
Smartphone as a Sensor in mHealth: Narrative Overview, SWOT Analysis, and Proposal of Mobile Biomarkers

 , , ,
, , , 

Abstract
1. Introduction
- Q1
- What is the status of smartphone-only passive monitoring as an approach?
- Q2
- What advancements are needed to make this approach more reliable and adopted more widely?
- Q3
- How could the latest advancements in AI benefit mobile-based passive monitoring?
2. Methodology
Selection of Reviews
3. SWOT Analysis
3.1. Strengths
- Specific application to cancer monitoring, tackling a wide range of cancer symptoms ranging from physical to mental health [21].
3.2. Threats
3.3. Weaknesses
3.4. Opportunities
4. Discussion
- Decoupling advancements in analytic techniques from the implementation and deployment of virtual sensors.
- Decoupling data collection from third-party providers (private or public), enabling the creation of a personal data vault for individual use or for sharing with public or private care providers as needed throughout one’s lifetime.
- How AI technologies are changing user interaction modalities, replacing traditional forms and wizards with conversational interfaces [36].
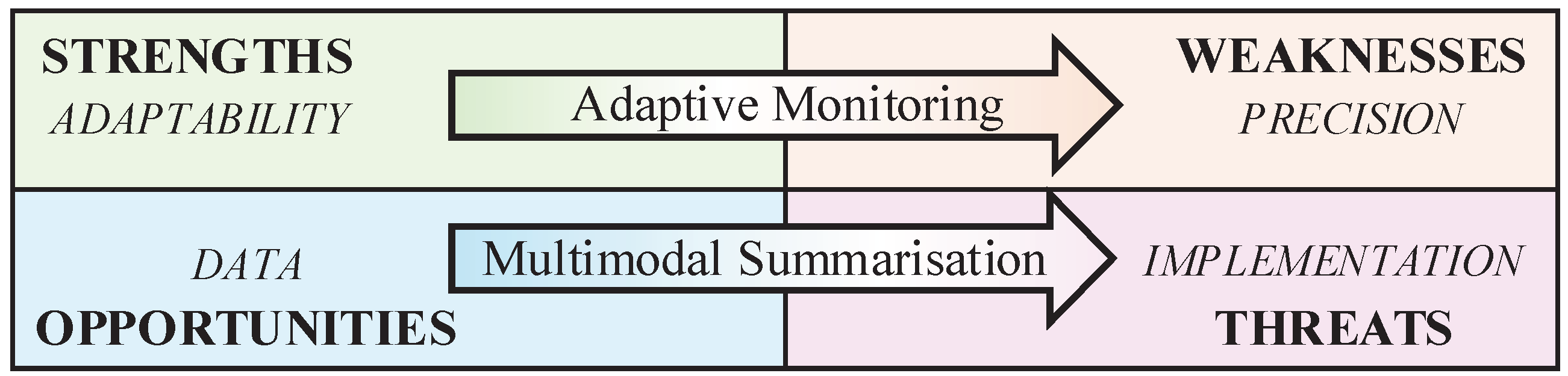
5. Proposed Approach—Mobile Biomarkers
5.1. Multimodal Summarisation
5.2. Adaptive Monitoring
- Small-data machine learning, where large datasets are not available, such as smartphone-based models trained on user data. Small-data machine learning requires “optimal utilisation of data” achieved by interacting with experts (or users) [56].
- Pattern mining in exploratory data analysis, which involves incrementally improving the model by incorporating user insights to identify relevant elements in the data. This approach also serves the dual purpose of enhancing model explainability through user input [56].
- Low-computing resource machine learning—improved, again, by an IML-optimised use of data [56].
- Activity recognition using a dynamic set of sensors (i.e., alternative combinations of smartphone sensors based on actual use) [57], emerged from the narrative meta-review as particularly relevant for improving the quality of passive monitoring analysis.
