
Modulating Elements of Nurse Resilience in Population Care during the COVID-19 Pandemic

 , ,
, ,  ,
,  and
and
Abstract
1. Introduction
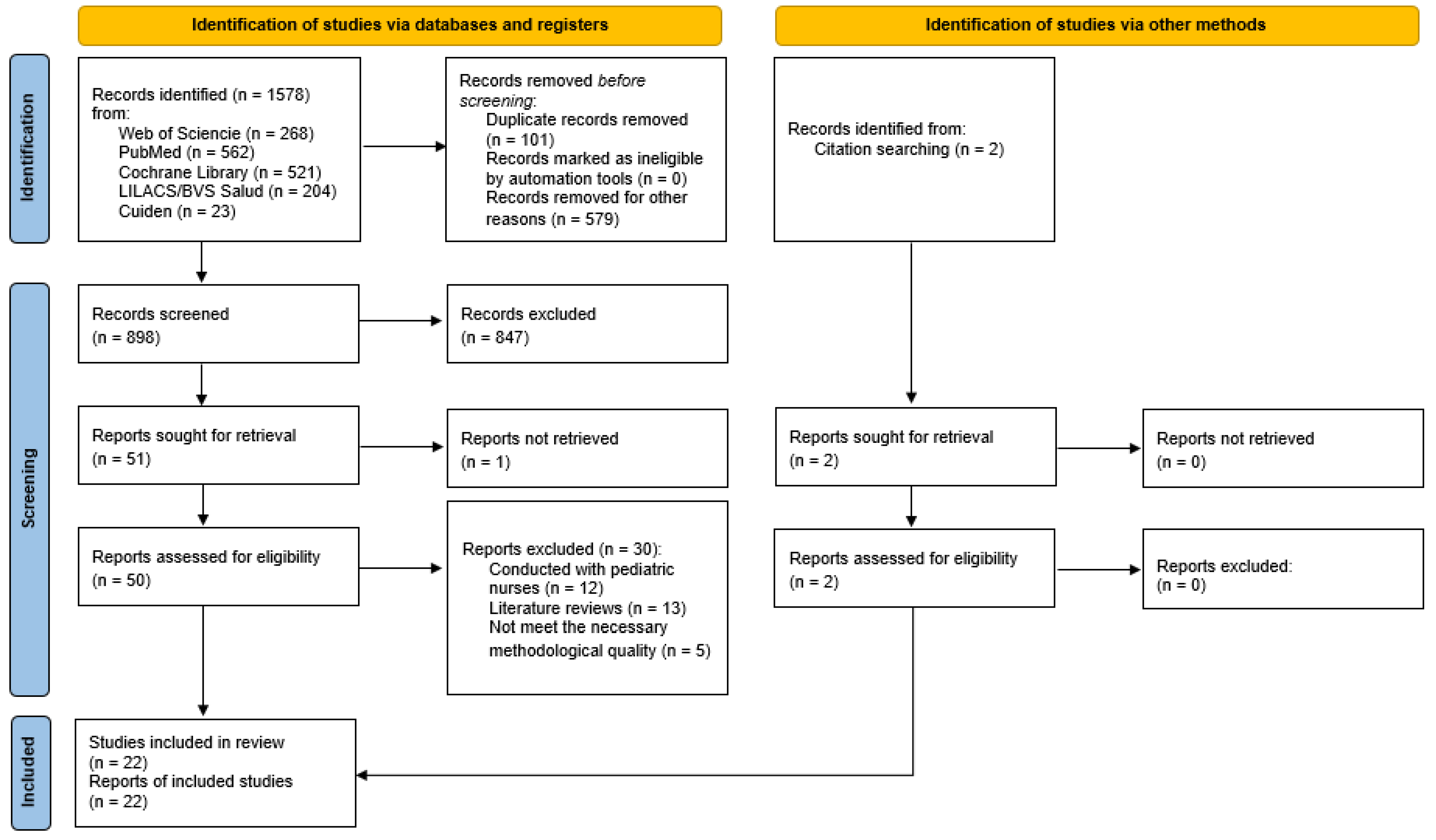
2. Materials and Methods
2.1. Design
2.2. Protocol Development and PICO Question
2.3. Selection Criteria
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Search Strategy
2.5. Study Variables
3. Results
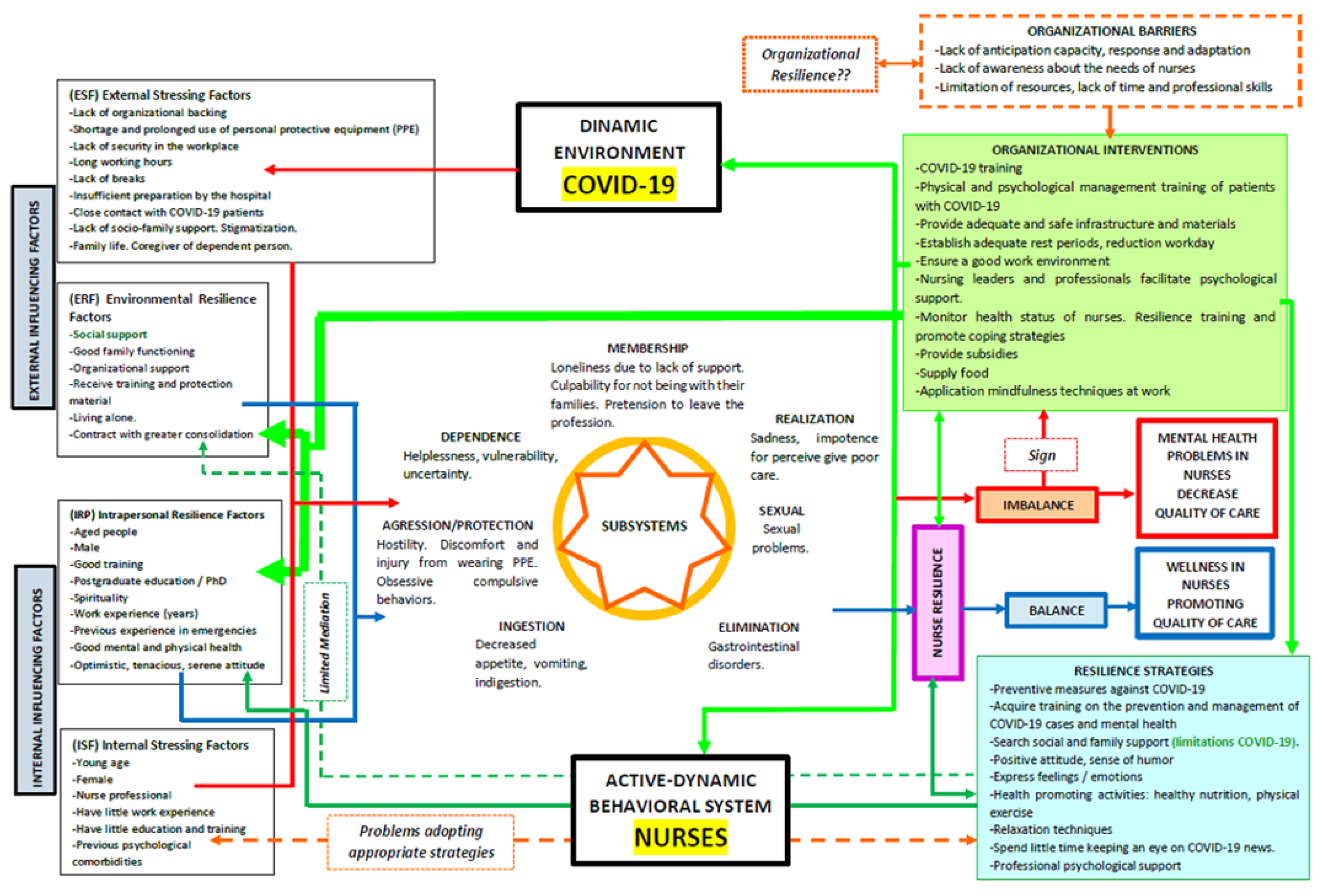
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Council of Nurses El Consejo Internacional de Enfermeras y Nursing Now Celebran la Declaración de 2020 Como el Año Internacional de la Enfermera y la Partera. Available online: https://www.icn.ch/es/noticias/el-consejo-internacional-de-enfermeras-y-nursing-now-celebran-la-declaracion-de-2020-como (accessed on 10 September 2021).
