
A Radiographic and Clinical Comparison of Immediate vs. Early Loading (4 Weeks) of Implants with a New Thermo-Chemically Treated Surface: A Randomized Clinical Trial

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
- -
- Undisturbed, completely healed edentulous sites, at least four months after tooth/teeth extraction;
- -
- Adequate bone volume verified by CBCT (cone beam computed tomography) for the placement of a dental implant of at least 8 mm in length and 3.5 mm in diameter; this means at least 9 mm of bone in the vertical dimension and 6.5 mm in the horizontal dimension;
- -
- No bone regeneration procedures required;
- -
- Adequate prosthetic conditions for proper crown or bridge installation;
- -
- Natural antagonist dentition, whether restored or untreated teeth;
- -
- Presence of at least 4 mm of keratinized mucosa from the buccal to lingual side of the edentulous ridge;
- -
- Absence of oral infections, gingival inflammation, untreated periodontitis, or mucosal diseases.
2.2. General Exclusion Criteria
- -
- Uncontrolled systemic diseases;
- -
- Pregnancy;
- -
- Bone-related disorders such as osteoporosis;
- -
- Drug abuse or alcoholism;
- -
- Smoking habit of >10 cigarettes per day;
- -
- Severe bruxism or severe temporomandibular junction disorders;
- -
- Previous history of implant failure.
2.3. Location and Clinicians
2.4. Implants and Abutments
2.5. Pre-Treatment Procedures
2.6. Surgical Interventions
- (A)
