Closed-Loop Temperature Control Based on Fiber Bragg Grating Sensors for Laser Ablation of Hepatic Tissue



 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
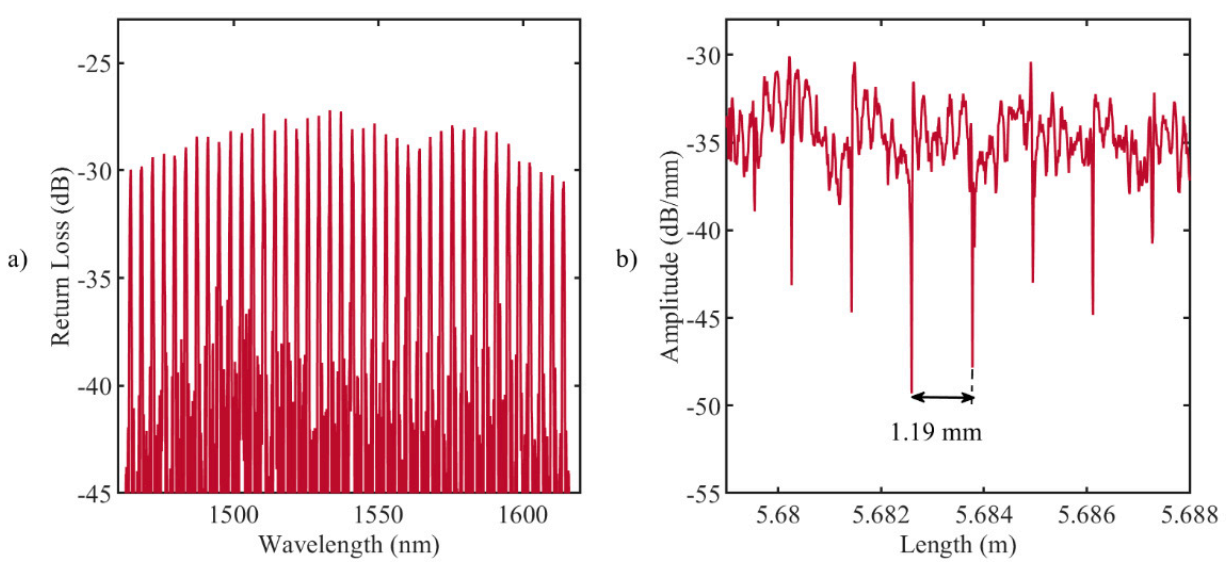
2.1. FBG-Based Sensing
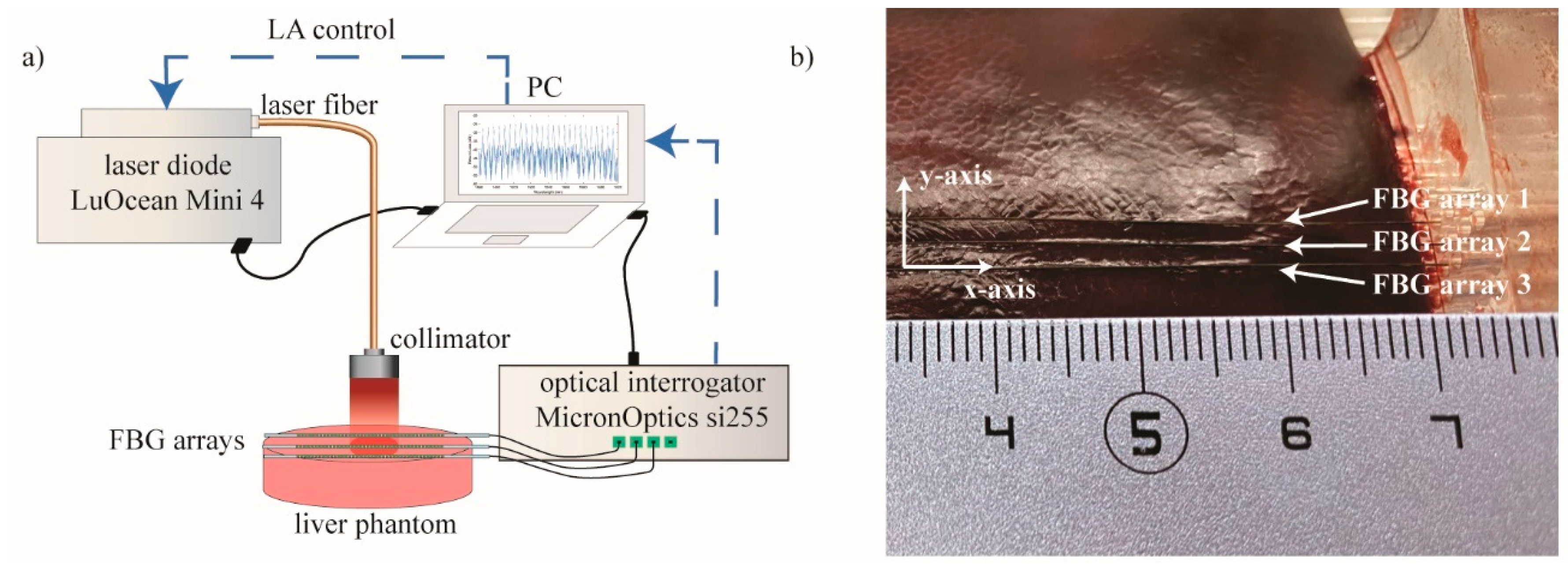
2.2. Experimental Setup
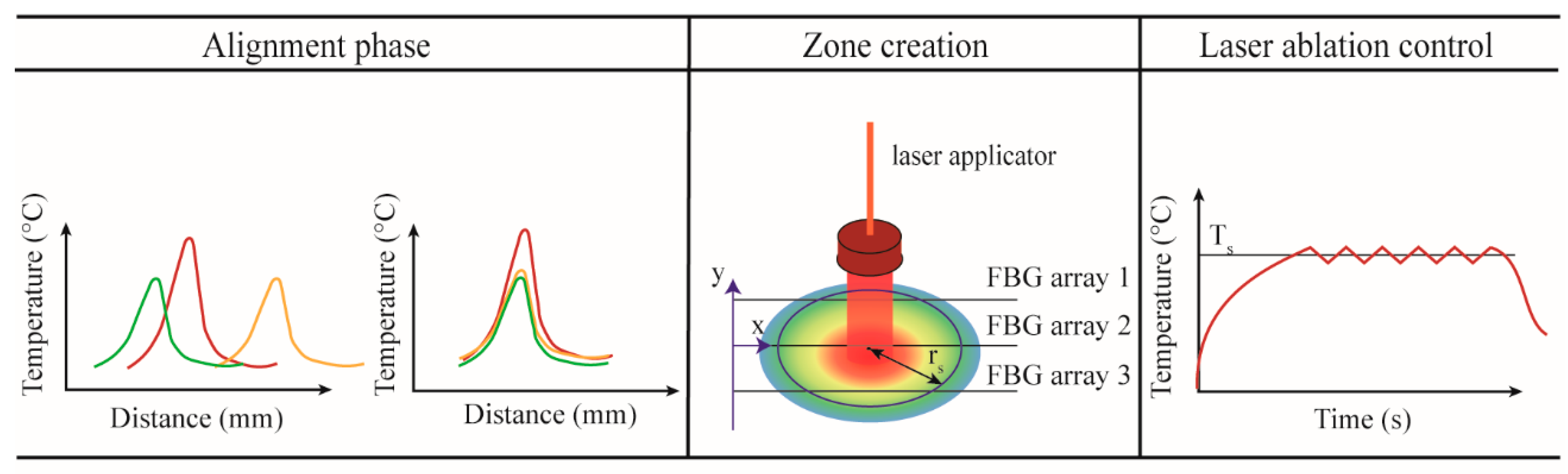
2.3. Temperature-Feedback Control Strategy for the Zone Control Logic
3. Results
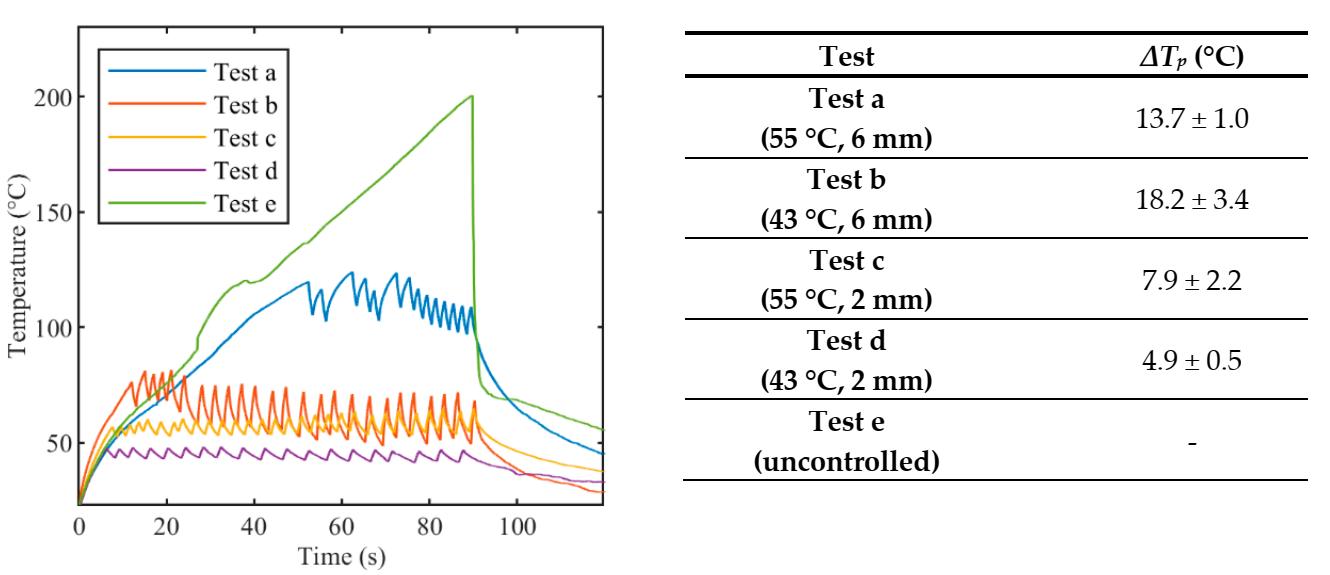
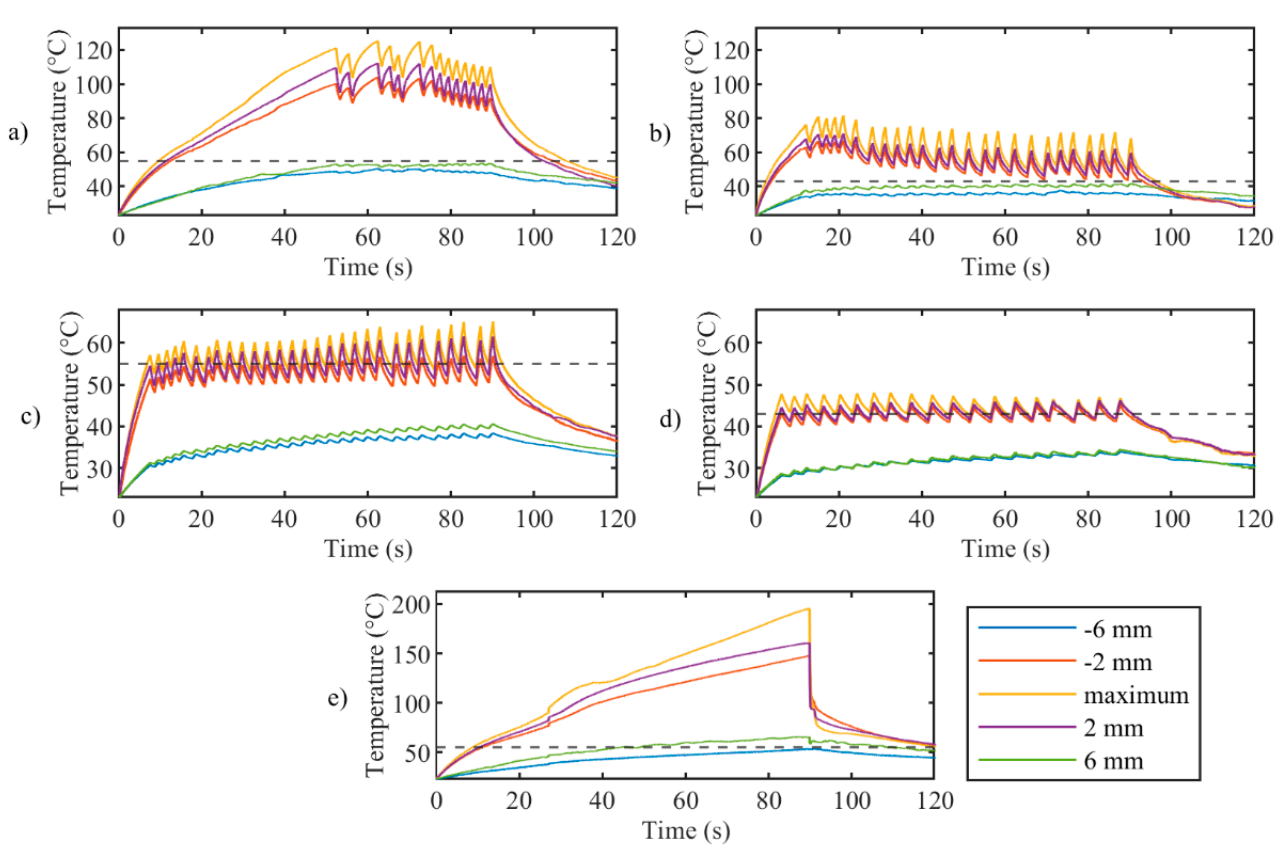
3.1. Thermal Analyses on the Temperature Profiles Measured by FBG Array 2
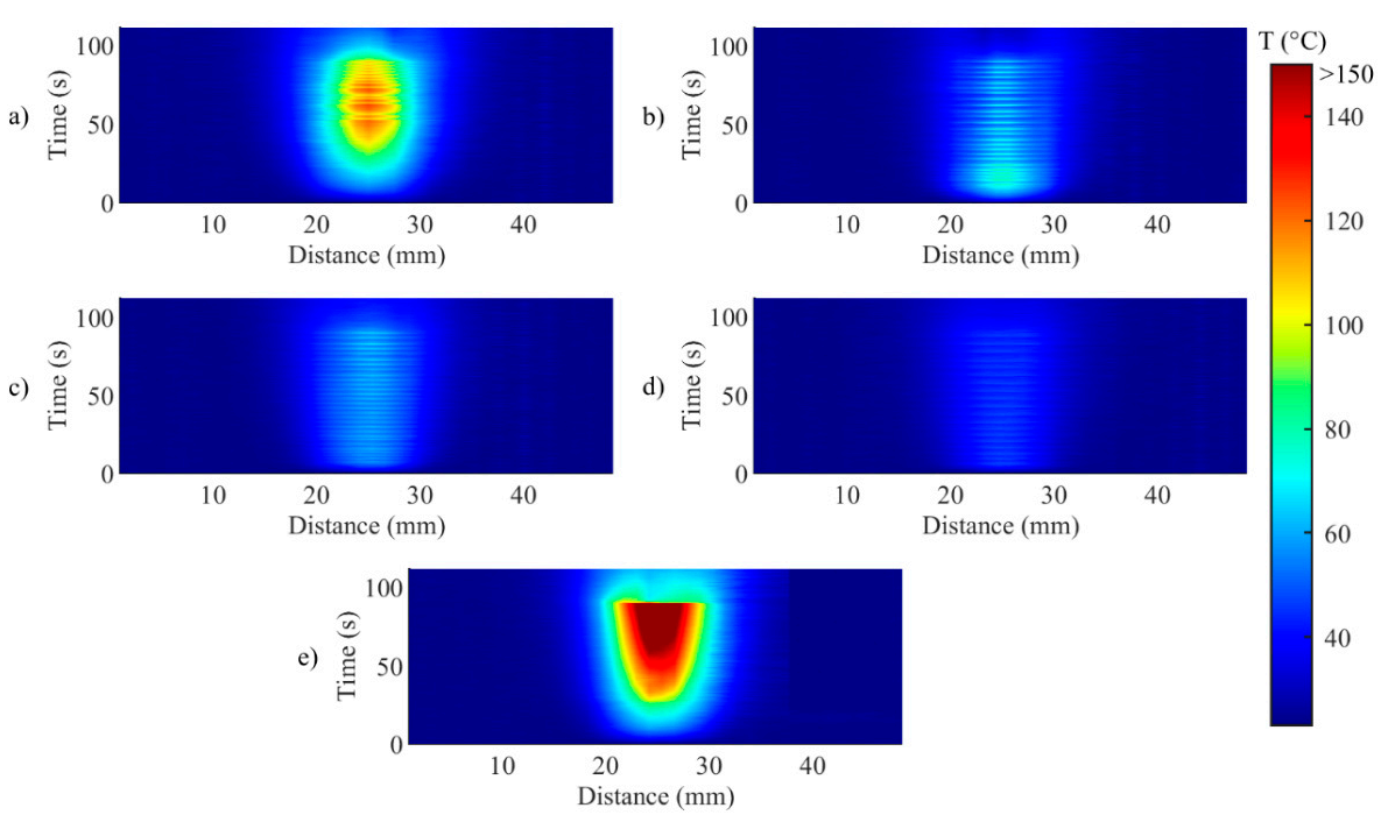
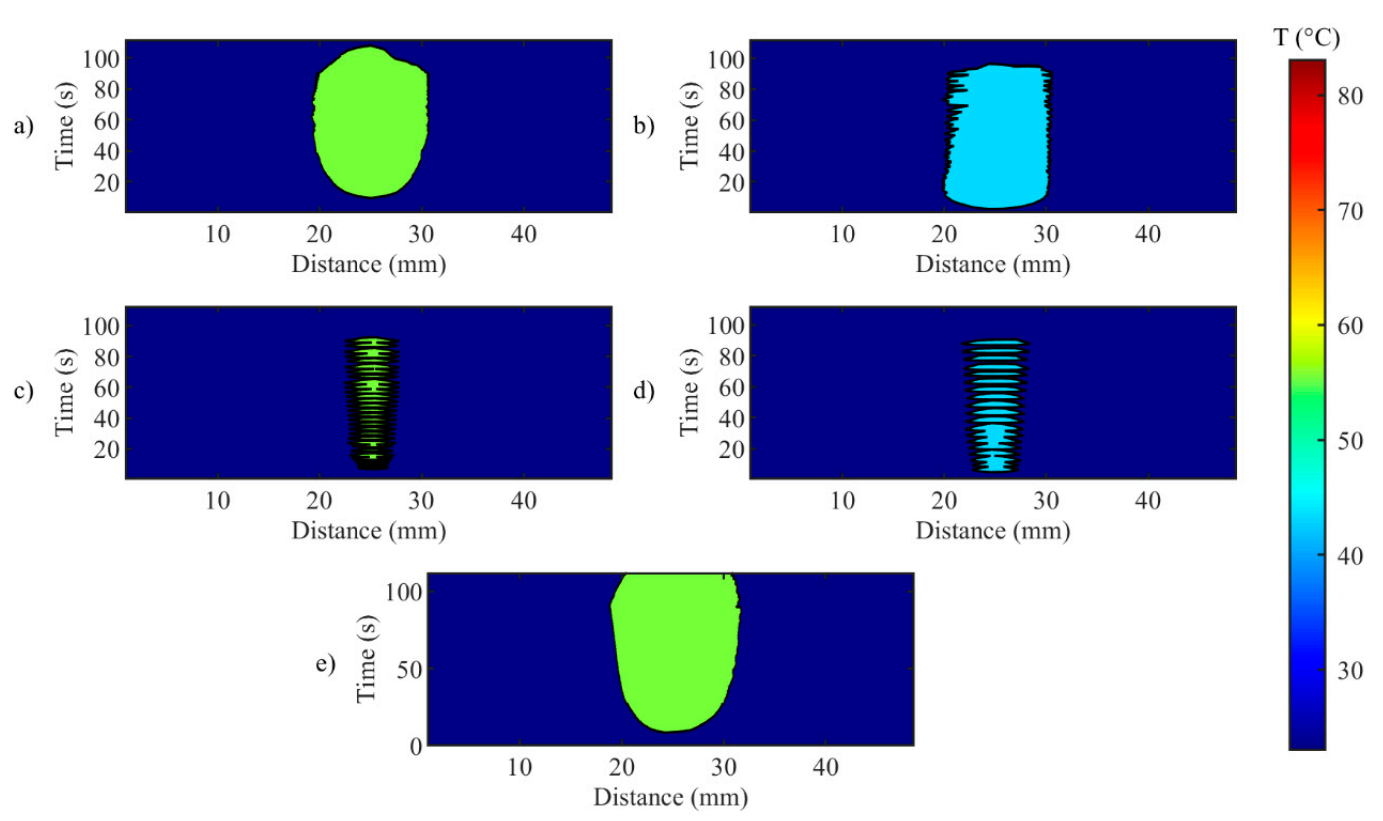
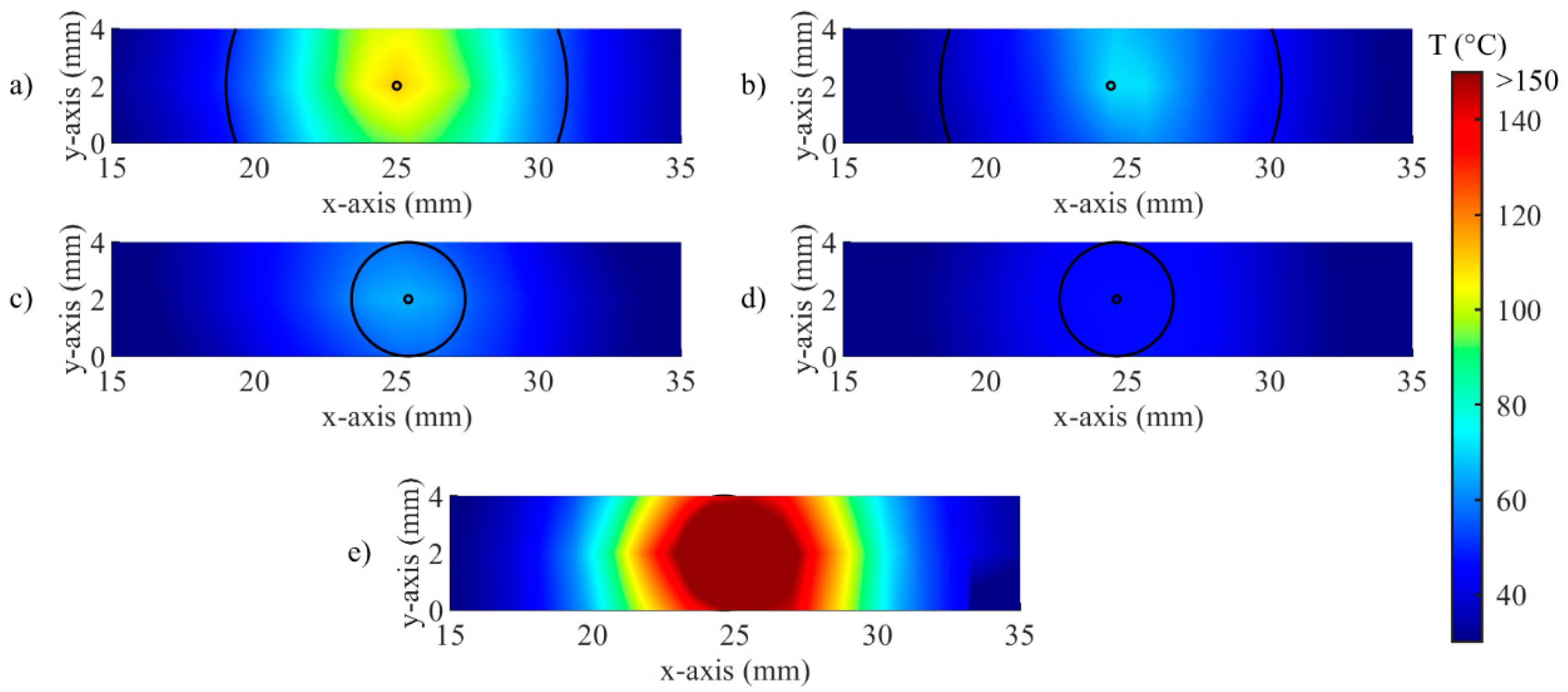
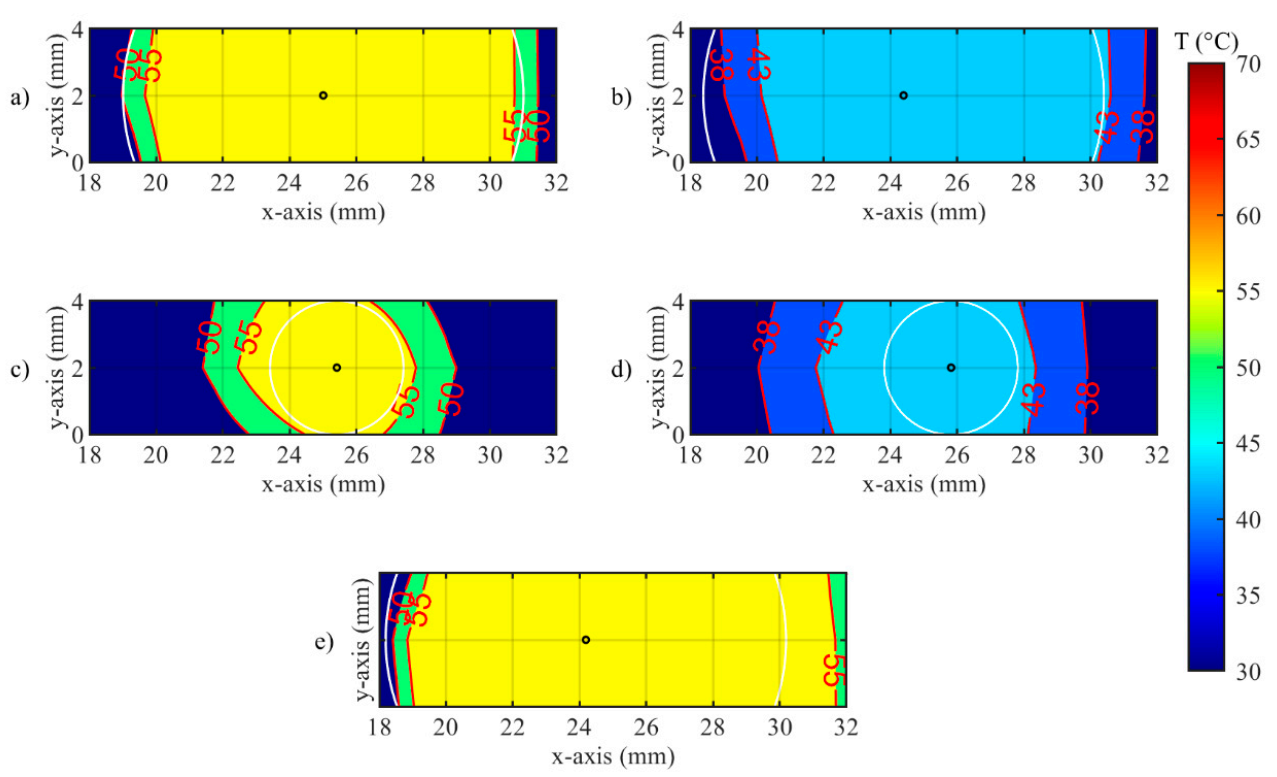
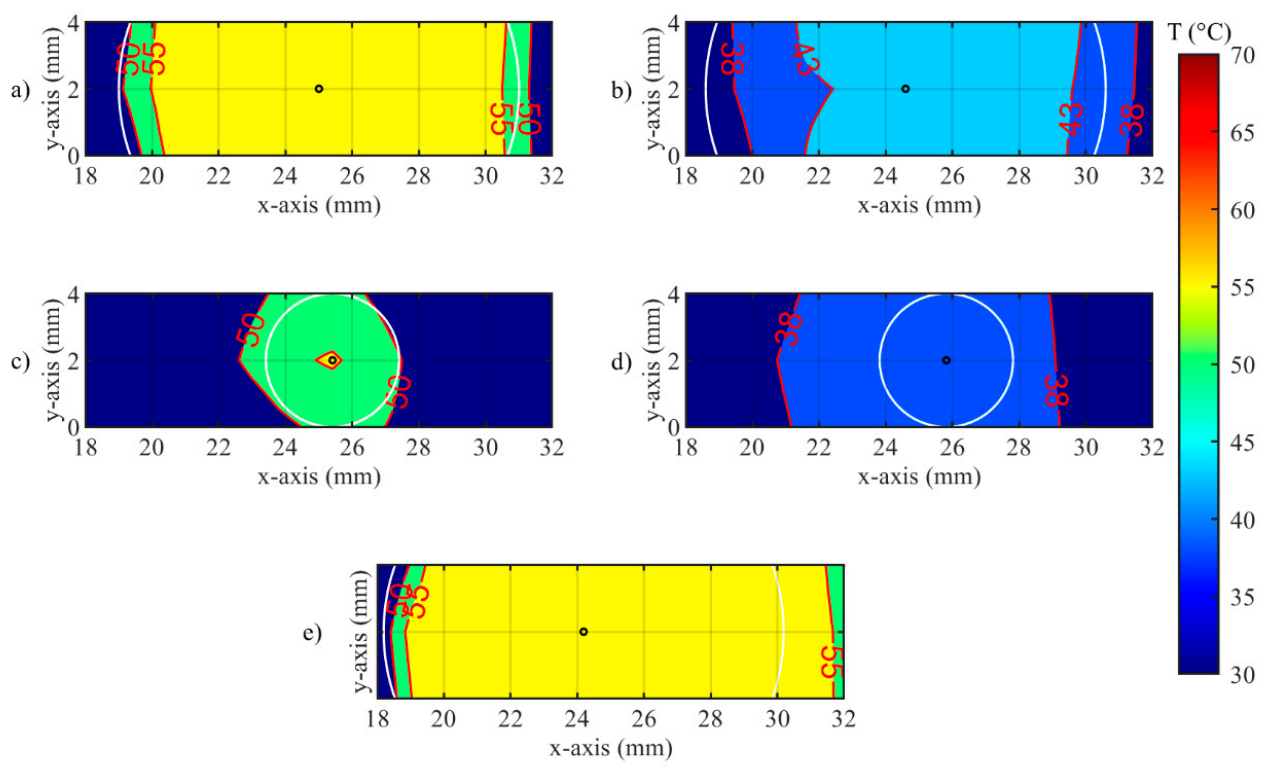
3.2. Thermal Analyses on the Spatial Temperature Distribution
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sartori, S.; Di Vece, F.; Ermili, F.; Tombesi, P. Laser Ablation of Liver Tumors: An Ancillary Technique, or an Alternative to Radiofrequency and Microwave? World J. Radiol. 2017, 9, 91. [Google Scholar] [CrossRef] [PubMed]
- Brace, C.L. Radiofrequency and Microwave Ablation of the Liver, Lung, Kidney, and Bone: What Are the Differences? Curr. Probl. Diagn. Radiol. 2009, 38, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Chu, K.F.; Dupuy, D.E. Thermal Ablation of Tumours: Biological Mechanisms and Advances in Therapy. Nat. Rev. Cancer 2014, 14, 199. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Brace, C.L.; Lee, F.T., Jr.; Goldberg, S.N. Principles of and Advances in Percutaneous Ablation. Radiology 2011, 258, 351–369. [Google Scholar] [CrossRef] [PubMed]