- Hui, D.S.; Azhar, E.I.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; Mchugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The Continuing 2019-NCoV Epidemic Threat of Novel Coronaviruses to Global Health—The Latest 2019 Novel Coronavirus Outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Announces COVID-19 Outbreak a Pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 10 September 2021).
- Center for Systems Sciencie and Engineering at JHU COVID-19 Dashboard. 2021. Available online: https://gisanddata.maps.arcgis.com/apps/dashboards/bda7594740fd40299423467b48e9ecf6 (accessed on 22 September 2021).
- International Council of Nurses. El CIE Confirma el Fallecimiento de 1500 Enfermeras por COVID-19 en 44 Países y Estima que las Muertes de Trabajadores Sanitarios por Esta Enfermedad Podrían Superar las 20,000 en Todo el Mundo. Available online: https://www.icn.ch/es/noticias/el-cie-confirma-el-fallecimiento-de-1-500-enfermeras-por-covid-19-en-44-paises-y-estima (accessed on 10 September 2021).
- Garbern, S.C.; Ebbeling, L.G.; Bartels, S.A. A Systematic Review of Health Outcomes among Disaster and Humanitarian Responders. Prehosp. Disaster Med. 2016, 31, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Tahan, H.M. Essential Case Management Practices Amidst the Novel Coronavirus Disease 2019 (COVID-19) Crisis: Part 2. Prof. Case Manag. 2020, 25, 267–284. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.; Vilagut, G.; Mortier, P.; Ferrer, M.; Alayo, I.; Aragón-Peña, A.; Aragonès, E.; Campos, M.; Cura-González, I.D.; Emparanza, J.I.; et al. Mental Health Impact of the First Wave of COVID-19 Pandemic on Spanish Healthcare Workers: A Large Cross-Sectional Survey. Rev. Psiquiatr. Salud Ment. 2021, 14, 90–105. [Google Scholar] [CrossRef] [PubMed]
- Shih, F.-J.; Turale, S.; Lin, Y.-S.; Gau, M.-L.; Kao, C.-C.; Yang, C.-Y.; Liao, Y.-C. Surviving a Life-Threatening Crisis: Taiwan’s Nurse Leaders’ Reflections and Difficulties Fighting the SARS Epidemic. J. Clin. Nurs. 2009, 18, 3391–3400. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Kang, W.S.; Cho, A.-R.; Kim, T.; Park, J.K. Psychological Impact of the 2015 MERS Outbreak on Hospital Workers and Quarantined Hemodialysis Patients. Compr. Psychiatry 2018, 87, 123–127. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Galea, S.; Bucciarelli, A.; Vlahov, D. What Predicts Psychological Resilience after Disaster? The Role of Demographics, Resources, and Life Stress. J. Consult. Clin. Psychol. 2007, 75, 671–682. [Google Scholar] [CrossRef] [PubMed]
- García del Castillo, J.; García del Castillo-López, Á.; López-Sánchez, C.; Dias, P. Conceptualización Teórica de La Resiliencia Psicosocial y Su Relación Con La Salud. Health Addict. Drog. 2016, 16, 59. [Google Scholar] [CrossRef]
- Caro Alonso, P.Á.; Rodríguez-Martín, B.; Caro Alonso, P.Á.; Rodríguez-Martín, B. Potencialidades de La Resiliencia Para Los Profesionales de Enfermería. Index Enferm. 2018, 27, 42–46. [Google Scholar]
- Marriner Tomey, A.; Raile Alligood, M. Modelos y Teorías En Enfermería, 7th ed.; Elsevier Masson: Paris, France, 2011; 856p. [Google Scholar]
- Cortés Recaball, J.E. La Resiliencia: Una Mirada Desde la Enfermería. Cienc. Enferm. 2010, 16, 27–32. [Google Scholar] [CrossRef]
- Benavent Garcés, A.; Ferrer Ferrandis, E.; Francisco del Rey, C. Fundamentos de Enfermería, 2nd ed.; DAE: Madrid, Spain, 2003. [Google Scholar]
- Cleary, M.; Kornhaber, R.; Thapa, D.K.; West, S.; Visentin, D. The Effectiveness of Interventions to Improve Resilience among Health Professionals: A Systematic Review. Nurse Educ. Today 2018, 71, 247–263. [Google Scholar] [CrossRef] [PubMed]
- Arrogante, O.; Pérez-García, A.M.; Aparicio-Zaldívar, E.G. Recursos personales relevantes para el bienestar psicológico en el personal de enfermería. Enferm. Intensiva 2016, 27, 22–30. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Stone, P.W. Popping the (PICO) Question in Research and Evidence-Based Practice. Appl. Nurs. Res. ANR 2002, 15, 197–198. [Google Scholar] [CrossRef] [PubMed]
- MeSH Browser. Medical Subject Headings 2021. Available online: https://meshb.nlm.nih.gov/search (accessed on 10 September 2021).
