Abstract
Childhood immunization is one of the most effective public health measures, yet inequities remain in marginalized populations across Asia, where parental adherence is essential to sustaining the Expanded Program on Immunization. This narrative review examines determinants of adherence among under-five children in disadvantaged communities. Following PRISMA guidelines, searches of PubMed, Scopus, and Google Scholar identified studies published between 2015 and 2025, with earlier key works included as relevant. Twenty-one studies from South, Southeast, and East Asia were analyzed. Five domains were associated with adherence: socioeconomic and access factors, where maternal education, household income, and possession of immunization cards were positive predictors, while remote residence was a barrier; trust, cultural beliefs, and social norms, with misinformation and vaccine controversies reducing uptake, and provider trust and supportive norms improving it; migration and mobility, as migrant, stateless, and left-behind children had lower coverage due to weak registration and disrupted caregiving; household and caregiver dynamics, where decision-making by family or community members shaped uptake, while large family size and maternal employment limited adherence; and health system capacity, with inadequate infrastructure and follow-up hindering coverage and integration with maternal–child health services facilitating it. Addressing these intersecting barriers through equity-focused strategies is critical to achieving universal immunization coverage.
1. Introduction
Childhood immunization is one of the most effective public health interventions for reducing morbidity and mortality from vaccine-preventable diseases (VPDs) [1]. Despite global efforts through programs like the World Health Organization’s Expanded Program on Immunization (EPI), disparities in vaccine uptake persist [2]—particularly among marginalized populations in Asia. These populations often live in geographically remote, socioeconomically disadvantaged, or politically marginalized contexts, compounding barriers to immunization access and adherence [3]. Marginalized groups in Asia include slum communities under overcrowding, informal housing, poor sanitation, and limited public services.Haor communities in the wetland areas of Bangladesh include residents who often disrupt healthcare access in flooding seasons.Rohingya refugees refer to a stateless Muslim minority displaced from Myanmar and living in often-overcrowded settlements.Makeshift camps refer to temporary, unregistered refugee shelters that lack formal infrastructure.And left-behind children refer to those whose parents have migrated for work—often across borders or to urban areas, leaving children in the care of relatives or guardians, with inconsistent health service follow-up.
Parental adherence to immunization schedules plays a pivotal role in ensuring timely protection of children under five years of age. However, parental decisions are shaped by a complex interplay of factors that include cultural beliefs, trust in health systems, perceived vaccine efficacy, and experiences with health service delivery. In ethnic minority communities, traditional norms, language barriers, and historical exclusion from mainstream health campaigns may further hinder vaccine acceptance and completion [4].
Asia has a diverse array of marginal groups and offers a unique landscape for exploring how contextual factors shape parental behavior toward immunization. Yet, existing research is fragmented across countries and regions, lacking a cohesive synthesis of the key determinants that influence adherence among these groups. This narrative review aimed to consolidate and critically analyze the literature on determinants of parental adherence to childhood immunization among children under five in the marginalized population in Asia. By identifying common barriers and facilitators across cultural and national contexts, this review seeks to inform culturally responsive immunization strategies and policies to improve vaccine equity across the region.
2. Materials and Methods
2.1. Study Selection
Although systematic search methods and PRISMA guidelines were used to enhance transparency and reproducibility, this review adopts a narrative design and thematic synthesis approach. We conducted a narrative literature review of studies published between 2015 and 2025 (with earlier landmark studies included if relevant), publications in English, and studies conducted in Asia, with a country-specific focus. Searches were performed in PubMed, Scopus, and Google Scholar. Search strategies were adapted to the syntax of each database, and full Boolean strings are provided in Table 1. A small number of systematic reviews were retained for contextual insights. Their findings were not coded, counted, or included in the synthesis themes. This review did not adopt an umbrella design or aggregate findings from secondary reviews.

Table 1.
Key terms or Boolean operators used for searching in each database.
Geographic scope of selected studies (Figure A2/Appendix B): this review focuses on marginalized populations within South and Southeast Asia, where disparities in childhood immunization coverage are most pronounced due to intersecting social, economic, and health system barriers. Countries represented in the included studies include India, Bangladesh, Nepal, Pakistan, Myanmar, Indonesia, Vietnam, Cambodia, and the Philippines.
Refugee and displaced populations such as the Rohingya (from Myanmar, residing in Bangladesh), urban slum dwellers, and left-behind children of migrant workers are considered within the national and subnational contexts of these countries.
Western Asia was excluded to maintain regional coherence, as the sociopolitical drivers of marginalization and immunization system structures differ substantially. Inclusion would have introduced heterogeneity that limits comparative synthesis across themes.
2.2. Eligible Criteria
The inclusion and exclusion criteria focused on determinants of parental and caregiver adherence to childhood immunization in children under five in marginalized populations across Asia. The 2015–2025 time frame was chosen to capture evidence relevant to recent immunization policies and health system changes. Only English-language studies were considered due to feasibility. Restricting to marginalized populations helped highlight barriers and facilitators among groups at greatest risk of incomplete immunization. Besides original articles, quantitative studies were included. Qualitative studies were also incorporated to provide contextual insights into barriers and facilitators. In addition to primary research articles, relevant systematic reviews were included when they were used to contextualize findings and highlight broader patterns, while individual studies provided detailed evidence from marginalized populations in Asia.
Geography: This review focused on “Asia” including South, Southeast, and East Asia, following the United Nations’ geoscheme classification.
