Auditory Cue Based on the Golden Ratio Can Improve Gait Patterns in People with Parkinson’s Disease


 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Additional Clinical Evaluation
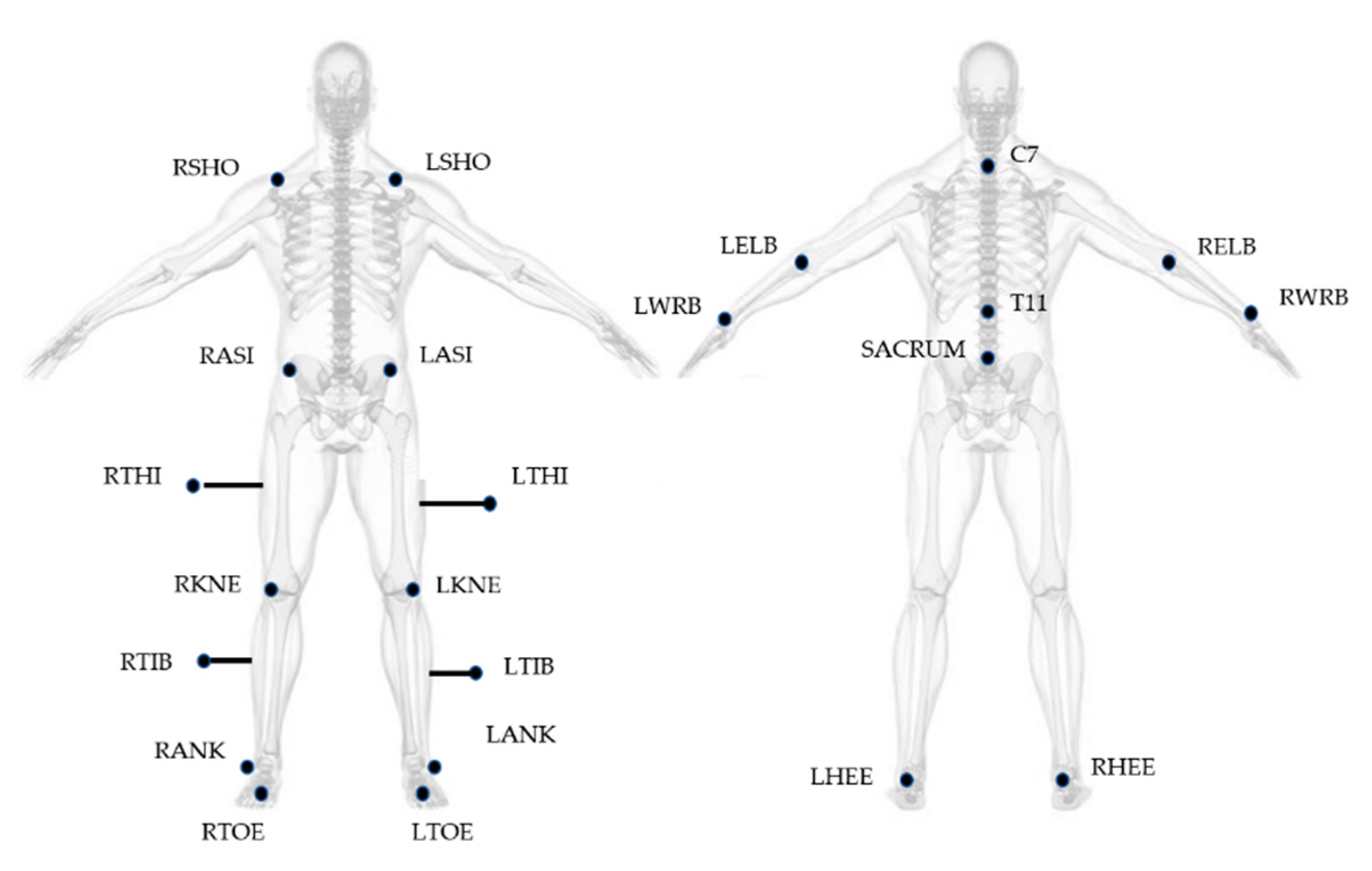
2.3. Instrumentation
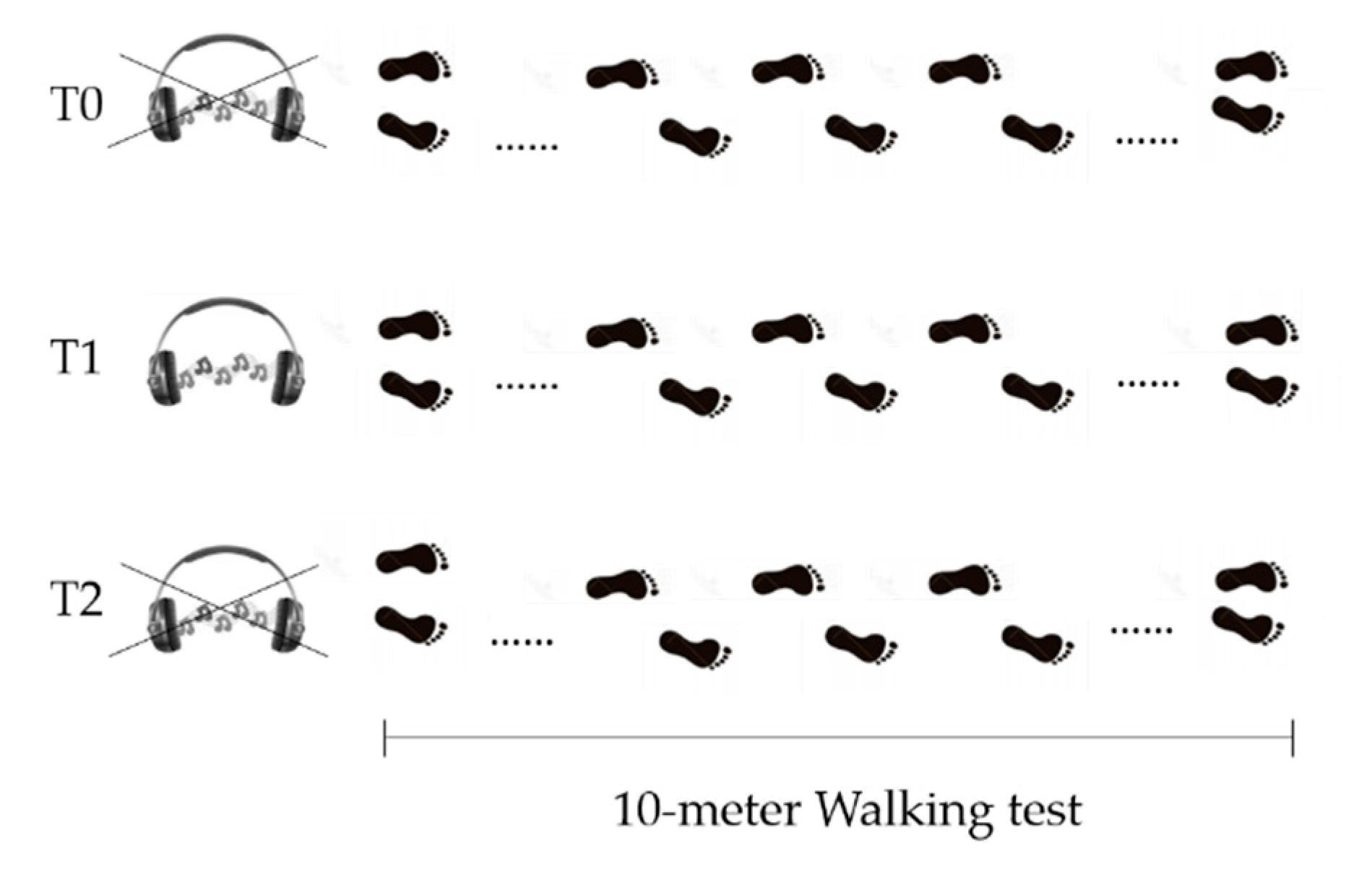
2.4. Study Design
- Before Golden Rhythm (GR) administration (T0): patients were asked to walk at their preferred walking speed. After the five trials, average walking speed was calculated and used to obtain the personalized GR (further information about GR calculation are reported below). The resulting rhythm structure had a duration equal to the gait cycle duration for each patient, with the abovementioned proportion between the two gait phases equal to ϕ.
