Abstract
After reconstruction, the return to full competition rate of athletes is low, while the re-injury rate remains high despite the completion of a rehabilitation programme. Primary ACL prevention programmes are well developed, yet few research papers focus on secondary ACL injury prevention. The aim of current review is to determine if current ACL secondary prevention training has a positive influence on the re-injury rate, the clinical or functional outcomes, or the risk of re-injury in athletes. Studies investigating secondary prevention of ACL were searched in PubMed and EBSCOhost, followed by a review of the references in the identified articles. The existing evidence suggests that neuromuscular training, eccentric strengthening, and plyometric exercises may have a potential impact on improving biomechanical, functional, and psychological outcomes in athletes; however, the studies on the prevention of second ACL injury in athletes is scarce and inconclusive. Future research is needed to investigate the effectiveness of secondary ACL prevention in reducing the re-injury rates. (PROSPERO Registration number: CRD42021291308).
1. Introduction
Anterior Cruciate Ligament (ACL) injuries are one of the most common traumatic knee injuries in sports [1]. Approximately 200,000 to 250,000 ACL injuries occur annually within the United States [2], which have doubled over the past two decades despite the increasing research effort and the development of ACL prevention programmes [3]. ACL injuries may often be associated with meniscus injuries (55–65%) and cartilage injuries (16–46%) [4], causing a four-times higher risk of knee osteoarthritis [5], where patients may end up requiring a total knee replacement [6]. ACL injuries may also lead to an impairment of knee-related quality of life at 5 to 25 years [7].
Approximately 175,000 ACL reconstructions (ACLR) are performed each year in the United States [8]. After one year of surgery, 66% of the athletes were able to participate in a modified or full competition [9], and 55% could return to competition at their pre-injury level [10]. However, athletes who return to high levels of sport are 30 to 40 times more likely to suffer a second ACL injury compared with uninjured athlete [11]. It is reported that nearly 1 in 3 to 4 young, active athletes will sustain an ipsilateral or contralateral ACL injury after returning to sports [12], while nearly half of those happen within two months of returning to sports [13]. It was reported in a previous systematic review that the overall rate of secondary ACL injury was 27% in young athletes after ACLR [14], while young female athletes may have an even higher rate of re-injury up to 32% [15,16].
Previous ACL injuries not only contribute to a higher risk of ipsilateral ACL re-injury but also of contralateral ACL injuries [17]. The risk of a contralateral ACL injury was reported to be 5% in male athletes and 26% in female athletes, which means the risk of female athletes suffering from a contralateral ACL injury is as high as six times compared to male athletes [18].
The factors contributing to a higher risk of a second ACL injury include limb asymmetry in muscle strength and functional performance [19], neuromuscular impairments [20], psychological factors such as fear of re-injury and poor self-efficacy [21], and proprioceptive loss [22]. Quadriceps femoris muscle strength asymmetries may be associated with gait asymmetries, impaired alignment of the hip and knee, and alteration in knee biomechanics [23]. The altered neuromuscular timing and recruitment can lead to dynamic knee valgus stress in the lower limb; it has also been reported that female athletes show four times greater activation of their hamstring muscles than males during knee dynamic stress motion [24]. As muscle strength, neuromuscular control, and joint proprioception are essential factors contributing to the dynamic stability of the knee joint and are much impaired after an ACL reconstruction [22], exercises or training may be required to restore knee stability and function after a standardised rehabilitation programme.
Multiple reviews and meta-analyses on ACL injury prevention programmes (IPPs) have found that both plyometric and strength exercises were effective in preventing primary ACL injuries, while mixed results were found as to whether or not balance training needs to be included [25,26,27]. However, there is a lack of reviews or evidence towards secondary ACL injury prevention despite a low return to full competition rate and a high re-injury rate, as mentioned above.
The current review aims to provide insights into the impacts of currently developed ACL secondary injury prevention training on athletes. This may include the effectiveness to reduce a secondary injury rate or to reduce the risk of re-injury, types, and intensity of exercises that may be beneficial, and the ability to restore a normal knee function or better clinical and functional outcomes. These may help to (1) improve the understanding of how current secondary ACL prevention training is developed; (2) improve the understanding of the effectiveness of different types of exercises in reducing the risk of re-injury; (3) improve athletic performance while reducing the re-injury rate when athletes return to competitive sports.
