
Secondary Anterior Cruciate Ligament Injury Prevention Training in Athletes: What Is the Missing Link?


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection
2.3. Data Analysis
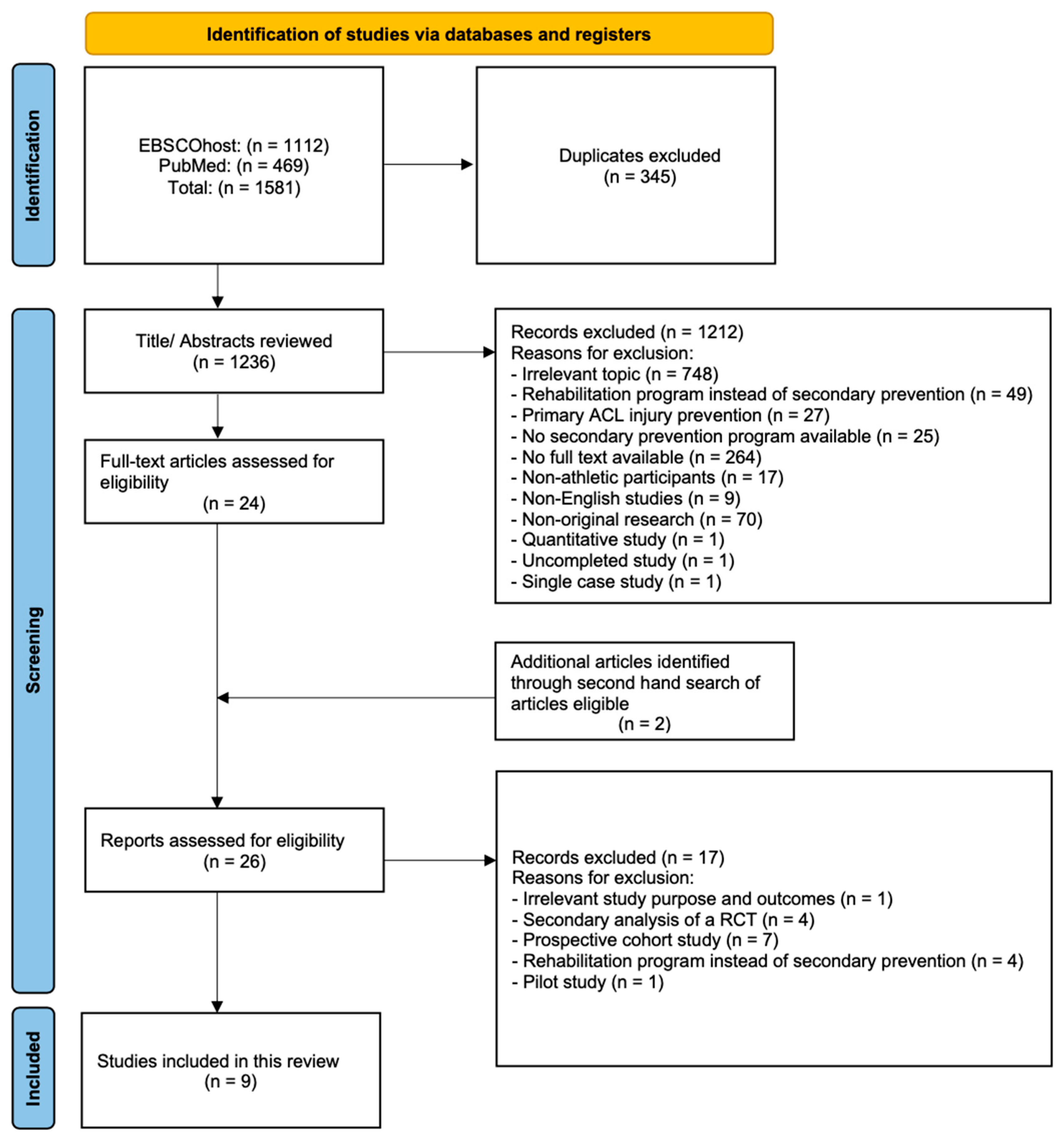
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McLean, S.G.; Huang, X.; Van Den Bogert, A.J. Association between lower extremity posture at contact and peak knee valgus moment during sidestepping: Implications for ACL injury. Clin. Biomech. 2005, 20, 863–870. [Google Scholar] [CrossRef]
- Yu, B.; Garrett, W.E. Mechanisms of non-contact ACL injuries. Br. J. Sport. Med. 2007, 41, i47–i51. [Google Scholar] [CrossRef]
- Kaeding, C.C.; Léger-St-Jean, B.; Magnussen, R.A. Epidemiology and diagnosis of anterior cruciate ligament injuries. Clin. Sport. Med. 2017, 36, 1–8. [Google Scholar] [CrossRef]
- Wyatt, R.W.; Inacio, M.C.; Liddle, K.D.; Maletis, G.B. Prevalence and incidence of cartilage injuries and meniscus tears in patients who underwent both primary and revision anterior cruciate ligament reconstructions. Am. J. Sport. Med. 2014, 42, 1841–1846. [Google Scholar] [CrossRef] [PubMed]
- Barenius, B.; Ponzer, S.; Shalabi, A.; Bujak, R.; Norlén, L.; Eriksson, K. Increased risk of osteoarthritis after anterior cruciate ligament reconstruction: A 14-year follow-up study of a randomized controlled trial. Am. J. Sport. Med. 2014, 42, 1049–1057. [Google Scholar] [CrossRef]
- Suter, L.G.; Smith, S.R.; Katz, J.N.; Englund, M.; Hunter, D.J.; Frobell, R.; Losina, E. Projecting lifetime risk of symptomatic knee osteoarthritis and total knee replacement in individuals sustaining a complete anterior cruciate ligament tear in early adulthood. Arthritis Care Res. 2017, 69, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Filbay, S.R.; Culvenor, A.G.; Ackerman, I.N.; Russell, T.G.; Crossley, K.M. Quality of life in anterior cruciate ligament-deficient individuals: A systematic review and meta-analysis. Br. J. Sport. Med. 2015, 49, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Spindler, K.P.; Wright, R.W. Anterior cruciate ligament tear. New Engl. J. Med. 2008, 359, 2135–2142. [Google Scholar] [CrossRef]
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to the preinjury level of competitive sport after anterior cruciate ligament reconstruction surgery: Two-thirds of patients have not returned by 12 months after surgery. Am. J. Sport. Med. 2011, 39, 538–543. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: An updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br. J. Sport. Med. 2014, 48, 1543–1552. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, A.J.; Grandhi, R.K.; Schneider, D.K.; Stanfield, D.; Webster, K.E.; Myer, G.D. Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: A systematic review and meta-analysis. Am. J. Sport. Med. 2016, 44, 1861–1876. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.M.; Pareek, A.; Krych, A.J.; Hewett, T.E.; Levy, B.A.; Stuart, M.J.; Dahm, D.L. Are female soccer players at an increased risk of second anterior cruciate ligament injury compared with their athletic peers? Am. J. Sport. Med. 2016, 44, 2492–2498. [Google Scholar] [CrossRef] [PubMed]
- Grindem, H.; Snyder-Mackler, L.; Moksnes, H.; Engebretsen, L.; Risberg, M.A. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: The Delaware-Oslo ACL cohort study. Br. J. Sport. Med. 2016, 50, 804–808. [Google Scholar] [CrossRef]
