healthy Ageing framework, which promotes environments that support older adults [48]. However, in settings where digital literacy is low or management is unsupportive, working from home or the office can widen inequality, particularly for people with long-term conditions [47,53].
4.3. Policy and Practice Relevance
Policies must consider the diversity of older workers. Age-friendly home-based work is not just about participation but also about removing structural barriers that prevent it—such as digital exclusion, inflexible pension systems, and deeply rooted workplace age discrimination [14,18,45,53]. A life-course approach is crucial, since digitalization affects different cohorts in different ways [50,51].
Organizational-level inclusive HR practices such as ICT-based onboarding, mentoring, and leader–employee participation have proven useful [18,23,34,40]. At the systemic level, restructuring labor and disability evaluation systems remains essential. For example, Italy’s OECD review highlighted the fragmentation of its disability evaluation system, which left many qualified older workers uncovered; using function-based tools such as the WHO Disability Assessment Schedule (WHODAS) can help improve inclusion [53].
Digitalization presents both opportunities and challenges. It enables flexible work arrangements and longer careers but demands lifelong learning and adaptability to technology [50,51]. Technology can empower as well as exclude, unless deliberate interventions are implemented [22,28,51]. Key enabling factors include flexible schedules, gradual retirements [19,24], digital upskilling [31], inclusive workplace cultures [18,23,34], and autonomy in team structures [53].
From this synthesis, several policy recommendations emerge:
- Digital inclusion: Governments and employers should provide targeted digital literacy programs, ergonomically designed tools, and reliable internet access [48,50].
- Anti-ageism measures: Recruitment, advancement, and preservation procedures should address stereotypes and include inclusive teachings [16,18].
- Pension modernization: Pension plans should support hybrid and part-time telework without reducing benefits for older workers [49].
- Health-adaptive job design: Work environments can incorporate ergonomic and psychosocial adaptations for older workers [47,54].
Successful policies balance personalized adaptability with organizational responsibility, ensuring that digital literacy, ergonomics support, and fairness are fundamental, not optional.
These recommendations align with ISO 25550:2022, the international standard for age-inclusive workforce policies, which assesses flexible workforce arrangements, technology access, and age-sensitive HR practices as vital for older workers [55].
4.4. Research Gaps
Despite years of research, age-specific evidence remains limited outside high-income regions [47,48,53]. No studies including data from the Middle East or Sub-Saharan Africa were identified. Future research should focus on low- and middle-income settings where the informal economy and weaker digital infrastructure create unique challenges [51]. Variables such as gender, education, disability, and caregiving were reported inconsistently [47,50,51,52]. Older women, in particular, are often underrepresented despite facing dual caregiving and workforce duties [52]. This underrepresentation limits the ability of existing studies to inform equitable policies. Methodologically, most studies are cross-sectional and rely on self-reported proxies, such as satisfaction, rather than on health indicators [14,22,27]. Prospective and mixed-method research could help establish causal relationships among remote work, health, and labor participation. Expanding coverage to underrepresented regions and occupations would make telework policies more applicable globally [48,49,50,51].
4.5. Strengths and Limitations
The broad time span (2000–2025) allowed this review to incorporate evolving perspectives on remote work, from early pilot studies to post-pandemic normalization [18,48]. Its transdisciplinary approach, based on JBI and PRISMA-ScR templates [11,12,13], improves reliability. However, as a scoping review, no formal quality assessment was conducted, and variability in study design and outcomes makes direct comparisons difficult [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,53]. Many studies focused on intermediate rather than clinical health outcomes, which limits causal inference. Additionally, technological and policy changes over 25 years introduce contextual variability. Despite these challenges, consistent patterns emerged across disciplines, highlighting digital inclusion, workplace flexibility, and intergenerational equity as key elements of healthy aging in the future of work.