Populations: parents, mothers, fathers, or primary caregivers responsible for vaccination decisions for children under five years of age.
Context: marginalized populations defined as groups facing barriers to healthcare access due to social, economic, cultural, or geographic disadvantages (e.g., slum dwellers, rural poor, urban poor, indigenous peoples, migrants, refugees, minorities, hard-to-reach populations, underserved or disadvantaged groups).
We excluded studies on adult immunization, clinical vaccine efficacy trials, and studies focusing exclusively on a single vaccine (e.g., measles-only, polio-only). The aim of this review was to identify determinants of parental adherence to the overall childhood immunization schedule under the Expanded Program on Immunization (EPI), rather than determinants specific to one antigen. An exception was made when such studies provided insights into broader determinants of parental adherence (e.g., socioeconomic status, cultural beliefs, access barriers) that influence the entire childhood immunization schedule. In these cases, determinants were extracted and synthesized at the program level rather than vaccine-specific. Countries of Western Asia, including those in the Arabian Peninsula and the broader Middle East and North Africa (MENA) region, were excluded.
2.3. Search Strategy
This narrative review was performed according to the guidelines of Preferred Re-porting Items for Systematic Reviews and Meta-Analyses (PRISMA).The search was conducted from 3 January 2025 to 15 May 2025.Relevant studies were identified from the major bibliographic databases (PubMed, Scopus, Google Scholar) that are presented in Table A1/Appendix A, focusing on determinants of parental adherence to childhood immunization in children under five in marginalized populations in Asia. The comprehensive search string of published literature applied the combinations of key terms and Boolean operators (see Table 1).
The PRISMA diagram (Figure 1) reveals the selection process and shows the reasons for exclusion. The initial search across PubMed, Scopus, and Google Scholar yielded 756 records. After removing duplicates, conference proceedings, and non-peer-reviewed sources (n) = 627), 129 records remained for title and abstract screening. Of these, 94 records were excluded for reasons including the following: wrong population (not parents/caregivers of under-five children, or not marginalized groups), wrong setting (studies conducted outside Asia or in high-income countries), wrong outcome/focus (articles on vaccine efficacy, safety, or clinical outcomes rather than determinants of parental adherence), and publication type/insufficient data (commentaries, editorials, protocols, or abstracts lacking relevant information).Thirty-five full-text articles were assessed for eligibility. Fourteen were excluded for the same reasons—wrong population (n = 5), wrong outcome (n = 4), wrong setting (n = 2), adult immunization focus (n = 2), and insufficient data (n = 1). Finally, 21 studies met all inclusion criteria and were included in the narrative synthesis. Two included studies were themselves systematic reviews.These were not integrated into the thematic synthesis alongside primary studies.Instead, they were retained for context and triangulation.Findings from these reviews were cited descriptively where relevant but were not used to identify or code determinants.No data were duplicated from primary studies already included.
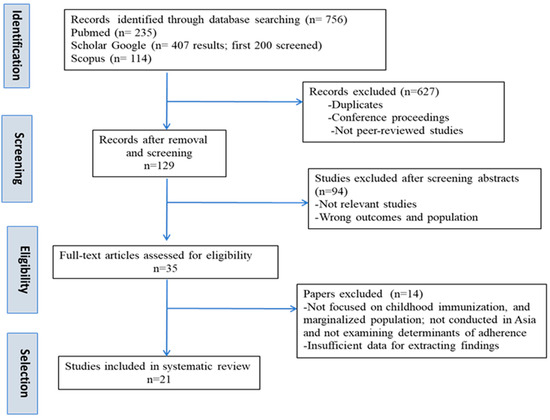
Figure 1.
The PRISMA flow diagram describing the study selection process. Note: This flow diagram follows PRISMA-style formatting for transparency but reflects procedures adapted to a narrative literature review.
2.4. Data Extraction and Analsis
Findings from quantitative studies were summarized to highlight measurable determinants such as socioeconomic, demographic, and healthcare access factors, while qualitative studies were narratively integrated to capture contextual influences.Four authors independently extracted data using a standardized template in Microsoft Excel, and qualitative findings were organized and coded using NVivo 12 to ensure consistency and reduce bias.The extracted information includedAuthor, Year; Country/Region; Population (parents/caregivers/children); Study Design; Sample size/Data source; Determinants examined; Key findings (direction/association); Qualitative themes/quotes; Contextual insights (policy, system, cultural); and Strengths/Limitations (see Table 2). The primary outcome variables were the determinants of parental adherence to childhood immunization.Discrepancies between extractors were resolved through discussion and consensus, with adjudication by a senior author when necessary.For reference management, EndNote X9 was used to organize citations and remove duplicates.The evidence was then synthesized thematically to identify converging and complementary influences across study types.
Table 2.
Data extraction from 21 studies included in the systematic review.
2.5. Risk of Bias and Quality Assessment
Because this review included both quantitative and qualitative studies, formal meta-analysis was not feasible. Instead, study quality was appraised descriptively. For quantitative studies, considerations included clarity of population definition, representativeness of sampling, validity of immunization outcome measures, and adjustment for confounding factors (adapted from the Newcastle–Ottawa Scale) [24]. For qualitative studies, credibility and transferability of findings were assessed based on methodological clarity and depth of contextual insights (adapted from the CASP Qualitative Checklist) [25]. For review-level evidence, transparency of search strategies, inclusion criteria, and synthesis methods were considered. In Table A2/Appendix A, of the twenty-one included studies, nine were judged to be at low risk of bias, primarily large-scale quantitative analyses based on nationally representative datasets such as DHS, MICS, and IFLS, as well as two systematic reviews. Only primary studies included in thematic synthesis were appraised for risk of bias.