5.3. Clinical Tasks
5.4. Ethics of Mobile Biomarkers
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rowland, S.P.; Fitzgerald, J.E.; Holme, T.; Powell, J.; McGregor, A. What is the clinical value of mHealth for patients? NPJ Digit. Med. 2020, 3, 4. [Google Scholar] [CrossRef] [PubMed]
- Spinsante, S.; Montanini, L.; Gambi, E.; Lambrinos, L.; Pereira, F.; Pombo, N.; Garcia, N. Smartphones as Multipurpose Intelligent Objects for AAL: Two Case Studies. In Proceedings of the Smart Objects and Technologies for Social Good: Second International Conference, GOODTECHS 2016, Venice, Italy, 30 November–1 December 2016; Proceedings 2. Springer: Berlin/Heidelberg, Germany, 2017; pp. 125–134. [Google Scholar]
- Woods, L.S.; Duff, J.; Roehrer, E.; Walker, K.; Cummings, E. Patients’ experiences of using a consumer mHealth app for self-management of heart failure: Mixed-methods study. JMIR Hum. Factors 2019, 6, e13009. [Google Scholar] [CrossRef] [PubMed]
- Meyerowitz-Katz, G.; Ravi, S.; Arnolda, L.; Feng, X.; Maberly, G.; Astell-Burt, T. Rates of Attrition and Dropout in App-Based Interventions for Chronic Disease: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2020, 22, e20283. [Google Scholar] [CrossRef]
- Weik, L.; Fehring, L.; Mortsiefer, A.; Meister, S. Understanding inherent influencing factors to digital health adoption in general practices through a mixed-methods analysis. NPJ Digit. Med. 2024, 7, 47. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, P.; Liu, J.; Gong, Y.; Wang, J.; Guo, Y. Emerging artificial intelligence–empowered mhealth: Scoping review. JMIR mHealth uHealth 2022, 10, e35053. [Google Scholar] [CrossRef]
- Sheikh, M.; Qassem, M.; Kyriacou, P.A. Wearable, environmental, and smartphone-based passive sensing for mental health monitoring. Front. Digit. Health 2021, 3, 662811. [Google Scholar] [CrossRef]
- Ghazinoory, S.; Abdi, M.; Azadegan-Mehr, M. SWOT methodology: A state-of-the-art review for the past, a framework for the future. J. Bus. Econ. Manag. 2011, 12, 24–48. [Google Scholar] [CrossRef]
- Coravos, A.; Khozin, S.; Mandl, K.D. Developing and adopting safe and effective digital biomarkers to improve patient outcomes. NPJ Digit. Med. 2019, 2, 14. [Google Scholar] [CrossRef]
- Sukhera, J. Narrative reviews: Flexible, rigorous, and practical. J. Grad. Med Educ. 2022, 14, 414–417. [Google Scholar] [CrossRef]
- Kulkarni, P.; Kirkham, R.; McNaney, R. Opportunities for smartphone sensing in e-health research: A narrative review. Sensors 2022, 22, 3893. [Google Scholar] [CrossRef]
- Baxter, C.; Carroll, J.A.; Keogh, B.; Vandelanotte, C. Assessment of mobile health apps using built-in smartphone sensors for diagnosis and treatment: Systematic survey of apps listed in international curated health app libraries. JMIR mHealth uHealth 2020, 8, e16741. [Google Scholar] [CrossRef] [PubMed]
- Cornet, V.P.; Holden, R.J. Systematic review of smartphone-based passive sensing for health and wellbeing. J. Biomed. Inform. 2018, 77, 120–132. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P. Smartphone applications for patients’ health and fitness. Am. J. Med. 2016, 129, 11–19. [Google Scholar] [CrossRef]
- Khoo, L.S.; Lim, M.K.; Chong, C.Y.; McNaney, R. Machine Learning for Multimodal Mental Health Detection: A Systematic Review of Passive Sensing Approaches. Sensors 2024, 24, 348. [Google Scholar] [CrossRef]
- Krichen, M. Anomalies detection through smartphone sensors: A review. IEEE Sens. J. 2021, 21, 7207–7217. [Google Scholar] [CrossRef]
- Majumder, S.; Deen, M.J. Smartphone sensors for health monitoring and diagnosis. Sensors 2019, 19, 2164. [Google Scholar] [CrossRef]
- Qirtas, M.M.; Zafeiridi, E.; Pesch, D.; White, E.B. Loneliness and Social Isolation Detection Using Passive Sensing Techniques: Scoping Review. JMIR mHealth uHealth 2022, 10, e34638. [Google Scholar] [CrossRef]