5. Conclusions
This scoping review demonstrates an urgent imperative to redefine flexible and remote work as a long-term solution for advancing healthy, inclusive, and productive aging at the workplace. Based on 33 studies mainly in high-income and international settings, the current evidence indicates that flexible working can contribute to greater autonomy, reduced physical stress, and improved work–life integration, particularly among older workers with chronic illness or caregiving obligations.
However, these benefits are not guaranteed. Without intentional investment in digital infrastructure, age-friendly technologies, and inclusive workplace policies, remote work can reinforce exclusion, widen digital divides, and increase inequalities, especially among workers with limited digital skills, disabilities, or informal employment.
Telework is not a neutral practice; its outcomes depend on the quality of technological access, leadership culture, and policy design. Persistent barriers, such as ageist attitudes, rigid pension systems, and inadequate training, continue to block equal participation. Employers and policymakers must respond proactively by expanding digital literacy programs, subsidizing connectivity costs and equipment, and incorporating anti-ageism measures into organizational and legal frameworks. Reforms in pensions, employment, and social care also need to support flexible, late-life work.
Economically, it helps older adults keep rural or hybrid jobs by increasing workforce resilience, reducing healthcare costs, and leveraging extensive experience, supported by both the WHO Decade of Healthy Ageing and the Ottawa Charter for Health Promotion. However, significant research gaps still exist, especially in low- and middle-income countries, and regarding intersectional issues such as gender, disability, and rurality.
Ultimately, telework can promote healthy and fair aging only when guided by intentional, evidence-based, and inclusive strategies. For employers, policymakers, and researchers, this presents both a responsibility and a chance to reshape the future of work, rooted in dignity, health, and intergenerational fairness.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph22111719/s1. File S1: Full Search Strategy. File S2: Covidence Screening Documentation. File S3: Data Extraction Sheet. File S4: Completed PRISMA-ScR Checklist. All supplementary files and documentation related to this scoping review have been archived and made openly accessible via the Open Science Framework (OSF): https://osf.io/tdgsv (accessed on 23 September 2025). https://doi.org/10.17605/OSF.IO/B6H7C (accessed on 23 September 2025).
Author Contributions
Conceptualization, K.A.K. and M.G.; methodology, T.K. and M.S.; validation, K.A., T.K. and M.G.; formal analysis, M.S. and T.K.; investigation, M.S., T.K. and K.A.; data curation, K.A., M.S. and A.M.S.; writing—original draft preparation, K.A.; writing—review and editing, M.G., K.A.K., T.K. and M.S.; visualization, M.S. and A.M.S.; supervision, K.A.K. and M.G.; project administration, K.A.; Funding Acquisition, M.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable. This study did not involve human or animal subjects, and no new data were collected.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing was not performed in this study.
Acknowledgments
We would like to thank Marie T. Ascher New York Medical College, for substantive contributions to search design, execution, and documentation. We also thank Rosa O. Rodriguez, a student at New York Medical College, for her thoughtful review and constructive suggestions, which helped improve the quality and clarity of this manuscript.
Conflicts of Interest
The authors have no affiliation or financial involvement with any institution or organization that might have a financial interest in the topics or materials presented in this manuscript.
References
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2020 Highlights. Available online: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/undesa_pd-2020_world_population_ageing_highlights.pdf (accessed on 11 August 2025).
- World Health Organization. Decade of Healthy Ageing: Baseline Report; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/9789240017900 (accessed on 11 August 2025).
- Eurofound; International Labour Office. Working Anytime, Anywhere: The Effects on the World of Work; Publications Office of the European Union: Luxembourg; International Labour Office: Geneva, Switzerland, 2017; Available online: https://www.eurofound.europa.eu/en/publications/all/working-anytime-anywhere-effects-world-work (accessed on 11 August 2025).
- Eurofound. Living, Working and COVID-19. 2021. Available online: https://www.eurofound.europa.eu/en/publications/2021/living-working-and-covid-19-update-april-2021-mental-health-and-trust-decline (accessed on 11 August 2025).