2. Materials and Methods
Data management of this systematic review is reported in line with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) [28]. The review protocol has been registered in PROSPERO (Registration number: CRD42021291308).
2.1. Search Strategy
An electronic literature search has been conducted of the PubMed (1964 to 2021) and EBSCOhost (CINAHL, MEDLINE, ScienceDirect (1985 to 2021)) databases. The search identified all articles containing the terms “ACL” or “Anterior cruciate ligament”, “Second* injur* prevent*” or (“Reinjur* or re-injur* or recur*” and prevent*) or (Reconstruct* and train*), and “Athlet*.
2.2. Selection
Randomised control trials, randomised clinical trials, control trials, and therapeutic studies have been included. Review articles and meta-analyses have been included initially to locate all possible related studies. The reference lists of the included articles have also been reviewed for relevant articles. Dissertations, textbook chapters, articles without a full copy, qualitative studies, literature reviews, guidelines, audits, and single case studies were not considered.
The inclusion criteria included (1) English-language studies, (2) studies that contain a secondary ACL injury prevention training for athletes who have undergone a unilateral ACL reconstruction, (3) subjects included had a primary unilateral ACL injury and have completed an ACL reconstruction rehabilitation, and (4) studies that contain the effects of training on the clinical or functional outcomes, or modification of ACL re-injury risk factors, or influence on the rate of an ipsilateral or contralateral ACL re-injury. The exclusion criteria included (1) studies of primary ACL injury prevention, and (2) the subjects included had any previous ACL injuries on either limb with or without a reconstruction before this incidence.
2.3. Data Analysis
The articles identified were assessed for inclusion according to the inclusion criteria mentioned above based on their title and abstract according to an abstract review form. If they met the criteria or if it was unclear, the full text was retrieved. Irrelevant studies were excluded. The data extraction and the risk of bias assessment were completed with reference to the data extraction form provided by Cochrane Developmental, Psychosocial and Learning Problems, 2014 [29]. The data from each included study were abstracted for (1) sample demographics and sample size; (2) any control or comparison groups; (3) the intervention; (4) any information about the ACLR and post-ACLR rehabilitation; (5) ACL secondary prevention training components, duration, and the exercise types; (6) the key outcome measures; and (7) the key findings after the ACL secondary injury prevention training.
3. Results
The literature search elicited a total of 1581 references, while 345 were found to be duplicated and another 1212 were excluded. Two additional articles were identified through a second-hand search of articles eligible. A total of 26 studies were reviewed in full-text, while 16 were excluded. The risk of bias was assessed using the Cochrane risk of bias framework. Nine articles met the final inclusion criteria for the current systematic review [20,30,31,32,33,34,35,36,37] (Figure 1).
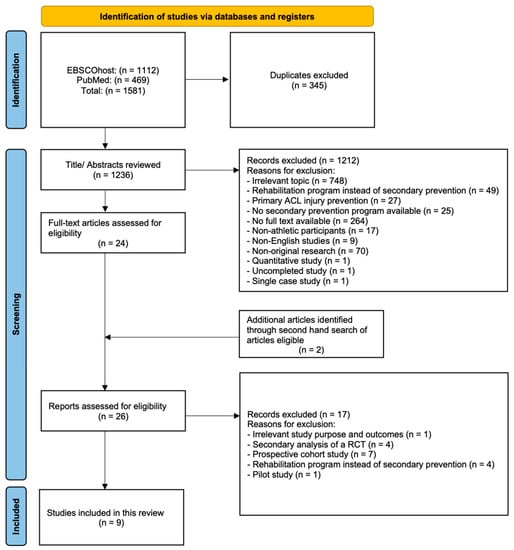
Figure 1.
Flow of information through the systematic literature search and screening.
