
Drastic Cardiac Reverse Remodeling Following Catheter Ablation in Patients with Atrial Fibrillation and Heart Failure



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Care Report
2.1. Before Admission
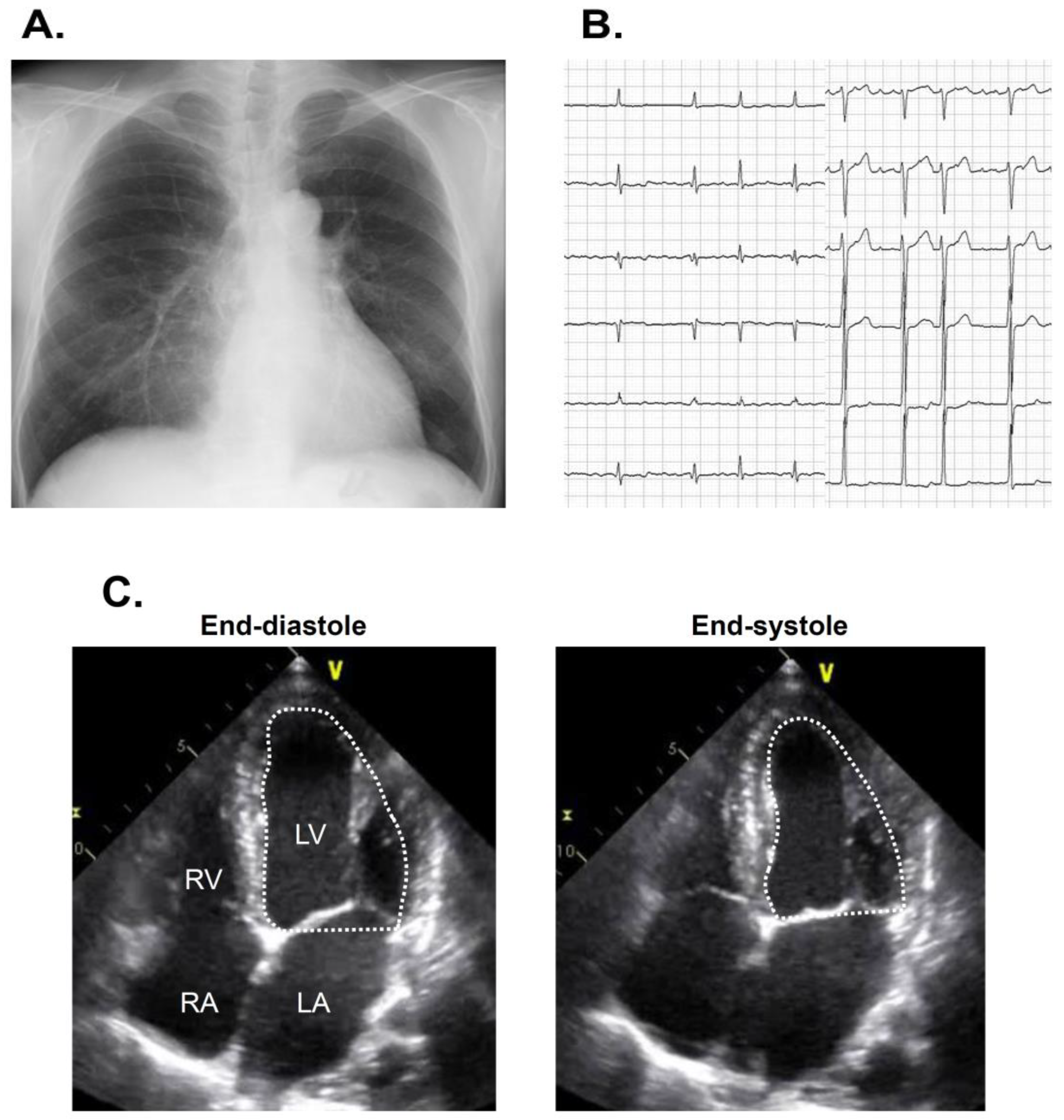
2.2. On Admission
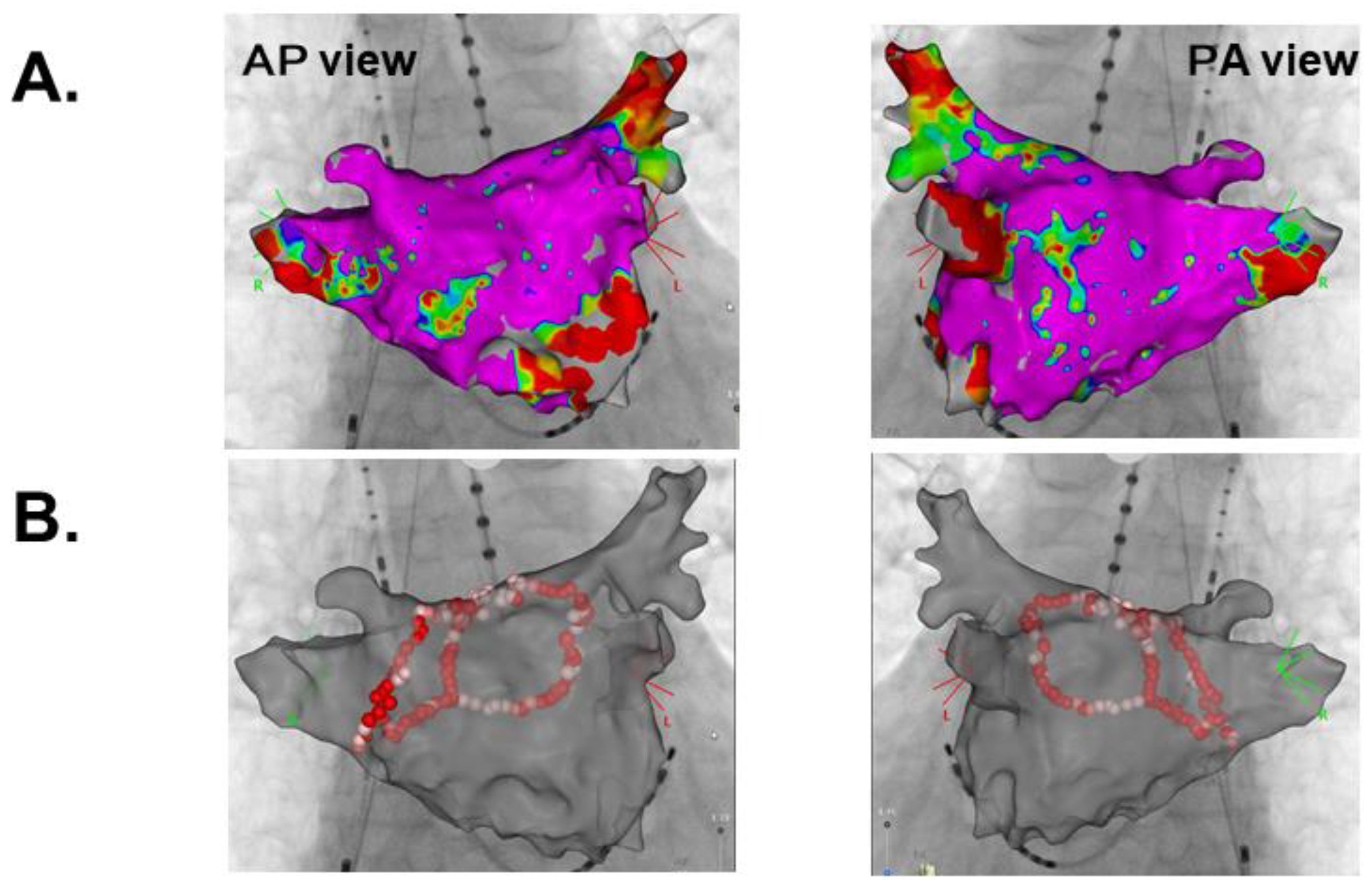
2.3. In-Hospital Course
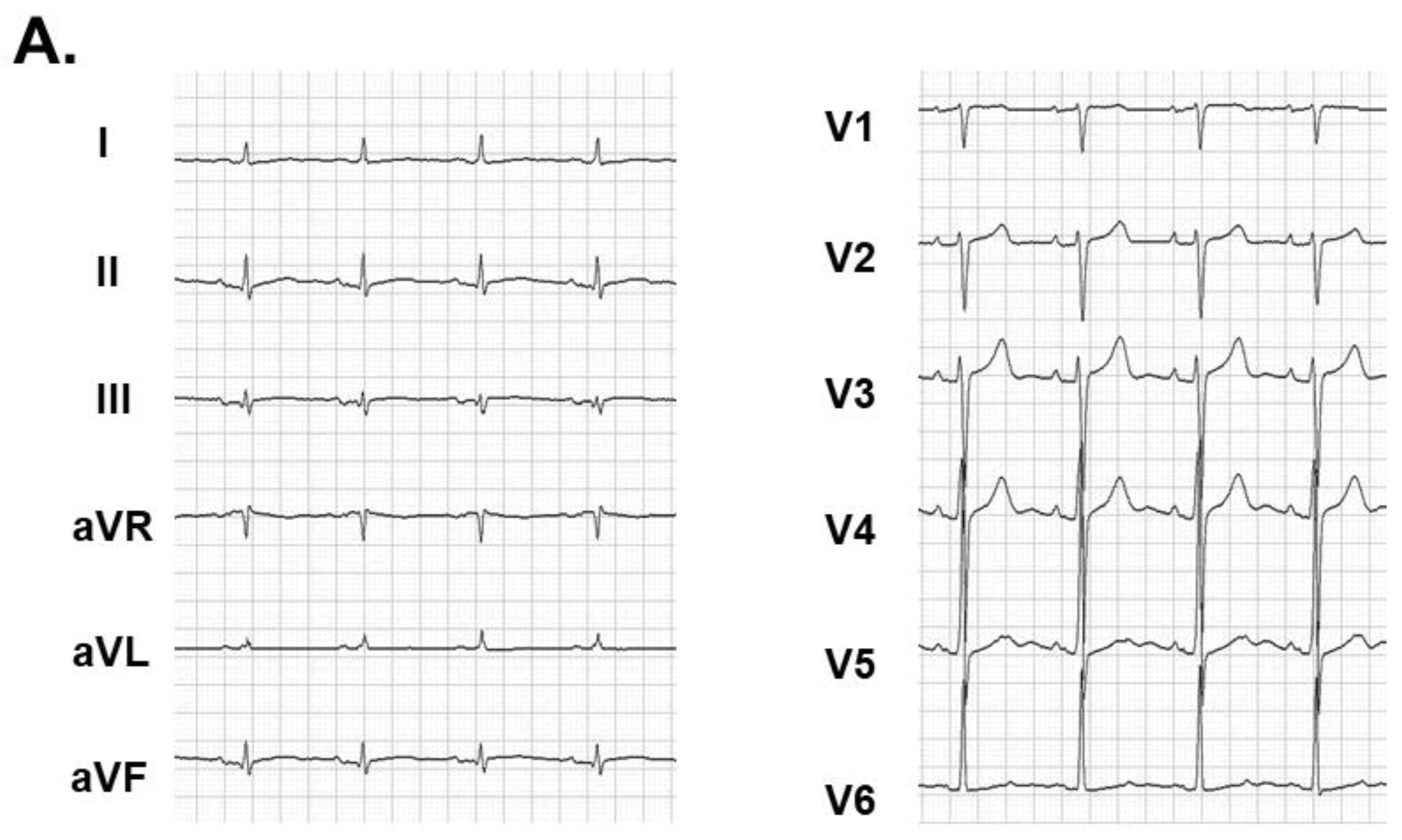
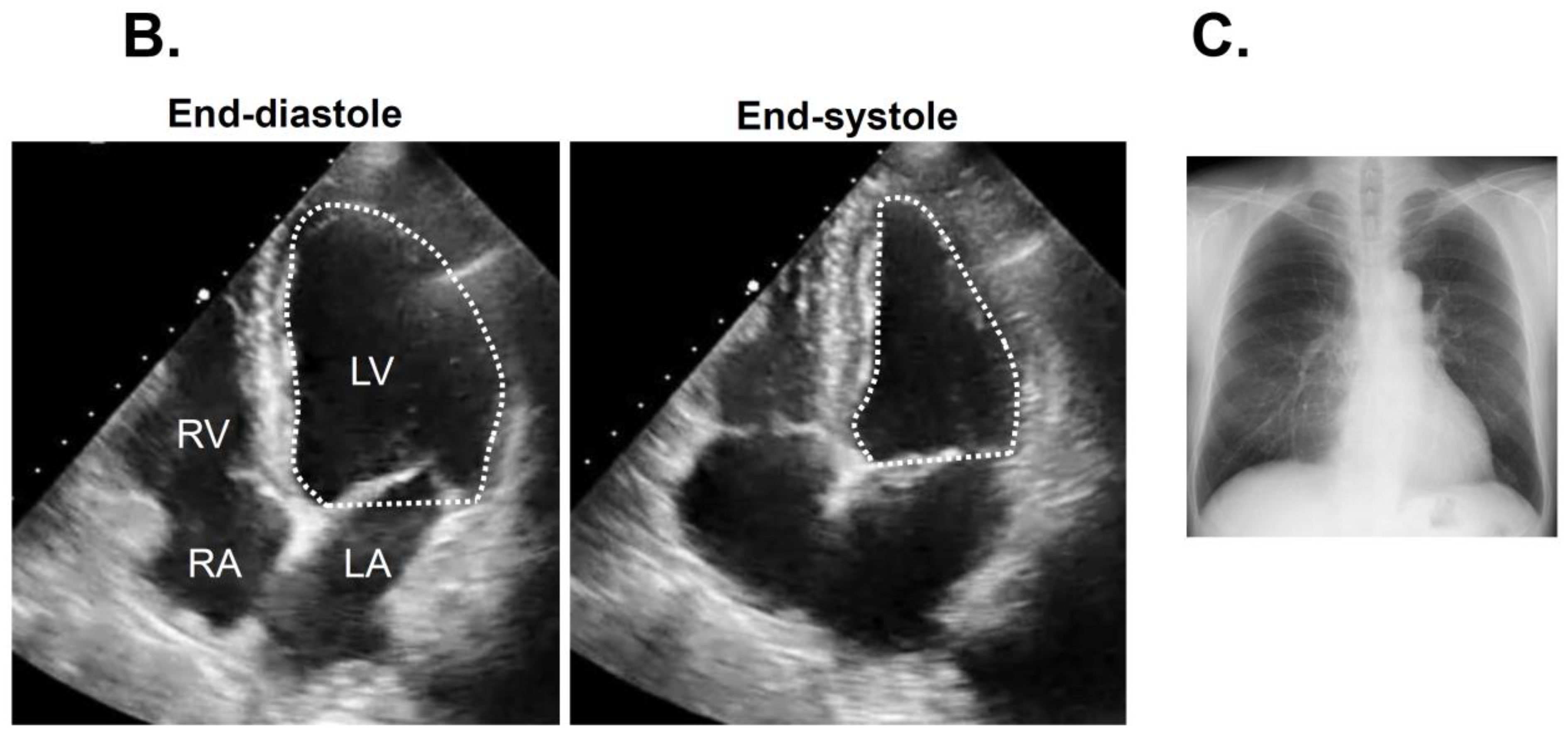
2.4. Three-Month Follow-Up
3. Discussion
3.1. Atrial Fibrillation and Heart Failure
3.2. Indication of Rhythm Control
3.3. Implication of Rhythm Control on Cardiac Reverse Remodeling
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclosure
References
- Cha, Y.M.; Redfield, M.M.; Shen, W.K.; Gersh, B.J. Atrial fibrillation and ventricular dysfunction: A vicious electromechanical cycle. Circulation 2004, 109, 2839–2843. [Google Scholar] [CrossRef] [PubMed]
