
Hospital Employees’ Well-Being Six Months after the COVID-19 Outbreak: Results from a Psychological Screening Program in Italy

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. The Well-Being Project
2.2. Participants
2.3. Measures
2.3.1. Anxiety
2.3.2. Depression
2.3.3. Post-Traumatic Stress Disorder
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Paticipants
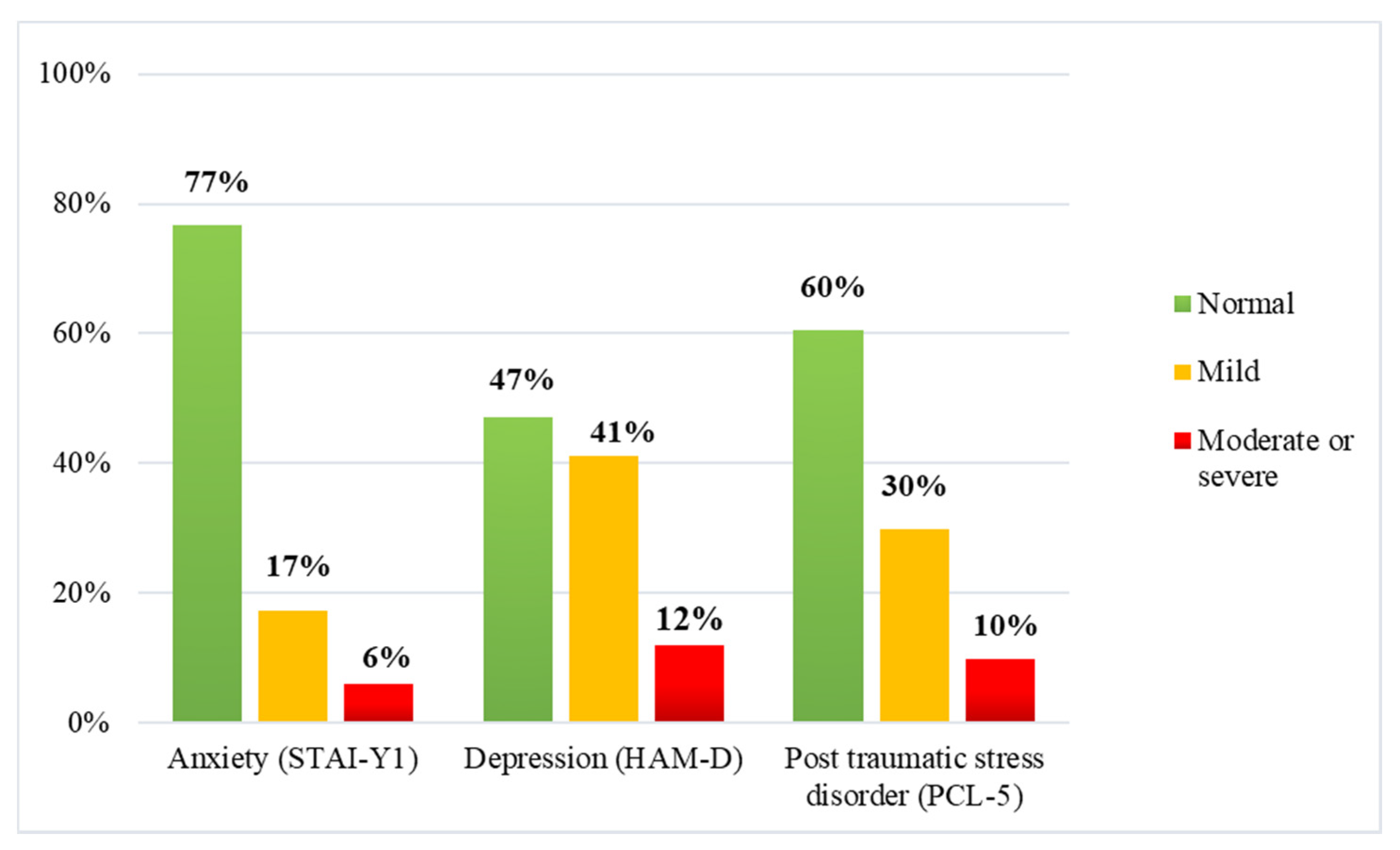
3.2. Anxiety, Depression, and Post-Traumatic Stress Disorder
3.3. Clinical Support
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sorbello, M.; El-Boghdadly, K.; Di Giacinto, I.; Cataldo, R.; Esposito, C.; Falcetta, S.; Merli, G.; Cortese, G.; Corso, R.M.; Bressan, F.; et al. The Italian coronavirus disease 2019 outbreak: Recommendations from clinical practice. Anaesthesia 2020, 75, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain. Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J. Diabetes Metab. Disord. 2020, 19, 1967–1978. [Google Scholar] [CrossRef]
- Spoorthy, M.S.; Pratapa, S.K.; Mahant, S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic–A review. Asian J. Psychiatr. 2020, 51, 102119. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. 2020, 288, 112936. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wang, W.; Sun, Y.; Qian, W.; Liu, Z.; Wang, R.; Qi, L.; Yang, J.; Song, X.; Zhou, X.; et al. The prevalence and risk factors of psychological disturbances of frontline medical staff in china under the COVID-19 epidemic: Workload should be concerned. J. Affect. Disord. 2020, 277, 510–514. [Google Scholar] [CrossRef]
- Liu, C.-Y.; Yang, Y.; Zhang, X.-M.; Xu, X.; Dou, Q.-L.; Zhang, W.-W. The prevalence and influencing factors for anxiety in medical workers fighting COVID-19 in China: A cross-sectional survey. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Di Tella, M.; Romeo, A.; Benfante, A.; Castelli, L. Mental health of healthcare workers during the COVID-19 pandemic in Italy. J. Eval. Clin. Pract. 2020, 26, 1583–1587. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental health outcomes among frontline and second-line health care workers during the Coronavirus disease 2019 (COVID-19) pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef]
- Liang, Y.; Chen, M.; Zheng, X.; Liu, J. Screening for Chinese medical staff mental health by SDS and SAS during the outbreak of COVID-19. J. Psychosom. Res. 2020, 133, 110102. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Xu, Q.; Wang, C.; Wang, J. Psychological status of surgical staff during the COVID-19 outbreak. Psychiatry Res. 2020, 288, 112955. [Google Scholar] [CrossRef] [PubMed]
- Lasalvia, A.; Bonetto, C.; Porru, S.; Carta, A.; Tardivo, S.; Bovo, C.; Ruggeri, M.; Amaddeo, F. The psychological impact of the COVID-19 pandemic on health care workers in a highly burdened area of north-east Italy. Epidemiol. Psychiatr. Sci. 2020. [Google Scholar] [CrossRef]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 779–788. [Google Scholar] [CrossRef]