Of the nine studies, none investigated the effects of secondary prevention programmes on the ACL re-injury rate in athletes, while all of them assessed the influence of these programmes on the modification of risk factors for a second ACL injury in athletes. All nine studies were prospective, while six were prospective randomised controlled trials, and three were prospective randomised clinical trials. Two studies were conducted for elite athletes at provincial or international levels. Table 1 summarises the characteristics of the participants, the surgical and rehabilitation information, the intervention, the key outcomes, and the key findings of the nine studies. These studies involved a total of 347 subjects, who were active in sports participation or competition before the injury. Overall, four studies found that secondary prevention programmes (including neuromuscular training, eccentric, and plyometric exercises) were effective in modifying risk factors for re-injury in athletes, including improving knee proprioception, functional performance, knee stability, landing biomechanics, and psychological readiness to return to sports. In contrast, five studies found that secondary prevention programmes (including running retraining, strength, agility, plyometrics, and perturbation training) were not effective in modifying the risk factors of an ACL re-injury in athletes (three focusing on restoring gait symmetries, one focusing on muscular and functional recovery, and one focusing on functional outcomes). Table 2 summarises the risk of bias in the included studies according to the Cochrane risk of bias framework [29].

Table 1.
Summary of the included studies.
Table 2.
The risk of bias assessment of the included studies according to the Cochrane risk of bias framework [28].
4. Discussion
The aim of the current review is to determine if current ACL secondary prevention training has a positive influence on the re-injury rate, the clinical or functional outcomes, or the risk of re-injury in athletes. The principal findings of the current systematic review are as follows: (1) the available literature related to secondary ACL prevention in athletes is scarce; (2) the level of evidence of the existing literature is diversified; (3) most of the studies investigated if secondary prevention may be effective in modifying the risk factors of ACL re-injury rather than to reduce the re-injury rates; (4) the effectiveness of secondary prevention on modifying the risk factors of ACL re-injury in athletes is controversial; (5) the existing evidence suggests that neuromuscular training, eccentric strengthening, and plyometric exercises may improve biomechanical, functional, and psychological outcomes, and knee proprioception in athletes after ACLR and rehabilitation, which is similar to the current findings of a primary ACL prevention programme; and (6) there is no evidence that a secondary injury prevention program can accelerate the regaining of gait symmetry after ACLR.
The existing literature mainly focuses on the risk factors that contribute to an ACL injury, primary injury prevention programmes, surgical techniques, and rehabilitation after ACLR [38]. The available literature related to secondary ACL prevention in athletes is scarce, while the quality and level of evidence are diversified. There are limited randomised trials available, while most literature available are cohort studies or pilot studies, with a lower level of evidence (level II or III evidence) [39,40,41,42,43,44,45,46]. As cohort studies or pilot studies may potentially have a higher risk of bias compared with randomised trials, it would be difficult to interpret and evaluate the effects of interventions with randomised trials [47]. Therefore, the current review included only randomised trials (level I or II evidence).
In addition, most existing literature reported the influence of secondary prevention on the modification of the risk factors of ACL re-injury rather than the re-injury rates. Two papers reported the re-injury rates after participating in a secondary ACL prevention programme [48,49]. However, both papers were secondary analyses and were excluded from the current review. In the nine included studies, there was no report of the re-injury rate. As the modification of ACL re-injury risk factors may not directly relate to the re-injury rate or the risk of re-injury, more research is needed in the future to investigate the effectiveness of secondary ACL prevention on reducing the re-injury rate.
In the nine included studies, the risk factors they aimed to modify and the exercise approach they used varied from one another. Therefore, the effectiveness of secondary prevention on modifying the risk factors of ACL re-injury is controversial, depending on the specific risk factors they were looking into, and the exercise approaches they used. The risk factors that the included studies focused on were (1) impaired neuromuscular control, knee stability, and proprioception loss; (2) asymmetry in muscle strength and functional performance; (3) psychological response; and (4) gait asymmetry.
Six studies looked into neuromuscular control, knee stability, proprioception, and muscular and functional recovery [20,31,34,35,36,37]. One of the six studies investigated if the clinical and functional outcomes could be different for athletes participating in a secondary prevention programme or a secondary prevention programme plus perturbation training [20]. They found no clinically meaningful differences between the two groups, but there was no report on the effectiveness of either group on improving the clinical or functional outcomes. Another study found that a running retraining programme did not appear to influence the knee’s muscular and functional recovery [37]. The random sequence generation, allocation concealment, and blinding of outcome assessment were not documented in the above study, so the risk of bias was unclear. The remaining four studies reported the positive impacts of neuromuscular training towards neuromuscular control, knee dynamic stability, proprioception, and muscular and functional recovery [31,34,35,36], while Kasmi et al. (2021) reported a combination of eccentric and plyometric exercises may be the most effective to stimulate positive changes in the above outcomes. This may indicate that a specific neuromuscular training including strengthening and plyometric exercises may be essential to promote a positive neuromuscular and functional recovery, while solely a sports-specific training itself may be insufficient in promoting neuromuscular and functional improvement in athletes after ACLR and a traditional rehabilitation.
