
A Successful Experience of Individualized Vancomycin Dosing in Critically Ill Patients by Using a Loading Dose and Maintenance Dose

 ,
, 
 ,
,  and
and 
Abstract
1. Introduction
2. Results
2.1. Demographics and Baseline Characteristics
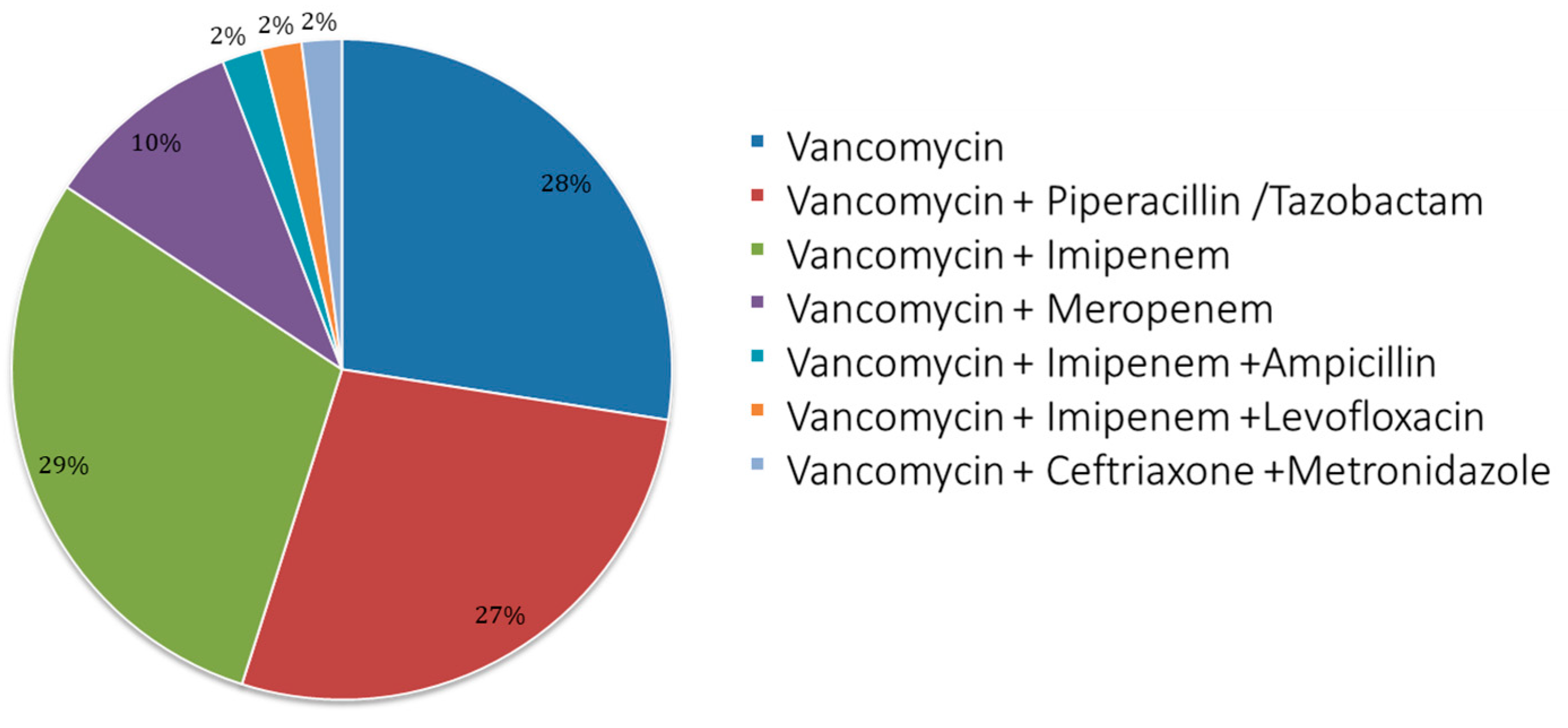
2.2. Vancomycin Treatment Characteristics
2.3. Loading and Maintenance Doses Analyzed by the Antibiotic Kinetics® Software
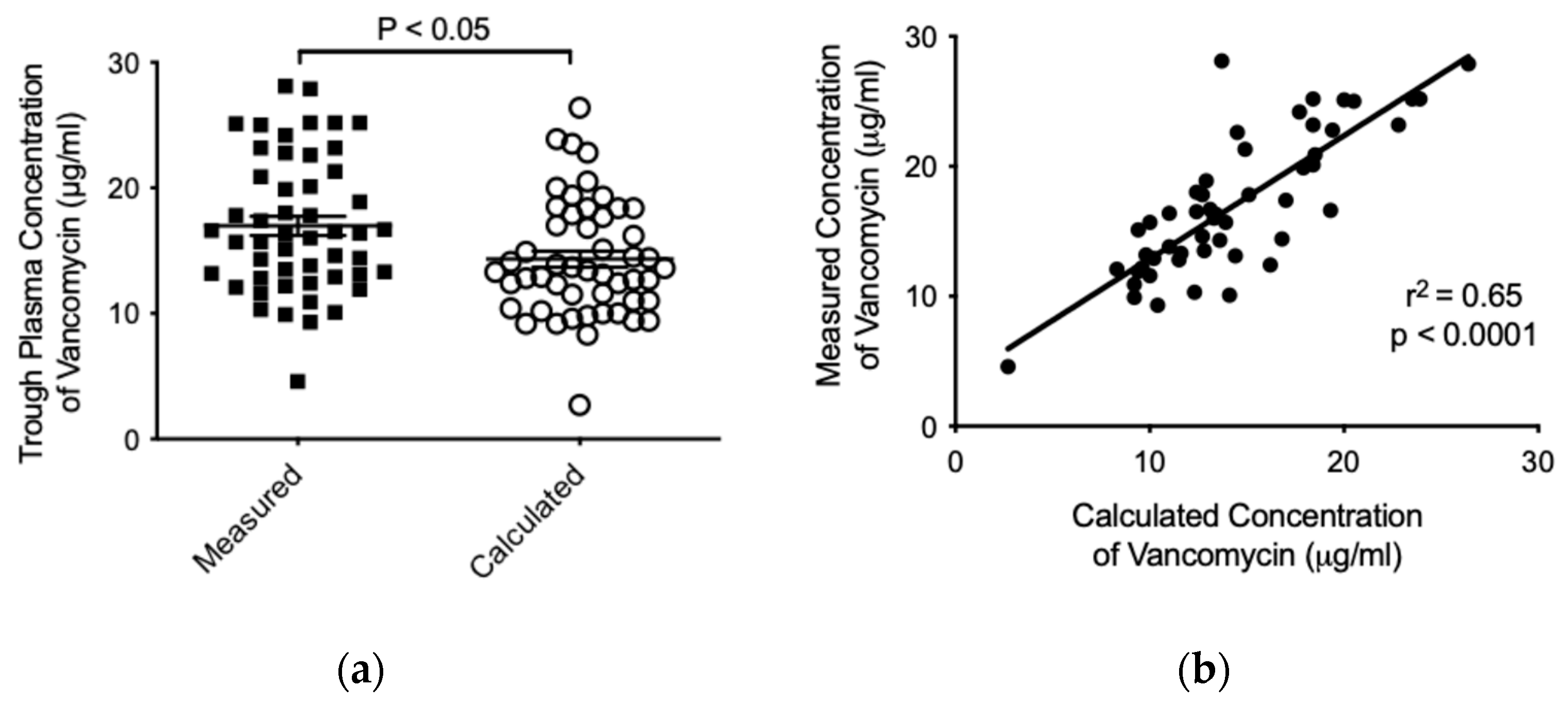
2.4. Analysis of Vancomycin Pharmacokinetics by Using the Antibiotic Kinetics® Software
3. Discussion
4. Materials and Methods
4.1. Subjects and Patient Selection
4.2. Vancomycin Loading Dose and Patient Follow-Up
4.3. Vancomycin Plasma Concentration Assay
4.4. Data and Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| APACHE | Acute Physiology and Chronic Health Evaluation |
| AUC0–24 | Area under the 24 h concentration–time curve |
| CG | Cockcroft–Gault |
| eGFR | Estimated glomerular filtration rate |
| ICU | Intensive care unit |
| MDRD-6v | 6-Variable Modification of Diet in Renal Disease |
| MIC | Minimum inhibitory concentration |
| PK/PD | Pharmacokinetic/pharmacodynamic |
| SS | Steady state |
References
- Gopalakrishnan, A.V.; Sunish, S.C.; Mathew, B.S.; Prabha, R.; Mathew, S.K. Stability of Vancomycin in Whole Blood. Ther. Drug Monit. 2021, 43, 443–444. [Google Scholar] [CrossRef] [PubMed]
- Moellering, R.C. Vancomycin: A 50-Year Reassessment. Clin. Infect. Dis. 2006, 42 (Suppl. 1), S3–S4. [Google Scholar] [CrossRef] [PubMed]
- Morales Castro, D.; Dresser, L.; Granton, J.; Fan, E. Pharmacokinetic Alterations Associated with Critical Illness. Clin. Pharmacokinet. 2023, 62, 209–220. [Google Scholar] [CrossRef]
- Zhang, T.; Krekels, E.H.J.; Smit, C.; van Dongen, E.P.A.; Brüggemann, R.J.M.; Knibbe, C.A.J. How to Dose Vancomycin in Overweight and Obese Patients with Varying Renal (Dys)Function in the Novel Era of AUC 400-600 Mg·h/L-Targeted Dosing. Clin. Pharmacokinet. 2024, 63, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Oyaert, M.; Spriet, I.; Allegaert, K.; Smits, A.; Vanstraelen, K.; Peersman, N.; Wauters, J.; Verhaegen, J.; Vermeersch, P.; Pauwels, S. Factors Impacting Unbound Vancomycin Concentrations in Different Patient Populations. Antimicrob. Agents Chemother. 2015, 59, 7073–7079. [Google Scholar] [CrossRef]