- The Joanna Briggs Institute. New JBI Levels of Evidence. Available online: https://jbi.global/sites/default/files/2019-05/JBI-Levels-of-evidence_2014_0.pdf (accessed on 10 September 2021).
- Zingg, W.; Castro-Sanchez, E.; Secci, F.V.; Edwards, R.; Drumright, L.N.; Sevdalis, N.; Holmes, A.H. Innovative Tools for Quality Assessment: Integrated Quality Criteria for Review of Multiple Study Designs (ICROMS). Public Health 2016, 133, 19–37. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A Measurement Tool to Assess the Methodological Quality of Systematic Reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Declaración de La Iniciativa STROBE (Strengthening the Reporting of Observational Studies in Epidemiology): Directrices Para La Comunicación de Estudios Observacionales. Gac. Sanit. 2008, 22, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Afshari, D.; Nourollahi-darabad, M.; Chinisaz, N. Demographic Predictors of Resilience among Nurses during the COVID-19 Pandemic. Work 2021, 68, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Balay-odao, E.M.; Alquwez, N.; Inocian, E.P.; Alotaibi, R.S. Hospital Preparedness, Resilience, and Psychological Burden Among Clinical Nurses in Addressing the COVID-19 Crisis in Riyadh, Saudi Arabia. Front. Public Health 2021, 8, 943. [Google Scholar] [CrossRef]
- Cai, H.; Tu, B.; Ma, J.; Chen, L.; Fu, L.; Jiang, Y.; Zhuang, Q. Psychological Impact and Coping Strategies of Frontline Medical Staff in Hunan between January and March 2020 During the Outbreak of Coronavirus Disease 2019 (COVID-19) in Hubei, China. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e924171. [Google Scholar] [CrossRef]
- Cai, W.; Lian, B.; Song, X.; Hou, T.; Deng, G.; Li, H. A Cross-Sectional Study on Mental Health among Health Care Workers during the Outbreak of Corona Virus Disease 2019. Asian J. Psychiatry 2020, 51, 102111. [Google Scholar] [CrossRef] [PubMed]
- De Pinho, L.G.; Sampaio, F.; Sequeira, C.; Teixeira, L.; Fonseca, C.; Lopes, M.J. Portuguese Nurses’ Stress, Anxiety, and Depression Reduction Strategies during the COVID-19 Outbreak. Int. J. Environ. Res. Public Health 2021, 18, 3490. [Google Scholar] [CrossRef] [PubMed]
- Del Pozo-Herce, P.; Garrido-García, R.; Santolalla-Arnedo, I.; Gea-Caballero, V.; García-Molina, P.; Ruiz de Viñaspre-Hernández, R.; Rodríguez-Velasco, F.J.; Juárez-Vela, R. Psychological Impact on the Nursing Professionals of the Rioja Health Service (Spain) Due to the SARS-CoV-2 Virus. Int. J. Environ. Res. Public Health 2021, 18, 580. [Google Scholar] [CrossRef] [PubMed]
- Giusti, E.M.; Pedroli, E.; D’Aniello, G.E.; Stramba Badiale, C.; Pietrabissa, G.; Manna, C.; Stramba Badiale, M.; Riva, G.; Castelnuovo, G.; Molinari, E. The Psychological Impact of the COVID-19 Outbreak on Health Professionals: A Cross-Sectional Study. Front. Psychol. 2020, 11, 1684. [Google Scholar] [CrossRef]
- Kim, S.C.; Quiban, C.; Sloan, C.; Montejano, A. Predictors of Poor Mental Health among Nurses during COVID-19 Pandemic. Nurs. Open 2021, 8, 900–907. [Google Scholar] [CrossRef]
- Kılınç, T.; Çelik, A.S. Relationship between the Social Support and Psychological Resilience Levels Perceived by Nurses during the COVID-19 Pandemic: A Study from Turkey. Perspect. Psychiatr. Care 2021, 57, 1000–1008. [Google Scholar] [CrossRef]
- Labrague, L.J.; de los Santos, J. COVID-19 Anxiety among Frontline Nurses: Predictive Role of Organisational Support, Personal Resilience and Social Support. J. Nurs. Manag. 2020, 28, 1653–1661. [Google Scholar] [CrossRef]
- Leng, M.; Wei, L.; Shi, X.; Cao, G.; Wei, Y.; Xu, H.; Zhang, X.; Zhang, W.; Xing, S.; Wei, H. Mental Distress and Influencing Factors in Nurses Caring for Patients with COVID-19. Nurs. Crit. Care 2021, 26, 94–101. [Google Scholar] [CrossRef]
- Lorente, L.; Vera, M.; Peiró, T. Nurses´ Stressors and Psychological Distress during the COVID-19 Pandemic: The Mediating Role of Coping and Resilience. J. Adv. Nurs. 2020, 77, 1335–1344. [Google Scholar] [CrossRef]
- Luceño-Moreno, L.; Talavera-Velasco, B.; García-Albuerne, Y.; Martín-García, J. Symptoms of Posttraumatic Stress, Anxiety, Depression, Levels of Resilience and Burnout in Spanish Health Personnel during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The Psychological and Mental Impact of Coronavirus Disease 2019 (COVID-19) on Medical Staff and General Public—A Systematic Review and Meta-Analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef] [PubMed]
- Lyu, H.; Yao, M.; Zhang, D.; Liu, X. The Relationship among Organizational Identity, Psychological Resilience and Work Engagement of the First-Line Nurses in the Prevention and Control of COVID-19 Based on Structural Equation Model. Risk Manag. Healthc. Policy 2020, 13, 2379–2386. [Google Scholar] [CrossRef] [PubMed]
- Nie, A.; Su, X.; Zhang, S.; Guan, W.; Li, J. Psychological Impact of COVID-19 Outbreak on Frontline Nurses: A Cross-Sectional Survey Study. J. Clin. Nurs. 2020, 29, 4217–4226. [Google Scholar] [CrossRef] [PubMed]
- Ou, X.; Chen, Y.; Liang, Z.; Wen, S.; Li, S.; Chen, Y. Resilience of Nurses in Isolation Wards during the COVID-19 Pandemic: A Cross-Sectional Study. Psychol. Health Med. 2021, 26, 98–106. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, C.; Pan, W.; Zheng, J.; Gao, J.; Huang, X.; Cai, S.; Zhai, Y.; Latour, J.M.; Zhu, C. Stress, Burnout, and Coping Strategies of Frontline Nurses During the COVID-19 Epidemic in Wuhan and Shanghai, China. Front. Psychiatry 2020, 11, 565520. [Google Scholar] [CrossRef]
- Pollock, A.; Campbell, P.; Cheyne, J.; Cowie, J.; Davis, B.; McCallum, J.; McGill, K.; Elders, A.; Hagen, S.; McClurg, D.; et al. Interventions to Support the Resilience and Mental Health of Frontline Health and Social Care Professionals during and after a Disease Outbreak, Epidemic or Pandemic: A Mixed Methods Systematic Review. Cochrane Database Syst. Rev. 2020, 11, CD013779. [Google Scholar] [CrossRef]
- Cunill Olivas, M.; Aymerich Andreu, M.; Serdà Ferrer, B.-C.; Patiño Masó, J. The Impact of COVID-19 on Spanish Health Professionals: A Description of Physical and Psychological Effects. Int. J. Ment. Health Promot. 2020, 22, 185–198. [Google Scholar] [CrossRef]
- Rieckert, A.; Schuit, E.; Bleijenberg, N.; ten Cate, D.; de Lange, W.; de Man-van Ginkel, J.M.; Mathijssen, E.; Smit, L.C.; Stalpers, D.; Schoonhoven, L.; et al. How Can We Build and Maintain the Resilience of Our Health Care Professionals during COVID-19? Recommendations Based on a Scoping Review. BMJ Open 2021, 11, e043718. [Google Scholar] [CrossRef]
- Rodriguez-Vega, B.; Palao, Á.; Muñoz-Sanjose, A.; Torrijos, M.; Aguirre, P.; Fernández, A.; Amador, B.; Rocamora, C.; Blanco, L.; Marti-Esquitino, J.; et al. Implementation of a Mindfulness-Based Crisis Intervention for Frontline Healthcare Workers During the COVID-19 Outbreak in a Public General Hospital in Madrid, Spain. Front. Psychiatry 2020, 11, 1170. [Google Scholar] [CrossRef]