Regarding psychological responses, factors such as fear of re-injury, confidence, self-efficacy, and psychological readiness to return to sports were potential barriers for athletes after ACLR [50]. One of the nine studies mentioned that eccentric and plyometric exercises were able to improve the psychological outcomes [35]. They found that the combination of the two types of exercises was able to induce a greater improvement in the psychological status and level of confidence of athletes. However, the randomisation process may be potentially biased as the group allocation was realised by adjusting the BMI, age, and sex of the study participants. Multiple meta-analyses have found that strengthening and plyometric exercises were effective in preventing primary ACL injuries [25,26,27]. The current review suggested that these exercises may not only be effective in preventing a primary ACL injury, but also effective in influencing the risk factors of a re-injury, such as limb asymmetries, muscle imbalance, impaired proprioception and knee position sense, and psychological factors. In other words, a primary prevention programme may also be used for a secondary prevention purpose, especially when secondary prevention programmes are not widely developed nowadays.
Regarding gait asymmetries, three studies investigated if a secondary prevention programme or a secondary prevention programme plus perturbation training is effective in improving walking mechanics [30,32,33]. All of the three studies used a programme called ACL-SPORTS, which included muscle strengthening exercises, agility drills, balance exercises, dynamic sport-related tasks, and perturbation training. They all found that both groups were not effective in restoring gait symmetry in the short term, while gait asymmetries mostly resolved after 2 years post-ACLR, regardless of the intervention group. It is worth noting that the potential risk of bias may be high in Capin et al. (2017), as the random sequence generation, allocation concealment, and blinding procedures were not documented. As gait impairments may be present even in the absence of clinical or functional deficits [30,51,52], gait symmetries may not be a strong indicator or risk factor of an ACL re-injury. As gait may vary from time to time, gait assessment may not be as reliable and functional as other outcome measures, such as functional tests.
The primary strength of the current review is that the level of evidence is high as only randomised trials were included. This may potentially reduce the risk of bias. In addition, there is confidence that all adequate studies have been identified because the reference lists of all included and excluded studies have been screened or searched.
The current review also has some limitations. To start with, the participants of the included studies tended to share particular characteristics (very active in sports participation before the injury, achieved good recovery over the ACLR limb, a high percentage of muscle strength symmetry, and participating in sports involving frequent cutting and pivoting). In addition, the number of male and female athletes was unequal in the included studies (253 males, 94 females). Therefore, the results of the current review may not be generalisable to other populations such as athletes who have poor recovery and a higher extent of limb asymmetries after ACLR. Another limitation of the current review is that the ACL secondary prevention programmes included in the study are not sports specific. This is mainly limited by the scarcity of literature available in this field.
5. Conclusions
Given the scarcity of the literature available related to secondary ACL prevention in athletes with the diversified level of evidence and lack of reports towards the re-injury rate, more research is needed in the future regarding the effectiveness of secondary ACL prevention on reducing the re-injury rates. In addition, more research should be conducted investigating if sports-specific secondary prevention programmes may positively influence the ACL re-injury rates and modify the specific risk factors of re-injury in different sports. The effectiveness of secondary prevention in modifying the risk factors of ACL re-injury in athletes is controversial. The existing evidence suggests that neuromuscular training, eccentric strengthening, and plyometric exercises may have a positive impact on the biomechanical, functional, and psychological outcomes in athletes, while secondary prevention programmes may be ineffective in influencing gait asymmetries. This may indicate that a primary ACL prevention programme may also be valid in secondary ACL injury prevention.