The remaining twelve studies were assessed as moderate risk, consisting mainly of smaller cross-sectional surveys, qualitative inquiries, and mixed-methods designs that, while valuable for contextual insights, were limited by sample size, non-probability sampling, or restricted generalizability. No study was classified as high risk, and all provided sufficient methodological transparency to contribute meaningfully to the synthesis. Given the narrative design of this review, no study was excluded on the basis of quality alone, but risk-of-bias assessments were used to guide interpretation of findings.
3. Results
3.1. Overview of Included Studies
This review included 21 studies published between 2016 and 2025, conducted in India, Bangladesh, Pakistan, Nepal, Vietnam, China, Malaysia, Lao PDR, and the Philip-pines, along with two regional systematic reviews from Southeast Asia. Designs included quantitative cross-sectional surveys [4,5,6,17,19,20,21], large national analyses [7,8,15,16], qualitative studies [3,9,18,22,23,24], mixed-methods approaches [10,11], and systematic reviews [12,13,14]. Populations studied were slum dwellers, refugees, migrants, left-behind children, ethnic minorities, and rural/remote households. Data extractions from included studies are described in Table 2.
3.2. Thematic Synthesis of Determinants of Parental Adherence
A narrative thematic synthesis was conducted to identify recurring determinants of parental adherence across included studies. Themes were developed through an inductive–deductive approach, combining a priori coding (based on the research objectives and literature) with emergent codes identified during full-text review). Coded segments were clustered into five overarching thematic domains:
- (1)
- Socioeconomic and access inequities;
- (2)
- Trust, cultural beliefs and social norms;
- (3)
- Migration, refugee, and mobility-related vulnerabilities;
- (4)
- Household and caregiver dynamics;
- (5)
- Health system and program.
Representative codes and illustrative quotes from qualitative studies are presented in Table 3 to support transparency and contextual insight.
Table 3.
Representative codes and illustrative quotes and insights supporting thematic domains.
Mapping of determinants to thematic domains is provided in Table A3/Appendix A. The interactions between five domains are visualized in Figure A1/Appendix B.
3.2.1. Socioeconomic and Access Inequities
Socioeconomic position consistently shaped parental adherence. Maternal education and household wealth were repeatedly shown to increase the likelihood of complete immunization [5,8,12]. For instance, Bangladesh surveys revealed that possession of an EPI card and higher maternal education reduced zero-dose status in slums and haor communities [5]. In India, national analyses confirmed that facility quality interacts with household wealth, exacerbating rich–poor disparities in rural areas [7]. In Indonesia, inequalities by maternal education and socioeconomic status persisted across provinces [15]. Geographic access compounded socioeconomic barriers. Remote and ethnic minority populations in the Lao PDR and Vietnam border and highland regions experienced lower adherence due to distance, transport costs, and language barriers [3,4,16].
3.2.2. Trust, Cultural Beliefs, and Social Norms
Trust in healthcare providers and cultural beliefs were major determinants of parental decisions. In Pakistan’s slums, adherence was hindered by misconceptions about side effects and religious opposition [11]. In Bangladesh’s Rohingya settlements, parents in registered camps demonstrated higher adherence than those in makeshift camps, reflecting stronger trust in formal systems [17].
Social norms and interpersonal communication strongly predicted vaccination intentions in India’s urban slums, explaining nearly half of the variance in behavioral intention models [6]. In the Philippines, the Dengvaxia® vaccine controversy eroded trust, reducing measles vaccine uptake [18]. A systematic review also highlighted how misinformation, online narratives, and fear of autism reinforced distrust, particularly among higher-SES and more educated parents [14].
In Nepal, caregivers described providers as unresponsive, while health workers described inadequate community cooperation, underscoring the cycle of mutual distrust [9].
3.2.3. Migration, Refugee, and Mobility-Related Vulnerabilities
Refugee and migrant status was consistently linked with incomplete immunization. Among Rohingya children in Malaysia, only 2.5% were fully immunized, with birthplace and access to health services as major predictors [19]. Similarly, stateless children of North Korean refugees in China had coverage ranging only from 12% to 98%, compared with nearly universal coverage among local children [20].
Left-behind children in China had the lowest non-national immunization program (NIP) vaccine coverage, reflecting disrupted care arrangements [21]. A systematic review confirmed that left-behind children are also at greater risk of incomplete immunization and other adverse health outcomes [13]. In Vietnam’s border regions, minority children had extremely low adherence (18.9%), which was associated with structural barriers and low parental self-efficacy [4].
3.2.4. Household and Caregiver Dynamics
Caregiver characteristics and family structures significantly were associated with adherence. Maternal occupation and mobility were associated with incomplete immunization in India, where working mothers were less able to attend vaccination sessions [10]. In Bangladesh’s refugee camps, father’s education and employment predicted adherence, particularly in makeshift settlements [17]. In Vietnam’s border areas, firstborn and younger children were more likely to be vaccinated [4]. Extended family members also played a role. Grandmothers and fathers were actively engaged in decision-making in Nepal [9], while tribal chiefs were gatekeepers in rural Pakistan, shaping community-level acceptance [22].