- Manually, by means of a calibrated torsion torque wrench (Klockner Implant System, SOADCO S.L., Andorra) at the time of placing the implant.
- (B)
- Manually, after the use of the torque wrench, according to the following criteria at the time of the abutment connection: Type A: IT > 35 N/cm, and the implant could not be rotated manually; type B: IT < 35 N/cm and the implant could not be rotated manually; type C: IT < 35 N/cm and the implant could be rotated manually; type D: the implant could be rotated manually and moved in a vertical direction. In this case (i.e., type D), the patient was excluded from the study, and a delayed loading protocol was carried out.
- (C)
- By radiofrequency, using the Osstell® device and Osstell® transducers (Smart-Pegs®) (Osstell®, Gothenburg, Sweden) in order to obtain of the implant stability quotient (ISQ) values. The transducers were connected to the abutments, screwed at 5 N/cm.
2.7. Prosthetic Procedure
2.8. Outcomes
2.9. Provisional and Definitive Restoration Follow-Ups
2.10. Adverse Events
2.11. PROMs (Patient-Reported Outcome Measures)
2.12. Statistical Analysis
3. Results
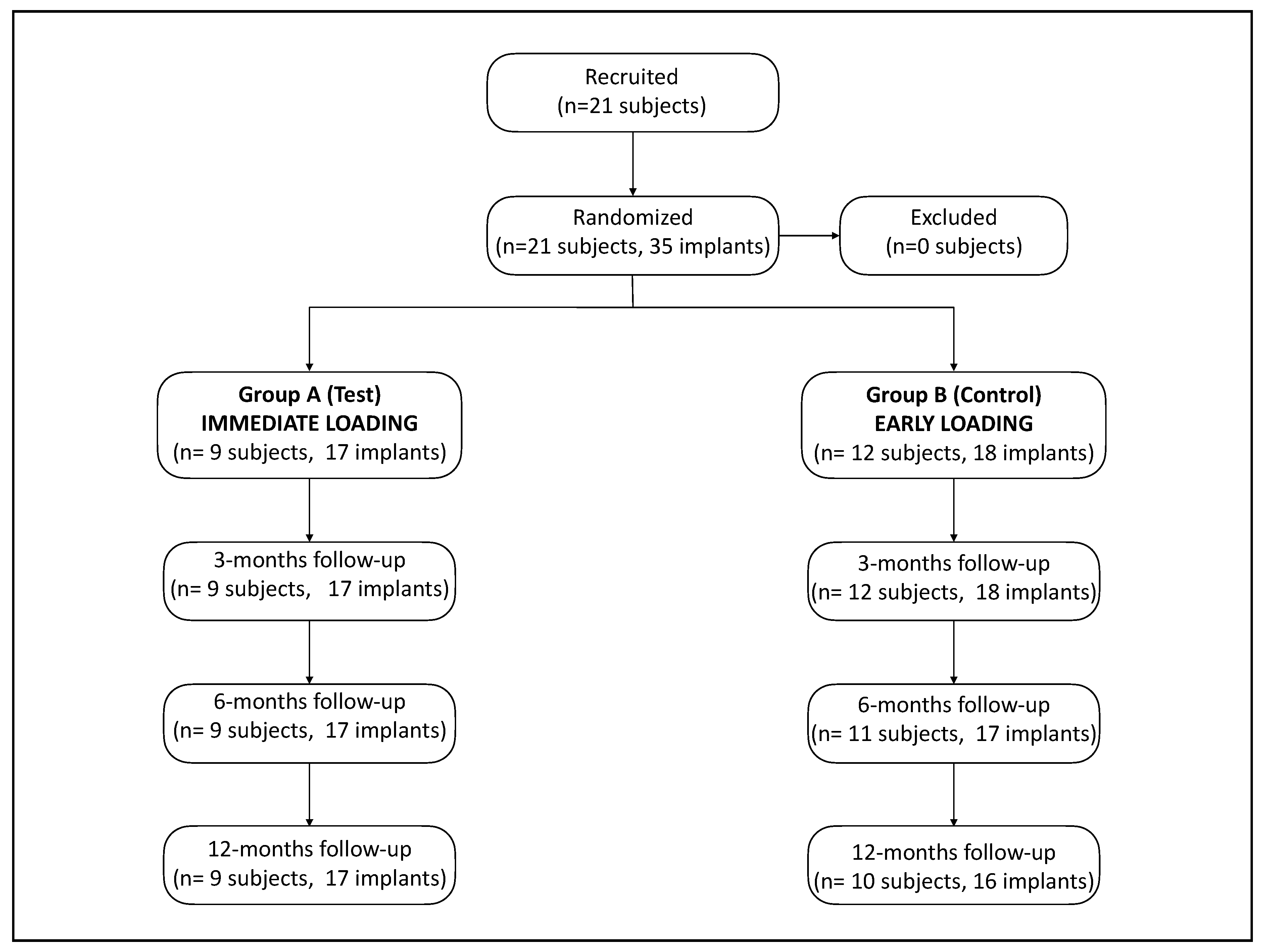
3.1. Study Population
3.2. Demographic Data
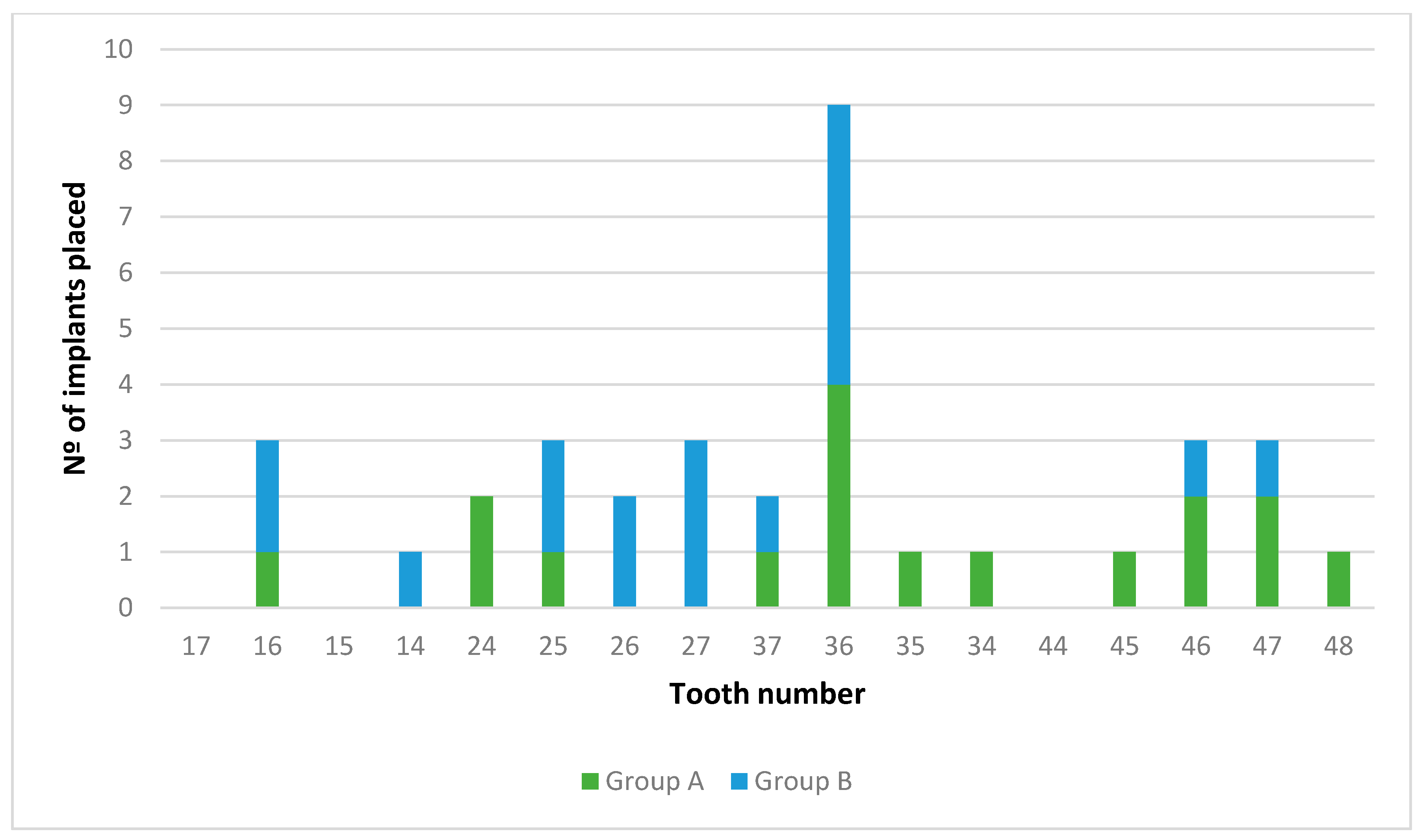
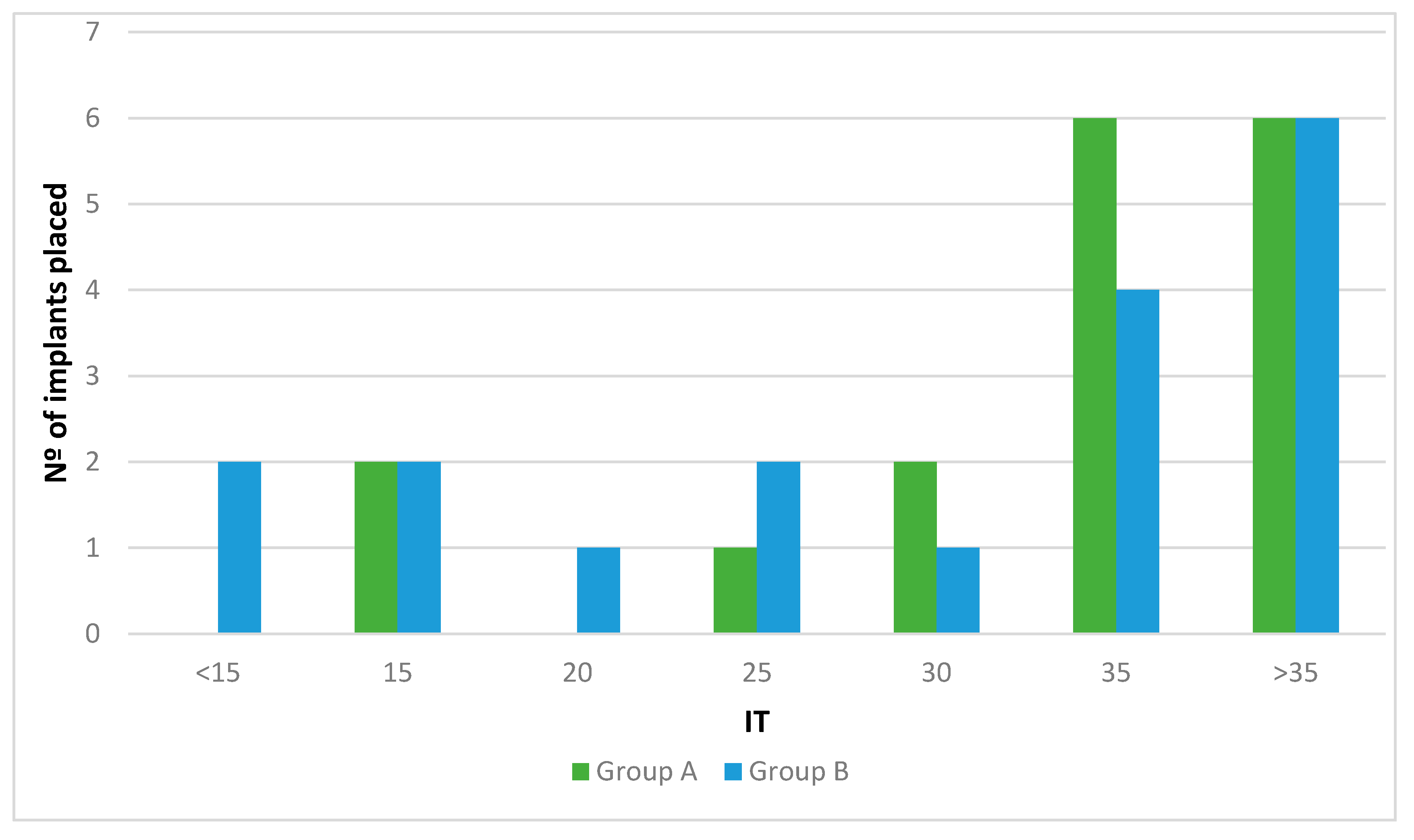
3.3. Interventions
3.4. Clinical Variables
3.5. ISQ measurements
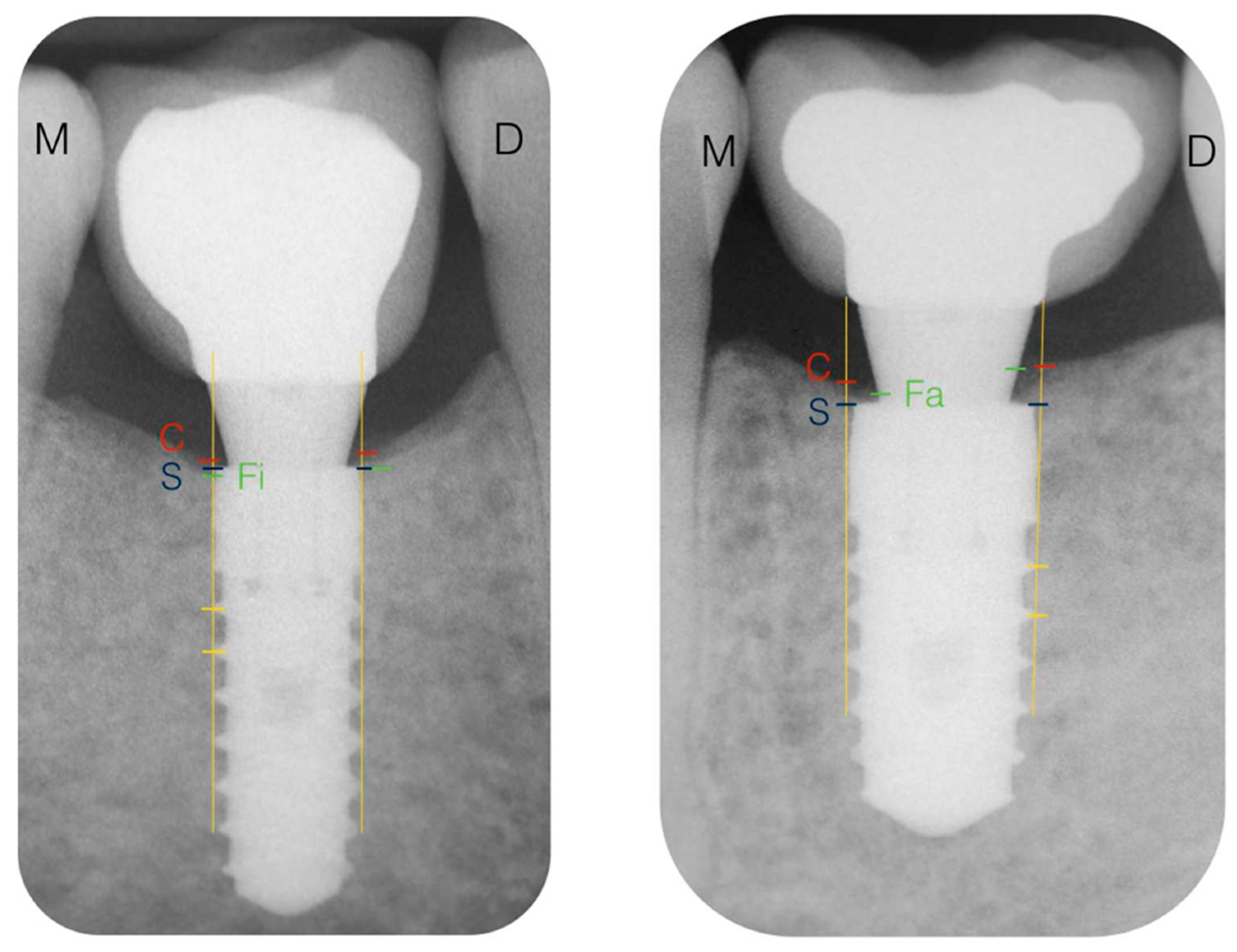
3.6. Radiographic Variables: Changes of Marginal Bone Level (CMBL)
- Marginal bone level at the crest (MBLc): There were no statistically significant differences between groups (p = 0.12). Analyzing the MBLc according to the moment when it was measured, there were statistically significant differences between all surgeries and the rest of the moments of registration (4, 8, and 12 weeks and 6 and 12 months). There were no statistically significant differences (p = 0.00) between the MBLc at all follow-up visits.
- Marginal bone level at the implant (MBLi): There were no statistically significant differences between groups (p = 0.195). Analyzing the MBLi according to the moment when it was measured, there were statistically significant differences only between the moment of surgery and 12 weeks. There were no statistically significant differences (p = 0.00) between the MBLi at any other moment.
- Marginal bone level at the abutment (MBLa): There were statistically significant differences between groups (p = 0.042). Analyzing the MBLa according to the moment when it was measured, there were statistically significant differences (p = 0.024) between the moment of surgery and all of the follow-up visits. Bone contact at the abutment was observed in 51.35% and 61.7% of the implants at 4 and 12 weeks, respectively. These values remained constant after 6 and 12 months with a rate of 63.6% and 67.6%. At the end of the observation period (one year), 66.6% of the implants in Group A and 68.75% in Group B showed bone contact at the abutment. None of these differences were statistically significant.