- Neves, B.B.; Amaro, F. Too old for technology? How the elderly of Lisbon use and perceive ICT. J. Community Inform. 2012, 8. [Google Scholar] [CrossRef]
- Van der Lippe, T.; Lippényi, Z. Co-workers working from home and individual and team performance. New Technol. Work Employ. 2020, 35, 60–79. [Google Scholar] [CrossRef] [PubMed]
- Mann, S.; Holdsworth, L. The psychological impact of teleworking: Stress, emotions and health. New Technol. Work Employ. 2003, 18, 196–211. [Google Scholar] [CrossRef]
- Vyas, L.; Butakhieo, N. The impact of working from home during COVID-19 on work and life domains: An exploratory study on Hong Kong. Policy Des. Pract. 2021, 4, 59–76. [Google Scholar] [CrossRef]
- World Health Organization. Ottawa Charter for Health Promotion; WHO: Geneva, Switzerland, 1986; Available online: https://www.who.int/publications/i/item/ottawa-charter-for-health-promotion (accessed on 11 August 2025).
- Keating, N. A research framework for the United Nations Decade of Healthy Ageing (2021–2030). Eur. J. Ageing 2022, 19, 775–787. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews (2020 version). In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2020; pp. 406–451. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Abraham, K.G.; Hershbein, B.; Houseman, S.N. Contract work at older ages. J. Pension Econ. Financ. 2021, 20, 426–447. [Google Scholar] [CrossRef]
- Andreassi, S.; Monaco, S.; Salvatore, S.; Sciabica, G.M.; De Felice, G.; Petrovska, E.; Mariani, R. To Work or Not to Work, That Is the Question: The Psychological Impact of the First COVID-19 Lockdown. Healthcare 2021, 9, 1754. [Google Scholar] [CrossRef]
- Arvola, R.; Tint, P.; Kristjuhan, Ü.; Siirak, V. Impact of telework on the perceived work environment of older workers. Sci. Ann. Econ. Bus. 2017, 64, 199–214. [Google Scholar] [CrossRef]
- Beekman, E.M.; Van Hooff, M.M.L.; Adiasto, K.; Claessens, B.J.C.; Van der Heijden, B.I.J.M. Is This (Tele)working? A path model analysis of the relationship between telework, job demands and job resources, and sustainable employability. Work (Read. Mass.) 2025, 80, 295–313. [Google Scholar] [CrossRef]
- Bal, P.M.; Jansen, P.G.W. Idiosyncratic deals for older workers. In Aging Workers and the Employee-Employer Relationship; Bal, P.M., Ed.; Springer: Cham, Switzerland, 2014; pp. 129–144. [Google Scholar] [CrossRef]
- Buonomo, I.; Ferrara, B.; Pansini, M.; Benevene, P. Job Satisfaction and Perceived Structural Support. Int. J. Environ. Res. Public Health 2023, 20, 6205. [Google Scholar] [CrossRef]
- Czaja, S.J.; Sharit, J. Aging and Work: Issues and Implications in a Changing Landscape; Johns Hopkins University Press: Baltimore, MD, USA, 2009; pp. 1–320. [Google Scholar]
- Damman, M.; Henkens, K. Gender differences in workplace flexibility among older workers. J. Appl. Gerontol. 2020, 39, 915–921. [Google Scholar] [CrossRef]
- Seifert, A.; Cotten, S.R.; Xie, B. A double burden of exclusion? Digital and social exclusion of older adults in times of COVID-19. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e99–e103. [Google Scholar] [CrossRef]
- Dijkstra, K. Future work skills for older workers. Gerontechnology 2024, 23, 1. [Google Scholar] [CrossRef]
- Dropkin, J.; Moline, J.; Kim, H.; Gold, J.E. Blended Work as a Bridge Between Traditional Workplace Employment and Retirement: A Conceptual Review. Work Aging Retire. 2016, 4, 373–383. [Google Scholar] [CrossRef]
