
Assessing Interactions between PNPLA3 and Dietary Intake on Liver Steatosis in Mexican-Origin Adults

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
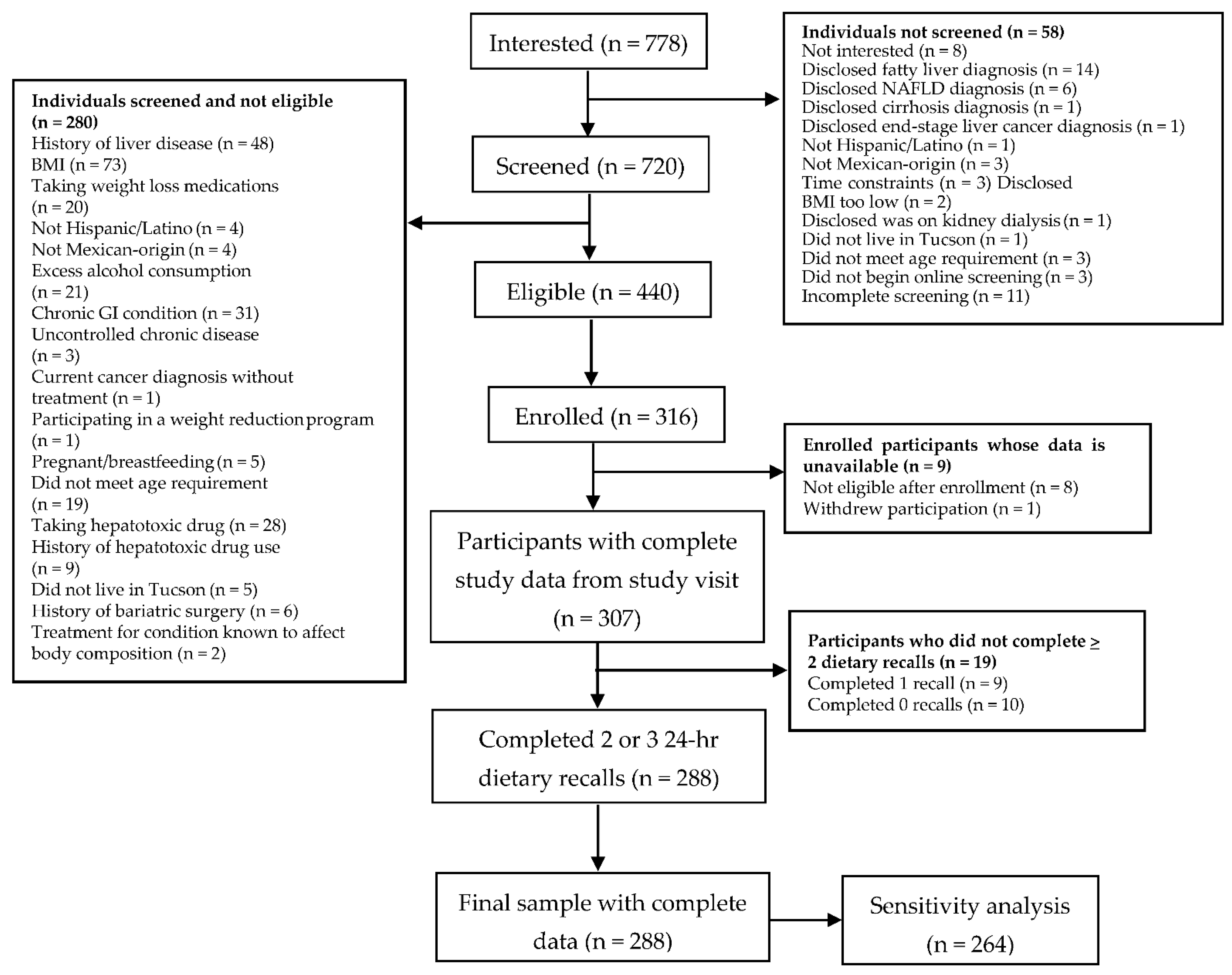
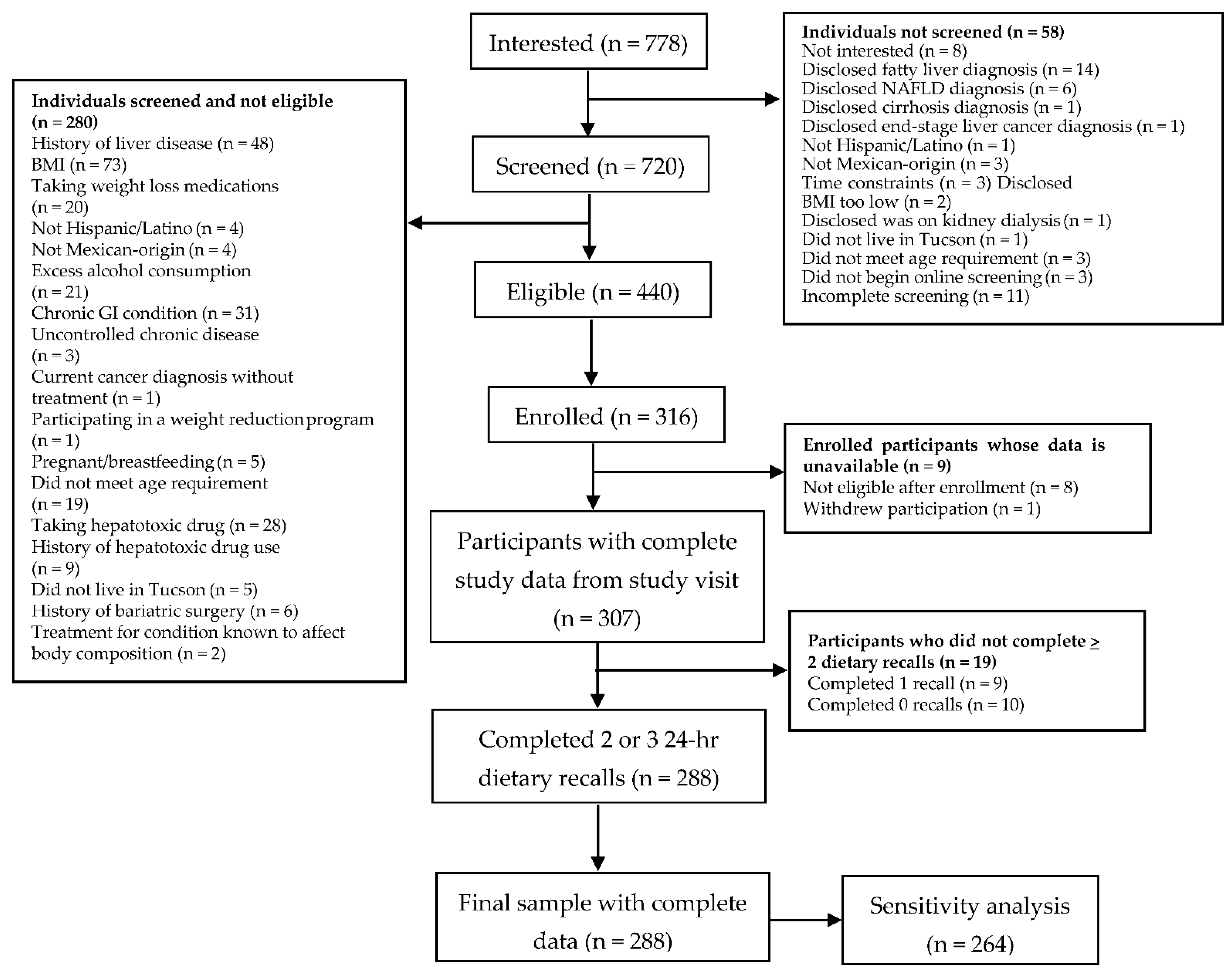
2.1. Study Participation
2.2. Study Measures
2.2.1. Anthropometrics
2.2.2. Liver Steatosis
2.2.3. Dietary Assessment
2.2.4. Genotyping
2.2.5. Statistical Procedures
2.2.6. Sensitivity Analyses
3. Results
Participant Characteristics
4. Discussion
4.1. Strengths and Limitations
4.2. Implications of Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Coefficient | SE | p-Value | |
|---|---|---|---|
| Energy (kcals) | 0.079 | 0.536 | 0.88 |
| Protein (% of energy) | −0.144 | 0.499 | 0.77 |
| Fat (% of energy) | 0.850 | 0.437 | 0.05 |
| n-3 PUFA (% of energy) | 2.777 | 2.675 | 0.30 |
| n-6 PUFA (% of energy) | 0.147 | 0.428 | 0.73 |
| n-6/n-3 PUFA | −0.738 | 1.022 | 0.47 |
| Carbohydrates (% of energy) | 0.544 | 0.342 | 0.11 |
| Fructose (% of energy) | −0.246 | 1.079 | 0.82 |
| Total sugar (% of energy) | −0.337 | 0.393 | 0.39 |
| Added sugar (% of energy) | −0.100 | 0.418 | 0.81 |
| Dietary fiber (g/d) | 0.279 | 0.382 | 0.47 |
| Insoluble fiber (g/d) | 0.566 | 0.550 | 0.31 |
| Soluble fiber (g/d) | −0.041 | 1.032 | 0.97 |
| Glycemic index | −0.627 | 0.566 | 0.27 |
| Glycemic load | −0.039 | 0.071 | 0.58 |
| No Diagnosis of Type 2 Diabetes and Not Currently Using Lipid-Lowering Medication (n = 245) | Diagnosis of Type 2 Diabetes and/or Currently Using Lipid-Lowering Medication (n = 43) | p-Value 2 | |
|---|---|---|---|
| Energy (kcals) | 1439.4 (1144.6, 1793.9) | 1464.1 (1137.1, 1658.3) | 0.94 |
| Protein (g/d) | 64.4 (49.2, 77.9) | 63.4 (55.0, 75.7) | 0.63 |
| Protein (% of energy) | 17.8 (14.6, 21.3) | 18.3 (16.2, 21.7) | 0.35 |
| Fat (g/d) | 54.5 (39.8, 72.7) | 61.0 (42.0, 66.3) | 0.69 |
| Fat (% of energy) | 33.9 (30.2, 39.0) | 35.0 (30.8, 38.9) | 0.41 |
| n-3 PUFA (g/d) | 1.3 (0.8, 1.8) | 1.2 (0.8, 2.1) | 0.79 |
| n-3 PUFA (% of energy) | 0.8 (0.6, 1.0) | 0.8 (0.6, 1.0) | 0.66 |
| n-6 PUFA (g/d) | 10.8 (7.3, 14.8) | 11.2 (7.8, 15.4) | 0.60 |
| n-6 PUFA (% of energy) | 6.6 (5.6, 8.2) | 7.4 (5.5, 8.3) | 0.36 |
| n-6/n-3 PUFA | 8.3 (7.3, 9.8) | 8.4 (7.5, 10.7) | 0.50 |
| Carbohydrates (g/d) | 174.0 (132.0, 218.3) | 166.9 (128.5, 205.9) | 0.61 |
| Carbohydrates (% of energy) | 46.3 (41.7, 51.3) | 45.0 (39.0, 50.0) | 0.36 |
| Fructose (g/d) | 13.6 (7.7, 21.2) | 12.1 (5.9, 17.9) | 0.16 |
| Fructose (% of energy) | 3.7 (2.5, 5.8) | 3.0 (2.0, 4.7) | 0.09 |
| Total sugar (g/d) | 64.1 (46.6, 86.7) | 60.6 (42.2, 79.2) | 0.30 |
| Total sugar (% of energy) | 17.9 (14.0, 23.8) | 15.3 (12.7, 20.8) | 0.10 |