- During Golden Rhythm administration (T1): the personalized GR cue was administered to each patient for at least 5 min before the data collection, while they were asked to familiarize with the rhythm while walking. After this time, five walking trials were recorded.
- After Golden Rhythm administration (T2): the measurement was performed at least 5 min after the stimulus removal. An additional five trials were collected.
2.5. Data Analysis
2.6. The Golden Ratio
2.7. Statistical Analysis
3. Results
3.1. Comparison of Computed Parameters before, during, and after GR Administration
3.2. Correlations before, during and after Golden Rhythm Administration
3.3. Correlations of Deltas before, during and after Golden Rhythm Administration
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dauer, W.; Przedborski, S. Parkinson’s disease: Mechanisms and models. Neuron 2003, 39, 889–909. [Google Scholar] [CrossRef]
- Jankovic, J. Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.E.; Iansek, R.; Matyas, T.A.; Summers, J.J. Stride length regulation in Parkinson’s disease: Normalization strategies and underlying mechanisms. Brain 1996, 119, 551–568. [Google Scholar] [CrossRef] [PubMed]
- Peppe, A.; Chiavalon, C.; Pasqualetti, P.; Crovato, D.; Caltagirone, C. Does gait analysis quantify motor rehabilitation efficacy in Parkinson’s disease patients? Gait Posture 2007, 26, 452–462. [Google Scholar] [CrossRef]
- Luria, A.R. The Frontal Lobes and the Regulation of Behavior; Academic Press, Inc.: Cambridge, MA, USA, 1973. [Google Scholar]
- Takahashi, H.; Takada, Y.; Nagai, N.; Urano, T.; Takada, A. Serotonergic neurons projecting to hippocampus activate locomotion. Brain Res. 2000, 869, 194–202. [Google Scholar] [CrossRef]
- Iosa, M.; Morone, G.; Fusco, A.; Marchetti, F.; Caltagirone, C.; Paolucci, S.; Peppe, A. Loss of fractal gait harmony in Parkinson’s Disease. Clin. Neurophysiol. 2016, 127, 1540–1546. [Google Scholar] [CrossRef]
- Nombela, C.; Hughes, L.E.; Owen, A.M.; Grahn, J.A. Into the groove: Can rhythm influence Parkinson’s disease? Neurosci. Biobehav. Rev. 2013, 37, 2564–2570. [Google Scholar] [CrossRef]
- Ebersbach, G.; Sojer, M.; Valldeoriola, F.; Wissel, J.; Müller, J.; Tolosa, E.; Poewe, W. Comparative analysis of gait in Parkinson’s disease, cerebellar ataxia and subcortical arteriosclerotic encephalopathy. Brain 1999, 122, 1349–1355. [Google Scholar] [CrossRef]
- Asai, Y.; Nomura, T.; Sato, S.; Tamaki, A.; Matsuo, Y.; Mizukura, I.; Abe, K. A coupled oscillator model of disordered interlimb coordination in patients with Parkinson’s disease. Biol. Cybern. 2003, 88, 152–162. [Google Scholar] [CrossRef]
- Muthukrishnan, N.; Abbas, J.J.; Shill, H.A.; Krishnamurthi, N. Cueing paradigms to improve gait and posture in parkinson’s disease: A narrative review. Sensors 2019, 19, 5468. [Google Scholar] [CrossRef]