3.7. Patient-Reported Outcome Measurements (PROMs)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontology 2000 2017, 73, 7–21. [Google Scholar] [CrossRef]
- Gallardo, Y.N.R.; da Silva-Olivio, I.R.; Gonzaga, L.; Sesma, N.; Martin, W. A Systematic Review of Clinical Outcomes on Patients Rehabilitated with Complete-Arch Fixed Implant-Supported Prostheses According to the Time of Loading. J. Prosthodont. 2019, 28, 958–968. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Chen, C.J.; Chuang, S.K.; Weber, H.P. Implant loading protocols for edentulous patients with fixed prostheses: A systematic review and meta-analysis. Int. J. Oral. Maxillofac. Implant. 2014, 29, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Grusovin, M.G.; Maghaireh, H.; Worthington, H.V. Interventions for replacing missing teeth: Different times for loading dental implants. Cochrane Database Syst. Rev. 2013, 2013, CD003878. [Google Scholar] [CrossRef] [PubMed]
- Weber, H.P.; Morton, D.; Gallucci, G.O.; Roccuzzo, M.; Cordaro, L.; Grutter, L. Consensus statements and recommended clinical procedures regarding loading protocols. Int. J. Oral. Maxillofac. Implant. 2009, 24, 180–183. [Google Scholar]
- De Bruyn, H.; Raes, S.; Ostman, P.O.; Cosyn, J. Immediate loading in partially and completely edentulous jaws: A review of the literature with clinical guidelines. Periodontology 2000 2014, 66, 153–187. [Google Scholar] [CrossRef]
- Han, J.; Tang, Z.; Zhang, X.; Meng, H. A prospective, multi-center study assessing early loading with short implants in posterior regions. A 3-year post-loading follow-up study. Clin. Implant. Dent. Relat. Res. 2018, 20, 34–42. [Google Scholar] [CrossRef]
- Nicolau, P.; Korostoff, J.; Ganeles, J.; Jackowski, J.; Krafft, T.; Neves, M.; Divi, J.; Rasse, M.; Guerra, F.; Fischer, K. Immediate and early loading of chemically modified implants in posterior jaws: 3-year results from a prospective randomized multicenter study. Clin. Implant. Dent. Relat. Res. 2013, 15, 600–612. [Google Scholar] [CrossRef]
- Weerapong, K.; Sirimongkolwattana, S.; Sastraruji, T.; Khongkhunthian, P. Comparative study of immediate loading on short dental implants and conventional dental implants in the posterior mandible: A randomized clinical trial. Int. J. Oral. Maxillofac. Implant. 2019, 34, 141–149. [Google Scholar] [CrossRef]
- Smeets, R.; Stadlinger, B.; Schwarz, F.; Beck-Broichsitter, B.; Jung, O.; Precht, C.; Kloss, F.; Grobe, A.; Heiland, M.; Ebker, T. Impact of Dental Implant Surface Modifications on Osseointegration. Biomed. Res. Int. 2016, 2016, 6285620. [Google Scholar] [CrossRef]
- Felice, P.; Grusovin, M.G.; Barausse, C.; Grandi, G.; Esposito, M. Safety and effectiveness of early loaded maxillary titanium implants with a novel nanostructured calcium-incorporated surface (Xpeed): 3-year results from a pilot multicenter randomised controlled trial. Eur. J. Oral. Implantol. 2015, 8, 245–254. [Google Scholar] [PubMed]
- Ong, J.L.; Chan, D.C. Hydroxyapatite and their use as coatings in dental implants: A review. Crit. Rev. Biomed. Eng. 2000, 28, 667–707. [Google Scholar] [CrossRef] [PubMed]
- van Oirschot, B.A.; Bronkhorst, E.M.; van den Beucken, J.J.; Meijer, G.J.; Jansen, J.A.; Junker, R. Long-term survival of calcium phosphate-coated dental implants: A meta-analytical approach to the clinical literature. Clin. Oral Implant. Res. 2013, 24, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Xuereb, M.; Camilleri, J.; Attard, N.J. Systematic review of current dental implant coating materials and novel coating techniques. Int. J. Prosthodont. 2015, 28, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Roy, M.; Bandyopadhyay, A.; Bose, S. Induction Plasma Sprayed Nano Hydroxyapatite Coatings on Titanium for Orthopaedic and Dental Implants. Surf. Coat. Technol. 2011, 205, 2785–2792. [Google Scholar] [CrossRef] [PubMed]
- Cannizzaro, G.; Felice, P.; Minciarelli, A.F.; Leone, M.; Viola, P.; Esposito, M. Early implant loading in the atrophic posterior maxilla: 1-stage lateral versus crestal sinus lift and 8 mm hydroxyapatite-coated implants. A 5-year randomised controlled trial. Eur. J. Oral. Implantol. 2013, 6, 13–25. [Google Scholar]
- Mistry, S.; Roy, R.; Kundu, B.; Datta, S.; Kumar, M.; Chanda, A.; Kundu, D. Clinical Outcome of Hydroxyapatite Coated, Bioactive Glass Coated, and Machined Ti6Al4V Threaded Dental Implant in Human Jaws: A Short-Term Comparative Study. Implant. Dent. 2016, 25, 252–260. [Google Scholar] [CrossRef]
- Ichikawa, T.; Hirota, K.; Kanitani, H.; Wigianto, R.; Kawamoto, N.; Matsumoto, N.; Miyake, Y. Rapid bone resorption adjacent to hydroxyapatite-coated implants. J. Oral. Implantol. 1996, 22, 232–235. [Google Scholar]
- van Oirschot, B.A.; Bronkhorst, E.M.; van den Beucken, J.J.; Meijer, G.J.; Jansen, J.A.; Junker, R. A systematic review on the long-term success of calcium phosphate plasma-spray-coated dental implants. Odontology 2016, 104, 347–356. [Google Scholar] [CrossRef]
- Kokubo, T.; Kushitani, H.; Sakka, S.; Kitsugi, T.; Yamamuro, T. Solutions able to reproduce in vivo surface-structure changes in bioactive glass-ceramic A-W. J. Biomed. Mater. Res. 1990, 24, 721–734. [Google Scholar] [CrossRef]
- Kokubo, T.; Takadama, H. How useful is SBF in predicting in vivo bone bioactivity? Biomaterials 2006, 27, 2907–2915. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.M.; Miyaji, F.; Kokubo, T.; Nakamura, T. Preparation of bioactive Ti and its alloys via simple chemical surface treatment. J. Biomed. Mater. Res. 1996, 32, 409–417. [Google Scholar] [CrossRef]