| Added sugar (g/d) | 37.4 (22.9, 57.7) | 32.7 (16.4, 47.0) | 0.16 |
| Added sugar (% of energy) | 10.8 (6.6, 16.0) | 9.1 (5.4, 11.7) | 0.04 |
| Dietary fiber (g/d) | 14.7 (11.4, 20.7) | 16.4 (11.3, 21.2) | 0.42 |
| Insoluble fiber (g/d) | 9.6 (7.2, 13.5) | 11.4 (6.7, 14.8) | 0.48 |
| Soluble fiber (g/d) | 5.1 (3.7, 7.1) | 5.0 (4.0, 7.6) | 0.55 |
| Glycemic index | 56.7 ± 4.9 | 57.5 ± 4.2 | 0.26 |
| Glycemic load | 89.2 (63.7, 109.1) | 88.1 (65.8, 105.5) | 0.84 |
References
- Younossi, Z.M.; Stepanova, M.; Younossi, Y.; Golabi, P.; Mishra, A.; Rafiq, N.; Henry, L. Epidemiology of chronic liver diseases in the USA in the past three decades. Gut 2020, 69, 564–568. [Google Scholar] [CrossRef]
- Fleischman, M.W.; Budoff, M.; Zeb, I.; Li, D.; Foster, T. NAFLD prevalence differs among hispanic subgroups: The multi-ethnic study of atherosclerosis. World J. Gastroenterol. 2014, 20, 4987–4993. [Google Scholar] [CrossRef] [PubMed]
- Lazo, M.; Hernaez, R.; Eberhardt, M.S.; Bonekamp, S.; Kamel, I.; Guallar, E.; Koteish, A.; Brancati, F.L.; Clark, J.M. Prevalence of Nonalcoholic Fatty Liver Disease in the United States: The Third National Health and Nutrition Examination Survey, 1988–1994. Am. J. Epidemiol. 2013, 178, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Harrison, S.A.; Torgerson, S.; Hayashi, P.H. The natural history of nonalcoholic fatty liver disease: A clinical histopathological study. Am. J. Gastroenterol. 2003, 98, 2042–2047. [Google Scholar] [CrossRef]
- Argo, C.K.; Caldwell, S.H. Epidemiology and Natural History of Non-Alcoholic Steatohepatitis. Clin. Liver Dis. 2009, 13, 511–531. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalasani, N.; Younossi, Z.; LaVine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Siegel, R.L.; Fedewa, S.A.; Miller, K.D.; Goding-Sauer, A.; Pinheiro, P.S.; Martinez-Tyson, D.; Jemal, A. Cancer statistics for Hispanics/Latinos, 2015. CA Cancer J. Clin. 2015, 65, 457–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parikh, N.; Marrero, W.J.; Wang, J.; Steuer, J.; Tapper, E.B.; Konerman, M.A.; Singal, A.G.; Hutton, D.W.; Byon, E.; Lavieri, M.S. Projected increase in obesity and non-alcoholic-steatohepatitis-related liver transplantation waitlist additions in the United States. Hepatology 2019, 70, 487–495. [Google Scholar] [CrossRef]
- Cholankeril, G.; Gonzalez, H.C.; Satapathy, S.K.; Gonzalez, S.A.; Hu, M.; Khan, M.A.; Yoo, E.R.; Li, A.; Kim, D.; Nair, S.; et al. Increased Waitlist Mortality and Lower Rate for Liver Transplantation in Hispanic Patients With Primary Biliary Cholangitis. Clin. Gastroenterol. Hepatol. 2018, 16, 965–973.e2. [Google Scholar] [CrossRef]