- Di Matteo, F.M.; Saccomandi, P.; Martino, M.; Pandolfi, M.; Pizzicannella, M.; Balassone, V.; Schena, E.; Pacella, C.M.; Silvestri, S.; Costamagna, G. Feasibility of EUS-Guided Nd:YAG Laser Ablation of Unresectable Pancreatic Adenocarcinoma. Gastrointest. Endosc. 2018, 88, 168–174.e1. [Google Scholar] [CrossRef]
- Zhou, Y.-F. High Intensity Focused Ultrasound in Clinical Tumor Ablation. World J. Clin. Oncol. 2011, 2, 8. [Google Scholar] [CrossRef]
- Lubner, M.G.; Brace, C.L.; Hinshaw, J.L.; Lee, F.T., Jr. Microwave Tumor Ablation: Mechanism of Action, Clinical Results, and Devices. J. Vasc. Interv. Radiol. 2010, 21, S192–S203. [Google Scholar] [CrossRef]
- Goldberg, S.N. Radiofrequency Tumor Ablation: Principles and Techniques. In Multi-Treatment Modalities of Liver Tumours; Springer: Boston, MA, USA, 2002; pp. 87–118. [Google Scholar]
- Stafford, R.J.; Fuentes, D.; Elliott, A.A.; Weinberg, J.S.; Ahrar, K. Laser-Induced Thermal Therapy for Tumor Ablation. Crit. Rev. Biomed. Eng. 2010, 38, 79–100. [Google Scholar] [CrossRef]
- Schena, E.; Saccomandi, P.; Fong, Y. Laser Ablation for Cancer: Past, Present and Future. J. Funct. Biomater. 2017, 8, 19. [Google Scholar] [CrossRef]
- Tozburun, S. Superficial Photothermal Laser Ablation of Ex Vivo Sheep Esophagus Using a Cone-shaped Optical Fiber Tip. J. Biophotonics 2020, 13, e201960116. [Google Scholar] [CrossRef]
- Quero, G.; Saccomandi, P.; Kwak, J.-M.; Dallemagne, B.; Costamagna, G.; Marescaux, J.; Mutter, D.; Diana, M. Modular Laser-Based Endoluminal Ablation of the Gastrointestinal Tract: In Vivo Dose–Effect Evaluation and Predictive Numerical Model. Surg. Endosc. 2019, 33, 3200–3208. [Google Scholar] [CrossRef] [PubMed]