Author Contributions
Conceptualization, C.-Y.W., K.-M.M. and S.-H.Y.; methodology, C.-Y.W. and K.-M.M.; formal analysis and data curation, C.-Y.W.; writing—original draft preparation, C.-Y.W. and K.-M.M.; writing—review and editing, C.-Y.W., K.-M.M. and S.-H.Y.; supervision, S.-H.Y.; project administration, C.-Y.W., K.-M.M. and S.-H.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Thank you to the Master of Science in Sports Medicine & Health Science programme, The Chinese University of Hong Kong.
Conflicts of Interest
The authors declare no conflict of interest.
References
- McLean, S.G.; Huang, X.; Van Den Bogert, A.J. Association between lower extremity posture at contact and peak knee valgus moment during sidestepping: Implications for ACL injury. Clin. Biomech. 2005, 20, 863–870. [Google Scholar] [CrossRef]
- Yu, B.; Garrett, W.E. Mechanisms of non-contact ACL injuries. Br. J. Sport. Med. 2007, 41, i47–i51. [Google Scholar] [CrossRef]
- Kaeding, C.C.; Léger-St-Jean, B.; Magnussen, R.A. Epidemiology and diagnosis of anterior cruciate ligament injuries. Clin. Sport. Med. 2017, 36, 1–8. [Google Scholar] [CrossRef]
- Wyatt, R.W.; Inacio, M.C.; Liddle, K.D.; Maletis, G.B. Prevalence and incidence of cartilage injuries and meniscus tears in patients who underwent both primary and revision anterior cruciate ligament reconstructions. Am. J. Sport. Med. 2014, 42, 1841–1846. [Google Scholar] [CrossRef] [PubMed]
- Barenius, B.; Ponzer, S.; Shalabi, A.; Bujak, R.; Norlén, L.; Eriksson, K. Increased risk of osteoarthritis after anterior cruciate ligament reconstruction: A 14-year follow-up study of a randomized controlled trial. Am. J. Sport. Med. 2014, 42, 1049–1057. [Google Scholar] [CrossRef]
- Suter, L.G.; Smith, S.R.; Katz, J.N.; Englund, M.; Hunter, D.J.; Frobell, R.; Losina, E. Projecting lifetime risk of symptomatic knee osteoarthritis and total knee replacement in individuals sustaining a complete anterior cruciate ligament tear in early adulthood. Arthritis Care Res. 2017, 69, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Filbay, S.R.; Culvenor, A.G.; Ackerman, I.N.; Russell, T.G.; Crossley, K.M. Quality of life in anterior cruciate ligament-deficient individuals: A systematic review and meta-analysis. Br. J. Sport. Med. 2015, 49, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Spindler, K.P.; Wright, R.W. Anterior cruciate ligament tear. New Engl. J. Med. 2008, 359, 2135–2142. [Google Scholar] [CrossRef]
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to the preinjury level of competitive sport after anterior cruciate ligament reconstruction surgery: Two-thirds of patients have not returned by 12 months after surgery. Am. J. Sport. Med. 2011, 39, 538–543. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: An updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br. J. Sport. Med. 2014, 48, 1543–1552. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, A.J.; Grandhi, R.K.; Schneider, D.K.; Stanfield, D.; Webster, K.E.; Myer, G.D. Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: A systematic review and meta-analysis. Am. J. Sport. Med. 2016, 44, 1861–1876. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.M.; Pareek, A.; Krych, A.J.; Hewett, T.E.; Levy, B.A.; Stuart, M.J.; Dahm, D.L. Are female soccer players at an increased risk of second anterior cruciate ligament injury compared with their athletic peers? Am. J. Sport. Med. 2016, 44, 2492–2498. [Google Scholar] [CrossRef] [PubMed]
- Grindem, H.; Snyder-Mackler, L.; Moksnes, H.; Engebretsen, L.; Risberg, M.A. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: The Delaware-Oslo ACL cohort study. Br. J. Sport. Med. 2016, 50, 804–808. [Google Scholar] [CrossRef]