- De Kock, J.H.; Latham, H.A.; Leslie, S.J.; Grindle, M.; Munoz, S.A.; Ellis, L.; Polson, R.; O’Malley, C.M. A rapid review of the impact of COVID-19 on the mental health of healthcare workers: Implications for supporting psychological well-being. BMC Public Health 2021, 21, 1–18. [Google Scholar] [CrossRef]
- Santabárbara, J.; Bueno-Notivol, J.; Lipnicki, D.M.; Olaya, B.; Pérez-Moreno, M.; Gracia-García, P.; Idoiaga-Mondragon, N.; Ozamiz-Etxebarria, N. Prevalence of anxiety in health care professionals during the COVID-19 pandemic: A rapid systematic review (on published articles in Medline) with meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 107, 110244. [Google Scholar] [CrossRef]
- Tan, B.Y.Q.; Chew, N.W.S.; Lee, G.K.H.; Jing, M.; Goh, Y.; Yeo, L.L.L.; Zhang, K.; Chin, H.-K.; Ahmad, A.; Khan, F.A.; et al. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann. Intern. Med. 2020, 173, 317–320. [Google Scholar] [CrossRef]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L.; et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain. Behav. Immun. 2020, 88, 916–919. [Google Scholar] [CrossRef]
- Eftekhar Ardebili, M.; Naserbakht, M.; Bernstein, C.; Alazmani-Noodeh, F.; Hakimi, H.; Ranjbar, H. Healthcare providers experience of working during the COVID-19 pandemic: A qualitative study. Am. J. Infect. Control 2020, 49, 547–554. [Google Scholar] [CrossRef]
- Szmyd, B.; Karuga, F.F.; Bartoszek, A.; Staniecka, K.; Siwecka, N.; Bartoszek, A.; Błaszczyk, M.; Radek, M. Attitude and behaviors towards SARS-CoV-2 vaccination among healthcare workers: A cross-sectional study from Poland. Vaccines 2021, 9, 218. [Google Scholar] [CrossRef]
- Smereka, J.; Szarpak, L. The use of personal protective equipment in the COVID-19 pandemic era. Am. J. Emerg. Med. 2020, 38, 1529–1530. [Google Scholar] [CrossRef] [PubMed]
- DiBenigno, J.; Kerrissey, M. Structuring mental health support for frontline caregivers during COVID-19: Lessons from organisational scholarship on unit-aligned support. BMJ Lead. 2020, 4, 124–127. [Google Scholar] [CrossRef]
- Weibelzahl, S.; Reiter, J.; Duden, G. Depression and anxiety in healthcare professionals during the COVID-19 Pandemic. Epidemiol. Infect. 2021, 149, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef] [PubMed]
- Rosenstein, A.H. Hospital administration response to physician stress and burnout. Hosp. Pract. 2019, 47, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Muller, A.E.; Hafstad, E.V.; Himmels, J.P.W.; Smedslund, G.; Flottorp, S.; Stensland, S.Ø.; Stroobants, S.; Van de Velde, S.; Vist, G.E. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory STAI (Form Y); Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Pedrabissi, L.; Santiniello, M. Manuale Dell’adattamento Italiano Dello STAI Forma Y.; Organizzazioni Speciali: Firenze, Italy, 1989. [Google Scholar]