- Saab, S.; Manne, V.; Nieto, J.; Schwimmer, J.B.; Chalasani, N.P. Nonalcoholic Fatty Liver Disease in Latinos. Clin. Gastroenterol. Hepatol. 2016, 14, 5–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romeo, S.; Kozlitina, J.; Xing, C.; Pertsemlidis, A.; Cox, D.; Pennacchio, L.A.; Boerwinkle, E.; Cohen, J.C.; Hobbs, H.H. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat. Genet. 2008, 40, 1461–1465. [Google Scholar] [CrossRef] [Green Version]
- Martínez, L.A.; Larrieta, E.; Calva, J.J.; Kershenobich, D.; Torre, A. The Expression of PNPLA3 Polymorphism could be the Key for Severe Liver Disease in NAFLD in Hispanic Population. Ann. Hepatol. 2017, 16, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Bruschi, F.V.; Tardelli, M.; Claudel, T.; Trauner, M. PNPLA3 expression and its impact on the liver: Current perspectives. Hepatic Med. 2017, 9, 55–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero-Gómez, M.; Zelber-Sagi, S.; Trenell, M. Treatment of NAFLD with diet, physical activity and exercise. J. Hepatol. 2017, 67, 829–846. [Google Scholar] [CrossRef] [Green Version]
- Barrera, F.; George, J. The Role of Diet and Nutritional Intervention for the Management of Patients with NAFLD. Clin. Liver Dis. 2014, 18, 91–112. [Google Scholar] [CrossRef]
- Jensen, T.; Abdelmalek, M.F.; Sullivan, S.; Nadeau, K.J.; Green, M.; Roncal, C.; Nakagawa, T.; Kuwabara, M.; Sato, Y.; Kang, D.-H.; et al. Fructose and sugar: A major mediator of non-alcoholic fatty liver disease. J. Hepatol. 2018, 68, 1063–1075. [Google Scholar] [CrossRef] [Green Version]
- Pettinelli, P.; Del Pozo, T.; Araya, J.; Rodrigo, R.; Araya, A.V.; Smok, G.; Csendes, A.; Gutierrez, L.; Rojas, J.; Korn, O.; et al. Enhancement in liver SREBP-1c/PPAR-alpha ratio and steatosis in obese patients: Correlations with insulin resistance and n-3 long-chain polyunsaturated fatty acid depletion. Biochim. Biophys. Acta 2009, 1792, 1080–1086. [Google Scholar] [CrossRef] [Green Version]
- Davis, J.N.; Lê, K.-A.; Walker, R.W.; Vikman, S.; Spruijt-Metz, D.; Weigensberg, M.J.; Allayee, H.; Goran, M.I. Increased hepatic fat in overweight Hispanic youth influenced by interaction between genetic variation in PNPLA3 and high dietary carbohydrate and sugar consumption. Am. J. Clin. Nutr. 2010, 92, 1522–1527. [Google Scholar] [CrossRef] [Green Version]
- Dongiovanni, P.; Valenti, L. A Nutrigenomic Approach to Non-Alcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2017, 18, 1534. [Google Scholar] [CrossRef] [Green Version]