- Molina, F.J.C. Nosocomios higienistas: El caso Florence Nightingale. Cult. Cuid. 2013, 36, 96–105. [Google Scholar] [CrossRef][Green Version]
- Maunder, R.; Hunter, J.; Vincent, L.; Bennett, J.; Peladeau, N.; Leszcz, M.; Sadavoy, J.; Verhaeghe, L.M.; Steinberg, R.; Mazzulli, T. The Immediate Psychological and Occupational Impact of the 2003 SARS Outbreak in a Teaching Hospital. CMAJ Can. Med. Assoc. J. 2003, 168, 1245–1251. [Google Scholar]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely Mental Health Care for the 2019 Novel Coronavirus Outbreak Is Urgently Needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The Psychological Impact of the SARS Epidemic on Hospital Employees in China: Exposure, Risk Perception, and Altruistic Acceptance of Risk. Can. J. Psychiatry Rev. Can. Psychiatr. Assoc. 2009, 54, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Chew, Q.H.; Wei, K.C.; Vasoo, S.; Chua, H.C.; Sim, K. Narrative Synthesis of Psychological and Coping Responses towards Emerging Infectious Disease Outbreaks in the General Population: Practical Considerations for the COVID-19 Pandemic. Singap. Med. J. 2020, 61, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Chou, L.-P.; Li, C.-Y.; Hu, S.C. Job Stress and Burnout in Hospital Employees: Comparisons of Different Medical Professions in a Regional Hospital in Taiwan. BMJ Open 2014, 4, e004185. [Google Scholar] [CrossRef]
- Maunder, R.G.; Lancee, W.J.; Rourke, S.; Hunter, J.J.; Goldbloom, D.; Balderson, K.; Petryshen, P.; Steinberg, R.; Wasylenki, D.; Koh, D.; et al. Factors Associated With the Psychological Impact of Severe Acute Respiratory Syndrome on Nurses and Other Hospital Workers in Toronto. Psychosom. Med. 2004, 66, 938–942. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.; Lim, M.K.; Chia, S.E.; Ko, S.M.; Qian, F.; Ng, V.; Tan, B.H.; Wong, K.S.; Chew, W.M.; Tang, H.K.; et al. Risk Perception and Impact of Severe Acute Respiratory Syndrome (SARS) on Work and Personal Lives of Healthcare Workers in Singapore: What Can We Learn? Med. Care 2005, 43, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Chung, B.P.M.; Wong, T.K.S.; Suen, E.S.B.; Chung, J.W.Y. SARS: Caring for Patients in Hong Kong. J. Clin. Nurs. 2005, 14, 510–517. [Google Scholar] [CrossRef]
- Khalid, I.; Khalid, T.J.; Qabajah, M.R.; Barnard, A.G.; Qushmaq, I.A. Healthcare Workers Emotions, Perceived Stressors and Coping Strategies During a MERS-CoV Outbreak. Clin. Med. Res. 2016, 14, 7–14. [Google Scholar] [CrossRef]
- Leng, M.; Xiu, H.; Yu, P.; Feng, J.; Wei, Y.; Cui, Y.; Zhang, M.; Zhou, Y.; Wei, H. Current State and Influencing Factors of Nurse Resilience and Perceived Job-Related Stressors. J. Contin. Educ. Nurs. 2020, 51, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.-F.; Cross, W.; Plummer, V.; Lam, L.; Luo, Y.-H.; Zhang, J.-P. Exploring Resilience in Chinese Nurses: A Cross-Sectional Study. J. Nurs. Manag. 2017, 25, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Chua, S.E.; Cheung, V.; Cheung, C.; McAlonan, G.M.; Wong, J.W.S.; Cheung, E.P.T.; Chan, M.T.Y.; Wong, M.M.C.; Tang, S.W.; Choy, K.M.; et al. Psychological Effects of the SARS Outbreak in Hong Kong on High-Risk Health Care Workers. Can. J. Psychiatry Rev. Can. Psychiatr. Assoc. 2004, 49, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-S.; Lee, E.-H.; Park, N.-R.; Choi, Y.H. Mental Health of Nurses Working at a Government-Designated Hospital during a MERS-CoV Outbreak: A Cross-Sectional Study. Arch. Psychiatr. Nurs. 2018, 32, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.R.; Cartwright, S. Social Support, Job Stress, Health, and Job Satisfaction among Nurses in the United Kingdom. Int. J. Stress Manag. 2002, 9, 163–182. [Google Scholar] [CrossRef]
- Hu, S.H.; Yu, Y.-M.; Chang, W.-Y.; Lin, Y.-K. Social Support and Factors Associated with Self-Efficacy among Acute-Care Nurse Practitioners. J. Clin. Nurs. 2018, 27, 876–882. [Google Scholar] [CrossRef]
- Tusaie, K.; Dyer, J. Resilience: A Historical Review of the Construct. Holist. Nurs. Pract. 2004, 18, 3–8. [Google Scholar] [CrossRef]
- Stanisławski, K. The Coping Circumplex Model: An Integrative Model of the Structure of Coping with Stress. Front. Psychol. 2019, 10, 694. [Google Scholar] [CrossRef]
- Lazarus, R. Toward Better Research on Stress and Coping. Am. Psychol. 2000, 55, 665–673. [Google Scholar] [CrossRef]
- Day, A.L.; Livingstone, H.A. Gender Differences in Perceptions of Stressors and Utilization of Social Support among University Students. Can. J. Behav. Sci. 2003, 35, 73–83. [Google Scholar] [CrossRef]
- González-Morales, M.G.; Rodríguez, I.; Peiró, J.M. A Longitudinal Study of Coping and Gender in a Female-Dominated Occupation: Predicting Teachers’ Burnout. J. Occup. Health Psychol. 2010, 15, 29–44. [Google Scholar] [CrossRef]
- Jackson, D.; Bradbury-Jones, C.; Baptiste, D.; Gelling, L.; Morin, K.; Neville, S.; Smith, G.D. Life in the Pandemic: Some Reflections on Nursing in the Context of COVID-19. J. Clin. Nurs. 2020, 29, 2041–2043. [Google Scholar] [CrossRef] [PubMed]
- Preti, E.; Di Mattei, V.; Perego, G.; Ferrari, F.; Mazzetti, M.; Taranto, P.; Di Pierro, R.; Madeddu, F.; Calati, R. The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Curr. Psychiatry Rep. 2020, 22, 43. [Google Scholar] [CrossRef] [PubMed]
- Kemper, K.J.; Mo, X.; Khayat, R. Are Mindfulness and Self-Compassion Associated with Sleep and Resilience in Health Professionals? J. Altern. Complement. Med. 2015, 21, 496–503. [Google Scholar] [CrossRef]
- Greenberg, N.; Wessely, S.; Wykes, T. Potential Mental Health Consequences for Workers in the Ebola Regions of West Africa—A Lesson for All Challenging Environments. J. Ment. Health 2015, 24, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Kamal-Yanni, M. Never Again: Building Resilient Health Systems and Learning from the Ebola Crisis; Oxfam International: Nairobi, Kenya, 2015; Volume 12, Available online: https://oxfamilibrary.openrepository.com/bitstream/handle/10546/550092/bp-never-again-resilient-health-systems-ebola-160415-fr.pdf (accessed on 10 September 2021).
- Traynor, M. Guest Editorial: What’s Wrong with Resilience. J. Res. Nurs. 2018, 23, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Kruk, M.E.; Myers, M.; Varpilah, S.T.; Dahn, B.T. What Is a Resilient Health System? Lessons from Ebola. Lancet 2015, 385, 1910–1912. [Google Scholar] [CrossRef]
- Jackson, D.; Firtko, A.; Edenborough, M. Personal Resilience as a Strategy for Surviving and Thriving in the Face of Workplace Adversity: A Literature Review. J. Adv. Nurs. 2007, 60, 1–9. [Google Scholar] [CrossRef]