3.2.5. Health System and Programmatic Factors
Supply-side determinants emerged as equally important. In India, higher-quality facilities improved both the completeness and timeliness of vaccination [7]. In Pakistan’s underserved districts, shortages of female vaccinators, poor staff capacity, and weak community engagement contributed to dropout and refusals [22]. Provider perspectives from China emphasized systemic barriers, including staff shortages, vaccine hesitancy, and fragmented information systems [23].
Programmatic tools also mattered. EPI card possession was one of the strongest predictors of adherence in Bangladesh [5]. In China, providers recommended improved follow-up mechanisms such as maternal–child health visits and school verification to strengthen continuity [23]. Reviews across Southeast Asia confirmed the positive impact of antenatal care visits, institutional delivery, and maternal–child health integration on immunization compliance [12].
3.2.6. Summary
Across the 21 studies, adherence to childhood immunization among marginalized populations in Asia was consistently shaped by structural inequities (education, wealth, geography), trust and social perceptions, migration-related vulnerabilities, household decision-making dynamics, and health system/programmatic quality. These determinants interact and reinforce one another, highlighting the need for equity-oriented, context-sensitive strategies to strengthen EPI coverage in marginalized populations.
4. Discussion
4.1. Principal Findings
This review synthesized 21 studies on determinants of parental adherence to childhood immunization among children under five in marginalized populations in South, Southeast, and East Asia. Across settings, adherence was shaped by five interrelated themes.
Socioeconomic and access inequities were consistent determinants. Maternal education, household wealth, and possession of vaccination documentation (e.g., EPI card) strongly predicted adherence. Remoteness and transport costs compounded inequities, particularly for highland, border, and minority communities.
Parental decisions regarding childhood immunization were shaped by trust, cultural beliefs, and prevailing social norms. Misconceptions about vaccine safety, religious objections, and misinformation reduced uptake, whereas trust in providers and supportive social norms enhanced it. The Dengvaxia® controversy in the Philippines demonstrated how one event can erode trust across the broader immunization program.
Migration, refugee, and mobility-related vulnerabilities were striking. Refugee and stateless children in Malaysia and China, and left-behind children of migrants, had markedly lower coverage compared to host populations. Mobility and weak registration systems undermined continuity of care.
Household and caregiver dynamics were important contextual factors. Fathers, grandmothers, and community leaders were often reported to play key roles in parental decision-making, underscoring that vaccination is not solely a maternal responsibility. Larger household size, birth order, and maternal employment status were also associated with immunization uptake.
Finally, health system and programmatic factors strongly shaped adherence. Facility readiness, staffing, provider communication, and follow-up systems were frequently associated with immunization inequities.
Tools such as the EPI card in Bangladesh emerged as powerful equity instruments, while lack of outreach, female vaccinators, and community mobilization undermined program success.
4.2. Comparison with Prior Reviews
The findings of this review are consistent with earlier global analyses that identified maternal education, socioeconomic status, and health service access as core determinants of immunization coverage [26,27,28]. In this review, “coverage” refers to the proportion of children who received vaccinations, commonly used as a health system performance indicator. “Adherence”, on the other hand, refers to caregivers’ timely compliance with the recommended vaccination schedule—capturing not just whether vaccines were received but also whether they were administered at the appropriate ages and intervals.
Like prior reviews, this synthesis confirms that education and wealth gradients are strongly associated with child vaccination status across diverse contexts.
However, the present review adds four contributions. First, it emphasizes context-specific vulnerabilities unique to Asia, such as left-behind children of migrants, ethnic minorities in highlands and border areas, and the lasting effects of vaccine controversies. Second, it demonstrates the interdependence of demand- and supply-side determinants. For instance, demand may be high but undermined by provider distrust, weak infrastructure, or lack of follow-up. Similarly, possession of an EPI card was consistently associated with improved adherence, highlighting the role of programmatic design. Trust, provider relationships, and communication are equally critical. For example, even when awareness was high, distrust of providers or poor facility quality limited adherence—a pattern not fully captured in quantitative-only global reviews. Third, this review underscores how vaccine controversies and misinformation uniquely shape adherence in Asia. The Dengvaxia® case in the Philippines illustrates how negative experiences with one vaccine can spill over to others, echoing findings from global research on how rumors and misinformation erode vaccine confidence [18,29,30].
Finally, unlike broader global reviews that often emphasize national averages, this synthesis focuses explicitly on marginalized populations. In doing so, it highlights how structural exclusion—systemic barriers embedded in health, social, and legal systems—amplifies inequities in immunization. Such exclusion arises when refugee and stateless children are denied access due to legal restrictions, when migrants and left-behind children are missed because of weak registration and follow-up systems, or when ethnic minorities in remote areas face geographic and language barriers not addressed by mainstream programs. These dynamics show that under-immunization is not merely the result of parental choice but often reflects institutional and societal structures that fail to equitably serve all groups [31].
4.3. Implications for Policy and Practice
Improving immunization adherence in marginalized populations requires integrated strategies. Equity-focused approaches should prioritize underserved groups by expanding outreach, reducing indirect costs, and strengthening registration systems, consistent with global recommendations to target zero-dose children [32].
Community engagement must rebuild trust, counter misinformation, and include fathers, grandmothers, and community and religious leaders—an approach supported by other reviews showing that community ownership improves vaccine uptake [33].