- Santoro, N.; Savoye, M.; Kim, G.; Marotto, K.; Shaw, M.M.; Pierpont, B.; Caprio, S. Hepatic Fat Accumulation Is Modulated by the Interaction between the rs738409 Variant in the PNPLA3 Gene and the Dietary Omega6/Omega3 PUFA Intake. PLoS ONE 2012, 7, e37827. [Google Scholar] [CrossRef] [Green Version]
- Sevastianova, K.; Kotronen, A.; Gastaldelli, A.; Perttilä, J.; Hakkarainen, A.; Lundbom, J.; Suojanen, L.; Orho-Melander, M.; Lundbom, N.; Ferrannini, E.; et al. Genetic variation in PNPLA3 (adiponutrin) confers sensitivity to weight loss-induced decrease in liver fat in humans. Am. J. Clin. Nutr. 2011, 94, 104–111. [Google Scholar] [CrossRef]
- Basuray, S.; Smagris, E.; Cohen, J.C.; Hobbs, H.H. The PNPLA3 variant associated with fatty liver disease (I148M) accumulates on lipid droplets by evading ubiquitylation. Hepatology 2017, 66, 1111–1124. [Google Scholar] [CrossRef] [Green Version]
- Scorletti, E.; West, A.; Bhatia, L.; Hoile, S.P.; McCormick, K.G.; Burdge, G.C.; Lillycrop, K.; Clough, G.F.; Calder, P.; Byrne, C.D. Treating liver fat and serum triglyceride levels in NAFLD, effects of PNPLA3 and TM6SF2 genotypes: Results from the WELCOME trial. J. Hepatol. 2015, 63, 1476–1483. [Google Scholar] [CrossRef] [Green Version]
- Stojkovic, I.A.; Ericson, U.; Rukh, G.; Riddestråle, M.; Romeo, S.; Orho-Melander, M. The PNPLA3 Ile148Met interacts with overweight and dietary intakes on fasting triglyceride levels. Genes Nutr. 2014, 9, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liangpunsakul, S.; Beaudoin, J.J.; Shah, V.H.; Puri, P.; Sanyal, A.J.; Kamath, P.S.; Lourens, S.G.; Tang, Q.; Katz, B.P.; Crabb, D.W.; et al. Interaction between the patatin-like phospholipase domain-containing protein 3 genotype and coffee drinking and the risk for acute alcoholic hepatitis. Hepatol. Commun. 2018, 2, 29–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, J.X.Q.; Pradhan, F.; Zimmer, S.; Niu, S.; Crotty, P.; Tracey, J.; Schneider, C.; Heitman, S.J.; Kaplan, G.; Swain, M.G.; et al. The Feasibility and Reliability of Transient Elastography Using Fibroscan®: A Practice Audit of 2335 Examinations. Can. J. Gastroenterol. Hepatol. 2014, 28, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1998. [Google Scholar]
- Mikolasevic, I.; Lukic, A.; Juric, T.; Klapan, M.; Madzar, P.; Krolo, N.; Kolovrat, D.; Jurica, I.; Kedmenec, I.; Kihas, D.; et al. Non-alcoholic fatty liver disease and transient elastography. Explor. Med. 2020, 1, 205–217. [Google Scholar] [CrossRef]