- Thaut, M.H.; McIntosh, G.C.; Rice, R.R.; Miller, R.A.; Rathbun, J.; Brault, J.M. Rhythmic auditory stimulation in gait training for Parkinson’s disease patients. Mov. Disord. 1996, 11, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Thaut, M.H. The future of music in therapy and medicine. Ann. N. Y. Acad. Sci. 2005, 1060, 303–308. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, G.C.; Brown, S.H.; Rice, R.R.; Thaut, M.H. Rhythmic auditory-motor facilitation of gait patterns in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1997, 62, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Ashoori, A.; Eagleman, D.M.; Jankovic, J. Effects of auditory rhythm and music on gait disturbances in Parkinson’s disease. Front. Neurol. 2015, 6, 234. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Lowenthal, J.; Herman, T.; Gruendlinger, L.; Peretz, C.; Giladi, N. Rhythmic auditory stimulation modulates gait variability in Parkinson’s disease. Eur. J. Neurosci. 2007, 26, 2369–2375. [Google Scholar]
- Lim, I.; van Wegen, E.; de Goede, C.; Deutekom, M.; Nieuwboer, A.; Willems, A.; Jones, D.; Rochester, L.; Kwakkel, G. Effects of external rhythmical cueing on gait in patients with Parkinson’s disease: A systematic review. Clin. Rehabil. 2005, 19, 695–713. [Google Scholar] [CrossRef]
- Rochester, L.; Hetherington, V.; Jones, D.; Nieuwboer, A.; Willems, A.M.; Kwakkel, G.; Van Wegen, E. The effect of external rhythmic cues (auditory and visual) on walking during a functional task in homes of people with Parkinson’s disease. Arch. Phys. Med. Rehabil. 2005, 86, 999–1006. [Google Scholar] [CrossRef]
- Spaulding, S.J.; Barber, B.; Colby, M.; Cormack, B.; Mick, T.; Jenkins, M.E. Cueing and gait improvement among people with Parkinson’s disease: A meta-analysis. Arch. Phys. Med. Rehabil. 2013, 94, 562–570. [Google Scholar] [CrossRef]
- Willems, A.M.; Nieuwboer, A.; Chavret, F.; Desloovere, K.; Dom, R.; Rochester, L.; Jones, D.; Kwakkel, G.; Van Wegen, E. The use of rhythmic auditory cues to influence gait in patients with Parkinson’s disease, the differential effect for freezers and non-freezers, an explorative study. Disabil. Rehabil. 2006, 28, 721–728. [Google Scholar] [CrossRef]
- Iosa, M.; Fusco, A.; Marchetti, F.; Morone, G.; Caltagirone, C.; Paolucci, S.; Peppe, A. The golden ratio of gait harmony: Repetitive proportions of repetitive gait phases. Biomed Res. Int. 2013. [Google Scholar] [CrossRef]
- Bilney, B.; Morris, M.; Webster, K. Concurrent related validity of the GAITRite† walkway system for quantification of the spatial and temporal parameters of gait. Gait Posture 2003, 17, 68–74. [Google Scholar] [CrossRef]
- Steinert, A.; Sattler, I.; Otte, K.; Röhling, H.; Mansow-Model, S.; Müller-Werdan, U. Using new camera-based technologies for gait analysis in older adults in comparison to the established GAITrite system. Sensors 2020, 20, 125. [Google Scholar]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-Mental State: A practical method for grading the cognitive state of patients fro clinicians. J. Psychiatr. 1975, 12, 162–167. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E. Performance-Oriented Assessment of Mobility Problems in Elderly Patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef]
- Jenkinson, C.; Fitzpatrick, R.; Peto, V.; Greenhall, R.; Hyman, N. The Parkinson’s disease questionnaire (PDQ-39): Development and validation of a Parkinson’s disease summary index score. Age Ageing 1997, 26, 353–357. [Google Scholar] [CrossRef]