The integration of maternal and child health (MCH)services with routine immunization is recognized as an important global health strategy, particularly in low- and middle-income countries. Linking immunization with services such as antenatal care, institutional delivery, and school-entry checks can reduce missed opportunities and improve continuity of care. This review reinforces prior evidence showing that integrated service delivery not only strengthens immunization uptake but also enhances equity by reaching mothers and children who might otherwise remain outside the health system [34].
Migrant and refugee inclusion is essential, echoing calls from global health policy frameworks that immunization services should transcend legal or administrative barriers [35].
4.4. Evidence Gaps and Future Research Directions
Despite the breadth of evidence, several gaps remain. Populations such as indigenous communities beyond Vietnam, seasonal migrants, fathers as primary decision-makers, and caregivers of children with disabilities were underrepresented. Determinants related to digital registration/ID systems, disinformation dynamics in Asian contexts, interpersonal provider–caregiver quality, and indirect costs remain poorly studied.
Furthermore, programmatic evidence is particularly limited. Few studies rigorously evaluated outreach/mobile services, incentive schemes, defaulter tracing, or multilingual counseling, despite their relevance to marginalized groups. Future research must move beyond descriptive studies to rigorous intervention evaluations, as emphasized in recent global reviews [36].
4.5. Strengths and Limitations
This review contributes a comprehensive synthesis across multiple marginalized populations in Asia, integrating evidence from surveys, and qualitative inquiries. Its focus on determinants rather than vaccine efficacy highlights the social and structural barriers to immunization adherence. Study quality was considered in interpreting the results.Findings from studies rated as lower quality (e.g., lacking clarity in methods or sampling) were interpreted with caution and weighed less heavily in the synthesis of themes.Two retained systematic reviews served a supplementary role.Their findings were referenced contextually but did not inform the thematic structure or determinant mapping to avoid duplication bias.
However, limitations include restriction to English-language studies between 2015 and 2025, which may exclude local-language research. The narrative approach precludes meta-analysis and introduces potential selection bias. Study heterogeneity further limited comparability across countries.
5. Conclusions
Parental adherence to childhood immunization in marginalized Asian populations is shaped by (1) socioeconomic inequities, (2) trust and cultural beliefs, (3) migration vulnerabilities, (4) household dynamics, and (5) health system quality. These determinants interact, reinforcing disadvantages. Addressing them will require equity-oriented, context-specific approaches that integrate service delivery, strengthen trust, and adapt to the realities of marginalized groups. Filling evidence gaps with targeted research and program evaluations is essential to achieve universal immunization coverage and ensure no child is left behind.
Author Contributions
Conceptualization, C.N.L., N.N., and N.C.; methodology, C.N.L., A.D.T., N.C., and L.T.K.N.; software, U.T.T.N., N.C., and A.D.T.; validation, N.N., U.T.T.N., and L.T.K.N.; formal analysis, C.N.L. and N.C.; investigation, N.N., N.C., and A.D.T.; resources, U.T.T.N. and L.T.K.N.; data curation, A.D.T.; writing—original draft preparation, N.N. and C.N.L.; writing—review and editing, C.N.L. and N.C.; visualization, U.T.T.N.; supervision, N.N.; project administration, C.N.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data generated in this study is available by contacting the corresponding author, Cua Ngoc Le, if requested reasonably.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Table A1.
Database and source used in review.
Table A1.
Database and source used in review.
| Database/Source | Coverage | Notes |
|---|---|---|
| PubMed/MEDLINE | Biomedical and public health literature | MeSH + free text |
| Scopus | Multidisciplinary, large coverage | Includes conference proceedings |
| WHO Global Index Medicus (WPRIM, IMSEAR, AIM) | Regional databases for Asia | Captures local research |
| Google Scholar | General search and gray literature | First 200 results screened (out of 407 retrieved) |
Table A2.
Risk of bias and quality appraisal of included studies.
Table A2.
Risk of bias and quality appraisal of included studies.