- Mizuno, T.; Mizokami, F.; Fukami, K.; Ito, K.; Shibasaki, M.; Nagamatsu, T.; Furuta, K. The Influence of Severe Hypoalbuminemia on the Half-Life of Vancomycin in Elderly Patients with Methicillin-Resistant Staphylococcus Aureus Hospital-Acquired Pneumonia. Clin. Interv. Aging 2013, 8, 1323–1328. [Google Scholar] [CrossRef]
- Song, K.-H.; Kim, H.B.; Kim, H.; Lee, M.J.; Jung, Y.; Kim, G.; Hwang, J.-H.; Kim, N.-H.; Kim, M.; Kim, C.-J.; et al. Impact of Area under the Concentration-Time Curve to Minimum Inhibitory Concentration Ratio on Vancomycin Treatment Outcomes in Methicillin-Resistant Staphylococcus Aureus Bacteraemia. Int. J. Antimicrob. Agents 2015, 46, 689–695. [Google Scholar] [CrossRef]
- Varghese, J.M.; Roberts, J.A.; Lipman, J. Antimicrobial Pharmacokinetic and Pharmacodynamic Issues in the Critically Ill with Severe Sepsis and Septic Shock. Crit. Care Clin. 2011, 27, 19–34. [Google Scholar] [CrossRef]
- Ulldemolins, M.; Roberts, J.A.; Lipman, J.; Rello, J. Antibiotic Dosing in Multiple Organ Dysfunction Syndrome. Chest 2011, 139, 1210–1220. [Google Scholar] [CrossRef]
- Moise-Broder, P.A.; Forrest, A.; Birmingham, M.C.; Schentag, J.J. Pharmacodynamics of Vancomycin and Other Antimicrobials in Patients with Staphylococcus Aureus Lower Respiratory Tract Infections. Clin. Pharmacokinet. 2004, 43, 925–942. [Google Scholar] [CrossRef]
- Kullar, R.; Davis, S.L.; Levine, D.P.; Rybak, M.J. Impact of Vancomycin Exposure on Outcomes in Patients with Methicillin-Resistant Staphylococcus Aureus Bacteremia: Support for Consensus Guidelines Suggested Targets. Clin. Infect. Dis. 2011, 52, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Oda, K.; Shoji, K.; Hanai, Y.; Takahashi, Y.; Fujii, S.; Hamada, Y.; Kimura, T.; Mayumi, T.; Ueda, T.; et al. Clinical Practice Guidelines for Therapeutic Drug Monitoring of Vancomycin in the Framework of Model-Informed Precision Dosing: A Consensus Review by the Japanese Society of Chemotherapy and the Japanese Society of Therapeutic Drug Monitoring. Pharmaceutics 2022, 14, 489. [Google Scholar] [CrossRef]
- Oshima, Y.; Matsumoto, M.; Munakata, S.; Tokimatsu, I.; Hattori, N.; Kotani, T.; Kusumoto, S.; Sagara, H.; Kato, M. Prediction of Area Under the Curve from Urinary Vancomycin Concentrations Measured Using a Simple Method. AAPS J. 2025, 27, 39. [Google Scholar] [CrossRef]