- Fechter, C. The role of health in flexible working arrangements in Germany. Z. Für Gerontol. Und Geriatr. 2020, 53, 334–339. [Google Scholar] [CrossRef]
- Francis-Levin, J.; Webster, N.J.; Brauer, S.G.; Armstrong, T.J.; Antonucci, T.C. Experiences and contexts of remote work among older, mid-life and young adults: The case for age-specific remote work interventions. Gerontechnology 2024, 23, 1. [Google Scholar] [CrossRef]
- Oakman, J.; Kinsman, N.; Stuckey, R.; Graham, M.; Weale, V. A rapid review of mental and physical health effects of working at home. BMC Public Health 2020, 20, 1825. [Google Scholar] [CrossRef]
- Chen, M.K.L.; Gardiner, E. Supporting older workers to work: A systematic review. Pers. Rev. 2019, 48, 1318–1335. [Google Scholar] [CrossRef]
- Hamouche, S.; Parent-Lamarche, A. Teleworkers’ job performance: A study examining the role of age as an important diversity component of companies’ workforce. J. Organ. Eff. 2023, 10, 293–311. [Google Scholar] [CrossRef]
- Hauret, L.; Martin, L.; Poussing, N. Teleworkers’ digital up-skilling: Evidence from the spring 2020 lockdown. Inf. Soc. 2024, 40, 215–231. [Google Scholar] [CrossRef]
- Koreshi, S.Y.; Alpass, F. Understanding the use of Flexible Work Arrangements Among Older New Zealand Caregivers. J. Appl. Gerontol. 2023, 42, 1045–1055. [Google Scholar] [CrossRef]
- Johnson, R.W. Phased Retirement and Workplace Flexibility for Older Adults: Opportunities and Challenges. Ann. Am. Acad. Political Soc. Sci. 2011, 638, 68–85. [Google Scholar] [CrossRef]
- Patrickson, M. Teleworking: Potential employment opportunities for older workers? Int. J. Manpow. 2002, 23, 704–715. [Google Scholar] [CrossRef]
- Park, S.; Chaudhuri, S.; Johnson, K.R. Engaging new hires in remote environments. Eur. J. Train. Dev. 2025. ahead-of-print. [Google Scholar] [CrossRef]
- Hunter, L.Y.; Ginn, M.; Meares, W.L.; Hatcher, W. Telework and Work Flexibility in the United States Federal Government Post-Pandemic. Public Adm. Q. 2024, 48, 149–161. [Google Scholar] [CrossRef]
- Phuong, T.T.; Sukontamarn, P. Effect of the COVID-19 pandemic on the employment and income of older workers in Vietnam. Asian Soc. Work. Policy Rev. 2024, 18, e12307. [Google Scholar] [CrossRef]
- Scheibe, S.; Retzlaff, L.; Hommelhoff, S.; Schmitt, A. Age-related differences in the use of boundary management tactics when teleworking: Implications for productivity and work-life balance. J. Occup. Organ. Psychol. 2024, 97, 1330–1352. [Google Scholar] [CrossRef]
- Oude Mulders, J.; Henkens, K.; van Dalen, H.P. How Do Employers Respond to Aging Workforce? In Trends in Aging and Work; Springer: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Kim, J. Pandemic-Induced Telework Divide of Federal Workforces. Public Pers. Manag. 2024, 53, 36–60. [Google Scholar] [CrossRef]
- Shifrin, N.V.; Michel, J.S. Flexible work arrangements and employee health: A meta-analytic review. Work Stress 2021, 36, 60–85. [Google Scholar] [CrossRef]
- Zhao, H.; Xie, H. Workplace Intelligent Technology Use and Health of Older Remote Workers. J. Occup. Environ. Med. 2025, 67, 469–476. [Google Scholar] [CrossRef]
- Spoladore, D.; Trombetta, A. Ambient Assisted Working Solutions for the Ageing Workforce: A Literature Review. Electronics 2023, 12, 101. [Google Scholar] [CrossRef]