| Author, Year | Country/Region | Study Type | Appraisal Outcomes | Notes |
|---|---|---|---|---|
| * Ichimura et al., 2022 [16] | Lao People’s Democratic Republic | Nationwide cross-sectional study (multistage cluster sampling) | Low risk | Nationwide sampling; vaccination records validated; minor bias from excluding children without cards. |
| * Siramaneerat & Agushybana 2021 [8] | Indonesia | Quantitative DHS multilevel analysis | Low risk | Large representative DHS dataset; multilevel modeling; recall bias possible. |
| * Sinuraya et al. 2024 [15] | Indonesia | Quantitative IFLS secondary analysis | Low risk | Large national dataset; advanced regression; limited by secondary data use. |
| * Miras et al., 2023 [18] | Philippines | Qualitative ethnography | Moderate risk | Rich contextual insights; theory-driven; limited by single urban setting and purposive sample. |
| * Das et al., 2024 [5] | Bangladesh (slums and haors) | Quantitative, cross-sectional | Moderate risk | Good description; convenience sampling; risk of reporting bias. |
| * Nguyen et al., 2025 [3] | Vietnam (Daklak highlands) Ethnic minority mothers and HCWs | Qualitative (IDIs, FGDs, observation) | Moderate risk | Valuable contextual insights; small sample; limited generalizability. |
| * Rimal et al., 2024 [6] | India (Varanasi slums) | Quantitative (survey) | Low risk | Large sample size. Clear determinants identified; non-probability sampling; recall bias. |
| * Francis et al., 2021 [10] | India (Vellore, Tamil Nadu) | Mixed-methods (survey + FGDs) | Moderate risk. | Combines survey and FGDs; limited sample; good contextual triangulation |
| * Muhammad et al., 2023 [11] | Pakistan (Karachi slums) | Mixed-methods | Moderate risk. | Sample adequate; limited confounder control; self-reported immunization status. |
| * Racaite et al., 2021 [13] | Multi-country (review, China focus) | Quantitative study | Low risk | Good sampling; clear analysis; strong data on NIP vs. non-NIP vaccines. |
| Kalaij et al., 2021 [12] | Southeast Asia (multi-country) | Systematic review | Low risk | Transparent synthesis; PRISMA-based; complements primary studies |
| * Tran et al., 2025 [4] | Vietnam–Cambodia border (Dong Thap) | Quantitative (survey + regression) | Moderate risk | Good integration of quantitative and qualitative data; limited by local scope. |
| * Ahmed et al., 2023 [17] | Bangladesh | Quantitative (cross-sectional survey) | Moderate risk | Good sample in difficult-to-access refugee camps; limited generalizability beyond Cox’s Bazar. |
| * Summan et al., 2022 [7] | India (rural, multi-state) | Quantitative (national survey analysis, decomposition) | Low risk | Robust national survey and facility data; large sample size |
| * Paul et al., 2022 [9] | Nepal (Makwanpur District) | Qualitative (IDIs, KIIs, FGDs) | Moderate risk | Rich qualitative depth; district-level scope only. |
| Novilla et al., 2023 [14] | Multi- countries | Systematic review | Low risk | Comprehensive SR; most evidence, indirect transferability. |
| * Al-Haroni et al., 2023 [19] | Malaysia (Ampang district, Kuala Lumpur) | Quantitative (cross-sectional) | Moderate risk | limited generalizability (one district) |
| * Chung et al., 2016 [20] | China (Yanbian) | Quantitative (survey + vaccination cards) | Moderate risk | Comparative survey; limited to one prefecture. |
| * Zhou et al., 2023 [21] | China (Zhejiang & Henan) | Quantitative (cross-sectional survey) | Low risk | Large survey and generalizability; self-report bias possible. |
| * Qayyum et al., 2021 [22] | Pakistan (Rajanpur district) | Qualitative (IDIs, FGDs) | Moderate risk | Qualitative depth; not generalizable quantitatively. |
| * Lin et al., 2022 [23] | China (Sichuan, Guangdong, Henan) | Qualitative (interviews) | Moderate risk | Good provider perspective; small sample |
Note: Criteria for appraisal were adapted from commonly used frameworks for assessing risk of bias in observational and qualitative studies, including the Newcastle–Ottawa Scale (for cross-sectional studies) and the Critical Appraisal Skills Programme (CASP) checklist (for qualitative research), but applied descriptively to align with the narrative review design. Studies marked with an asterisk (*) were appraised using these criteria. The two systematic reviews (Kalaij et al., 2021 [12]; Novilla et al., 2023 [14]) were appraised for general quality and transparency but were not thematically synthesized. Only primary studies informed the thematic domains.
Table A3.
Mapping of determinants to thematic domains.
Table A3.
Mapping of determinants to thematic domains.
| Determinants Identified from Included Studies | Thematic Domains |
|---|---|
| Maternal education, household wealth, EPI card possession | Socioeconomic and access inequities |
| Geographic remoteness, transport barriers, rural residence | Socioeconomic and access inequities |
| Misconceptions about vaccines, fear of side effects, religious objections | Trust, cultural beliefs and social norms |
| Misinformation, media influence, vaccine controversies (e.g., Dengvaxia® in the Philippines) | Trust, cultural beliefs and social norms |
| Refugee status (Rohingya in Malaysia, displaced populations in camps) | Migration, refugee, and mobility-related vulnerabilities |
| Stateless children, left-behind children, seasonal migrants | Migration, refugee, and mobility-related vulnerabilities |
| Birth order, family size, father’s age, caregiver occupation | Household and caregiver dynamics |
| Influence of grandmothers, fathers, tribal/community leaders | Household and caregiver dynamics |
| Facility quality, staff shortages, availability of female vaccinators | Health system and program |
| Provider communication, follow-up mechanisms, integration with maternal–child health services | Health system and program |
Appendix B

Figure A1.
Conceptual Framework for determinants of parental adherence to childhood immunization in marginalized populations (Asia).

Figure A2.
Countries included in the review (South and Southeast Asia). Note: Countries highlighted in blue represent those within South and Southeast Asia that were included in this review. Countries shown in gray (e.g., in Western Asia and the Middle East) were excluded from the review due to regional, political, and health system differences that limit thematic comparability.