- Aparicio, C.; Manero, J.M.; Conde, F.; Pegueroles, M.; Planell, J.A.; Vallet-Regi, M.; Gil, F.J. Acceleration of apatite nucleation on microrough bioactive titanium for bone-replacing implants. J. Biomed. Mater. Res. A 2007, 82, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Nishiguchi, S.; Fujibayashi, S.; Kim, H.M.; Kokubo, T.; Nakamura, T. Biology of alkali- and heat-treated titanium implants. J. Biomed. Mater. Res. A 2003, 67, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Pattanayak, D.K.; Yamaguchi, S.; Matsushita, T.; Kokubo, T. Nanostructured positively charged bioactive TiO2 layer formed on Ti metal by NaOH, acid and heat treatments. J. Mater. Sci. Mater. Med. 2011, 22, 1803–1812. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Gil, F.J.; Planell, J.A.; Engel, E. Human-osteoblast proliferation and differentiation on grit-blasted and bioactive titanium for dental applications. J. Mater. Sci. Mater. Med. 2002, 13, 1105–1111. [Google Scholar] [CrossRef] [PubMed]
- Nogueras-Bayona, J.; Gil, F.J.; Salsench, J.; Martinez-Gomis, J. Roughness and bonding strength of bioactive apatite layer on dental implants. Implant. Dent. 2004, 13, 185–189. [Google Scholar] [CrossRef][Green Version]
- Albertini, M.; Fernandez-Yague, M.; Lazaro, P.; Herrero-Climent, M.; Rios-Santos, J.V.; Bullon, P.; Gil, F.J. Advances in surfaces and osseointegration in implantology. Biomimetic surfaces. Med. Oral. Patol. Oral. Cir. Bucal. 2015, 20, e316–e325. [Google Scholar] [CrossRef]
- Aparicio, C.; Padros, A.; Gil, F.J. In vivo evaluation of micro-rough and bioactive titanium dental implants using histometry and pull-out tests. J. Mech. Behav. Biomed. Mater. 2011, 4, 1672–1682. [Google Scholar] [CrossRef]
- Simmons, D.E.; Palaiologou, A.; Teitelbaum, A.G.; Billiot, S.; Popat, L.J.; Maney, P. Immediate and Early Loading of Hydrothermally Treated, Hydroxyapatite-Coated Dental Implants: 2-Year Results from a Prospective Clinical Study. J. Oral. Implantol. 2016, 42, 17–25. [Google Scholar] [CrossRef]
- Lazzara, R.J.; Porter, S.S. Platform switching: A new concept in implant dentistry for controlling postrestorative crestal bone levels. Int. J. Periodontics Restor. Dent. 2006, 26, 9–17. [Google Scholar]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Platform switch and dental implants: A meta-analysis. J. Dent. 2015, 43, 629–646. [Google Scholar] [CrossRef] [PubMed]
- Santiago, J.F., Jr.; Batista, V.E.; Verri, F.R.; Honorio, H.M.; de Mello, C.C.; Almeida, D.A.; Pellizzer, E.P. Platform-switching implants and bone preservation: A systematic review and meta-analysis. Int. J. Oral. Maxillofac. Surg. 2016, 45, 332–345. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, I.; Berglundh, T.; Lindhe, J. The mucosal barrier following abutment dis/reconnection. An experimental study in dogs. J. Clin. Periodontol. 1997, 24, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Alves, C.C.; Munoz, F.; Cantalapiedra, A.; Ramos, I.; Neves, M.; Blanco, J. Marginal bone and soft tissue behavior following platform switching abutment connection/disconnection—A dog model study. Clin. Oral Implant. Res. 2015, 26, 983–991. [Google Scholar] [CrossRef]
- Becker, K.; Mihatovic, I.; Golubovic, V.; Schwarz, F. Impact of abutment material and dis-/re-connection on soft and hard tissue changes at implants with platform-switching. J. Clin. Periodontol. 2012, 39, 774–780. [Google Scholar] [CrossRef]
- Degidi, M.; Nardi, D.; Piattelli, A. One abutment at one time: Non-removal of an immediate abutment and its effect on bone healing around subcrestal tapered implants. Clin. Oral Implant. Res. 2011, 22, 1303–1307. [Google Scholar] [CrossRef]
- Grandi, T.; Guazzi, P.; Samarani, R.; Garuti, G. Immediate positioning of definitive abutments versus repeated abutment replacements in immediately loaded implants: Effects on bone healing at the 1-year follow-up of a multicentre randomised controlled trial. Eur. J. Oral. Implantol. 2012, 5, 9–16. [Google Scholar]
- Molina, A.; Sanz-Sanchez, I.; Martin, C.; Blanco, J.; Sanz, M. The effect of one-time abutment placement on interproximal bone levels and peri-implant soft tissues: A prospective randomized clinical trial. Clin. Oral Implant. Res. 2017, 28, 443–452. [Google Scholar] [CrossRef]
- Armitage, G.C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef]
- Misch, C.E. Divisions of available bone in implant dentistry. Int. J. Oral. Implantol. 1990, 7, 9–17. [Google Scholar] [PubMed]
- Kokovic, V.; Jung, R.; Feloutzis, A.; Todorovic, V.S.; Jurisic, M.; Hammerle, C.H. Immediate vs. early loading of SLA implants in the posterior mandible: 5-year results of randomized controlled clinical trial. Clin. Oral Implant. Res. 2014, 25, e114–e119. [Google Scholar] [CrossRef] [PubMed]
- Zollner, A.; Ganeles, J.; Korostoff, J.; Guerra, F.; Krafft, T.; Bragger, U. Immediate and early non-occlusal loading of Straumann implants with a chemically modified surface (SLActive) in the posterior mandible and maxilla: Interim results from a prospective multicenter randomized-controlled study. Clin. Oral Implant. Res. 2008, 19, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Gil, F.J.; Manzanares, N.; Badet, A.; Aparicio, C.; Ginebra, M.P. Biomimetic treatment on dental implants for short-term bone regeneration. Clin. Oral Investig. 2014, 18, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Di Girolamo, M.; Calcaterra, R.; Di Gianfilippo, R.; Arcuri, C.; Baggi, L. Bone level changes around platform switching and platform matching implants: A systematic review with meta-analysis. Oral. Implantol. (Rome) 2016, 9, 1–10. [Google Scholar] [PubMed]