- Kay, J.; Memon, M.; Marx, R.G.; Peterson, D.; Simunovic, N.; Ayeni, O.R. Over 90% of children and adolescents return to sport after anterior cruciate ligament reconstruction: A systematic review and meta-analysis. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 1019–1036. [Google Scholar] [CrossRef] [PubMed]
- Shelbourne, K.D.; Gray, T.; Haro, M. Incidence of subsequent injury to either knee within 5 years after anterior cruciate ligament reconstruction with patellar tendon autograft. Am. J. Sport. Med. 2009, 37, 246–251. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A. Exploring the high reinjury rate in younger patients undergoing anterior cruciate ligament reconstruction. Am. J. Sport. Med. 2016, 44, 2827–2832. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A.; Leigh, W.B.; Richmond, A.K. Younger patients are at increased risk for graft rupture and contralateral injury after anterior cruciate ligament reconstruction. Am. J. Sport. Med. 2014, 42, 641–647. [Google Scholar] [CrossRef]
- Paterno, M.V.; Rauh, M.J.; Schmitt, L.C.; Ford, K.R.; Hewett, T.E. Incidence of contralateral and ipsilateral anterior cruciate ligament (ACL) injury after primary ACL reconstruction and return to sport. Clin. J. Sport Med. 2012, 22, 116. [Google Scholar] [CrossRef]
- Schmitt, L.C.; Paterno, M.V.; Ford, K.R.; Myer, G.D.; Hewett, T.E. Strength asymmetry and landing mechanics at return to sport after ACL reconstruction. Med. Sci. Sport. Exerc. 2015, 47, 1426. [Google Scholar] [CrossRef]
- Arundale, A.J.; Cummer, K.; Capin, J.J.; Zarzycki, R.; Snyder-Mackler, L. Report of the clinical and functional primary outcomes in men of the ACL-SPORTS trial: Similar outcomes in men receiving secondary prevention with and without perturbation training 1 and 2 years after ACL reconstruction. Clin. Orthop. Relat. Res. 2017, 475, 2523–2534. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fear of re-injury in people who have returned to sport following anterior cruciate ligament reconstruction surgery. J. Sci. Med. Sport 2012, 15, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Adhya, B.; Dhillon, M.S.; Saini, A. A study on the role of proprioceptive training in non operative ACL injury rehabilitation. Quadriceps Femoris Strength Train. Eff. Neuromuscul. Electr. Stimul. Isometric Exerc. Osteoarthr. Knee 2015, 9, 3232. [Google Scholar] [CrossRef]
- Arhos, E.K.; Capin, J.J.; Buchanan, T.S.; Snyder-Mackler, L. Quadriceps Strength Symmetry Does Not Modify Gait Mechanics after ACL Reconstruction, Rehabilitation and Return-to-Sport Training. Am. J. Sport. Med. 2021, 49, 417. [Google Scholar] [CrossRef] [PubMed]
- Marotta, N.; Demeco, A.; Moggio, L.; Isabello, L.; Iona, T. Correlation between dynamic knee valgus and quadriceps activation time in female athletes. J. Phys. Educ. Sport 2020, 20, 2508–2512. [Google Scholar]
- Taylor, J.B.; Waxman, J.P.; Richter, S.J.; Shultz, S.J. Evaluation of the effectiveness of anterior cruciate ligament injury prevention programme training components: A systematic review and meta-analysis. Br. J. Sport. Med. 2015, 49, 79–87. [Google Scholar] [CrossRef]
- Sugimoto, D.; Myer, G.D.; Foss, K.D.B.; Pepin, M.J.; Micheli, L.J.; Hewett, T.E. Critical components of neuromuscular training to reduce ACL injury risk in female athletes: Meta-regression analysis. Br. J. Sport. Med. 2016, 50, 1259–1266. [Google Scholar] [CrossRef]