- Saccomandi, P.; Quero, G.; Gassino, R.; Lapergola, A.; Guerriero, L.; Diana, M.; Vallan, A.; Perrone, G.; Schena, E.; Costamagna, G.; et al. Laser Ablation of the Biliary Tree: In Vivo Proof of Concept as Potential Treatment of Unresectable Cholangiocarcinoma. Int. J. Hyperth. 2018, 34, 1372–1380. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Choi, J.; Bang, D.; Kim, E.; Lim, E.-K.; Park, H.; Suh, J.-S.; Lee, K.; Yoo, K.-H.; Kim, E.-K.; et al. Convertible Organic Nanoparticles for Near-Infrared Photothermal Ablation of Cancer Cells. Angew. Chem. Int. Ed. 2011, 50, 441–444. [Google Scholar] [CrossRef] [PubMed]
- Asadi, S.; Bianchi, L.; De Landro, M.; Korganbayev, S.; Schena, E.; Saccomandi, P. Laser-Induced Optothermal Response of Gold Nanoparticles: From a Physical Viewpoint to Cancer Treatment Application. J. Biophotonics 2020, e202000161. [Google Scholar] [CrossRef]
- Gangi, A.; Alizadeh, H.; Wong, L.; Buy, X.; Dietemann, J.-L.; Roy, C. Osteoid Osteoma: Percutaneous Laser Ablation and Follow-up in 114 Patients. Radiology 2007, 242, 293–301. [Google Scholar] [CrossRef]
- Schwarzmaier, H.-J.; Eickmeyer, F.; von Tempelhoff, W.; Fiedler, V.U.; Niehoff, H.; Ulrich, S.D.; Yang, Q.; Ulrich, F. MR-Guided Laser-Induced Interstitial Thermotherapy of Recurrent Glioblastoma Multiforme: Preliminary Results in 16 Patients. Eur. J. Radiol. 2006, 59, 208–215. [Google Scholar] [CrossRef]
- Pacella, C.M.; Bizzarri, G.; Guglielmi, R.; Anelli, V.; Bianchini, A.; Crescenzi, A.; Pacella, S.; Papini, E. Thyroid Tissue: US-Guided Percutaneous Interstitial Laser Ablation—A Feasibility Study. Radiology 2000, 217, 673–677. [Google Scholar] [CrossRef]
- Vogl, T.J.; Straub, R.; Eichler, K.; Söllner, O.; Mack, M.G. Colorectal Carcinoma Metastases in Liver: Laser-Induced Interstitial Thermotherapy—Local Tumor Control Rate and Survival Data. Radiology 2004, 230, 450–458. [Google Scholar] [CrossRef]