- Mikolasevic, I.; Orlic, L.; Franjic, N.; Hauser, G.; Stimac, D.; Milic, S. Transient elastography (FibroScan®) with controlled attenuation parameter in the assessment of liver steatosis and fibrosis in patients with nonalcoholic fatty liver disease—Where do we stand? World J. Gastroenterol. 2016, 22, 7236–7251. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.M.; Ingwersen, L.A.; Vinyard, B.T.; Moshfegh, A.J. Effectiveness of the US Department of Agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am. J. Clin. Nutr. 2003, 77, 1171–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schakel, S.F.; Buzzard, I.M.; Gebhardt, S.E. Procedures for Estimating Nutrient Values for Food Composition Databases. J. Food Compos. Anal. 1997, 10, 102–114. [Google Scholar] [CrossRef] [Green Version]
- Speliotes, E.K.; Yerges-Armstrong, L.M.; Wu, J.; Hernaez, R.; Kim, L.J.; Palmer, C.D.; Gudnason, V.; Eiriksdottir, G.; Garcia, M.E.; Launer, L.J.; et al. Genome-Wide Association Analysis Identifies Variants Associated with Nonalcoholic Fatty Liver Disease That Have Distinct Effects on Metabolic Traits. PLoS Genet. 2011, 7, e1001324. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Watt, G.P.; De La Cerda, I.; Pan, J.; Fallon, M.B.; Beretta, L.; Loomba, R.; Lee, M.; McCormick, J.B.; Fisher-Hoch, S.P. Elevated Glycated Hemoglobin Is Associated With Liver Fibrosis, as Assessed by Elastography, in a Population-Based Study of M exican A mericans. Hepatol. Commun. 2020, 4, 1793–1801. [Google Scholar] [CrossRef]
- Alferink, L.J.M.; Jong, J.C.K.-D.; Erler, N.S.; Veldt, B.J.; Schoufour, J.D.; De Knegt, R.J.; Ikram, M.A.; Metselaar, H.J.; La Janssen, H.; Franco, O.H.; et al. Association of dietary macronutrient composition and non-alcoholic fatty liver disease in an ageing population: The Rotterdam Study. Gut 2018, 68, 1088–1098. [Google Scholar] [CrossRef]
- Chung, M.; Ma, J.; Patel, K.; Berger, S.; Lau, J.; Lichtenstein, A.H. Fructose, high-fructose corn syrup, sucrose, and nonalcoholic fatty liver disease or indexes of liver health: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 833–849. [Google Scholar] [CrossRef] [Green Version]
- Chiu, S.; Sievenpiper, J.L.; de Souza, R.J.; Cozma, A.I.; Mirrahimi, A.; Carleton, A.J.; Ha, V.; Di Buono, M.; Jenkins, A.L.; Leiter, L.A.; et al. Effect of fructose on markers of non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of controlled feeding trials. Eur. J. Clin. Nutr. 2014, 68, 416–423. [Google Scholar] [CrossRef]
- Green, C.J.; Hodson, L. The Influence of Dietary Fat on Liver Fat Accumulation. Nutrients 2014, 6, 5018–5033. [Google Scholar] [CrossRef] [PubMed]
- Hydes, T.; Alam, U.; Cuthbertson, D.J. The Impact of Macronutrient Intake on Non-alcoholic Fatty Liver Disease (NAFLD): Too Much Fat, Too Much Carbohydrate, or Just Too Many Calories? Front. Nutr. 2021, 8. [Google Scholar] [CrossRef]