- Powell, L.E.; Moore, D.S.; Ellis, R.; Kosma, M.; Fabre, J.M.; McCarter, K.S.; Wood, R.H. The Activities-specific Balance Confidence ( ABC ) Scale * The Activities-specific Balance Confidence (ABC) Scale. Res. Q. Exerc. Sport 2011, 50, 545–554. [Google Scholar]
- Davis, R.B.; Õunpuu, S.; Tyburski, D.; Gage, J.R. A gait analysis data collection and reduction technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Iosa, M.; Morone, G.; Paolucci, S. Phi in physiology, psychology and biomechanics: The golden ratio between myth and science. BioSystems 2018, 165, 31–39. [Google Scholar] [CrossRef]
- Alcock, L.; Galna, B.; Lord, S.; Rochester, L. Characterisation of foot clearance during gait in people with early Parkinson׳s disease: Deficits associated with a dual task. J. Biomech. 2016, 49, 2763–2769. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age [yrs] 70.9 (8.4) | Gender 16 M,4 F | Height [cm] 167.3 (8.8) | Body Mass [kg] 69.4 (10.9) | PD Duration [yrs] 10.0 (6.2) | LD Duration [yrs] 9.4 (5.6) | |
|---|---|---|---|---|---|---|
| 1 | 83 | M | 176 | 73 | 5 | 5 |
| 2 | 63 | F | 167 | 58 | 10 | 9 |
| 3 | 72 | M | 168 | 64 | 13 | 12 |
| 4 | 78 | F | 150 | 49 | 8 | 8 |
| 5 | 59 | M | 158 | 60 | 20 | 20 |
| 6 | 67 | M | 165 | 61 | 25 | 20 |
| 7 | 63 | M | 171 | 67 | 15 | 15 |
| 8 | 77 | M | 169 | 67 | 9 | 9 |
| 9 | 53 | F | 152 | 51 | 7 | 7 |
| 10 | 69 | M | 170 | 63 | 10 | 8 |
| 11 | 64 | M | 181 | 79 | 11 | 10 |
| 12 | 70 | M | 175 | 91 | 10 | 10 |
| 13 | 83 | M | 162 | 65 | 12 | 11 |
| 14 | 71 | F | 155 | 76 | 4 | 4 |
| 15 | 68 | M | 164 | 77 | 7 | 7 |
| 16 | 76 | M | 180 | 70 | 1 | 1 |
| 17 | 79 | M | 165 | 75 | 7 | 6 |
| 18 | 85 | M | 173 | 77 | 6 | 6 |
| 19 | 65 | M | 178 | 78 | 1 | 1 |
| 20 | 67 | M | 168 | 87 | 20 | 20 |
| Clinical Scale | Range | Score |
|---|---|---|
| MDS-UPDRS (Part III) | 0–132 | 22.5 (6.7) |
| MMSE | 0–30 | 22.5 (2.2) |
| Tinetti Gait and Balance | 0–28 | 22.4 (4.7) |
| PDQ-39 | 0–100 | 34.5 (19) |
| ABC | 0–100 | 39.0 (16.0) |
| Features | Measure | Features | Measure |
|---|---|---|---|
| Stride time | s | Walking Speed | m/s |
| Stance time | s | Cadence | Steps/min |
| Stance Percentage | %stride | Width of the step | m |
| Stride length | m | Golden Ratio (ϕ) | Stride/stance |
| Swing time | s | Lateral Malleoli displacement (hMaxMalleoli) | m |
| Swing Percentage | %stride | Arm Swing (hMaxWrist) | m |
| Double support time | s | Toe Clearance second hallux (Toe Clearance) | m |
| Double support Percentage | %stride |
| T0 | T1 | T2 | |||||
|---|---|---|---|---|---|---|---|
| Golden Ratio (MA) | Golden Ratio (LA) | Golden Ratio (MA) | Golden Ratio (LA) | Golden Ratio (MA) | Golden Ratio (LA) | ||
| Age | −0.529 * | −0.402 | −0.529 * | −0.402 | −0.404 | −0.406 | |
| MDS-UPDRS | −0.213 | −0.297 | −0.213 | −0.297 | −0.373 | −0.474 * | |
| Disease duration | 0.436 | 0.449 * | 0.436 | 0.449 * | −0.006 | 0.207 | |
| Stride time | MA | −0.116 | −0.332 | −0.116 | −0.332 | −0.348 | −0.233 |
| LA | −0.209 | −0.305 | −0.209 | −0.305 | −0.498 * | −0.214 | |
| Stance Percentage | MA | −0.825 ** | −0.607 * | −0.825 ** | −0.607 ** | −0.998 ** | −0.277 |
| LA | 0.777 ** | −0.868 ** | −0.771 ** | −0.868 ** | −0.310 | −0.995 ** | |