- Annibali, S.; Bignozzi, I.; Cristalli, M.P.; Graziani, F.; La Monaca, G.; Polimeni, A. Peri-implant marginal bone level: A systematic review and meta-analysis of studies comparing platform switching versus conventionally restored implants. J. Clin. Periodontol. 2012, 39, 1097–1113. [Google Scholar] [CrossRef]
- Atieh, M.A.; Ibrahim, H.M.; Atieh, A.H. Platform switching for marginal bone preservation around dental implants: A systematic review and meta-analysis. J. Periodontol. 2010, 81, 1350–1366. [Google Scholar] [CrossRef]
- Gracis, S.; Michalakis, K.; Vigolo, P.; von Steyern, P.V.; Zwahlen, M.; Sailer, I. Internal vs. external connections for abutments/reconstructions: A systematic review. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 202–216. [Google Scholar] [CrossRef]
- Cochran, D.L.; Mau, L.P.; Higginbottom, F.L.; Wilson, T.G.; Bosshardt, D.D.; Schoolfield, J.; Jones, A.A. Soft and hard tissue histologic dimensions around dental implants in the canine restored with smaller-diameter abutments: A paradigm shift in peri-implant biology. Int. J. Oral. Maxillofac. Implant. 2013, 28, 494–502. [Google Scholar] [CrossRef][Green Version]
- Esposito, M.; Bressan, E.; Grusovin, M.G.; D’Avenia, F.; Neumann, K.; Sbricoli, L.; Luongo, G. Do repeated changes of abutments have any influence on the stability of peri-implant tissues? One-year post-loading results from a multicentre randomised controlled trial. Eur. J. Oral. Implantol. 2017, 10, 57–72. [Google Scholar]
- Cochran, D.L.; Bosshardt, D.D.; Grize, L.; Higginbottom, F.L.; Jones, A.A.; Jung, R.E.; Wieland, M.; Dard, M. Bone response to loaded implants with non-matching implant-abutment diameters in the canine mandible. J. Periodontol. 2009, 80, 609–617. [Google Scholar] [CrossRef] [PubMed]
- de Siqueira, R.A.C.; Fontao, F.; Sartori, I.A.M.; Santos, P.G.F.; Bernardes, S.R.; Tiossi, R. Effect of different implant placement depths on crestal bone levels and soft tissue behavior: A randomized clinical trial. Clin. Oral Implant. Res. 2017, 28, 1227–1233. [Google Scholar] [CrossRef] [PubMed]
- Fetner, M.; Fetner, A.; Koutouzis, T.; Clozza, E.; Tovar, N.; Sarendranath, A.; Coelho, P.G.; Neiva, K.; Janal, M.N.; Neiva, R. The Effects of Subcrestal Implant Placement on Crestal Bone Levels and Bone-to-Abutment Contact: A Microcomputed Tomographic and Histologic Study in Dogs. Int. J. Oral. Maxillofac. Implant. 2015, 30, 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Di Mambro, A.; Giansanti, M.; Brandetti, G.; Calasso, S. A 36-month follow-up prospective cohort study on peri-implant bone loss of Morse Taper connection implants with platform switching. J. Oral. Sci. 2016, 58, 49–57. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Huang, B.; Meng, H.; Zhu, W.; Witek, L.; Tovar, N.; Coelho, P.G. Influence of placement depth on bone remodeling around tapered internal connection implants: A histologic study in dogs. Clin. Oral Implant. Res. 2015, 26, 942–949. [Google Scholar] [CrossRef]
- Degidi, M.; Perrotti, V.; Shibli, J.A.; Novaes, A.B.; Piattelli, A.; Iezzi, G. Equicrestal and subcrestal dental implants: A histologic and histomorphometric evaluation of nine retrieved human implants. J. Periodontol. 2011, 82, 708–715. [Google Scholar] [CrossRef]
- Koutouzis, T.; Neiva, R.; Nair, M.; Nonhoff, J.; Lundgren, T. Cone beam computed tomographic evaluation of implants with platform-switched Morse taper connection with the implant-abutment interface at different levels in relation to the alveolar crest. Int. J. Oral. Maxillofac. Implant. 2014, 29, 1157–1163. [Google Scholar] [CrossRef]
- Degidi, M.; Daprile, G.; Piattelli, A. Marginal bone loss around implants with platform-switched Morse-cone connection: A radiographic cross-sectional study. Clin. Oral Implant. Res. 2017, 28, 1108–1112. [Google Scholar] [CrossRef]
- Schwarz, F.; Alcoforado, G.; Nelson, K.; Schaer, A.; Taylor, T.; Beuer, F.; Strietzel, F.P. Impact of implant-abutment connection, positioning of the machined collar/microgap, and platform switching on crestal bone level changes. Camlog Foundation Consensus Report. Clin. Oral Implant. Res. 2014, 25, 1301–1303. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Coulthard, P.; Worthington, H.V. Different loading strategies of dental implants: A Cochrane systematic review of randomised controlled clinical trials. Eur. J. Oral. Implantol. 2008, 1, 259–276. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; Willings, M.; Coulthard, P.; Worthington, H.V. The effectiveness of immediate, early, and conventional loading of dental implants: A Cochrane systematic review of randomized controlled clinical trials. Int. J. Oral. Maxillofac. Implant. 2007, 22, 893–904. [Google Scholar]
- Lioubavina-Hack, N.; Lang, N.P.; Karring, T. Significance of primary stability for osseointegration of dental implants. Clin. Oral. Implant. Res. 2006, 17, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Strub, J.R.; Jurdzik, B.A.; Tuna, T. Prognosis of immediately loaded implants and their restorations: A systematic literature review. J. Oral. Rehabil. 2012, 39, 704–717. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Lang, N.P.; Rangert, B. Validity and clinical significance of biomechanical testing of implant/bone interface. Clin. Oral Implant. Res. 2006, 17 (Suppl. 2), 2–7. [Google Scholar] [CrossRef]
- Herrero-Climent, M.; Albertini, M.; Rios-Santos, J.V.; Lazaro-Calvo, P.; Fernandez-Palacin, A.; Bullon, P. Resonance frequency analysis-reliability in third generation instruments: Osstell mentor(R). Med. Oral. Patol. Oral. Cir. Bucal. 2012, 17, e801–e806. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.M.; Chiu, C.L.; Yeh, C.Y.; Lee, S.Y. Factors influencing the resonance frequency of dental implants. J. Oral. Maxillofac. Surg. 2003, 61, 1184–1188. [Google Scholar] [CrossRef]