- Barisone, M.G.; Lerda, S.; Ansaldi, S.; De Vincenzo, E.; Angelini, G. Psychopathology and epilepsy: Clinical experience in a Centre for the Diagnosis and Care of epilepsy. J. Psychopatol. 2004, 10, 336–346. [Google Scholar]
- Hamilton, M. A Rating Scale for Depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Pancheri, P.; Picardi, A.; Pasquini, M.; Gaetano, P.; Biondi, M. Psychopathological dimensions of depression: A factor study of the 17-item Hamilton depression rating scale in unipolar depressed outpatients. J. Affect. Disord. 2002, 68, 41–47. [Google Scholar] [CrossRef]
- Zimmerman, M.; Martinez, J.H.; Young, D.; Chelminski, I.; Dalrymple, K. Severity classification on the Hamilton depression rating scale. J. Affect. Disord. 2013, 150, 384–388. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM 5); American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P. The PTSD Checklist for DSM-5 (PCL-5). 2013. Available online: https://www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp#obtain (accessed on 20 June 2020).
- Bovin, M.J.; Marx, B.P.; Weathers, F.W.; Gallagher, M.W.; Rodriguez, P.; Schnurr, P.P.; Keane, T.M. Psychometric properties of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (PCL-5) in veterans. Psychol. Assess. 2016, 28, 1379–1391. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows, Version 26.0. 2019; IBM Corp: Armonk, NY, USA, 2019. [Google Scholar]
- Lissoni, B.; Del Negro, S.; Brioschi, P.; Casella, G.; Fontana, I.; Bruni, C.; Lamiani, G. Promoting resilience in the acute phase of the COVID-19 pandemic: Psychological interventions for intensive care unit (ICU) clinicians and family members. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S105–S107. [Google Scholar] [CrossRef] [PubMed]
- Buselli, R.; Baldanzi, S.; Corsi, M.; Chiumiento, M.; Del Lupo, E.; Carmassi, C.; Dell’Osso, L.; Cristaudo, A. Psychological care of health workers during the COVID-19 Outbreak in Italy: Preliminary report of an Occupational Health Department (AOUP) responsible for monitoring hospital staff condition. Sustainability 2020, 12, 5039. [Google Scholar] [CrossRef]
- Tomlin, J.; Dalgleish-Warburton, B.; Lamph, G. Psychosocial support for healthcare workers during the COVID-19 pandemic. Front. Psychol. 2020, 11, 1–7. [Google Scholar] [CrossRef]
- Giusti, E.M.; Pedroli, E.; D’Aniello, G.E.; Stramba Badiale, C.; Pietrabissa, G.; Manna, C.; Stramba Badiale, M.; Riva, G.; Castelnuovo, G.; Molinari, E. The Psychological Impact of the COVID-19 Outbreak on Health Professionals: A Cross-Sectional Study. Front. Psychol. 2020, 11, 1–9. [Google Scholar] [CrossRef]
- DeWolfe, D.J. Training Manual for Mental Health and Human Service Workers in Major Disasters, 2nd ed.; Nordboe, D., Ed.; US Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services: Washington, DC, USA, 2000.