- Kay, J.; Memon, M.; Marx, R.G.; Peterson, D.; Simunovic, N.; Ayeni, O.R. Over 90% of children and adolescents return to sport after anterior cruciate ligament reconstruction: A systematic review and meta-analysis. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 1019–1036. [Google Scholar] [CrossRef] [PubMed]
- Shelbourne, K.D.; Gray, T.; Haro, M. Incidence of subsequent injury to either knee within 5 years after anterior cruciate ligament reconstruction with patellar tendon autograft. Am. J. Sport. Med. 2009, 37, 246–251. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A. Exploring the high reinjury rate in younger patients undergoing anterior cruciate ligament reconstruction. Am. J. Sport. Med. 2016, 44, 2827–2832. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A.; Leigh, W.B.; Richmond, A.K. Younger patients are at increased risk for graft rupture and contralateral injury after anterior cruciate ligament reconstruction. Am. J. Sport. Med. 2014, 42, 641–647. [Google Scholar] [CrossRef]
- Paterno, M.V.; Rauh, M.J.; Schmitt, L.C.; Ford, K.R.; Hewett, T.E. Incidence of contralateral and ipsilateral anterior cruciate ligament (ACL) injury after primary ACL reconstruction and return to sport. Clin. J. Sport Med. 2012, 22, 116. [Google Scholar] [CrossRef]
- Schmitt, L.C.; Paterno, M.V.; Ford, K.R.; Myer, G.D.; Hewett, T.E. Strength asymmetry and landing mechanics at return to sport after ACL reconstruction. Med. Sci. Sport. Exerc. 2015, 47, 1426. [Google Scholar] [CrossRef]
- Arundale, A.J.; Cummer, K.; Capin, J.J.; Zarzycki, R.; Snyder-Mackler, L. Report of the clinical and functional primary outcomes in men of the ACL-SPORTS trial: Similar outcomes in men receiving secondary prevention with and without perturbation training 1 and 2 years after ACL reconstruction. Clin. Orthop. Relat. Res. 2017, 475, 2523–2534. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fear of re-injury in people who have returned to sport following anterior cruciate ligament reconstruction surgery. J. Sci. Med. Sport 2012, 15, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Adhya, B.; Dhillon, M.S.; Saini, A. A study on the role of proprioceptive training in non operative ACL injury rehabilitation. Quadriceps Femoris Strength Train. Eff. Neuromuscul. Electr. Stimul. Isometric Exerc. Osteoarthr. Knee 2015, 9, 3232. [Google Scholar] [CrossRef]
- Arhos, E.K.; Capin, J.J.; Buchanan, T.S.; Snyder-Mackler, L. Quadriceps Strength Symmetry Does Not Modify Gait Mechanics after ACL Reconstruction, Rehabilitation and Return-to-Sport Training. Am. J. Sport. Med. 2021, 49, 417. [Google Scholar] [CrossRef] [PubMed]
- Marotta, N.; Demeco, A.; Moggio, L.; Isabello, L.; Iona, T. Correlation between dynamic knee valgus and quadriceps activation time in female athletes. J. Phys. Educ. Sport 2020, 20, 2508–2512. [Google Scholar]
- Taylor, J.B.; Waxman, J.P.; Richter, S.J.; Shultz, S.J. Evaluation of the effectiveness of anterior cruciate ligament injury prevention programme training components: A systematic review and meta-analysis. Br. J. Sport. Med. 2015, 49, 79–87. [Google Scholar] [CrossRef]
- Sugimoto, D.; Myer, G.D.; Foss, K.D.B.; Pepin, M.J.; Micheli, L.J.; Hewett, T.E. Critical components of neuromuscular training to reduce ACL injury risk in female athletes: Meta-regression analysis. Br. J. Sport. Med. 2016, 50, 1259–1266. [Google Scholar] [CrossRef]