- Arundale, A.J.; Bizzini, M.; Giordano, A.; Hewett, T.E.; Logerstedt, D.S.; Mandelbaum, B.; Scalzitti, D.A.; Silvers-Granelli, H.; Snyder-Mackler, L.; Altman, R.D.; et al. Exercise-based knee and anterior cruciate ligament injury prevention: Clinical practice guidelines linked to the international classification of functioning, disability and health from the academy of orthopaedic physical therapy and the American Academy of sports physical therapy. J. Orthop. Sport. Phys. Ther. 2018, 48, A1–A42. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br. Med. J. 2021, 88, 105906. [Google Scholar]
- Cochrane Developmental, Psychosocial and Learning Problems. Data Collection form for Intervention Reviews: RCTs and Non-RCTs; Cochrane Developmental, Psychosocial and Learning Problems: London, UK, 2014. [Google Scholar]
- Capin, J.J.; Zarzycki, R.; Arundale, A.; Cummer, K.; Snyder-Mackler, L. Report of the primary outcomes for gait mechanics in men of the ACL-SPORTS trial: Secondary prevention with and without perturbation training does not restore gait symmetry in men 1 or 2 years after ACL reconstruction. Clin. Orthop. Relat. Res. 2017, 475, 2513–2522. [Google Scholar] [CrossRef]
- Ghaderi, M.; Letafatkar, A.; Thomas, A.C.; Keyhani, S. Effects of a neuromuscular training program using external focus attention cues in male athletes with anterior cruciate ligament reconstruction: A randomized clinical trial. BMC Sport. Sci. Med. Rehabil. 2021, 13, 49. [Google Scholar] [CrossRef]
- Capin, J.J.; Zarzycki, R.; Ito, N.; Khandha, A.; Dix, C.; Manal, K.; Buchanan, T.S.; Snyder-Mackler, L. Gait mechanics in women of the ACL-SPORTS randomized control trial: Interlimb symmetry improves over time regardless of treatment group. J. Orthop. Res. 2019, 37, 1743–1753. [Google Scholar] [CrossRef] [PubMed]
- Capin, J.J.; Khandha, A.; Zarzycki, R.; Arundale, A.J.; Ziegler, M.L.; Manal, K.; Buchanan, T.S.; Snyder-Mackler, L. Gait mechanics and tibiofemoral loading in men of the ACL-SPORTS randomized control trial. J. Orthop. Res. 2018, 36, 2364–2372. [Google Scholar] [CrossRef] [PubMed]
- Ghaderi, M.; Letafatkar, A.; Almonroeder, T.G.; Keyhani, S. Neuromuscular training improves knee proprioception in athletes with a history of anterior cruciate ligament reconstruction: A randomized controlled trial. Clin. Biomech. 2020, 80, 105157. [Google Scholar] [CrossRef]
- Kasmi, S.; Zouhal, H.; Hammami, R.; Clark, C.C.T.; Hackney, A.C.; Hammami, A.; Chtara, M.; Chortane, S.G.; Salah, F.Z.B.; Granacher, U.; et al. The effects of eccentric and plyometric training programs and their combination on stability and the functional performance in the post-ACL-surgical rehabilitation period of elite female athletes. Front. Physiol. 2021, 12, 954. [Google Scholar] [CrossRef] [PubMed]
- Elias, A.R.; Harris, K.J.; LaStayo, P.C.; Mizner, R.L. Clinical efficacy of jump training augmented with body weight support after ACL reconstruction: A randomized controlled trial. Am. J. Sport. Med. 2018, 46, 1650–1660. [Google Scholar] [CrossRef]
- Dauty, M.; Menu, P.; Dubois, C. Effects of running retraining after knee anterior cruciate ligament reconstruction. Ann. Phys. Rehabil. Med. 2010, 53, 150–161. [Google Scholar] [CrossRef]
- Arundale, A.J.H.; Silvers-Granelli, H.J.; Myklebust, G. ACL injury prevention: Where have we come from and where are we going? J. Orthop. Res. 2021, 40, 43–54. [Google Scholar] [CrossRef]
- Nyland, J.; Greene, J.; Carter, S.; Brey, J.; Krupp, R.; Caborn, D. Return to sports bridge program improves outcomes, decreases ipsilateral knee re-injury and contralateral knee injury rates post-ACL reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 3676–3685. [Google Scholar] [CrossRef]
- Nagelli, C.; Wordeman, S.; Di Stasi, S.; Hoffman, J.; Marulli, T.; Hewett, T.E. Biomechanical deficits at the hip in athletes with ACL reconstruction are ameliorated with neuromuscular training. Am. J. Sport. Med. 2018, 46, 2772–2779. [Google Scholar] [CrossRef]