- Green, B.L.; Wilson, J.P.; Lindy, J.D. Conceptualizing Post-traumatic stress disorder: A Psychosocial Framework. In Trauma and its Wake, Volume I: The Study and Treatment of Post-Traumatic Stress Disorder; Figle, C., Ed.; Brunner/Mazel: New York, NY, USA, 1985; pp. 53–69. [Google Scholar]
- Myers, D.; Zunin, H.S.; Zunin, L. Grief: The art of coping with tragedy. Today’s Superv. 1990, 6, 14–15. [Google Scholar]
- Menichetti Delor, J.P.; Borghi, L.; Cao di San Marco, E.; Fossati, I.; Vegni, E. Phone follow up to families of COVID-19 patients who died at the hospital: Families’ grief reactions and clinical psychologists’ roles. Int. J. Psychol. 2021, ijop.12742. [Google Scholar] [CrossRef]
- Gesi, C.; Carmassi, C.; Cerveri, G.; Carpita, B.; Cremone, I.M.; Dell’Osso, L. Complicated grief: What to expect after the Coronavirus pandemic. Front. Psychiatry 2020, 11, 489. [Google Scholar] [CrossRef]
- Eaton, N.R.; Keyes, K.M.; Krueger, R.F.; Balsis, S.; Skodol, A.E.; Markon, K.E.; Grant, B.F.; Hasin, D.S. An invariant dimensional liability model of gender differences in mental disorder prevalence: Evidence from a national sample. J. Abnorm. Psychol. 2012, 121, 282–288. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S. Emotion regulation and psychopathology: The role of gender. Annu. Rev. Clin. Psychol. 2012, 8, 161–187. [Google Scholar] [CrossRef] [PubMed]
- Szmyd, B.; Bartoszek, A.; Karuga, F.F.; Staniecka, K.; Błaszczyk, M.; Radek, M. Medical Students and SARS-CoV-2 Vaccination: Attitude and Behaviors. Vaccines 2021, 9, 128. [Google Scholar] [CrossRef] [PubMed]
- Haller, M.; Norman, S.B.; Davis, B.C.; Capone, C.; Browne, K.; Allard, C.B. A model for treating COVID-19-related guilt, shame, and moral injury. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 174–176. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.; Ripp, J.; Trockel, M. Understanding and addressing sources of anxiety among health care professionals during the COVID-19 pandemic. JAMA 2020, 323, 2133. [Google Scholar] [CrossRef]
- Cox, C.L. ‘Healthcare Heroes’: Problems with media focus on heroism from healthcare workers during the COVID-19 pandemic. J. Med. Ethics 2020, 46, 510–513. [Google Scholar] [CrossRef]


{kind=link}
| Title of Mindful Practice | Description Offered to Employees | Duration of Practice (Minutes) |
|---|---|---|
| Practice of letting go. | This practice is useful to lighten your mind. The practice of letting go is useful for overcoming the crowding of involuntary thoughts and feelings that weigh on the mind, especially when you are exposed to stressful conditions or painful experiences. | 9.11 |
| Practice of the tree. | This practice of guided imagery is inspired by the stability, strength, and openness of the tree, which is rooted in the earth. This practice favors the engagement with the present moment and therefore helps to overcome the rumination that is oriented towards the past or the future. | 7.22 |
| Practice of kindness towards yourself. | This practice helps to manage the emotional discomfort resulting from specific painful events or stressors. This practice favors balance and acceptance of one’s own experience. | 13.16 |
| Mindfulness practice for healthcare professionals. | This practice is useful to relieve tension and physical fatigue of those who work in the healthcare field. By focusing on the breath, this practice favors self-care and the connection with the present moment and with oneself. | 13.32 |
| Variables | N (%) |
|---|---|
| Sex | |
| Male | 62 (20) |
| Female | 246 (80) |
| Age (years) | |
| Mean (SD) | 45.06 (11.34) |
| Median (range) | 47 (22–67) |
| Profession | |
| Administrative | 48 (16) |
| Physician | 48 (16) |