- Arundale, A.J.; Bizzini, M.; Giordano, A.; Hewett, T.E.; Logerstedt, D.S.; Mandelbaum, B.; Scalzitti, D.A.; Silvers-Granelli, H.; Snyder-Mackler, L.; Altman, R.D.; et al. Exercise-based knee and anterior cruciate ligament injury prevention: Clinical practice guidelines linked to the international classification of functioning, disability and health from the academy of orthopaedic physical therapy and the American Academy of sports physical therapy. J. Orthop. Sport. Phys. Ther. 2018, 48, A1–A42. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br. Med. J. 2021, 88, 105906. [Google Scholar]
- Cochrane Developmental, Psychosocial and Learning Problems. Data Collection form for Intervention Reviews: RCTs and Non-RCTs; Cochrane Developmental, Psychosocial and Learning Problems: London, UK, 2014. [Google Scholar]
- Capin, J.J.; Zarzycki, R.; Arundale, A.; Cummer, K.; Snyder-Mackler, L. Report of the primary outcomes for gait mechanics in men of the ACL-SPORTS trial: Secondary prevention with and without perturbation training does not restore gait symmetry in men 1 or 2 years after ACL reconstruction. Clin. Orthop. Relat. Res. 2017, 475, 2513–2522. [Google Scholar] [CrossRef]
- Ghaderi, M.; Letafatkar, A.; Thomas, A.C.; Keyhani, S. Effects of a neuromuscular training program using external focus attention cues in male athletes with anterior cruciate ligament reconstruction: A randomized clinical trial. BMC Sport. Sci. Med. Rehabil. 2021, 13, 49. [Google Scholar] [CrossRef]
- Capin, J.J.; Zarzycki, R.; Ito, N.; Khandha, A.; Dix, C.; Manal, K.; Buchanan, T.S.; Snyder-Mackler, L. Gait mechanics in women of the ACL-SPORTS randomized control trial: Interlimb symmetry improves over time regardless of treatment group. J. Orthop. Res. 2019, 37, 1743–1753. [Google Scholar] [CrossRef] [PubMed]
- Capin, J.J.; Khandha, A.; Zarzycki, R.; Arundale, A.J.; Ziegler, M.L.; Manal, K.; Buchanan, T.S.; Snyder-Mackler, L. Gait mechanics and tibiofemoral loading in men of the ACL-SPORTS randomized control trial. J. Orthop. Res. 2018, 36, 2364–2372. [Google Scholar] [CrossRef] [PubMed]
- Ghaderi, M.; Letafatkar, A.; Almonroeder, T.G.; Keyhani, S. Neuromuscular training improves knee proprioception in athletes with a history of anterior cruciate ligament reconstruction: A randomized controlled trial. Clin. Biomech. 2020, 80, 105157. [Google Scholar] [CrossRef]
- Kasmi, S.; Zouhal, H.; Hammami, R.; Clark, C.C.T.; Hackney, A.C.; Hammami, A.; Chtara, M.; Chortane, S.G.; Salah, F.Z.B.; Granacher, U.; et al. The effects of eccentric and plyometric training programs and their combination on stability and the functional performance in the post-ACL-surgical rehabilitation period of elite female athletes. Front. Physiol. 2021, 12, 954. [Google Scholar] [CrossRef] [PubMed]
- Elias, A.R.; Harris, K.J.; LaStayo, P.C.; Mizner, R.L. Clinical efficacy of jump training augmented with body weight support after ACL reconstruction: A randomized controlled trial. Am. J. Sport. Med. 2018, 46, 1650–1660. [Google Scholar] [CrossRef]
- Dauty, M.; Menu, P.; Dubois, C. Effects of running retraining after knee anterior cruciate ligament reconstruction. Ann. Phys. Rehabil. Med. 2010, 53, 150–161. [Google Scholar] [CrossRef]
- Arundale, A.J.H.; Silvers-Granelli, H.J.; Myklebust, G. ACL injury prevention: Where have we come from and where are we going? J. Orthop. Res. 2021, 40, 43–54. [Google Scholar] [CrossRef]