- McAllister, M.; McKinnon, J. The Importance of Teaching and Learning Resilience in the Health Disciplines: A Critical Review of the Literature. Nurse Educ. Today 2009, 29, 371–379. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Database | Search |
|---|---|
| WOS | ((nurs *) AND (COVID-19)) OR (coronavirus infections)) AND (Resilience, Psychological)) OR (Adaptation, Psychological)) OR (Stress, Psychological)) OR (Burnout, Psychological)) OR (uncertainty) |
| Medine/ PubMed | ((nurs *) AND (coronavirus infections)) AND (resilience, psychological) Filters: in the last 1 year |
| ((nurs *) AND (coronavirus infections)) AND (adaptation, psychological) Filters: in the last 1 year | |
| ((nurs *) AND (coronavirus infections)) AND (stress, psychological) Filters: in the last 1 year | |
| Cochrane Library | ((nurs *) AND (coronavirus infections)) AND (resilience, psychological) |
| ((nurs *) AND (coronavirus infections)) AND (adaptation, psychological) | |
| ((nurs *) AND (coronavirus infections)) AND (stress, psychological) | |
| LILACS/ BVS Salud | (nurs *) AND (coronavirus infections) AND (resilience, psychological) AND (year_cluster: [2020 TO 2021]) |
| (nurs *) AND (coronavirus infections) AND (adaptation, psychological) AND (year_cluster: [2020 TO 2021]) | |
| (nurs *) AND (coronavirus infections) AND (stress, psychological) AND (year_cluster: [2020 TO 2021]) | |
| Cuiden | (“enfermera”) AND ((“COVID-19”) AND (“resiliencia”)) |
| (“enfermera”) AND ((“COVID19”) AND (“afrontamiento”)) | |
| (“enfermera”) AND ((“COVID-19”) AND (“adaptación”)) | |
| (“enfermera”) AND ((“COVID-19”) AND (“agotamiento”)) | |
| (“enfermera”) AND ((“COVID-19”) AND (“estrés”)) |
| Author, Year, Location | Design and Sample | Aim | Variables | Results | Quality, LE *, LR ** |
|---|---|---|---|---|---|
| Nie et al., 2020 [41] China | Observational, descriptive, cross-sectional, descriptive study. 263 nurses. | To identify the prevalence and associated factors of psychological distress among frontline nurses during the COVID-19 outbreak. | Psychological distress, impact of the COVID-19 pandemic. | The risk factors that had the greatest impact on the nurses were: direct contact with patients with COVID-19, doubt about the efficacy of PPE, younger age, and stigmatization. Working overtime and changing work routine was not a risk factor for the nurses in this study. Loneliness, sadness, fear, and concern for their family members were triggered as responses. Faced with the stressors of the pandemic, nurses were more likely to develop positive strategies that were negatively related to psychological distress. Nurses who developed strategies such as overexertion in controlling coronavirus infection, avoidance, alcohol or drug use, and constructing false illusions were more likely to experience psychological distress. | STROBE 20/22 JBI *** 4b-C |
| Lyu et al., 2020 [40] China | Observational, descriptive, cross-sectional study. 216 nurses. | To explore how organizational identity and psychological resilience affect frontline nurses’ work engagement in coronavirus disease prevention and control 2019 (COVID-19) and to establish the relationship model based on these factors. | Level of resilience, organizational support, and work commitment. | The nurses in the study reported high levels of psychological resilience, which correlated positively with higher levels of perceived organizational support, leading to greater work engagement and quality of work. Resilience showed a mediating role between organizational support and nurses’ work engagement. Higher levels of resilience were also associated with having previously good emotional self-control and ability to adapt to challenges. The Chinese government issued a COVID-19 Disease Prevention and Control Plan, according to which Chinese hospitals were required to meet set standards and place special emphasis on developing organizational identity. Additional efforts were made to provide training and improve self-protection practices; protective measures were provided and evaluated, in turn improving nurses’ resilience and work engagement. | STROBE 19/22 JBI 4b-C |
| Cai et al., 2020 [29] China | Observational, descriptive, cross-sectional study. 1521 nurses. | To investigate psychological abnormality in healthcare workers struggling with the COVID-19 epidemic and to explore associations between social support, resilience, and mental health. | Influencing factors in psychological impact and the psychological responses they can trigger in nurses. | Risk factors influencing worse mental health outcomes were: younger age and lower family and social support, observing the increasing number of COVID-19 cases and deaths, and not having experience in public health emergencies. They tended to develop psychological abnormalities in interpersonal sensitivity, emotional distress, hostility, and obsessive–compulsive behaviors in response. The nurses in the sample presented moderate levels of resilience. Those who participated in previous epidemics had a significantly higher level of resilience compared to the others, which was associated with a better quality of the health interventions they provided. Perceived good social and organizational support, optimism, and tenacity were positively correlated with resilience and better mental health outcomes. | STROBE 20/22 JBI 4b-C |
| Cai et al., 2020 [28] China | Observational, descriptive, cross-sectional study. 534 health professionals: −248 nurses. −233 phisycians. −53 others. | To investigate the psychological impact and coping strategies of frontline medical personnel in Hunan province, adjacent to Hubei province, during the COVID-19 outbreak between January and March 2020. | Stressors and protective factors of healthcare professionals and psychological effects generated by the impact of the COVID-19 pandemic. | The factors associated with stress were: younger age, shortage of PPE, working in front of patients on the frontline, and seeing news about the evolution of COVID-19. Longer shifts and overtime were not a stressor. The predominant responses induced were: loss of control, feeling of vulnerability, nervousness, hostility, tension, concern for their safety and that of their families, and intention to leave their post. The availability of strict infection control guidelines, specialized equipment, recognition of their efforts by the hospital administration and the government, and the reduction in cases reported by COVID-19 were assumed to be protective factors. The most commonly used strategies to reduce stress were applying strict protective measures, seeking help from family and friends, having a positive attitude towards oneself and one’s work, and having a sense of humor. These strategies were mostly adopted by nurses compared to physicians and technicians. The least used strategy, in general, was to seek psychological support. Given the situation experienced by the nurses, in the survey, they expressed a number of interventions that could be made to promote their resilience and well-being: the availability of protective equipment, strict infection control guidelines, receiving specialized technical and emotional stress management training, and receiving support from hospital administration and government. | STROBE 19/22 JBI 4b-C |