- Rogan, J.; Bucci, S.; Firth, J. Health Care Professionals’ Views on the Use of Passive Sensing, AI, and Machine Learning in Mental Health Care: Systematic Review With Meta-Synthesis. JMIR Mental Health 2024, 11, e49577. [Google Scholar] [CrossRef]
- Straczkiewicz, M.; James, P.; Onnela, J.P. A systematic review of smartphone-based human activity recognition methods for health research. NPJ Digit. Med. 2021, 4, 148. [Google Scholar] [CrossRef]
- Stuijt, D.G.; Radanovic, I.; Kos, M.; Schoones, J.W.; Stuurman, F.E.; Exadaktylos, V.; Bins, A.D.; Bosch, J.J.; van Oijen, M.G. Smartphone-Based Passive Sensing in Monitoring Patients with Cancer: A Systematic Review. JCO Clin. Cancer Inform. 2023, 7, e2300141. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Ibrahim, A.; Parsia, B.; Poliakoff, E.; Harper, S. Passive social sensing with smartphones: A systematic review. Computing 2023, 105, 29–51. [Google Scholar] [CrossRef]
- Rizzo, A.; Kim, G.J. A SWOT analysis of the field of virtual reality rehabilitation and therapy. Presence 2005, 14, 119–146. [Google Scholar] [CrossRef]
- Albanese, G.A.; Bucchieri, A.; Podda, J.; Tacchino, A.; Buccelli, S.; De Momi, E.; Laffranchi, M.; Mannella, K.; Holmes, M.W.; Zenzeri, J.; et al. Robotic systems for upper-limb rehabilitation in multiple sclerosis: A SWOT analysis and the synergies with virtual and augmented environments. Front. Robot. AI 2024, 11, 1335147. [Google Scholar] [CrossRef] [PubMed]
- Stavros, J.; Cooperrider, D.; Kelley, D.L. Strategic inquiry appreciative intent: Inspiration to SOAR, a new framework for strategic planning. AI Pract. 2003, 5, 10–17. [Google Scholar]
- McConnell, E.R.; Bell, S.M.; Cote, I.; Wang, R.L.; Perkins, E.J.; Garcia-Reyero, N.; Gong, P.; Burgoon, L.D. Systematic Omics Analysis Review (SOAR) tool to support risk assessment. PLoS ONE 2014, 9, e110379. [Google Scholar] [CrossRef]
- Yusoff, M.S.B. A Practical Guide Using the NOISE Analysis Model for Strategic Action Planning in Health Profession Education. Educ. Med. J. 2024, 16, 199–210. [Google Scholar] [CrossRef]
- Zarestky, J.; Cole, C.S. Strengths, opportunities, aspirations, and results: An emerging approach to organization development. New Horizons Adult Educ. Hum. Resour. Dev. 2017, 29, 5–19. [Google Scholar] [CrossRef]
- Porter, M.E. The five competitive forces that shape strategy. Harv. Bus. Rev. 2008, 86, 78. [Google Scholar]
- Pavic, M.; Klaas, V.; Theile, G.; Kraft, J.; Tröster, G.; Blum, D.; Guckenberger, M. Mobile health technologies for continuous monitoring of cancer patients in palliative care aiming to predict health status deterioration: A feasibility study. J. Palliat. Med. 2020, 23, 678–685. [Google Scholar] [CrossRef]
- Pavic, M.; Klaas, V.; Theile, G.; Kraft, J.; Tröster, G.; Guckenberger, M. Feasibility and usability aspects of continuous remote monitoring of health status in palliative cancer patients using wearables. Oncology 2020, 98, 386–395. [Google Scholar] [CrossRef]
- Rooksby, J.; Morrison, A.; Murray-Rust, D. Student perspectives on digital phenotyping: The acceptability of using smartphone data to assess mental health. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems, New York, NY, USA, 4–9 May 2019; pp. 1–14. [Google Scholar]
- Eagle, N.; Pentland, A. Reality mining: Sensing complex social systems. Pers. Ubiquitous Comput. 2006, 10, 255–268. [Google Scholar] [CrossRef]
- Ryding, F.C.; Kuss, D.J. Passive objective measures in the assessment of problematic smartphone use: A systematic review. Addict. Behav. Rep. 2020, 11, 100257. [Google Scholar] [CrossRef] [PubMed]
- England, N. The 5 Pillars of Medical Diagnostics. Available online: https://digital.nhs.uk/cyber-and-data-security/guidance-and-assurance/network-segmentation/imaging/the-5-pillars-of-medical-diagnostics (accessed on 8 January 2025).