- Nyland, J.; Greene, J.; Carter, S.; Brey, J.; Krupp, R.; Caborn, D. Return to sports bridge program improves outcomes, decreases ipsilateral knee re-injury and contralateral knee injury rates post-ACL reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 3676–3685. [Google Scholar] [CrossRef]
- Nagelli, C.; Wordeman, S.; Di Stasi, S.; Hoffman, J.; Marulli, T.; Hewett, T.E. Biomechanical deficits at the hip in athletes with ACL reconstruction are ameliorated with neuromuscular training. Am. J. Sport. Med. 2018, 46, 2772–2779. [Google Scholar] [CrossRef]
- Nagelli, C.; Di Stasi, S.; Tatarski, R.; Chen, A.; Wordeman, S.; Hoffman, J.; Hewett, T.E. Neuromuscular Training Improves Self-Reported Function and Single-Leg Landing Hip Biomechanics in Athletes after Anterior Cruciate Ligament Reconstruction. Orthop. J. Sport. Med. 2020, 8, 1–7. [Google Scholar] [CrossRef]
- Nagelli, C.V.; Wordeman, S.C.; Di Stasi, S.; Hoffman, J.; Marulli, T.; Hewett, T.E. Neuromuscular Training Improves Biomechanical Deficits at the Knee in Anterior Cruciate Ligament Reconstructed-Athletes. Clin. J. Sport Med. 2019, 31, 113. [Google Scholar] [CrossRef]
- Nagelli, C.V.; Di Stasi, S.; Wordeman, S.C.; Chen, A.; Tatarski, R.; Hoffman, J.; Hewett, T.E. Knee biomechanical deficits during a single-leg landing task are addressed with neuromuscular training in anterior cruciate ligament-reconstructed athletes. Clin. J. Sport Med. 2019, 31, e347–e353. [Google Scholar] [CrossRef]
- Capin, J.J.; Failla, M.; Zarzycki, R.; Dix, C.; Johnson, J.L.; Smith, A.H.; Risberg, M.A.; Huston, L.J.; Spindler, K.P.; Snyder-Mackler, L. Superior 2-year functional outcomes among young female athletes after ACL reconstruction in 10 Return-to-Sport training sessions: Comparison of ACL-SPORTS randomized controlled trial with Delaware-Oslo and moon cohorts. Orthop. J. Sport. Med. 2019, 7, 2325967119861311. [Google Scholar] [CrossRef]
- Baez, S.; Cormier, M.; Andreatta, R.; Gribble, P.; Hoch, J.M. Implementation of In vivo exposure therapy to decrease injury-related fear in females with a history of ACL-Reconstruction: A pilot study. Phys. Ther. Sport 2021, 52, 217–223. [Google Scholar] [CrossRef]
- Meierbachtol, A.; Obermeier, M.; Yungtum, W.; Bottoms, J.; Paur, E.; Nelson, B.J.; Tompkins, M.; Chmielewski, T.L. Advanced training enhances readiness to return to sport after anterior cruciate ligament reconstruction. J. Orthop. Res. 2021, 40, 191–199. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2021; Version 6.2; Available online: www.training.cochrane.org/handbook (accessed on 22 February 2022).
- Arundale, A.; Capin, J.J.; Zarzycki, R.; Smith, A.H.; Snyder-Mackler, L. Two Year ACL Reinjury Rate of 2.5%: Outcomes Report of The Men in a Secondary ACL Injury Prevention Program (ACL-SPORTS). Int. J. Sport. Phys. Ther. 2018, 13, 422–431. [Google Scholar] [CrossRef]
- Johnson, J.L.; Capin, J.J.; Arundale, A.; Zarzycki, R.; Smith, A.H.; Snyder-Mackler, L. A Secondary Injury Prevention Program May Decrease Contralateral Anterior Cruciate Ligament Injuries in Female Athletes: 2-Year Injury Rates in the ACL-SPORTS Randomized Controlled Trial. J. Orthop. Sport. Phys. Ther. 2020, 50, 523–530. [Google Scholar] [CrossRef]
- Zarzycki, R.; Arhos, E.; Failla, M.; Capin, J.; Smith, A.H.; Snyder-Mackler, L. Association of the Psychological Response to the ACL-SPORTS Training Program and Self-reported Function at 2 Years after Anterior Cruciate Ligament Reconstruction. Am. J. Sport. Med. 2021, 49, 3495–3501. [Google Scholar] [CrossRef]