- Zasowski, E.J.; Murray, K.P.; Trinh, T.D.; Finch, N.A.; Pogue, J.M.; Mynatt, R.P.; Rybak, M.J. Identification of Vancomycin Exposure-Toxicity Thresholds in Hospitalized Patients Receiving Intravenous Vancomycin. Antimicrob. Agents Chemother. 2018, 62, e01684-17. [Google Scholar] [CrossRef] [PubMed]
- Hao, J.-J.; Chen, H.; Zhou, J.-X. Continuous versus Intermittent Infusion of Vancomycin in Adult Patients: A Systematic Review and Meta-Analysis. Int. J. Antimicrob. Agents 2016, 47, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.H.; Norris, R.; Barras, M.; Roberts, J.; Morris, R.; Doogue, M.; Jones, G.R.D. Therapeutic Monitoring of Vancomycin in Adult Patients: A Consensus Review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society Of Infectious Diseases Pharmacists. Clin. Biochem. Rev. 2010, 31, 21–24. [Google Scholar]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Therapeutic Monitoring of Vancomycin for Serious Methicillin-Resistant Staphylococcus Aureus Infections: A Revised Consensus Guideline and Review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Clin. Infect. Dis. 2020, 71, 1361–1364. [Google Scholar] [CrossRef]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin-Resistant Staphylococcus Aureus Infections in Adults and Children. Clin. Infect. Dis. 2011, 52, e18–e55. [Google Scholar] [CrossRef]
- Mohr, J.F.; Murray, B.E. Point: Vancomycin Is Not Obsolete for the Treatment of Infection Caused by Methicillin-Resistant Staphylococcus Aureus. Clin. Infect. Dis. 2007, 44, 1536–1542. [Google Scholar] [CrossRef]
- Álvarez, O.; Plaza-Plaza, J.C.; Ramirez, M.; Peralta, A.; Amador, C.A.; Amador, R. Pharmacokinetic Assessment of Vancomycin Loading Dose in Critically Ill Patients. Antimicrob. Agents Chemother. 2017, 61, e00280-17. [Google Scholar] [CrossRef]
- Revilla, N.; Martín-Suárez, A.; Pérez, M.P.; González, F.M.; Fernández de Gatta, M.D.M. Vancomycin Dosing Assessment in Intensive Care Unit Patients Based on a Population Pharmacokinetic/Pharmacodynamic Simulation. Br. J. Clin. Pharmacol. 2010, 70, 201–212. [Google Scholar] [CrossRef]
- Álvarez, R.; López Cortés, L.E.; Molina, J.; Cisneros, J.M.; Pachón, J. Optimizing the Clinical Use of Vancomycin. Antimicrob. Agents Chemother. 2016, 60, 2601–2609. [Google Scholar] [CrossRef] [PubMed]