- Manzano-Moreno, F.J.; Herrera-Briones, F.J.; Bassam, T.; Vallecillo-Capilla, M.F.; Reyes-Botella, C. Factors Affecting Dental Implant Stability Measured Using the Ostell Mentor Device: A Systematic Review. Implant. Dent. 2015, 24, 565–577. [Google Scholar] [CrossRef]
- Lachmann, S.; Jager, B.; Axmann, D.; Gomez-Roman, G.; Groten, M.; Weber, H. Resonance frequency analysis and damping capacity assessment. Part I: An in vitro study on measurement reliability and a method of comparison in the determination of primary dental implant stability. Clin. Oral Implant. Res. 2006, 17, 75–79. [Google Scholar] [CrossRef]
- Han, J.; Lulic, M.; Lang, N.P. Factors influencing resonance frequency analysis assessed by Osstell mentor during implant tissue integration: II. Implant surface modifications and implant diameter. Clin. Oral Implant. Res. 2010, 21, 605–611. [Google Scholar] [CrossRef]
- Huwiler, M.A.; Pjetursson, B.E.; Bosshardt, D.D.; Salvi, G.E.; Lang, N.P. Resonance frequency analysis in relation to jawbone characteristics and during early healing of implant installation. Clin. Oral Implant. Res. 2007, 18, 275–280. [Google Scholar] [CrossRef]
- Nedir, R.; Bischof, M.; Szmukler-Moncler, S.; Bernard, J.P.; Samson, J. Predicting osseointegration by means of implant primary stability. Clin. Oral Implant. Res. 2004, 15, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Bischof, M.; Nedir, R.; Szmukler-Moncler, S.; Bernard, J.P.; Samson, J. Implant stability measurement of delayed and immediately loaded implants during healing. Clin. Oral Implant. Res. 2004, 15, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Polo, M.; Ortega, R.; Gomez-Polo, C.; Martin, C.; Celemin, A.; Del Rio, J. Does Length, Diameter, or Bone Quality Affect Primary and Secondary Stability in Self-Tapping Dental Implants? J. Oral. Maxillofac. Surg. 2016, 74, 1344–1353. [Google Scholar] [CrossRef] [PubMed]
- Oates, T.W.; Valderrama, P.; Bischof, M.; Nedir, R.; Jones, A.; Simpson, J.; Toutenburg, H.; Cochran, D.L. Enhanced implant stability with a chemically modified SLA surface: A randomized pilot study. Int. J. Oral. Maxillofac. Implant. 2007, 22, 755–760. [Google Scholar]
- Sim, C.P.; Lang, N.P. Factors influencing resonance frequency analysis assessed by Osstell mentor during implant tissue integration: I. Instrument positioning, bone structure, implant length. Clin. Oral Implant. Res. 2010, 21, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Andres-Garcia, R.; Vives, N.G.; Climent, F.H.; Palacin, A.F.; Santos, V.R.; Climent, M.H.; Bullon, P. In vitro evaluation of the influence of the cortical bone on the primary stability of two implant systems. Med. Oral. Patol. Oral. Cir. Bucal. 2009, 14, E93–E97. [Google Scholar] [PubMed]
- Friberg, B.; Sennerby, L.; Linden, B.; Grondahl, K.; Lekholm, U. Stability measurements of one-stage Branemark implants during healing in mandibles. A clinical resonance frequency analysis study. Int. J. Oral. Maxillofac. Surg. 1999, 28, 266–272. [Google Scholar] [CrossRef]
- Ito, Y.; Sato, D.; Yoneda, S.; Ito, D.; Kondo, H.; Kasugai, S. Relevance of resonance frequency analysis to evaluate dental implant stability: Simulation and histomorphometrical animal experiments. Clin. Oral Implant. Res. 2008, 19, 9–14. [Google Scholar] [CrossRef]
- Brizuela-Velasco, A.; Alvarez-Arenal, A.; Gil-Mur, F.J.; Herrero-Climent, M.; Chavarri-Prado, D.; Chento-Valiente, Y.; Dieguez-Pereira, M. Relationship Between Insertion Torque and Resonance Frequency Measurements, Performed by Resonance Frequency Analysis, in Micromobility of Dental Implants: An In Vitro Study. Implant. Dent. 2015, 24, 607–611. [Google Scholar] [CrossRef]
- Levin, B.P. The Correlation Between Immediate Implant Insertion Torque and Implant Stability Quotient. Int. J. Periodontics Restor. Dent. 2016, 36, 833–840. [Google Scholar] [CrossRef]
- Staedt, H.; Palarie, V.; Staedt, A.; Wolf, J.M.; Lehmann, K.M.; Ottl, P.; Kammerer, P.W. Primary Stability of Cylindrical and Conical Dental Implants in Relation to Insertion Torque-A Comparative Ex Vivo Evaluation. Implant. Dent. 2017, 26, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Herrero-Climent, M.; Lopez-Jarana, P.; Lemos, B.F.; Gil, F.J.; Falcao, C.; Rios-Santos, J.V.; Rios-Carrasco, B. Relevant Design Aspects to Improve the Stability of Titanium Dental Implants. Materials 2020, 13, 1910. [Google Scholar] [CrossRef] [PubMed]
- Meredith, N.; Alleyne, D.; Cawley, P. Quantitative determination of the stability of the implant-tissue interface using resonance frequency analysis. Clin. Oral Implant. Res. 1996, 7, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Meredith, N.; Book, K.; Friberg, B.; Jemt, T.; Sennerby, L. Resonance frequency measurements of implant stability in vivo. A cross-sectional and longitudinal study of resonance frequency measurements on implants in the edentulous and partially dentate maxilla. Clin. Oral Implant. Res. 1997, 8, 226–233. [Google Scholar] [CrossRef]
- Sennerby, L.; Meredith, N. Implant stability measurements using resonance frequency analysis: Biological and biomechanical aspects and clinical implications. Periodontology 2000 2008, 47, 51–66. [Google Scholar] [CrossRef]
- Sennerby, L.; Persson, L.G.; Berglundh, T.; Wennerberg, A.; Lindhe, J. Implant stability during initiation and resolution of experimental periimplantitis: An experimental study in the dog. Clin. Implant. Dent. Relat. Res. 2005, 7, 136–140. [Google Scholar] [CrossRef]