- Di Matteo, F.; Martino, M.; Rea, R.; Pandolfi, M.; Rabitti, C.; Masselli, G.M.P.; Silvestri, S.; Pacella, C.M.; Papini, E.; Panzera, F. EUS-Guided Nd: YAG Laser Ablation of Normal Pancreatic Tissue: A Pilot Study in a Pig Model. Gastrointest. Endosc. 2010, 72, 358–363. [Google Scholar] [CrossRef]
- Saccomandi, P.; Schena, E.; Caponero, M.A.; Di Matteo, F.M.; Martino, M.; Pandolfi, M.; Silvestri, S. Theoretical Analysis and Experimental Evaluation of Laser-Induced Interstitial Thermotherapy in Ex Vivo Porcine Pancreas. IEEE Trans. Biomed. Eng. 2012, 59, 2958–2964. [Google Scholar] [CrossRef]
- Saccomandi, P.; Lapergola, A.; Longo, F.; Schena, E.; Quero, G. Thermal Ablation of Pancreatic Cancer: A Systematic Literature Review of Clinical Practice and Pre-Clinical Studies. Int. J. Hyperth. 2018, 35, 398–418. [Google Scholar] [CrossRef] [PubMed]
- Welch, A.J.; Van Gemert, M.J.C. Optical-Thermal Response of Laser-Irradiated Tissue; Welch, A.J., Van Gemert, M.J.C., Eds.; Springer: Dordrecht, The Netherlands, 2011. [Google Scholar] [CrossRef]
- Brace, C. Thermal Tumor Ablation in Clinical Use. IEEE Pulse 2011, 2, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Nomura, S.; Arake, M.; Morimoto, Y.; Tsujimoto, H.; Miyazaki, H.; Saitoh, D.; Shinomiya, N.; Hase, K.; Yamamoto, J.; Ueno, H. Thermal Sensor Circuit Using Thermography for Temperature-Controlled Laser Hyperthermia. J. Sens. 2017, 2017, 1–7. [Google Scholar] [CrossRef]
- Wheatley, D.N.; Kerr, C.; Gregory, D.W. Heat-Induced Damage to HeLa-S3 Cells: Correlation of Viability, Permeability, Osmosensitivity, Phase-Contrast Light-, Scanning Electron- and Transmission Electron-Microscopical Findings. Int. J. Hyperth. 1989, 5, 145–162. [Google Scholar] [CrossRef] [PubMed]
- Yarmolenko, P.S.; Moon, E.J.; Landon, C.; Manzoor, A.; Hochman, D.W.; Viglianti, B.L.; Dewhirst, M.W. Thresholds for Thermal Damage to Normal Tissues: An Update. Int. J. Hyperth. 2011, 27, 320–343. [Google Scholar] [CrossRef] [PubMed]