- Chaijamorn, W.; Wanakamanee, U. Pharmacokinetics of Vancomycin in Critically Ill Patients Undergoing Continuous Venovenous Haemodialysis. Int. J. Antimicrob. Agents 2014, 44, 367–368. [Google Scholar] [CrossRef]
- Rider, T.R.; Silinskie, K.M.; Hite, M.S.; Bress, J. Pharmacokinetics of Vancomycin in Critically Ill Patients Undergoing Sustained Low-Efficiency Dialysis. Pharmacotherapy 2020, 40, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Alobaid, A.S.; Hites, M.; Lipman, J.; Taccone, F.S.; Roberts, J.A. Effect of Obesity on the Pharmacokinetics of Antimicrobials in Critically Ill Patients: A Structured Review. Int. J. Antimicrob. Agents 2016, 47, 259–268. [Google Scholar] [CrossRef]
- Shahrami, B.; Najmeddin, F.; Mousavi, S.; Ahmadi, A.; Rouini, M.R.; Sadeghi, K.; Mojtahedzadeh, M. Achievement of Vancomycin Therapeutic Goals in Critically Ill Patients: Early Individualization May Be Beneficial. Crit. Care Res. Pract. 2016, 2016, 1245815. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Preuss, C.V.; Bernice, F. Vancomycin. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Aslan, A.T.; Kara, E.; Köksal, G.; Bilir, Y.; Saraçoğlu, K.T.; Eser, F.; Güner, R.; Alkan, S.; D’Avino, A.; Escudero-Sanchez, R.; et al. Comparison of Piperacillin-Tazobactam and Vancomycin (TZP-VAN) with Piperacillin-Tazobactam and Teicoplanin (TZP-TEI) for the Risk of Acute Kidney Injury (CONCOMITANT): A Prospective Observational, Multinational, Multi-Centre Cohort Study. Int. J. Antimicrob. Agents 2025, 65, 107446. [Google Scholar] [CrossRef]
- Momattin, H.; Zogheib, M.; Homoud, A.; Al-Tawfiq, J.A. Safety and Outcome of Pharmacy-Led Vancomycin Dosing and Monitoring. Chemotherapy 2016, 61, 3–7. [Google Scholar] [CrossRef]
- Haeseker, M.; Croes, S.; Neef, C.; Bruggeman, C.; Stolk, L.; Verbon, A. Evaluation of Vancomycin Prediction Methods Based on Estimated Creatinine Clearance or Trough Levels. Ther. Drug Monit. 2016, 38, 120–126. [Google Scholar] [CrossRef]
- Roberts, J.A.; Lipman, J. Pharmacokinetic Issues for Antibiotics in the Critically Ill Patient. Crit. Care Med. 2009, 37, 840–851. [Google Scholar] [CrossRef]