| Leng et al., 2020 [36] China | Observational, descriptive, cross-sectional study. 108 nurses. | To quantify the severity of post-traumatic stress disorder (PTSD) symptoms and stress of nurses and to explore factors that influence their psychological health when caring for patients with COVID-19. | Regulatory factors of psychological impact on nurses and triggered responses. Degree of nurses’ resilience. Organizational interventions to foster resilience. | The main sources of stress included working in an isolated environment, shortage and prolonged use of PPE, intensity of the workload, contact with patients with COVID-19, lack of family support, and insufficient work experience. These factors generated responses in the nurses’ sleep disturbances, feeling of loneliness, guilt, and fear for their safety. The nurses in the study had moderate resilience scores. Even the resilient nurses experienced some degree of mental distress, although significantly less compared to the others. Perceiving greater organizational support through leadership rounds; providing breaks, psychological support, training, and coaching; and a reduced workday were associated with better resilience scores. | STROBE 20/22 JBI 4b-C |
| Luo et al., 2020 [39] China | Systematic review and meta-analysis. 62 studies. | To assess the updated psychological and mental impact of the COVID-19 pandemic among health care workers. | Risk and protective factors related to psychological impact. | Among health professionals, factors such as being a woman, a nurse, working on the frontline in direct contact with COVID-19 patients, working in the most affected area, not having adequate protective measures, being aware of news about the evolution of COVID-19, and having a lack of training and family support were additionally associated with greater psychological distress. | AMSTAR-2 RATING High JBI 3a-A |
| Cunill et al., 2020 [45] Spain | Observational, descriptive, cross-sectional study. 1452 nurses. | To describe the physical and psychological symptoms in health care workers caring for patients with COVID-19. | Stressors and psychological and physical responses triggered by psychological impact on nurses. | Shortage of protective material, work overload, working in isolated environments, prolonged use of PPE, being a woman, being a nurse, and having children were detected as stressors. They triggered responses such as uncertainty due to not knowing if they have the disease, helplessness, discomfort, perception of not being able to perform their professional duties effectively, all of which give rise to physical symptoms, such as headaches, arms, legs, back, and precordial pain, fatigue and insomnia, gastrointestinal problems, decreased appetite, dyspnea, dizziness, and/or problems in sexual intercourse. | STROBE 21/22 JBI 4b-C |
| Luceño-Moreno et al., 2020 [38] Spain | Observational, descriptive, cross-sectional study. 1422 health professionals: −826 nurses. −428 physicians. −168 nursing assistants. | Analyzing post-traumatic stress, anxiety, and depression during the COVID-19 pandemic. | Influencing factors in the psychological impact of the COVID-19 pandemic on nurses and induced responses. | The risk and stress factors were: being a woman, being younger, having less work experience, working in a hospital, being a nurse, having a 12- or 24-hour on-call shift, and living with people at risk. The main responses were: uncertainty and fear of the possibility of being infected and being able to pass it on to family members. The levels of resilience of the health care workers evaluated were moderate. Resilience was negatively correlated with emotional exhaustion and depersonalization and positively influenced the mental health of healthcare workers. Having a graduate or doctoral degree was associated with higher levels of resilience. | STROBE 20/22 JBI 4b-C |
| Giusti et al., 2020 [32] Italy | Observational, descriptive, cross-sectional study. 330 health professionals: −140 physicians. −86 nurses. −38 nursing assistants. −67 others. | To assess the prevalence of burnout and psychopathological conditions in health professionals working in a healthcare institution in northern Italy and to identify sociodemographic, occupational, and psychological predictors of burnout. | Risk factors and their relationship with psychological symptoms. | Predictors of greater psychological impact were: longer working hours, previous psychological comorbidities, fear of infection, feelings of isolation, less perceived support from friends, female gender, being a nurse, age, working in the hospital, and being in contact with patients with COVID-19. | STROBE 20/22 JBI 4b-C |
| Labrague y de los Santos 2020 [35] Filipinas | Observational, descriptive, cross-sectional study. 325 nurses. | To examine the relative influence of personal resilience, social support, and organizational support on the reduction in COVID-19 anxiety in frontline nurses. | Regulatory factors of psychological impact in frontline nurses and triggered responses. Nurses’ level of resilience, organizational support, and social support. | The most significant risk factor for the nurses’ discomfort due to the impact of the pandemic was not feeling prepared for the management of patients with COVID-19 and perceiving little organizational and social support. The most frequent psychological and physical behavioral responses were: tonic immobility, insomnia, dizziness, loss of appetite, and abdominal discomfort. Nurses presented moderate levels of resilience. Better resilience scores were associated with greater perceptions of social and organizational support, and in turn, with reduced anxiety in nurses. | STROBE 20/22 JBI 4b-C |
| Kilinç y Çelik. 2020 [34] Turkey | Observational, descriptive, cross-sectional study. 370 nurses. | To determine the relationship between social support and levels of psychological resilience perceived by nurses in Turkey during the coronavirus disease pandemic-2019 (COVID-19). | Sociodemographic variables. Level of social support. Level of resilience. | The nurses’ levels of resilience were moderate. A significant positive directional relationship was observed between economic status, age, job consolidation, working conditions improved by the hospital, social and family support perceived by the nurses, and their level of psychological resilience. Being in contact with COVID-19 patients had a negative influence on the nurses’ levels of resilience. | STROBE 18/22 JBI 4b-C |