- van Eekeren, P.; Said, C.; Tahmaseb, A.; Wismeijer, D. Resonance Frequency Analysis of Thermal Acid-Etched, Hydrophilic Implants During First 3 Months of Healing and Osseointegration in an Early-Loading Protocol. Int. J. Oral. Maxillofac. Implant. 2015, 30, 843–850. [Google Scholar] [CrossRef]
- Ganeles, J.; Zollner, A.; Jackowski, J.; ten Bruggenkate, C.; Beagle, J.; Guerra, F. Immediate and early loading of Straumann implants with a chemically modified surface (SLActive) in the posterior mandible and maxilla: 1-year results from a prospective multicenter study. Clin. Oral Implant. Res. 2008, 19, 1119–1128. [Google Scholar] [CrossRef]
- Meijer, H.J.; Steen, W.H.; Bosman, F. Standardized radiographs of the alveolar crest around implants in the mandible. J. Prosthet. Dent. 1992, 68, 318–321. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A, Test (IMMEDIATE LOADING) | B, Control (EARLY LOADING) | p-Values | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| mPLI | 4 weeks | 0.13 | 0.25 | 0.08 | 0.17 | 0.590 |
| 3 months | 0.37 | 0.59 | 0.08 | 0.22 | 0.807 | |
| 6 months | 0.09 | 0.22 | 0.06 | 0.11 | 0.892 | |
| 12 months | 0.07 | 0.12 | 0.16 | 0.29 | 0.736 | |
| mSBI | 4 weeks | 1.44 | 0.60 | 1.25 | 0.51 | 0.424 |
| 3 months | 1.31 | 0.35 | 1.17 | 0.28 | 0.219 | |
| 6 months | 1.13 | 0.25 | 1.30 | 0.38 | 0.259 | |
| 12 months | 1.16 | 0.31 | 1.22 | 0.50 | 0.345 | |
| PD | 4 weeks | 1.96 | 0.53 | 2.00 | 0.78 | 0.845 |
| 3 months | 2.13 | 0.65 | 1.79 | 0.65 | 0.132 | |
| 6 months | 2.04 | 0.57 | 2.15 | 0.69 | 0.990 | |
| 12 months | 2.00 | 0.74 | 2.25 | 0.50 | 0.078 | |
| A, Test (IMMEDIATE LOADING) | B, Control (EARLY LOADING) | p-Values | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Asymmetry | 25th Percentile | 75th Percentile | Mean | Median | Asymmetry | 25th Percentile | 75th Percentile | ||
| Surgery | 72.03 d,e | 70.00 | 0.53 | 65.50 | 80.00 | 67.25 h,i | 66.00 | 1.31 | 62.75 | 68.38 | 0.072 |
| 4 weeks | 73.29 a,b,c | 70.50 | 0.68 | 64.50 | 79.50 | 66.94 f,g | 62.25 | 1.11 | 63.38 | 68.25 | 0.041 * |
| 8 weeks | 76.56 | 74.00 | 0.72 | 68.75 | 83.75 | 69.61 j | 68.75 | 1.97 | 65.88 | 69.63 | 0.014 * |
| 3 months | 77.18 a | 72.00 | 0.49 | 69.25 | 84.00 | 70.67 k | 70.00 | 1.68 | 67.00 | 71.50 | 0.049 * |
| 6 months | 78.88 c,e | 73.50 | 0.50 | 70.00 | 89.5 | 72.27 f,h,j | 70.00 | 1.79 | 68.00 | 73.00 | 0.062 |
| 12 months | 79.35 b,d | 73.00 | 0.38 | 70.00 | 88.25 | 72.75 g,I,k | 70.25 | 1.70 | 67.25 | 74.00 | 0.870 |
| A, Test (IMMEDIATE LOADING) | B, Control (EARLY LOADING) | p-Values | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| MBLc | Surgery | 0.87 | 0.59 | 1.25 | 0.39 | 0.03 * |
| 4 weeks | 0.60 | 0.58 | 0.89 | 0.54 | 0.14 | |
| 12 months | 0.51 | 0.63 | 0.76 | 0.70 | 0.28 | |
| MBLa | Surgery | 0.00 | 0.00 | 0.00 | 0.00 | 1 |
| A, Test (IMMEDIATE LOADING) | B, Control (EARLY LOADING) | p-Values | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Asymmetry | 25th Percentile | 75th Percentile | Mean | Median | Asymmetry | 25th Percentile | 75th Percentile | |||
| MBLc | 3 months | 0.53 | 0.67 | 0.07 | 0.08 | 0.85 | 0.92 | 0.75 | 1.39 | 0.58 | 1.20 | 0.089 |
| 6 months | 0.67 | 0.70 | 0.04 | 0.23 | 1.15 | 0.81 | 0.62 | 1.44 | 0.42 | 1.06 | 0.882 | |
| MBLi | Surgery | –0.03 | 0.00 | –3.14 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.386 |
| 4 weeks | –0.10 | 0.00 | –2.46 | –0.02 | 0.00 | –0.02 | 0.00 | –2.71 | 0.00 | 0.00 | 0.557 | |
| 3 months | –0.14 | –0.08 | –1.69 | –0.22 | 0.00 | –0.03 | 0.00 | –2.90 | 0.00 | 0.00 | 0.074 | |
| 6 months | –0.12 | 0.00 | –1.89 | –0.18 | 0.00 | –0.07 | 0.00 | –3.31 | –0.07 | 0.00 | 0.309 | |
| 12 months | –0.12 | 0.00 | –2.48 | –0.10 | 0.00 | –0.27 | 0.00 | –1.75 | –0.57 | 0.00 | 0.794 | |
| MBLa | 4 weeks | 0.45 | 0.27 | 0.96 | 0.00 | 0.81 | 0.37 | 0.22 | 1.09 | 0.00 | 0.69 | 0.658 |
| 3 months | 0.13 | 0.00 | 0.78 | 0.00 | 0.25 | 0.31 | 0.22 | 2.50 | 0.00 | 0.45 | 0.182 | |
| 6 months | 0.24 | 0.20 | 0.88 | 0.00 | 0.42 | 0.31 | 0.00 | 2.46 | 0.00 | 0.46 | 0.657 | |
| 12 months | 0.21 | 0.11 | 1.89 | 0.00 | 0.39 | 0.31 | 0.16 | 2.57 | 0.00 | 0.37 | 0.657 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albertini, M.; Herrero-Climent, F.; Díaz-Castro, C.M.; Nart, J.; Fernández-Palacín, A.; Ríos-Santos, J.V.; Herrero-Climent, M. A Radiographic and Clinical Comparison of Immediate vs. Early Loading (4 Weeks) of Implants with a New Thermo-Chemically Treated Surface: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 1223. https://doi.org/10.3390/ijerph18031223
Albertini M, Herrero-Climent F, Díaz-Castro CM, Nart J, Fernández-Palacín A, Ríos-Santos JV, Herrero-Climent M. A Radiographic and Clinical Comparison of Immediate vs. Early Loading (4 Weeks) of Implants with a New Thermo-Chemically Treated Surface: A Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2021; 18(3):1223. https://doi.org/10.3390/ijerph18031223
Chicago/Turabian StyleAlbertini, Matteo, Federico Herrero-Climent, Carmen María Díaz-Castro, Jose Nart, Ana Fernández-Palacín, José Vicente Ríos-Santos, and Mariano Herrero-Climent. 2021. "A Radiographic and Clinical Comparison of Immediate vs. Early Loading (4 Weeks) of Implants with a New Thermo-Chemically Treated Surface: A Randomized Clinical Trial" International Journal of Environmental Research and Public Health 18, no. 3: 1223. https://doi.org/10.3390/ijerph18031223
APA StyleAlbertini, M., Herrero-Climent, F., Díaz-Castro, C. M., Nart, J., Fernández-Palacín, A., Ríos-Santos, J. V., & Herrero-Climent, M. (2021). A Radiographic and Clinical Comparison of Immediate vs. Early Loading (4 Weeks) of Implants with a New Thermo-Chemically Treated Surface: A Randomized Clinical Trial. International Journal of Environmental Research and Public Health, 18(3), 1223. https://doi.org/10.3390/ijerph18031223