- Ivarsson, K.; Olsrud, J.; Sturesson, C. Feedback Interstitial Diode Laser (805 Nm) Thermotherapy System: Ex Vivo Evaluation and Mathematical Modeling With One and Four-Fibers. Lasers Surg. Med. 1998, 22, 86–96. [Google Scholar] [CrossRef]
- Möller, P.H.; Lindberg, L.; Henriksson, P.H.; Persson, B.R.; Tranberg, K.G. Temperature Control and Light Penetration in a Feedback Interstitial Laser Thermotherapy System. Int. J. Hyperth. 1996, 12, 49–63. [Google Scholar] [CrossRef]
- Wohlgemuth, W.A.; Wamser, È.; Reiss, T.; Wagner, T. In Vivo Laser-Induced Interstitial Thermotherapy of Pig Liver With a Temperature-Controlled Diode Laser and MRI Correlation. Lasers Surg. Med. 2001, 29, 374–378. [Google Scholar] [CrossRef]
- Lin, J.T.; Chiang, Y.S.; Lin, G.H.; Lee, H.; Liu, H.W. In Vitro Photothermal Destruction of Cancer Cells Using Gold Nanorods and Pulsed-Train near-Infrared Laser. J. Nanomater. 2012, 2012, 1385. [Google Scholar] [CrossRef]
- Lin, J.; Hong, Y.; Chang, C. Selective Cancer Therapy via IR-Laser-Excited Gold Nanorods. In Optical Interactions with Tissues and Cells XXI; Jansen, E.D., Thomas, R.J., Eds.; International Society for Optics and Photonics: San Francisco, CA, USA, 2010; Volume 7562, p. 75620R. [Google Scholar] [CrossRef]
- Saccomandi, P.; Schena, E.; Silvestri, S. Techniques for Temperature Monitoring during Laser-Induced Thermotherapy: An Overview. Int. J. Hyperth. 2013, 29, 609–619. [Google Scholar] [CrossRef]
- Manns, F.; Milne, P.J.; Gonzalez-Cirre, X.; Denham, D.B.; Parel, J.; Robinson, D.S. In Situ Temperature Measurements with Thermocouple Probes during Laser Interstitial Thermotherapy (LITT): Quantification and Correction of a Measurement Artifact. Lasers Surg. Med. Off. J. Am. Soc. Laser Med. Surg. 1998, 23, 94–103. [Google Scholar] [CrossRef]