| Swing Percentage | MA | 0.825 ** | 0.607 * | 0.825 ** | 0.607 * | 0.998 ** | 0.277 |
| LA | 0.777 ** | 0.853 ** | 0.777 ** | 0.853 ** | 0.308 | 0.995 ** | |
| Double Support Time | MA | −0.663 ** | −0.877 ** | −0.663 ** | −0.877 ** | −0.487 * | −0.794 ** |
| LA | −0.540 * | −0.421 | −0.540 * | −0.421 | −0.720 ** | −0.600 ** | |
| Step width | 0.455 * | 0.188 | 0.455 * | 0.188 | 0.606 ** | 0.358 | |
| Stride length | MA | 0.361 | 0.319 | 0.361 | 0.310 | 0.469 * | 0.191 |
| LA | 0.411 | 0.349 | 0.411 | 0.349 | 0.412 | 0.132 | |
| ϕ | MA | 1 | 0.675 ** | 0.675 ** | 1 | 1 | 0.305 |
| LA | 0.675 ** | 1 | 1 | 0.675 ** | 0.191 | 1 | |
| hMaxWrist | MA | −0.031 | −0.468 * | −0.031 | −0.468 | 0.229 | −0.111 |
| LA | −0.027 | −0.280 | −0.026 | −0.012 | −0.053 | 0.072 | |
| Walking speed | 0.324 | 0.364 | 0.324 | 0.364 | 0.564 ** | 0.275 | |
| T1-T0 | T2-T1 | T2-T0 | |||||
|---|---|---|---|---|---|---|---|
| Golden Ratio (MA) | Golden Ratio (LA) | Golden Ratio (MA) | Golden Ratio (LA) | Golden Ratio (MA) | Golden Ratio (LA) | ||
| Age | 0.467 * | −0.048 | 0.211 | 0.119 | 0.081 | 0.211 | |
| Disease duration | −0.568 ** | −0.529 ** | −0.311 | −0.117 | −0.112 | −0.231 | |
| Stride time | MA | −0.460 * | −0.295 | −0.039 | −0.229 | −0.039 | −0.229 |
| LA | −0.542 * | −0.283 | −0.229 | −0.185 | −0.229 | −0.185 | |
| Stance Percentage | MA | −0.941 ** | −0.439 | −0.630 ** | −0.278 | −0.630 ** | −0.278 |
| LA | −0.794 ** | −0.791 ** | −0.353 | −0.853 ** | −0.353 | −0.853 ** | |
| Swing Percentage | MA | 0.920 ** | 0.400 | 0.738 ** | 0.180 | 0.737 ** | 0.180 |
| LA | 0.776 ** | 0.800 ** | 0.229 | 0.869 ** | 0.259 | 0.869 ** | |
| Double Support Time | MA | −0.830 ** | −0.544 * | −0.340 | −0.797 ** | −0.340 | −0.797 ** |
| LA | −0.645 * | −0.250 | −0.317 | −0.226 | −0.317 | −0.226 | |
| Stride length | MA | 0.502 * | 0.373 | −0.197 | 0.057 | −0.197 | 0.057 |
| LA | −0.003 | 0.247 | −0.382 | −0.113 | −0.382 | −0.113 | |
| ϕ | MA | 1 | 0.582 ** | 1 | 0.266 | 1 | 0.266 |
| LA | 0.582 ** | 1 | 0.266 | 1 | 0.266 | 1 | |
| Toe Clearance | MA | −0.496 * | −0.293 | −0.354 | −0.038 | −0.354 | −0.038 |
| LA | −0.185 | 0.167 | −0.221 | 0.111 | −0.221 | −0.121 | |
| Walking speed | 0.364 | 0.307 | 0.081 | 0.621 ** | 0.081 | 0.523 ** | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belluscio, V.; Iosa, M.; Vannozzi, G.; Paravati, S.; Peppe, A. Auditory Cue Based on the Golden Ratio Can Improve Gait Patterns in People with Parkinson’s Disease. Sensors 2021, 21, 911. https://doi.org/10.3390/s21030911
Belluscio V, Iosa M, Vannozzi G, Paravati S, Peppe A. Auditory Cue Based on the Golden Ratio Can Improve Gait Patterns in People with Parkinson’s Disease. Sensors. 2021; 21(3):911. https://doi.org/10.3390/s21030911
Chicago/Turabian StyleBelluscio, Valeria, Marco Iosa, Giuseppe Vannozzi, Stefano Paravati, and Antonella Peppe. 2021. "Auditory Cue Based on the Golden Ratio Can Improve Gait Patterns in People with Parkinson’s Disease" Sensors 21, no. 3: 911. https://doi.org/10.3390/s21030911
APA StyleBelluscio, V., Iosa, M., Vannozzi, G., Paravati, S., & Peppe, A. (2021). Auditory Cue Based on the Golden Ratio Can Improve Gait Patterns in People with Parkinson’s Disease. Sensors, 21(3), 911. https://doi.org/10.3390/s21030911