- Stige, Å.; Zamani, E.D.; Mikalef, P.; Zhu, Y. Artificial intelligence (AI) for user experience (UX) design: A systematic literature review and future research agenda. Inf. Technol. People 2024, 37, 2324–2352. [Google Scholar] [CrossRef]
- Ma, C.; Li, J.; Wei, K.; Liu, B.; Ding, M.; Yuan, L.; Han, Z.; Poor, H.V. Trusted ai in multiagent systems: An overview of privacy and security for distributed learning. Proc. IEEE 2023, 111, 1097–1132. [Google Scholar] [CrossRef]
- Kirienko, M.; Sollini, M.; Ninatti, G.; Loiacono, D.; Giacomello, E.; Gozzi, N.; Amigoni, F.; Mainardi, L.; Lanzi, P.L.; Chiti, A. Distributed learning: A reliable privacy-preserving strategy to change multicenter collaborations using AI. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3791–3804. [Google Scholar] [CrossRef]
- Wei, W.; Liu, L. Trustworthy distributed ai systems: Robustness, privacy, and governance. ACM Comput. Surv. 2025, 57, 1–42. [Google Scholar] [CrossRef]
- Motahari-Nezhad, H.; Fgaier, M.; Mahdi Abid, M.; Péntek, M.; Gulácsi, L.; Zrubka, Z. Digital biomarker–based studies: Scoping review of systematic reviews. JMIR mHealth uHealth 2022, 10, e35722. [Google Scholar] [CrossRef]
- Motahari-Nezhad, H.; Al-Abdulkarim, H.; Fgaier, M.; Abid, M.M.; Péntek, M.; Gulácsi, L.; Zrubka, Z. Digital Biomarker–Based Interventions: Systematic Review of Systematic Reviews. J. Med. Internet Res. 2022, 24, e41042. [Google Scholar] [CrossRef]
- Vasudevan, S.; Saha, A.; Tarver, M.E.; Patel, B. Digital biomarkers: Convergence of digital health technologies and biomarkers. NPJ Digit. Med. 2022, 5, 36. [Google Scholar] [CrossRef]
- Barresi, G.; Gaggioli, A.; Sternini, F.; Ravizza, A.; Pacchierotti, C.; De Michieli, L. Digital twins and healthcare: Quick overview and human-centric perspectives. In mHealth and Human-Centered Design Towards Enhanced Health, Care, and Well-Being; Springer: Berlin/Heidelberg, Germany, 2023; pp. 57–78. [Google Scholar]
- Barresi, G.; Zenzeri, J.; Tessadori, J.; Laffranchi, M.; Semprini, M.; De Michieli, L. Neuro-gerontechnologies: Applications and opportunities. In Internet of Things for Human-Centered Design: Application to Elderly Healthcare; Springer: Berlin/Heidelberg, Germany, 2022; pp. 123–153. [Google Scholar]
- Lahat, D.; Adali, T.; Jutten, C. Multimodal data fusion: An overview of methods, challenges, and prospects. Proc. IEEE 2015, 103, 1449–1477. [Google Scholar] [CrossRef]
- Awad Abdellatif, A.; Emam, A.; Chiasserini, C.F.; Mohamed, A.; Jaoua, A.; Ward, R. Edge-based compression and classification for smart healthcare systems: Concept, implementation and evaluation. Expert Syst. Appl. 2019, 117, 1–14. [Google Scholar] [CrossRef]
- Abdellatif, A.A.; Mohamed, A.; Chiasserini, C.F.; Tlili, M.; Erbad, A. Edge Computing for Smart Health: Context-Aware Approaches, Opportunities, and Challenges. IEEE Netw. 2019, 33, 196–203. [Google Scholar] [CrossRef]
- Choo, M.; Park, D.; Cho, M.; Bae, S.; Kim, J.; Han, D.H. Exploring a multimodal approach for utilizing digital biomarkers for childhood mental health screening. Front. Psychiatry 2024, 15, 1348319. [Google Scholar] [CrossRef] [PubMed]
- Go ni, M.; Eickhoff, S.B.; Far, M.S.; Patil, K.R.; Dukart, J. Smartphone-based digital biomarkers for Parkinson’s disease in a remotely-administered setting. IEEE Access 2022, 10, 28361–28384. [Google Scholar] [CrossRef]
- Schwab, P.; Karlen, W. A deep learning approach to diagnosing multiple sclerosis from smartphone data. IEEE J. Biomed. Health Inform. 2020, 25, 1284–1291. [Google Scholar] [CrossRef]
- Ahmed, M.; Barkat Ullah, A.S. Infrequent pattern mining in smart healthcare environment using data summarization. J. Supercomput. 2018, 74, 5041–5059. [Google Scholar] [CrossRef]
- Index—FHIR v5.0.0—hl7.org. Available online: https://hl7.org/fhir/ (accessed on 12 December 2024).