| Nurses | 111 (36) |
| Allied healthcare professional | 18 (6) |
| Psychologist | 43 (14) |
| Physiotherapist | 10 (3) |
| Health and safety officer | 5 (2) |
| Biologist/Lab Technician | 12 (3) |
| Other | 13 (4) |
| Contact with COVID-19 patients | |
| Yes | 160 (52) |
| No | 148 (48) |
| Had COVID-19 | |
| Yes | 28 (9) |
| No | 280 (91) |
| Family members with COVID-19 | |
| Yes | 37 (12) |
| No | 271 (88) |
| Losses for COVID-19 in the personal context | |
| Yes | 47 (15) |
| No | 261 (85) |
| Losses for COVID-19 at work | |
| Yes | 124 (40) |
| No | 184 (60) |
| STAI-Y1 | HAM-D | PCL-5 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | |||||||
| Variable | OR | (95% C.I.) | OR | (95% C.I.) | OR | (95% C.I.) | OR | (95% C.I.) | OR | (95% C.I.) | OR | (95% C.I.) |
| Sex (F vs. M) | 1.05 | (0.54–2.03) | 1.14 | (0.56–2.23) | 2.75 ** | (1.44–5.25) | 2.82 * | (1.43–5.59) | 1.17 | (0.62–2.21) | 1.17 | (0.59–2.34) |
| Age (Years) | 1.02 | (0.99–1.04) | 1.01 | (0.98–1.04) | 1.01 | (0.99–1.03) | 1.02 | (0.99–1.04) | 1.01 | (0.99–1.04) | 1.01 | (0.99–1.04) |
| Profession | ||||||||||||
| Administrative 1 | 1 | - | 1 | - | 1 | - | 1 | - | 1 | - | 1 | - |
| Physician | 0.92 | (0.43–2.00) | 0.82 | (0.35–1.91) | 0.96 | (0.48–1.91) | 0.94 | (0.43–2.03) | 0.66 | (0.31–1.39) | 0.87 | (0.37–2.02) |
| Other healthcare prof | 1.45 | (0.71–2.95) | 1.41 | (0.65–3.08) | 0.75 | (0.37–1.52) | 0.62 | (0.28–1.36) | 0.83 | (0.40–1.76) | 0.58 | (0.25–1.32) |
| Contact with COVID-19 patients (Yes vs. No) | 1.08 | (0.64–1.85) | 0.99 | (0.51–1.93) | 0.95 | (0.58–1.56) | 1.03 | (0.51–1.96) | 1.71 * | (1.01–2.90) | 1.44 | (0.72–2.86) |
| Had COVID-19 (Yes vs. No) | 0.70 | (0.25–1.91) | 0.59 | (1.95–1.79) | 0.88 | (0.37–2,11) | 0.80 | (0.29–2.24) | 2.73 * | (1.08–6.86) | 1.63 | (0.56–4.76) |
| Family member with COVID-19 (Yes vs. No) | 1.54 | (0.72–3.31) | 1.24 | (0.50–3.05) | 1.47 | (0.68–3.18) | 1.46 | (0.56–3.80) | 2.86 * | (1.28–6.38) | 2.75 * | (1.01–7.48) |
| Losses for COVID-19 in the personal context (Yes vs. No) | 2.70 ** | (1.40–5.21) | 2.40 * | (1.16–4.98) | 1.18 | (0.59–2.34) | 1.04 | (0.47–2.31) | 0.89 | (0.42–1.86) | 0.59 | (0.24–1.44) |
| Losses for COVID-19 at work (Yes vs. No) | 1.10 | (0.64–1.88) | 1.04 | (0.57–1.91) | 1.38 | (0.84–2.29) | 1.60 | (0.90–2.85) | 1.96 * | (1.15–3.33) | 1.76 | (0.97–3.19) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamiani, G.; Borghi, L.; Poli, S.; Razzini, K.; Colosio, C.; Vegni, E. Hospital Employees’ Well-Being Six Months after the COVID-19 Outbreak: Results from a Psychological Screening Program in Italy. Int. J. Environ. Res. Public Health 2021, 18, 5649. https://doi.org/10.3390/ijerph18115649
Lamiani G, Borghi L, Poli S, Razzini K, Colosio C, Vegni E. Hospital Employees’ Well-Being Six Months after the COVID-19 Outbreak: Results from a Psychological Screening Program in Italy. International Journal of Environmental Research and Public Health. 2021; 18(11):5649. https://doi.org/10.3390/ijerph18115649
Chicago/Turabian StyleLamiani, Giulia, Lidia Borghi, Silvia Poli, Katia Razzini, Claudio Colosio, and Elena Vegni. 2021. "Hospital Employees’ Well-Being Six Months after the COVID-19 Outbreak: Results from a Psychological Screening Program in Italy" International Journal of Environmental Research and Public Health 18, no. 11: 5649. https://doi.org/10.3390/ijerph18115649
APA StyleLamiani, G., Borghi, L., Poli, S., Razzini, K., Colosio, C., & Vegni, E. (2021). Hospital Employees’ Well-Being Six Months after the COVID-19 Outbreak: Results from a Psychological Screening Program in Italy. International Journal of Environmental Research and Public Health, 18(11), 5649. https://doi.org/10.3390/ijerph18115649