- Foster-Thompson, L.; Mayhorn, C.B. Aging Workers and Technology. In The Oxford Handbook of Work and Aging; Hedge, J.W., Borman, W.C., Eds.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar] [CrossRef]
- Vanajan, A.; Bültmann, U.; Henkens, K. Health-related Work Limitations Among Older Workers—The Role of Flexible Work Arrangements and Organizational Climate. Gerontologist 2019, 60, 450–459. [Google Scholar] [CrossRef]
- Wang, C.; Zhang, Y.; Feng, J. How do older employees achieve successful ageing at work through generativity in the digital workplace? A self-affirmation perspective. J. Occup. Organ. Psychol. 2024, 97, 1475–1501. [Google Scholar] [CrossRef]
- Wissemann, M.; Pit, S.; Serafin, P.; Gebhardt, H. Strategic Guidance and Technological Solutions for Human Resources Management to Sustain an Aging Workforce: Review of International Standards, Research, and Use Cases. JMIR Hum. Factors 2022, 9, e27250. [Google Scholar] [CrossRef]
- Koolhaas, W.; van der Klink, J.J.; de Boer, M.R.; Groothoff, J.W.; Brouwer, S. Chronic health conditions and work ability in the ageing workforce: The impact of work conditions, psychosocial factors and perceived health. Int. Arch. Occup. Environ. Health 2014, 87, 433–443. [Google Scholar] [CrossRef]
- International Labour Organization. Teleworking During the COVID-19 Pandemic and Beyond: A Practical Guide; International Labour Organization: Geneva, Switzerland, 2020; Available online: https://www.ilo.org/sites/default/files/wcmsp5/groups/public/@europe/@ro-geneva/@ilo-paris/documents/meetingdocument/wcms_767510.pdf (accessed on 11 August 2025).
- Bureau of Labor Statistics. The rise in remote work since the pandemic and its impact on productivity. Beyond Numbers 2024, 13, 1–4. Available online: https://www.bls.gov/opub/btn/volume-13/remote-work-productivity.htm (accessed on 15 August 2025).
- Komp-Leukkunen, K. A Life-Course Perspective on Older Workers in Workplaces Undergoing Transformative Digitalization. Gerontologist 2023, 63, 1413–1418. [Google Scholar] [CrossRef]
- Piroșcă, G.I.; Șerban-Oprescu, G.L.; Badea, L.; Stanef-Puică, M.-R.; Valdebenito, C.R. Digitalization and Labor Market—A Perspective within the Framework of Pandemic Crisis. J. Theor. Appl. Electron. Commer. Res. 2021, 16, 2843–2857. [Google Scholar] [CrossRef]
- Money, A.; Hall, A.; Harris, D.; Eost-Telling, C.; McDermott, J.; Todd, C. Barriers to and facilitators of older people’s engagement with web-based services: Qualitative study of adults aged > 75 years. JMIR Aging 2024, 7, e46522. [Google Scholar] [CrossRef]
- OECD. Disability, Work and Inclusion in Italy: Better Assessment for Better Support; OECD Publishing: Paris, France, 2023. [Google Scholar] [CrossRef]
- Sharit, J.; Czaja, S.J.; Hernandez, M.A.; Nair, S.N. The Employability of Older Workers as Teleworkers: An Appraisal of Issues and an Empirical Study. Hum. Factors Ergon. Manuf. Serv. Ind. 2009, 19, 457–477. [Google Scholar] [CrossRef]
- ISO 25550:2022; Ageing Societies: General Requirements and Guidelines for an Age-Inclusive Workforce; 1st ed. International Organization for Standardization (ISO): Geneva, Switzerland, 2022. Available online: https://www.iso.org/obp/ui/en/#iso:std:iso:25550:ed-1:v1:en (accessed on 19 October 2025).




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).