- Bishop, C.M. Model-based machine learning. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2013, 371, 20120222. [Google Scholar] [CrossRef]
- Yang, Q.; Liu, Y.; Chen, T.; Tong, Y. Federated machine learning: Concept and applications. ACM Trans. Intell. Syst. Technol. (TIST) 2019, 10, 1–19. [Google Scholar] [CrossRef]
- Park, H.; Kim, S. Overviewing AI-Dedicated Hardware for On-Device AI in Smartphones. In Artificial Intelligence and Hardware Accelerators; Mishra, A., Cha, J., Park, H., Kim, S., Eds.; Springer International Publishing: Cham, Switzerland, 2023; pp. 127–150. [Google Scholar] [CrossRef]
- Wondimu, N.A.; Buche, C.; Visser, U. Interactive machine learning: A state of the art review. arXiv 2022, arXiv:2207.06196. [Google Scholar]
- Tegen, A.; Davidsson, P.; Persson, J.A. Activity recognition through interactive machine learning in a dynamic sensor setting. In Personal and Ubiquitous Computing; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–14. [Google Scholar]
- Jin, J.; Sun, W.; Al-Turjman, F.; Khan, M.B.; Yang, X. Activity pattern mining for healthcare. IEEE Access 2020, 8, 56730–56738. [Google Scholar] [CrossRef]
- Zhang, L.; Zhao, J.; Wang, Y.; Xie, B. Mining patterns of disease progression: A topic-model-based approach. In Exploring Complexity in Health: An Interdisciplinary Systems Approach; IOS Press: Amsterdam, The Netherlands, 2016; pp. 354–358. [Google Scholar]
- Pinaire, J.; Chabert, E.; Azé, J.; Bringay, S.; Landais, P. Sequential Pattern Mining to Predict Medical In-Hospital Mortality from Administrative Data: Application to Acute Coronary Syndrome. J. Healthc. Eng. 2021, 2021, 5531807. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Miron-Shatz, T.; Schumacher, N.; Krocza, J.; Diamantidis, C.; Albrecht, U.V. mHealth 2.0: Experiences, possibilities, and perspectives. JMIR mHealth uHealth 2014, 2, e3328. [Google Scholar] [CrossRef] [PubMed]
- Petrushin, A.; Freddolini, M.; Barresi, G.; Bustreo, M.; Laffranchi, M.; Del Bue, A.; De Michieli, L. IoT-powered monitoring systems for geriatric healthcare: Overview. In Internet of Things for Human-Centered Design: Application to Elderly Healthcare; Springer: Berlin/Heidelberg, Germany, 2022; pp. 99–122. [Google Scholar]
- Friedman, B.; Kahn, P.; Borning, A. Value sensitive design: Theory and methods. Univ. Wash. Tech. Rep. 2002, 2, 1–8. [Google Scholar]
- Detweiler, C.; Hindriks, K. Value-sensitive design patterns for pervasive health care. In Proceedings of the 2012 IEEE International Conference on Pervasive Computing and Communications Workshops, Lugano, Switzerland, 19–23 March 2012; pp. 908–913. [Google Scholar]
- Victor, G.; Barbu, A.; Bélisle-Pipon, J.C. Moral Values in Medical AI: A Scoping Review. 2024. Available online: https://www.researchsquare.com/article/rs-4391239/v1 (accessed on 5 June 2025).