- Holm, I.; Øiestad, B.E.; Risberg, M.A.; Aune, A.K. No Difference in Knee Function or Prevalence of Osteoarthritis after Reconstruction of the Anterior Cruciate Ligament with 4-Strand Hamstring Autograft versus Patellar Tendon—Bone Autograft: A Randomized Study with 10-Year Follow-up. Am. J. Sport. Med. 2010, 38, 448–454. [Google Scholar] [CrossRef]
- White, K.; Logerstedt, D.; Snyder-Mackler, L. Gait asymmetries persist 1 year after anterior cruciate ligament reconstruction. Orthop. J. Sport. Med. 2013, 1, 2325967113496967. [Google Scholar] [CrossRef]


{kind=link}
| Study | Study Design | Intervention | Description of Participants | ACLR and Post-ACLR Rehabilitation | Intervention Description | Key Outcome Measures | Key Findings |
|---|---|---|---|---|---|---|---|
| [20] | Randomised clinical trial | Compare clinical and functional outcomes of SAP group (strength, agility, plyometric, and secondary prevention treatment) and SAP + PERT group (SAP + perturbation training). |
|
| Duration: 4 weeks Frequency: 2 times a week Type of exercise: SAP: Progressive secondary ACL injury prevention exercises, agility drills, balance, dynamic sport-related tasks, and muscle strengthening exercises. SAP + PERT: All exercises in SAP group augmented with perturbation training. |
| There were no clinically meaningful differences between groups in knee function and self-reported outcome measures. The results indicate that perturbation training may not contribute additional benefit to knee functional or clinical outcomes. |
| [30] | Randomised clinical trial | Compare SAP group and SAP + PERT group with respect to gait mechanics and elimination of gait asymmetries 1 and 2 years after ACLR. |
|
| Duration: 4 weeks Frequency: 2 times a week Type of exercise: SAP: Progressive secondary ACL injury prevention exercises, agility drills, and plyometric exercises. SAP + PERT: All exercises in SAP group plus perturbation training (neuromuscular training requiring selective muscle activation in response to surface perturbations applied by a physical therapist). |
| Both groups were not effective in restoring interlimb symmetry among men 1 or 2 years after ACLR. Although gait asymmetries improved from 1 to 2 years postoperatively, meaningful asymmetries persisted in both groups. |
| [31] | Randomised clinical trial | Examine the effects of a neuromuscular training program that emphasizes external focus of attention cuing on biomechanics, knee proprioception, and patient-reported function. |
|
| Experimental group: Duration: 8 weeks Frequency: 3 times per week for week 1–6 and 2 times per week for week 7–8 Exercises included: double-leg squats, walking lunges, single-leg squats, double-leg drop jumps, single-leg stance on an unstable surface, single-leg standing long jumps. Control group: Duration: 8 weeks Content: Complete routine sport-specific skills training |
| The experimental group demonstrated improvements in landing biomechanics, proprioception, and patient-reported function. The control group demonstrated no changes in any variable over the same period. |
| [32] | Prospective randomised control trial | Compare SAP group and SAP + PERT group with respect to improvements in movement symmetry during walking. |
|