- Carson, P.E.; Johnson, G.R.; Dunkman, W.B.; Fletcher, R.D.; Farrell, L.; Cohn, J.N. The influence of atrial fibrillation on prognosis in mild to moderate heart failure. The V-HeFT Studies. The V-HeFT VA Cooperative Studies Group. Circulation 1993, 87, 102–110. [Google Scholar]
- Pozzoli, M.; Cioffi, G.; Traversi, E.; Pinna, G.D.; Cobelli, F.; Tavazzi, L. Predictors of primary atrial fibrillation and concomitant clinical and hemodynamic changes in patients with chronic heart failure: A prospective study in 344 patients with baseline sinus rhythm. J. Am. Coll. Cardiol. 1998, 32, 197–204. [Google Scholar] [CrossRef]
- Joglar, J.A.; Acusta, A.P.; Shusterman, N.H.; Ramaswamy, K.; Kowal, R.C.; Barbera, S.J. Effect of carvedilol on survival and hemodynamics in patients with atrial fibrillation and left ventricular dysfunction: Retrospective analysis of the US Carvedilol Heart Failure Trials Program. Am. Heart J. 2001, 142, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Roy, D.; Talajic, M.; Nattel, S.; Wyse, D.G.; Dorian, P.; Lee, K.L.; Bourassa, M.G.; Arnold, J.M.O.; Buxton, A.E.; Camm, A.J.; et