- Johnston, R.D.; Stephenson, M.C.; Crossland, H.; Cordon, S.M.; Palcidi, E.; Cox, E.F.; Taylor, M.A.; Aithal, G.P.; Macdonald, I.A. No Difference Between High-Fructose and High-Glucose Diets on Liver Triacylglycerol or Biochemistry in Healthy Overweight Men. Gastroenterology 2013, 145, 1016–1025.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nobili, V.; Liccardo, D.; Bedogni, G.; Salvatori, G.; Gnani, D.; Bersani, I.; Alisi, A.; Valenti, L.; Raponi, M. Influence of dietary pattern, physical activity, and I148M PNPLA3 on steatosis severity in at-risk adolescents. Genes Nutr. 2014, 9, 392. [Google Scholar] [CrossRef] [Green Version]
- Ford, E.S.; Dietz, W.H. Trends in energy intake among adults in the United States: Findings from NHANES. Am. J. Clin. Nutr. 2013, 97, 848–853. [Google Scholar] [CrossRef] [Green Version]
- Bothwell, E.K.G.; Ayala, G.X.; Conway, T.L.; Rock, C.L.; Gallo, L.C.; Elder, J.P. Underreporting of Food Intake among Mexican/Mexican-American Women: Rates and Correlates. J. Am. Diet. Assoc. 2009, 109, 624–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olendzki, B.C.; Ma, Y.; Hébert, J.R.; Pagoto, S.L.; Merriam, P.A.; Rosal, M.C.; Ockene, I.S. Underreporting of energy intake and associated factors in a Latino population at risk of developing type 2 diabetes. J. Am. Diet Assoc. 2008, 108, 1003–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, L. Gene-Diet Interactions in Complex Disease: Current Findings and Relevance for Public Health. Curr. Nutr. Rep. 2012, 1, 222–227. [Google Scholar] [CrossRef] [Green Version]
- Tinker, L.F.; Sarto, G.E.; Howard, B.V.; Huang, Y.; Neuhouser, M.L.; Mossavar-Rahmani, Y.; Beasley, J.M.; Margolis, K.; Eaton, C.B.; Phillips, L.S.; et al. Biomarker-calibrated dietary energy and protein intake associations with diabetes risk among postmenopausal women from the Women’s Health Initiative. Am. J. Clin. Nutr. 2011, 94, 1600–1606. [Google Scholar] [CrossRef] [PubMed]
- Davy, B.; Jahren, H. New markers of dietary added sugar intake. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 282–288. [Google Scholar] [CrossRef] [Green Version]
- Heianza, Y.; Qi, L. Gene-Diet Interaction and Precision Nutrition in Obesity. Int. J. Mol. Sci. 2017, 18, 787. [Google Scholar] [CrossRef] [Green Version]
- Meroni, M.; Longo, M.; Rustichelli, A.; Dongiovanni, P. Nutrition and Genetics in NAFLD: The Perfect Binomium. Int. J. Mol. Sci. 2020, 21, 2986. [Google Scholar] [CrossRef] [Green Version]
- Passel, J.S.; D’Vera, C.U.S. Population Projections: 2005–2050; Pew Research Center: Washington, DC, USA, 2008. [Google Scholar]
| Variable | CC (n = 72) | CG (n = 139) | GG (n = 77) | p-Value 2 |
|---|---|---|---|---|