- Schena, E.; Tosi, D.; Saccomandi, P.; Lewis, E.; Kim, T. Fiber Optic Sensors for Temperature Monitoring during Thermal Treatments: An Overview. Sensors 2016, 16, 1144. [Google Scholar] [CrossRef] [PubMed]
- Morra, F.; De Landro, M.; Korganbayev, S.; Wolf, A.; Dostovalov, A.; Cigada, A.; Saccomandi, P. Spatially Resolved Thermometry during Laser Ablation in Tissues: Distributed and Quasi-Distributed Fiber Optic-Based Sensing. Opt. Fiber Technol. 2020, 58, 102295. [Google Scholar] [CrossRef]
- Macchi, E.G.; Tosi, D.; Braschi, G.; Gallati, M.; Cigada, A.; Busca, G.; Lewis, E. Optical Fiber Sensors-Based Temperature Distribution Measurement in Ex Vivo Radiofrequency Ablation with Submillimeter Resolution. J. Biomed. Opt. 2014, 19, 117004. [Google Scholar] [CrossRef] [PubMed]
- Beccaria, A.; Bellone, A.; Mirigaldi, A.; Serafini, V.; Olivero, M.; Vallan, A.; Perrone, G. Temperature Monitoring of Tumor Hyperthermal Treatments with Optical Fibers: Comparison of Distributed and Quasi-Distributed Techniques. Opt. Fiber Technol. 2020, 60, 102340. [Google Scholar] [CrossRef]
- Erdogan, T. Fiber Grating Spectra. J. Light. Technol. 1997, 15, 1277–1294. [Google Scholar] [CrossRef]
- Lee, K.K.C.; Mariampillai, A.; Haque, M.; Standish, B.A.; Yang, V.X.D.; Herman, P.R. Temperature-Compensated Fiber-Optic 3D Shape Sensor Based on Femtosecond Laser Direct-Written Bragg Grating Waveguides. Opt. Express 2013, 21, 24076–24086. [Google Scholar] [CrossRef]
- Ashikbayeva, Z.; Aitkulov, A.; Jelbuldina, M.; Issatayeva, A.; Beisenova, A.; Molardi, C.; Saccomandi, P.; Blanc, W.; Inglezakis, V.J.; Tosi, D. Distributed 2D Temperature Sensing during Nanoparticles Assisted Laser Ablation by Means of High-Scattering Fiber Sensors. Sci. Rep. 2020, 10, 12593. [Google Scholar] [CrossRef]