- Feuerriegel, S.; Dolata, M.; Schwabe, G. Fair AI: Challenges and opportunities. Bus. Inf. Syst. Eng. 2020, 62, 379–384. [Google Scholar] [CrossRef]
- Bibi, A.; Noor, U.; Rashid, Z. Metaverse with Mobile Twin Edge Computing: Empowering Optimal Efficiency and Accuracy. In Proceedings of the 2024 International Conference on Engineering & Computing Technologies (ICECT), Islamabad, Pakistan, 23 May 2024; pp. 1–6. [Google Scholar]
- Damaševičius, R.; Maskeliūnas, R.; Misra, S. Supporting and shaping human decisions through internet of behaviors (iob): Perspectives and implications. In Machine Intelligence for Smart Applications: Opportunities and Risks; Springer: Berlin/Heidelberg, Germany, 2023; pp. 115–144. [Google Scholar]
- Li, N.; Hopfgartner, F. To log or not to log? SWOT analysis of self-tracking. In Lifelogging: Digital Self-Tracking and Lifelogging-Between Disruptive Technology and Cultural Transformation; Springer: Berlin/Heidelberg, Germany, 2016; pp. 305–325. [Google Scholar]
- Anderson, L.N.; Womack, J.J.; Ledford, C.J. Initial development and testing of a measure of credibility of mobile health apps: A clinical study among women seeking prenatal care. Atl. J. Commun. 2023, 31, 144–151. [Google Scholar] [CrossRef]
- Nadal, C.; Sas, C.; Doherty, G. Technology acceptance in mobile health: Scoping review of definitions, models, and measurement. J. Med. Internet Res. 2020, 22, e17256. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mental Conditions | Physical Conditions | Technical Focus | Clinical Focus | |
|---|---|---|---|---|
| Baxter, 2020 [12] | x | x | x | |
| Cornet & Holden, 2018 [13] | x | x | ||
| Higgins, 2016 [14] | x | x | ||
| Khoo, 2021 [15] | x | x | ||
| Krichen, 2021 [16] | x | x | x | |
| Kulkarni, 2021 [11] | x | x | x | |
| Mahsa, 2021 [7] | x | x | ||
| Majumder & Deen, 2019 [17] | x | x | ||
| Qirtas, 2021 [18] | x | x | ||
| Rogan, 2024 [19] | x | x | ||
| Straczkiewicz, 2021 [20] | x | x | ||
| Stuijt, 2023 [21] | x | x | x | |
| Zhang, 2023 [22] | x | x |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antonini, A.; Coşar, S.; Naja, I.; Haleem, M.S.; Macdonald, J.H.; Innominato, P.; Barresi, G. Smartphone as a Sensor in mHealth: Narrative Overview, SWOT Analysis, and Proposal of Mobile Biomarkers. Sensors 2025, 25, 3655. https://doi.org/10.3390/s25123655
Antonini A, Coşar S, Naja I, Haleem MS, Macdonald JH, Innominato P, Barresi G. Smartphone as a Sensor in mHealth: Narrative Overview, SWOT Analysis, and Proposal of Mobile Biomarkers. Sensors. 2025; 25(12):3655. https://doi.org/10.3390/s25123655
Chicago/Turabian StyleAntonini, Alessio, Serhan Coşar, Iman Naja, Muhammad Salman Haleem, Jamie Hugo Macdonald, Paquale Innominato, and Giacinto Barresi. 2025. "Smartphone as a Sensor in mHealth: Narrative Overview, SWOT Analysis, and Proposal of Mobile Biomarkers" Sensors 25, no. 12: 3655. https://doi.org/10.3390/s25123655
APA StyleAntonini, A., Coşar, S., Naja, I., Haleem, M. S., Macdonald, J. H., Innominato, P., & Barresi, G. (2025). Smartphone as a Sensor in mHealth: Narrative Overview, SWOT Analysis, and Proposal of Mobile Biomarkers. Sensors, 25(12), 3655. https://doi.org/10.3390/s25123655