| Sex, n (%) | 0.56 | |||
| Male | 23 (31.9) | 54 (38.8) | 26 (33.8) | |
| Female | 49 (68.1) | 85 (61.2) | 51 (66.2) | |
| Age (y), mean ± SD | 44.9 ± 12.1 | 44.2 ± 10.8 | 45.5 ± 10.8 | 0.69 |
| Weight (kg), median (IQR) | 86.6 (74.1, 99.5) | 84.6 (77.6, 93.5) | 87.5 (76.0, 100.2) | 0.50 |
| BMI (kg/m2), median (IQR) | 31.3 (28.0, 35.8) | 31.1 (28.9, 34.2) | 32.6 (29.3, 36.3) | 0.27 |
| Waist Circumference (cm), median (IQR) | 103.3 (97.0, 116.1) | 103.0 (96.4, 111.1) | 106.8 (99.2, 113.9) | 0.18 |
| Liver Steatosis (dB/m) 3, mean ± SD | 285.5 ± 53.4 | 283.7 ± 44.5 a | 302.4 ± 50.8 b | 0.02 |
| Liver Fibrosis (kPa) 4, median (IQR) | 5.1 (4.1, 5.9) | 5.0 (4.4, 6.2) | 5.0 (4.5, 6.6) | 0.50 |
| Income Level, n (%) | 0.18 | |||
| <$29 K | 35 (48.6) | 61 (43.9) | 47 (61.0) | |
| $30–59 K | 24 (33.3) | 55 (39.6) | 21 (27.3) | |
| >$60 K | 13 (18.1) | 23 (16.5) | 9 (11.7) | |
| Diabetes (yes), n | 6 (8.3) | 14 (10.1) | 8 (10.4) | 0.90 |
| Insurance (yes), n | 41 (56.9) | 92 (66.2) | 45 (58.4) | 0.33 |
| Current Use of Lipid-Lowering Medication (yes), n | 5 (6.9) | 9 (6.5) | 6 (7.8) | 0.93 |
| Variable | CC (n = 72) | CG (n = 139) | GG (n = 77) | p-Value 2 |
|---|---|---|---|---|
| Energy (kcals) | 1459 (1160,1682) | 1426 (1166, 1822) | 1430 (1079, 1730) | 0.42 |
| Protein (g/d) | 66.4 (53.5, 78.0) | 63.4 (49.4, 79.2) | 61.9 (47.8, 73.7) | 0.45 |
| Protein (% of energy) | 18.8 (14.9, 23.7) | 17.4 (15.1, 20.8) | 17.9 (14.6, 20.6) | 0.24 |
| Fat (g/d) | 55.8 (40.4, 73.0) | 56.3 (40.0, 74.0) | 54.5 (39.4, 65.7) | 0.57 |
| Fat (% of energy) | 33.8 (30.5, 37.8) | 33.4 (30.0, 39.4) | 36.6 (30.8, 39.0) | 0.72 |
| n-3 PUFA (g/d) | 1.3 (0.9, 1.9) | 1.3 (0.8, 2.0) | 1.2 (0.8, 1.7) | 0.514 |
| n-3 PUFA (% of energy) | 0.8 (0.6, 1.1) | 0.8 (0.6, 1.1) | 0.8 (0.6, 1.0) | 0.55 |
| n-6 PUFA (g/d) | 11.2 (7.6, 15.9) | 10.9 (7.9, 15.3) | 10.8 (6.4, 14.0) | 0.34 |
| n-6 PUFA (% of energy) | 6.7 (5.6, 8.5) | 6.8 (5.8, 8.5) | 6.6 (5.2, 7.6) | 0.36 |
| n-6/n-3 PUFA | 8.3 (7.0, 9.2) | 8.4 (7.5, 9.9) | 8.3 (7.3, 10.0) | 0.71 |
| Carbohydrates (g/d) | 175.4 (132.4, 208.3) | 166.9 (131.9, 218.3) | 169.0 (120.3, 211.1) | 0.44 |
| Carbohydrates (% of energy) | 46.1 (42.0, 51.2) | 46.7 (41.8, 51.3) | 45.1 (39.4, 51.3) | 0.65 |
| Fructose (g/d) | 13.6 (7.9, 21.2) | 13.3 (7.8, 20.5) | 13.3 (6.6, 20.9) | 0.74 |
| Fructose (% of energy) | 3.8 (2.6, 5.6) | 3.5 (2.5, 5.5) | 3.7 (2.0, 5.8) | 0.78 |
| Total sugar (g/d) | 59.4 (46.4, 85.3) | 64.6 (45.7, 87.7) | 61.7 (45.4, 84.6) | 0.75 |
| Total sugar (% of energy) | 17.6 (13.2, 22.9) | 17.6 (14.1, 23.1) | 18.1 (13.8, 24.3) | 0.84 |
| Added sugar (g/d) | 35.5 (19.7, 52.9) | 39.2 (23.3, 57.8) | 35.5 (22.3, 57.7) | 0.73 |