- Chen, W.; Gassino, R.; Liu, Y.; Carullo, A.; Perrone, G.; Vallan, A.; Tosi, D. Performance Assessment of FBG Temperature Sensors for Laser Ablation of Tumors. In Proceedings of the 2015 IEEE International Symposium on Medical Measurements and Applications (MeMeA) Proceedings, Turin, Italy, 7–9 May 2015; pp. 324–328. [Google Scholar]
- Gassino, R.; Liu, Y.; Konstantaki, M.; Vallan, A.; Pissadakis, S.; Perrone, G. A Fiber Optic Probe for Tumor Laser Ablation With Integrated Temperature Measurement Capability. J. Light. Technol. 2017, 35, 3447–3454. [Google Scholar] [CrossRef]
- Saccomandi, P.; Schena, E.; Di Matteo, F.M.; Pandolfi, M.; Martino, M.; Rea, R.; Silvestri, S. Laser Interstitial Thermotherapy for Pancreatic Tumor Ablation: Theoretical Model and Experimental Validation. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Boston, MA, USA, 30 August–3 September 2011. [Google Scholar] [CrossRef]
- De Vita, E.; De Landro, M.; Massaroni, C.; Iadicicco, A.; Saccomandi, P.; Schena, E.; Campopiano, S. Fiber Optic Sensors-Based Thermal Analysis of Perfusion-Mediated Tissue Cooling in Liver Undergoing Laser Ablation. IEEE Trans. Biomed. Eng. 2020, 1. [Google Scholar] [CrossRef]
- Dostovalov, A.V.; Wolf, A.A.; Parygin, A.V.; Zyubin, V.E.; Babin, S.A. Femtosecond Point-by-Point Inscription of Bragg Gratings by Drawing a Coated Fiber through Ferrule. Opt. Express 2016, 24, 16232–16237. [Google Scholar] [CrossRef] [PubMed]
- Gratten, K.T.V.; Meggitt, B.T. Optical Fiber Sensor Technology: Volume 3: Applications and Systems; Springer: Boston, MA, USA, 1999; Volume 3. [Google Scholar]
- Huang, L.; Dyer, R.S.; Lago, R.J.; Stolov, A.A.; Li, J. Mechanical Properties of Polyimide Coated Optical Fibers at Elevated Temperatures. In Optical Fibers and Sensors for Medical Diagnostics and Treatment Applications XVI; Gannot, I., Ed.; International Society for Optics and Photonics: San Francisco, CA, USA, 2016; p. 97020Y. [Google Scholar] [CrossRef]