- Nagelli, C.; Di Stasi, S.; Tatarski, R.; Chen, A.; Wordeman, S.; Hoffman, J.; Hewett, T.E. Neuromuscular Training Improves Self-Reported Function and Single-Leg Landing Hip Biomechanics in Athletes after Anterior Cruciate Ligament Reconstruction. Orthop. J. Sport. Med. 2020, 8, 1–7. [Google Scholar] [CrossRef]
- Nagelli, C.V.; Wordeman, S.C.; Di Stasi, S.; Hoffman, J.; Marulli, T.; Hewett, T.E. Neuromuscular Training Improves Biomechanical Deficits at the Knee in Anterior Cruciate Ligament Reconstructed-Athletes. Clin. J. Sport Med. 2019, 31, 113. [Google Scholar] [CrossRef]
- Nagelli, C.V.; Di Stasi, S.; Wordeman, S.C.; Chen, A.; Tatarski, R.; Hoffman, J.; Hewett, T.E. Knee biomechanical deficits during a single-leg landing task are addressed with neuromuscular training in anterior cruciate ligament-reconstructed athletes. Clin. J. Sport Med. 2019, 31, e347–e353. [Google Scholar] [CrossRef]
- Capin, J.J.; Failla, M.; Zarzycki, R.; Dix, C.; Johnson, J.L.; Smith, A.H.; Risberg, M.A.; Huston, L.J.; Spindler, K.P.; Snyder-Mackler, L. Superior 2-year functional outcomes among young female athletes after ACL reconstruction in 10 Return-to-Sport training sessions: Comparison of ACL-SPORTS randomized controlled trial with Delaware-Oslo and moon cohorts. Orthop. J. Sport. Med. 2019, 7, 2325967119861311. [Google Scholar] [CrossRef]
- Baez, S.; Cormier, M.; Andreatta, R.; Gribble, P.; Hoch, J.M. Implementation of In vivo exposure therapy to decrease injury-related fear in females with a history of ACL-Reconstruction: A pilot study. Phys. Ther. Sport 2021, 52, 217–223. [Google Scholar] [CrossRef]
- Meierbachtol, A.; Obermeier, M.; Yungtum, W.; Bottoms, J.; Paur, E.; Nelson, B.J.; Tompkins, M.; Chmielewski, T.L. Advanced training enhances readiness to return to sport after anterior cruciate ligament reconstruction. J. Orthop. Res. 2021, 40, 191–199. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2021; Version 6.2; Available online: www.training.cochrane.org/handbook (accessed on 22 February 2022).
- Arundale, A.; Capin, J.J.; Zarzycki, R.; Smith, A.H.; Snyder-Mackler, L. Two Year ACL Reinjury Rate of 2.5%: Outcomes Report of The Men in a Secondary ACL Injury Prevention Program (ACL-SPORTS). Int. J. Sport. Phys. Ther. 2018, 13, 422–431. [Google Scholar] [CrossRef]
- Johnson, J.L.; Capin, J.J.; Arundale, A.; Zarzycki, R.; Smith, A.H.; Snyder-Mackler, L. A Secondary Injury Prevention Program May Decrease Contralateral Anterior Cruciate Ligament Injuries in Female Athletes: 2-Year Injury Rates in the ACL-SPORTS Randomized Controlled Trial. J. Orthop. Sport. Phys. Ther. 2020, 50, 523–530. [Google Scholar] [CrossRef]
- Zarzycki, R.; Arhos, E.; Failla, M.; Capin, J.; Smith, A.H.; Snyder-Mackler, L. Association of the Psychological Response to the ACL-SPORTS Training Program and Self-reported Function at 2 Years after Anterior Cruciate Ligament Reconstruction. Am. J. Sport. Med. 2021, 49, 3495–3501. [Google Scholar] [CrossRef]
- Holm, I.; Øiestad, B.E.; Risberg, M.A.; Aune, A.K. No Difference in Knee Function or Prevalence of Osteoarthritis after Reconstruction of the Anterior Cruciate Ligament with 4-Strand Hamstring Autograft versus Patellar Tendon—Bone Autograft: A Randomized Study with 10-Year Follow-up. Am. J. Sport. Med. 2010, 38, 448–454. [Google Scholar] [CrossRef]
- White, K.; Logerstedt, D.; Snyder-Mackler, L. Gait asymmetries persist 1 year after anterior cruciate ligament reconstruction. Orthop. J. Sport. Med. 2013, 1, 2325967113496967. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).