References
- Shah, B. Immunization strategies for preventing infectious diseases in children. J Health Med. Res. Innov. 2025, 3, 7–12. [Google Scholar] [CrossRef]
- Ngwa, C.H.; Doungtsop, B.C.; Bihnwi, R.; Ngo, N.V.; Yang, N.M. Burden of vaccine-preventable diseases, trends in vaccine coverage and current challenges in the implementation of the expanded program on immunization: A situation analysis of Cameroon. Hum. Vaccines Immunother. 2022, 18, 1939620. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.H.; Mai, T.P.L.; Thwaites, C.L.; Van Nuil, J.I. High immunisation coverage but sporadic outbreaks of vaccine-preventable diseases: The structural gaps in vaccination uptake in central highlands, Vietnam. BMC Public Health 2025, 25, 2293. [Google Scholar] [CrossRef]
- Tran, D.A.; Suwanbamrung, C.; Stanikzai, M.H.; Chutipattana, N.; Shohaimin, S.; Khammaneechan, P.; Luan, L.M.; Dien, T.P.; Nam, T.T.; Tung, P.T.; et al. Parental predictors of childhood vaccination adherence in border areas of Southern Vietnam: A first look at minority communities. J. Pediatr. 2025, 101, 642–650. [Google Scholar] [CrossRef]
- Das, H.; Jannat, Z.; Fatema, K.; Momo, J.E.; Ali, M.W.; Alam, N.; Chowdhury, M.E.; Morgan, C.; Oliveras, E.; Correa, G.C.; et al. Prevalence of and factors associated with zero-dose and under-immunized children in selected areas of Bangladesh: Findings from Lot Quality Assurance Sampling Survey. Vaccine 2024, 42, 3247–3256. [Google Scholar] [CrossRef]
- Rimal, R.N.; Ganjoo, R.; Jamison, A.; Parida, M.; Tharmarajah, S. Social norms, vaccine confidence, and interpersonal communication as predictors of vaccination intentions: Findings from slum areas in Varanasi, India. Vaccine 2024, 42, 126038. [Google Scholar] [CrossRef]
- Summan, A.; Nandi, A.; Schueller, E.; Laxminarayan, R. Public health facility quality and child immunization outcomes in rural India: A decomposition analysis. Vaccine 2022, 40, 2388. [Google Scholar] [CrossRef]
- Siramaneerat, I.; Agushybana, F. Inequalities in immunization coverage in Indonesia: A multilevel analysis. Rural. Remote Health 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Paul, A.M.; Nepal, S.; Upreti, K.; Lohani, J.; Rimal, R.N. The last stretch: Barriers to and facilitators of full immunization among children in Nepal’s Makwanpur District, results from a qualitative study. PLoS ONE 2022, 17, e0261905. [Google Scholar] [CrossRef]
- Francis, M.R.; Nuorti, J.P.; Lumme-Sandt, K.; Kompithra, R.Z.; Balraj, V.; Kang, G.; Mohan, V.R. Vaccination coverage and the factors influencing routine childhood vaccination uptake among communities experiencing disadvantage in Vellore, southern India: A mixed-methods study. BMC Public Health 2021, 21, 1807. [Google Scholar] [CrossRef]
- Muhammad, A.; Ahmad, D.; Tariq, E.; Yunus, S.; Warsi, S.; Hasmat, L.; Khawar, H.; Jimenez, M.; Ashraf, M.; Shafiq, Y. Barriers to childhood vaccination in urban slums of Pakistan. East. Mediterr. Health J. 2023, 29, 371–379. [Google Scholar] [CrossRef]
- Kalaij, A.G.; Sugiyanto, M.; Ilham, A.F. Factors associated with vaccination compliance in Southeast Asian children: A systematic review. Asia Pac. J. Public Health 2021, 33, 479–488. [Google Scholar] [CrossRef]
- Račaitė, J.; Lindert, J.; Antia, K.; Winkler, V.; Sketerskienė, R.; Jakubauskienė, M.; Wulkau, L.; Šurkienė, G. Parent emigration, physical health and related risk and preventive factors of children left behind: A systematic review of literature. Int. J. Environ. Res. Public Health 2021, 18, 1167. [Google Scholar] [CrossRef]
- Novilla, M.L.; Goates, M.C.; Redelfs, A.H.; Quenzer, M.; Novilla, L.K.; Leffler, T.; Holt, C.A.; Doria, R.B.; Dang, M.T.; Hewitt, M.; et al. Why parents say no to having their children vaccinated against measles: A systematic review of the social determinants of parental perceptions on MMR vaccine hesitancy. Vaccines 2023, 11, 926. [Google Scholar] [CrossRef] [PubMed]
- Sinuraya, R.K.; Alfian, S.D.; Abdulah, R.; Postma, M.J.; Suwantika, A.A. Comprehensive childhood vaccination and its determinants: Insights from the Indonesia Family Life Survey (IFLS). J. Infect. Public Health 2024, 17, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Ichimura, Y.; Yanagisawa, N.; Thandar, M.M.; Pathammavong, C.; Phounphenghuk, K.; Nouanthong, P.; Tengbriacheu, C.; Khamphaphongphane, B.; Franzel-Sassanpour, L.E.; Yang, T.U.; et al. The determinants of immunization coverage among children aged between 12 and 35 months: A nationwide cross-sectional study in Lao People’s Democratic Republic. BMC Public Health 2022, 22, 2259. [Google Scholar] [CrossRef]
- Ahmed, N.; Ishtiak, A.S.; Rozars, M.F.; Bonna, A.S.; Alam, K.P.; Hossan, M.E.; Das, R.; Khan, J.; Mishu, T.Z.; Afrin, S.; et al. Factors associated with low childhood immunization coverage among Rohingya refugee parents in Cox’s Bazar, Bangladesh. PLoS ONE 2023, 18, e0283881. [Google Scholar] [CrossRef]