| Zhang et al., 2020 [43] China | Observational, descriptive, cross-sectional study. 110 nurses. | To identify stressors and burnout among frontline nurses caring for COVID-19 patients in Wuhan and Shanghai and explore perceived effective moral support strategies. | Stressors and responses to them in nurses who cared for patients with COVID-19. | The most frequent stressors among the nurses were: lack of family support, work experience, time spent working in isolation rooms, prolonged use of PPE, and younger age. Among the responses triggered by this were: loneliness, guilt, fear of separation from their families, uncertainty, fear of infection, discomfort due to prolonged use of PPE, and concern about providing poor nursing care. The strategies adopted by the nurses to cope with stress were: acquiring training, seeking information on mental health, adopting a positive attitude, participating in health-promoting activities, and practicing relaxation techniques. The least used were those related to seeking professional psychological support. According to the nurses, the most effective main support interventions that could be adopted by the hospital to contribute to reducing stress and improving their resilience and well-being were: support from supervisors, provision of sufficient material, clear instruction on treatment procedures and on COVID-19, offering sufficient time off, professional promotion, and offering psychological services. | STROBE 18/22 JBI 4b-C |
| Kim et al., 2021 [33] USA | Observational, descriptive, cross-sectional study. 320 enfermeras. | To examine the impact of various factors affecting nurses’ mental health during the COVID-19 pandemic. | Influencing factors in nurses in the face of the COVID-19 pandemic in relation to their stress level. | The level of stress, anxiety, and distress perceived by the nurses was moderate–severe, higher than that estimated before the pandemic. Predictors of stressors were: patient care with COVID-19, isolation, younger age, fewprofessional experience, and poor family functioning. Nurses reported moderate levels of resilience. Those with high levels were two to six times less likely to have poor mental health. Organizational support, good family functioning, and spirituality were factors that positively influenced the level of resilience, making nurses less likely to have poor mental health. | STROBE 18/22 JBI 4b-C |
| Rodríguez-Vega et al., 2020 [47] Spain | Qualitative study: exploratory research with a post-intervention evaluation. 150 health professionals. | Implementing a mindfulness-based intervention for frontline healthcare workers during the COVID-19 outbreak in a general public hospital in Madrid. | Attendance at the session. Job position. Perceived usefulness. | More than 3000 sessions were carried out by professionals of Intensive Care Units, COVID-19 Medical Units, and Emergency Services. It was well accepted specifically by nurses and nursing assistants; physicians presented more rejection and were the professionals who attended the least. The intervention was evaluated in the short term and qualified as very useful for reducing stress in frontline health workers, favoring their resilience and reflecting data on feasibility, usefulness, and safety. | ICROMS 17 JBI 3-C |
| Pollok et al., 2020 [44] UK | Systematic review. 16 studies applied to health professionals working on the frontline during epidemics or disease outbreaks. | To assess the effects of interventions aimed at supporting the resilience and mental health of frontline health and social care professionals during and after a disease outbreak, epidemic, or pandemic, as well as the barriers and facilitators to implementing them. | Interventions to promote resilience: related to working conditions; to support basic daily needs; psychological support. Barriers and guidelines for implementation. | Among the most prominent interventions to foster resilience of health professionals in other outbreaks were: those related to working conditions (regular breaks, shorter working hours, team meetings, relaxation/recreation areas in workplaces, provision of epidemic training for professionals, training of professionals in helping patients and self); to support basic daily needs (food, rest); and those of psychological support (online, group therapies, etc.). A number of barriers were identified, such as lack of awareness of the needs of frontline workers by organizations and limited resources and guidelines, for the successful implementation of resilience-related interventions. | AMSTAR-2 RATING High JBI 3b-B |
| Afshari et al., 2021 [26] Irán | Observational, descriptive, cross-sectional study. 387 nurses. | To determine the resilience score and demographic predictors among nurses working in hospitals involved with COVID-19. | Level of resilience. Demographic factors: age, gender, work experience, education level, marital status, and offspring. Sports activity, hospital classification, and degree of labor consolidation. | Nurses’ levels of resilience were low–moderate. Older age, educational level, experience, and a consolidated job position were positively correlated with resilience. Having children, being female, and not exercising were associated with lower resilience scores. | STROBE 18/22 JBI 4b-C |
| Ou et al., 2021 [42] China | Observational, descriptive, cross-sectional study. 92 nurses. | Evaluated the impact of supportive interventions on resilience and self-rated psychopathological symptoms of 92 nurses working in the COVID-19 isolation ward. | Psychopathological symptoms: somatization, obsessive–compulsive behaviors, problems in developing interpersonal sensitivity, depression, anxiety, hostility, phobia, paranoid ideation, and psychoticism. Level of resilience. | The nurses presented high levels of resilience, which were markedly higher than those obtained in other studies. Past experiences in public health emergencies and interventions developed by the hospital to foster organizational and social support, such as training of nurses to better manage the psychological problems of their patients and training on diagnostic guidelines and treatment of COVID-19 before entering the isolation ward. They were given priority access to PPE, a good working environment was fostered, flexible shifts were implemented according to work intensity, and a support team was established to protect the ward workforce. This notably influenced higher resilience scores in the nurses, considerably decreasing psychopathological symptoms, improving their sleep and eating quality, and leading to better mental health in nurses and quality results in their work. | STROBE 20/22 JBI 4b-C |