- Shimamoto, Y.; Fukuda, T.; Tanaka, K.; Komori, K.; Sadamitsu, D. Systemic Inflammatory Response Syndrome Criteria and Vancomycin Dose Requirement in Patients with Sepsis. Intensive Care Med. 2013, 39, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Kosmisky, D.E.; Griffiths, C.L.; Templin, M.A.; Norton, J.; Martin, K.E. Evaluation of a New Vancomycin Dosing Protocol in Morbidly Obese Patients. Hosp. Pharm. 2015, 50, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Prybylski, J.P. Vancomycin Trough Concentration as a Predictor of Clinical Outcomes in Patients with Staphylococcus Aureus Bacteremia: A Meta-Analysis of Observational Studies. Pharmacotherapy 2015, 35, 889–898. [Google Scholar] [CrossRef]
- Masich, A.M.; Kalaria, S.N.; Gonzales, J.P.; Heil, E.L.; Tata, A.L.; Claeys, K.C.; Patel, D.; Gopalakrishnan, M. Vancomycin Pharmacokinetics in Obese Patients with Sepsis or Septic Shock. Pharmacotherapy 2020, 40, 211–220. [Google Scholar] [CrossRef]
- van Hal, S.J.; Paterson, D.L.; Lodise, T.P. Systematic Review and Meta-Analysis of Vancomycin-Induced Nephrotoxicity Associated with Dosing Schedules That Maintain Troughs between 15 and 20 Milligrams per Liter. Antimicrob. Agents Chemother. 2013, 57, 734–744. [Google Scholar] [CrossRef] [PubMed]
- Reardon, J.; Lau, T.T.Y.; Ensom, M.H.H. Vancomycin Loading Doses: A Systematic Review. Ann. Pharmacother. 2015, 49, 557–565. [Google Scholar] [CrossRef]
- Butterfield, J.M.; Patel, N.; Pai, M.P.; Rosano, T.G.; Drusano, G.L.; Lodise, T.P. Refining Vancomycin Protein Binding Estimates: Identification of Clinical Factors That Influence Protein Binding. Antimicrob. Agents Chemother. 2011, 55, 4277–4282. [Google Scholar] [CrossRef]
- Li, L.; Miles, M.V.; Lakkis, H.; Zaritsky, A.L. Vancomycin-Binding Characteristics in Patients with Serious Infections. Pharmacotherapy 1996, 16, 1024–1029. [Google Scholar] [CrossRef]
- Li, X.; Xu, W.; Li, R.; Guo, Q.; Li, X.; Sun, J.; Sun, S.; Li, J. Prediction of Unbound Vancomycin Levels in Intensive Care Unit and Nonintensive Care Unit Patients: Total Bilirubin May Play an Important Role. Infect. Drug Resist. 2021, 14, 2543–2554. [Google Scholar] [CrossRef]
- Crew, P.; Heintz, S.J.; Heintz, B.H. Vancomycin Dosing and Monitoring for Patients with End-Stage Renal Disease Receiving Intermittent Hemodialysis. Am. J. Health-Syst. Pharm. 2015, 72, 1856–1864. [Google Scholar] [CrossRef]
- AbPK Patient Data. Available online: http://rxkinetics.net/abpk.aspx (accessed on 11 February 2025).