al. Rhythm Control versus Rate Control for Atrial Fibrillation and Heart Failure. N. Engl. J. Med. 2008, 358, 2667–2677. [Google Scholar] [CrossRef] [PubMed]
- Anselmino, M.; Matta, M.; D’Ascenzo, F.; Bunch, T.J.; Schilling, R.J.; Hunter, R.J. Catheter ablation of atrial fibrillation in patients with left ventricular systolic dysfunction: A systematic review and meta-analysis. Circ. Arrhythm Electrophysiol. 2014, 7, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- Kirstein, B.; Neudeck, S.; Gaspar, T.; Piorkowski, J.; Wechselberger, S.; Kronborg, M.B.; Zedda, A.; Hankel, A.; El-Armouche, A.; Tomala, J.; et al. Left atrial fibrosis predicts left ventricular ejection fraction response after atrial fibrillation ablation in heart failure patients: The Fibrosis-HF Study. Europace 2020, 22, 1812–1821. [Google Scholar] [CrossRef] [PubMed]
- Sardu, C.; Santamaria, M.; Rizzo, M.R.; Barbieri, M.; Di Marino, M.; Paolisso, G.; Santulli, G.; Marfella, R. Telemonitoring in heart failure patients treated by cardiac resynchronisation therapy with defibrillator (CRT-D): The TELECART Study. Int. J. Clin. Pr. 2016, 70, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Winkle, R.A.; Mead, R.H.; Engel, G.; Kong, M.H.; Fleming, W.; Salcedo, J. Impact of obesity on atrial fibrillation ablation: Patient characteristics, long-term outcomes, and complications. Heart Rhythm. 2017, 14, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Sardu, C.; Santamaria, M.; Funaro, S.; Sacra, C.; Barbieri, M.; Paolisso, P.; Marfella, R.; Paolisso, G.; Rizzo, M.R. Cardiac electrophysiological alterations and clinical response in cardiac resynchronization therapy with a defibrillator treated patients affected by metabolic syndrome. Medicine 2017, 96, e6558. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koi, T.; Kataoka, N.; Imamura, T.; Kinugawa, K. Drastic Cardiac Reverse Remodeling Following Catheter Ablation in Patients with Atrial Fibrillation and Heart Failure. Medicina 2021, 57, 511. https://doi.org/10.3390/medicina57050511
Koi T, Kataoka N, Imamura T, Kinugawa K. Drastic Cardiac Reverse Remodeling Following Catheter Ablation in Patients with Atrial Fibrillation and Heart Failure. Medicina. 2021; 57(5):511. https://doi.org/10.3390/medicina57050511
Chicago/Turabian StyleKoi, Takahisa, Naoya Kataoka, Teruhiko Imamura, and Koichiro Kinugawa. 2021. "Drastic Cardiac Reverse Remodeling Following Catheter Ablation in Patients with Atrial Fibrillation and Heart Failure" Medicina 57, no. 5: 511. https://doi.org/10.3390/medicina57050511
APA StyleKoi, T., Kataoka, N., Imamura, T., & Kinugawa, K. (2021). Drastic Cardiac Reverse Remodeling Following Catheter Ablation in Patients with Atrial Fibrillation and Heart Failure. Medicina, 57(5), 511. https://doi.org/10.3390/medicina57050511