| Lorente et al., 2021 [37] Spain | Observational, descriptive, cross-sectional study. 421 nurses. | To analyze the cross-sectional effect of sources of stress during the peak of the COVID-19 pandemic on nurses’ psychological distress, focusing on the mediating role of coping strategies, including problem-focused, emotion-focused, and resilience. | Stressors of nurses on the frontline of care for patients with COVID-19 and their response to those stressors. | Identified stressors: work overload, insufficient preparation to cope with work demands, and lack of support provoked fear of infection and death in nurses. Resilience is negatively and significantly related to psychological distress. Resilience can play an important role in improving mental health, but it will only reach higher levels and be a relevant mediator in the stressor–psychological distress relationship when the stressors have induced emotion- and problem-focused strategies. Individually, emotion-focused strategies combat psychological distress and are related to the development of resilience. Problem-focused strategies alone are related to higher levels of psychological stress and distress in nurses. Nurses who experience stress due to insufficient preparation and fear of contagion do not implement adequate coping strategies and thus will not be able to acquire resilience. | STROBE 20/22 JBI 4b-C |
| Rieckert A et al., 2021 [46] Nether- lands | Scoping review. 73 articles. | To explore how to develop and maintain the resilience of frontline healthcare professionals exposed to the working conditions of the COVID-19 outbreak. | Interventions before or during the outbreak to build nurse resilience. | Recommendations prior to the outbreak to promote resilience included: optimal provision of education, resilience training, and interventions to create a sense of preparedness for clinical practice. Recommendations during the outbreak consisted of: enhancing resilience through adequate provision of information, psychosocial support, and treatment; monitoring the health status of practitioners; and utilizing various forms and contents of psychosocial support. | AMSTAR-2 RATING Moderate JBI 4a-C |
| Balay-Odao et al., 2021 [27] Saudi Arabia | Observational, descriptive, cross-sectional study. 281 nurses. | To determine predictors of hospital preparedness in the management of patients with COVID-19 and psychological burden and resilience among clinical nurses in addressing the COVID-19 crisis in Saudi Arabia. | Influencing factors in the psychological burden of nurses. | The relevant factors that were revealed as predictors of psychological burden in nurses were: being female, living with family members, being married, working in the emergency area or isolation room, not being trained for the integral management of the patient with COVID-19, and having a low economic level. The nurses perceived high hospital preparedness to correlate with moderate–high levels of resilience, decreasing the mean score of anxiety, stress, and depression. Factors such as age, experience, educational level, degree of trust in authorities, and perceived social and family support fostered resilience and reduced nurses’ psychological burden. Hospital preparation, prevention, control, management, and containment of COVID-19, and government, social, and family support for nurses were relevant aspects that favored resilience. Having a learning attitude, positive thinking, and acquiring updated training were resilience strategies for nurses to adapt psychologically in a more optimal way. | STROBE 18/22 JBI 4b-C |
| Del Pozo-Herce et al., 2021 [31] Spain | Observational, descriptive, cross-sectional study. 605 health professionals: −63.14% nurses. −36.28% nursing assistants. | To determine the psychological impact of the SARS-CoV-2 virus on nursing professionals working in the Rioja Health Service (Spain). | Stressors and protective factors. Perceived emotions. | Influencing factors such as being a woman, being younger and less experienced, not having a consolidated contract, having dependent family members, and being in contact with COVID-19 patients gave rise to concerns about fear of becoming infected or infecting their loved ones, making mistakes, as well as negativism, emotional destabilization, and sadness for not providing adequate physical and/or psychoemotional care to the patient’s needs. The strategies developed by the health professionals were: seeking help from prepared materials, bibliographies, and psychological resources available online. A very small percentage sought specialized external help. Women used fewer coping strategies. | STROBE 20/22 JBI 4b-C |
| De Pinho et al., 2021 [30] Portugal | Observational, descriptive, cross-sectional study. 820 nurses. | To explore the association between mental-health-promotion strategies used by nurses during the COVID-19 outbreak and their symptoms of depression, anxiety, and stress. | Strategies to promote mental health. | Healthy eating, physical activity, resting between shifts, maintaining social contacts, verbalizing feelings/emotions, and spending less time seeking information on COVID-19 were strategies developed by nurses that were associated with better mental health. | STROBE 19/22 JBI 4b-C |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sierra-García, E.; Sosa-Palanca, E.M.; Saus-Ortega, C.; Ruiz-Hontangas, A.; Juárez-Vela, R.; Gea-Caballero, V. Modulating Elements of Nurse Resilience in Population Care during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4452. https://doi.org/10.3390/ijerph19084452
Sierra-García E, Sosa-Palanca EM, Saus-Ortega C, Ruiz-Hontangas A, Juárez-Vela R, Gea-Caballero V. Modulating Elements of Nurse Resilience in Population Care during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(8):4452. https://doi.org/10.3390/ijerph19084452
Chicago/Turabian StyleSierra-García, Ester, Eva María Sosa-Palanca, Carlos Saus-Ortega, Antonio Ruiz-Hontangas, Raúl Juárez-Vela, and Vicente Gea-Caballero. 2022. "Modulating Elements of Nurse Resilience in Population Care during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 8: 4452. https://doi.org/10.3390/ijerph19084452
APA StyleSierra-García, E., Sosa-Palanca, E. M., Saus-Ortega, C., Ruiz-Hontangas, A., Juárez-Vela, R., & Gea-Caballero, V. (2022). Modulating Elements of Nurse Resilience in Population Care during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(8), 4452. https://doi.org/10.3390/ijerph19084452