- Chung, J.; Oh, J.M.; Cho, E.M.; Jang, H.J.; Hong, S.B.; Lim, C.M.; Koh, Y.S. Optimal Dose of Vancomycin for Treating Methicillin-Resistant Staphylococcus Aureus Pneumonia in Critically Ill Patients. Anaesth. Intensive Care 2011, 39, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, I.; Amador, C.; Plaza, J.C.; Correa, G.; Amador, R. [Assessment of an active pharmacovigilance system carried out by a pharmacist]. Rev. Médica Chile 2014, 142, 998–1005. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Baseline Values (n = 51) |
| Age (years) | 58 (18–79) |
| Gender (M/F) | 36/15 |
| Height (m) | 1.68 (1.43–1.85) |
| Weight (kg) | 75 (45–105) |
| Serum creatinine (mg/dL) | 0.80 (0.28–2.07) |
| eGFR (mL/min/1.73 m2) CG equation | 103 (20–208) |
| eGFR (mL/min/1.73 m2) MDRD-6v formula | 84 (19–151) |
| APACHE II score | 21 (15–38) |
| Comorbidities | |
| Hypertension | 23% |
| Cancer | 18% |
| Type II diabetes mellitus | 17% |
| Non-hypertensive cardiomyopathies | 11% |
| Human immunodeficiency virus | 9% |
| Obstructive pulmonary syndrome | 8% |
| Dyslipidemia | 6% |
| Tuberculosis | 4% |
| Hepatitis | 2% |
| Others | 2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amador, J.S.; Vega, Á.; Araos, P.; Quiñones, L.A.; Amador, C.A. A Successful Experience of Individualized Vancomycin Dosing in Critically Ill Patients by Using a Loading Dose and Maintenance Dose. Pharmaceuticals 2025, 18, 677. https://doi.org/10.3390/ph18050677
Amador JS, Vega Á, Araos P, Quiñones LA, Amador CA. A Successful Experience of Individualized Vancomycin Dosing in Critically Ill Patients by Using a Loading Dose and Maintenance Dose. Pharmaceuticals. 2025; 18(5):677. https://doi.org/10.3390/ph18050677
Chicago/Turabian StyleAmador, Jorge S., Álvaro Vega, Patricio Araos, Luis A. Quiñones, and Cristián A. Amador. 2025. "A Successful Experience of Individualized Vancomycin Dosing in Critically Ill Patients by Using a Loading Dose and Maintenance Dose" Pharmaceuticals 18, no. 5: 677. https://doi.org/10.3390/ph18050677
APA StyleAmador, J. S., Vega, Á., Araos, P., Quiñones, L. A., & Amador, C. A. (2025). A Successful Experience of Individualized Vancomycin Dosing in Critically Ill Patients by Using a Loading Dose and Maintenance Dose. Pharmaceuticals, 18(5), 677. https://doi.org/10.3390/ph18050677