| Duration: 5 weeks Frequency: 2 times a week Exercises included: Nordic hamstrings, standing squats progressing to tuck jumps, drop jumps, triple single leg hopping, agility drills, quadriceps strengthening exercises. Specific to SAP: A sham intervention (the athlete stood on one leg on a stable surface and performed hip flexion against a resistance band with the opposite limb). Specific to SAP + PERT: 10 sessions of perturbation training (~30 min per session). |
| SAP training with and without perturbation training do not meaningfully improve walking mechanics among young female athletes. Asymmetrical gait mechanics persist to a large degree until 2 years after ACLR, long after patients have achieved symmetrical strength and functional performance and have returned to sports. |
| [33] | Prospective randomised control trial | Compare SAP group and SAP + PERT group with respect to tibiofemoral loading, muscle forces, and the immediate before and after intervention knee kinematics and kinetics during walking. |
|
| Duration: 5 weeks Frequency: 2 times a week Exercises included: Nordic hamstrings, standing squats progressing to tuck jumps, drop jumps, triple single leg hopping, agility drills, quadriceps strengthening exercises. Specific to SAP: Sham intervention Specific to SAP + PERT: 10 sessions of perturbation training (~30 min per session). |
| Neither SAP nor SAP + PERT training appears effective at altering gait mechanics in men in the short term; however, meaningful gait asymmetries mostly resolved between post-training and 2 years after ACLR regardless of the intervention group. |
| [34] | Randomised controlled trial | Examine the effects of a neuromuscular training program on knee proprioception in athletes who had returned to sports following ACL reconstruction. |
|
| Experimental group: Duration: 8 weeks Frequency: 2–3 times a week (total sessions: 22) Exercises included: single- and double-leg squats, lunges, drop jumps, single-leg stance on an unstable surface, countermovement jumps, long jumps, and horizontal bounds. Continue with the typical routine which focused on sport-related skills. |
| Athletes who participated in the neuromuscular training program exhibited better knee proprioception for their ACL-reconstructed limb, compared to athletes who did not participate in neuromuscular training (control). |
| [35] | Randomised controlled trial | Assess the effects of eccentric training, plyometric training, or a combination of the above two modalities, on measures of dynamic stability, psychological readiness to return to sport, and leg symmetry index in the post-ACLR rehabilitation period of elite female athletes. |
|
| Duration: 6 weeks Control group: instructed to follow their traditional program Experimental groups: Frequency: 2 additional sessions per week × 60 min per session (12 sessions in total in addition to the traditional program) Exercises included: Eccentric group: Nordic hamstring, eccentric hamstring curl, quadriceps eccentric leg extension, glute-hamstring raise. Plyometric group: Standing vertical hops, countermovement jump, depth jumps, multiple two-foot hurdle jumps, two-foot jumps (forward, backward, lateral), single-foot jumps. Combined group: combination of eccentric and plyometric groups |
| Despite all of the training methods inducing improvement outcomes to various extents, combined (eccentric/plyometric) training was the most effective protocol to stimulate positive changes in both stability and functional performance. |