- Miras, A.P.; Regencia, Z.J.; Baja, E.S. ‘I was terrified for my child’: Understanding the link between the Dengvaxia® controversy and the measles vaccine hesitancy in Pasay City, Philippines. J. Public Health 2023, 45, 912–918. [Google Scholar] [CrossRef]
- Al-Haroni, H.; Muthanna, A.; Nasir Mohd Desa, M.; Azzani, M. Immunisation coverage and its determinants among Rohingya refugee children in Malaysia. Aust J Gen Pract. 2023, 52, 712–719. [Google Scholar] [CrossRef]
- Chung, H.J.; Han, S.H.; Kim, H.; Finkelstein, J.L. Childhood immunizations in China: Disparities in health care access in children born to North Korean refugees. BMC Int. Health Hum. Rights 2016, 16, 13. [Google Scholar] [CrossRef]
- Zhou, Y.; Li, D.; Cao, Y.; Lai, F.; Wang, Y.; Long, Q.; Zhang, Z.; An, C.; Xu, X. Immunization coverage, knowledge, satisfaction, and associated factors of non-National Immunization Program vaccines among migrant and left-behind families in China: Evidence from Zhejiang and Henan provinces. Infect. Dis. Poverty 2023, 12, 69–80. [Google Scholar] [CrossRef]
- Qayyum, K.; Rehan, N.; Khalid, F.; Younas, M. Addressing community barriers to immunization in Rajanpur district, Pakistan: An implementation research. J. Glob. Health Rep. 2021, 5, e2021088. [Google Scholar] [CrossRef]
- Lin, S.Y.; Zhang, S.Y.; Chantler, T.; Sun, F.Y.; Zou, J.T.; Cheng, J.J.; Chen, Y.Q.; Sun, M.; Howard, N. Vaccination coverage determinants in low uptake areas of China: A qualitative study of provider perspectives in Sichuan, Guangdong, and Henan Provinces. Hum. Vaccines Immunother. 2022, 18, 2030623. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 15 March 2025).
- Critical Appraisal Skills Programme (CASP). CASP Qualitative Checklist; CASP: Oxford, UK, 2018; Available online: https://casp-uk.net/casp-tools-checklists/qualitative-studies-checklist/ (accessed on 21 February 2025).
- Rainey, J.J.; Watkins, M.; Ryman, T.K.; Sandhu, P.; Bo, A.; Banerjee, K. Reasons related to non-vaccination and under-vaccination of children in low and middle income countries: Findings from a systematic review of the published literature, 1999–2009. Vaccine 2011, 29, 8215–8221. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpoor, A.R.; Bergen, N.; Schlotheuber, A.; Gacic-Dobo, M.; Hansen, P.M.; Senouci, K.; Boerma, T.; Barros, A.J. State of inequality in diphtheria-tetanus-pertussis immunisation coverage in low-income and middle-income countries: A multicountry study of household health surveys. Lancet Glob. Health 2016, 4, e617–e626. [Google Scholar] [CrossRef]
- Ali, H.A.; Hartner, A.M.; Echeverria-Londono, S.; Roth, J.; Li, X.; Abbas, K.; Portnoy, A.; Vynnycky, E.; Woodruff, K.; Ferguson, N.M.; et al. Vaccine equity in low and middle income countries: A systematic review and meta-analysis. Int. J. Equity Health 2022, 21, 82. [Google Scholar] [CrossRef]
- Larson, H.J.; De Figueiredo, A.; Xiahong, Z.; Schulz, W.S.; Verger, P.; Johnston, I.G.; Cook, A.R.; Jones, N.S. The state of vaccine confidence 2016: Global insights through a 67-country survey. EBioMedicine. 2016, 12, 295–301. [Google Scholar] [CrossRef]
- De Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Clouston, S.; Kidman, R.; Palermo, T. Social inequalities in vaccination uptake among children aged 0–59 months living in Madagascar: An analysis of Demographic and Health Survey data from 2008 to 2009. Vaccine 2014, 32, 3533–3539. [Google Scholar] [CrossRef]
- Gandhi, G. Charting the evolution of approaches employed by the Global Alliance for Vaccines and Immunizations (GAVI) to address inequities in access to immunization: A systematic qualitative review of GAVI policies, strategies and resource allocation mechanisms through an equity lens (1999–2014). BMC Public Health 2015, 15, 1198. [Google Scholar] [CrossRef]
- Nashwan, A.J.; Abuhammad, S. Zero-Dose Children, Misinformation, and Vaccine Hesitancy. Cureus 2025, 17, e82028. [Google Scholar] [CrossRef]
- Shah, M.P.; Morgan, C.J.; Beeson, J.G.; Peach, E.; Davis, J.; McPake, B.; Wallace, A.S. Integrated Approaches for the Delivery of Maternal and Child Health Services with Childhood Immunization Programs in Low-and Middle-Income Countries: Systematic Review Update 2011–2020. Vaccines 2024, 12, 1313. [Google Scholar] [CrossRef]
- World Health Organization. Ensuring the Integration of Refugees and Migrants in Immunization Policies, Planning and Service Delivery Globally; Global Evidence Review on Health and Migration (GEHM) series; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Wiysonge, C.S.; Oyo-Ita, A.; Oringanje, C.; Nwachukwu, C.E.; Oduwole, O.; Meremikwu, M.M. Interventions for improving coverage of childhood immunisation in low- and middle-income countries. Cochrane Database Syst. Rev. 2016, 7, CD008145. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).