| Added sugar (% of energy) | 9.3 (5.9, 13.5) | 10.6 (7.0, 15.5) | 10.3 (6.4, 16.1) | 0.45 |
| Dietary fiber (g/d) | 16.8 (11.8, 22.2) | 14.9 (11.0, 21.1) | 13.7 (11.0, 18.6) | 0.06 |
| Insoluble fiber (g/d) | 10.2 (8.1, 14.5) | 9.6 (7.0, 13.6) | 8.8 (6.9, 12.0) | 0.12 |
| Soluble fiber (g/d) | 5.7 (4.5, 8.0) | 5.1 (3.9, 7.5) a | 4.8 (3.5, 6.1) b | 0.02 |
| Glycemic index | 56.4 ± 4.9 | 56.7 ± 4.6 | 57.6 ± 5.1 | 0.30 |
| Glycemic load | 90.1 (66.3, 104.0) | 87.2 (65.8, 110.7) | 89.2 (62.3, 108.6) | 0.62 |
| Coefficient | SE | p-Value | |
|---|---|---|---|
| Energy (per 100 kcals) | −0.246 | 0.511 | 0.63 |
| Protein (% of energy) | −0.136 | 0.475 | 0.78 |
| Fat (% of energy) | 0.629 | 0.391 | 0.11 |
| n-3 PUFA (% of energy) | 1.072 | 2.612 | 0.68 |
| n-6 PUFA (% of energy) | −0.090 | 0.410 | 0.83 |
| n-6/n-3 PUFA | −0.276 | 0.985 | 0.78 |
| Carbohydrates (% of energy) | −0.391 | 0.310 | 0.21 |
| Fructose (% of energy) | 0.274 | 1.012 | 0.79 |
| Total sugar (% of energy) | −0.220 | 0.369 | 0.55 |
| Added sugar (% of energy) | −0.182 | 0.403 | 0.65 |
| Dietary fiber (g/d) | 0.197 | 0.362 | 0.59 |
| Insoluble fiber (g/d) | 0.524 | 0.523 | 0.32 |
| Soluble fiber (g/d) | −0.475 | 0.980 | 0.63 |
| Glycemic index | −0.678 | 0.546 | 0.22 |
| Glycemic load | −0.082 | 0.068 | 0.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morrill, K.E.; Bland, V.L.; Klimentidis, Y.C.; Hingle, M.D.; Thomson, C.A.; Garcia, D.O. Assessing Interactions between PNPLA3 and Dietary Intake on Liver Steatosis in Mexican-Origin Adults. Int. J. Environ. Res. Public Health 2021, 18, 7055. https://doi.org/10.3390/ijerph18137055
Morrill KE, Bland VL, Klimentidis YC, Hingle MD, Thomson CA, Garcia DO. Assessing Interactions between PNPLA3 and Dietary Intake on Liver Steatosis in Mexican-Origin Adults. International Journal of Environmental Research and Public Health. 2021; 18(13):7055. https://doi.org/10.3390/ijerph18137055
Chicago/Turabian StyleMorrill, Kristin E., Victoria L. Bland, Yann C. Klimentidis, Melanie D. Hingle, Cynthia A. Thomson, and David O. Garcia. 2021. "Assessing Interactions between PNPLA3 and Dietary Intake on Liver Steatosis in Mexican-Origin Adults" International Journal of Environmental Research and Public Health 18, no. 13: 7055. https://doi.org/10.3390/ijerph18137055
APA StyleMorrill, K. E., Bland, V. L., Klimentidis, Y. C., Hingle, M. D., Thomson, C. A., & Garcia, D. O. (2021). Assessing Interactions between PNPLA3 and Dietary Intake on Liver Steatosis in Mexican-Origin Adults. International Journal of Environmental Research and Public Health, 18(13), 7055. https://doi.org/10.3390/ijerph18137055