| [36] | Randomised controlled trial | To examine the effect of a jump training program on patient-reported function and biomechanical measures and to determine whether a high-repetition program with decreased intensity via body weight support (BWS) will improve functional, mechanical, and neuromuscular outcomes. |
|
| Duration: 8 weeks Frequency: twice-weekly ×1 h long Form of training: Individual sessions Exercises and progression: Jump training under normal body weight conditions (JWBW) group Training progressed from 80–100 contacts per session in the first week to 120–200 contacts per session in the eighth week. Jump training augmented by a customed body weight support system group (JWBWS): Training was initiated at a BWS level of 30%, then decreased by 10% every 2 weeks, and without BWS at the final 2 weeks of training. |
| Both groups demonstrated significant improvements in both patient-reported and performance-based measures, while there were no significant differences between groups. However, the patients in the JTBW group had a statistically higher probability of effusion with training, which may indicate the improved training tolerance with less risk for knee effusion in the JTBWS group is clinically preferential. |
| [37] | Randomised controlled trial | To investigate the impact of running retraining on the muscular strength of the knee’s extensors and flexors at 4 and 6 months after ACLR. |
|
| The retrained group: Duration: 8 weeks Frequency: 3 times a week Exercises and progression: running intensity chosen based on the percentage of the maximal heart frequency. Control group: No intervention was given. |
| The running retraining program did not appear to influence the knee’s muscular and functional recovery. |
| Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Outcome Reporting | Other Sources of Bias | |
|---|---|---|---|---|---|---|---|
| Arundale et al., 2017 [20] |  | |  | | | | |
| Capin et al., 2017 [30] |  | | | | | | |
| Ghaderi et al., 2021 [31] | | | | | | | |
| Capin et al., 2019 [32] | | | | | | | |
| Capin et al., 2018 [33] | | | | | | | |
| Ghaderi et al., 2020 [34] | | | | | | | |
| Kasmi et al., 2021 [35] | | | | | | | |
| Elias et al., 2018 [36] | | | | | | | |
| Dauty et al., 2010 [37] | | | | | | | |
: Low risk of bias : Unclear risk of bias : High risk of bias.Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, C.-Y.; Mok, K.-M.; Yung, S.-H. Secondary Anterior Cruciate Ligament Injury Prevention Training in Athletes: What Is the Missing Link? Int. J. Environ. Res. Public Health 2023, 20, 4821. https://doi.org/10.3390/ijerph20064821
Wong C-Y, Mok K-M, Yung S-H. Secondary Anterior Cruciate Ligament Injury Prevention Training in Athletes: What Is the Missing Link? International Journal of Environmental Research and Public Health. 2023; 20(6):4821. https://doi.org/10.3390/ijerph20064821
Chicago/Turabian StyleWong, Choi-Yan (Tiffany), Kam-Ming Mok, and Shu-Hang (Patrick) Yung. 2023. "Secondary Anterior Cruciate Ligament Injury Prevention Training in Athletes: What Is the Missing Link?" International Journal of Environmental Research and Public Health 20, no. 6: 4821. https://doi.org/10.3390/ijerph20064821
APA StyleWong, C.-Y., Mok, K.-M., & Yung, S.-H. (2023). Secondary Anterior Cruciate Ligament Injury Prevention Training in Athletes: What Is the Missing Link? International Journal of Environmental Research and Public Health, 20(6), 4821. https://doi.org/10.3390/ijerph20064821