- Othonos, A.; Kalli, K.; Kohnke, G.E. Fiber Bragg Gratings: Fundamentals and Applications in Telecommunications and Sensing. Phys. Today 2000, 53, 61. [Google Scholar] [CrossRef]
- Brinkmann, R.; Hansen, C.; Mohrenstecher, D.; Scheu, M.; Birngruber, R. Analysis of Cavitation Dynamics during Pulsed Laser Tissue Ablation by Optical On-Line Monitoring. IEEE J. Sel. Top. Quantum Electron. 1996, 2, 826–835. [Google Scholar] [CrossRef]
- Korganbayev, S.; Pini, R.; Orrico, A.; Wolf, A.; Dostovalov, A.; Saccomandi, P. Towards Temperature-Controlled Laser Ablation Based on Fiber Bragg Grating Array Temperature Measurements. In Proceedings of the 2020 IEEE International Workshop on Metrology for Industry 4.0 & IoT, Roma, Italy, 3–5 June 2020; pp. 268–272. [Google Scholar]
- Thomsen, S. Pathologic Analysis of Photothermal and Photomechanical Effects of Laser-Tissue Interactions. Photochem. Photobiol. 1991, 53, 825–835. [Google Scholar] [CrossRef]
- Nagarajan, V.K.; Ward, J.M.; Yu, B. Association of Liver Tissue Optical Properties and Thermal Damage. Lasers Surg. Med. 2020, 52, 779–787. [Google Scholar] [CrossRef]
- Nguyen, T.H.; Park, S.; Hlaing, K.K.; Kang, H.W. Temperature Feedback-Controlled Photothermal Treatment with Diffusing Applicator: Theoretical and Experimental Evaluations. Biomed. Opt. Express 2016, 7, 1932. [Google Scholar] [CrossRef]
- Sun, L.; Collins, C.M.; Schiano, J.L.; Smith, M.B.; Smith, N.B. Adaptive Real-Time Closed-Loop Temperature Control for Ultrasound Hyperthermia Using Magnetic Resonance Thermometry. Concepts Magn. Reson. Part B Magn. Reson. Eng. 2005, 27B, 51–63. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
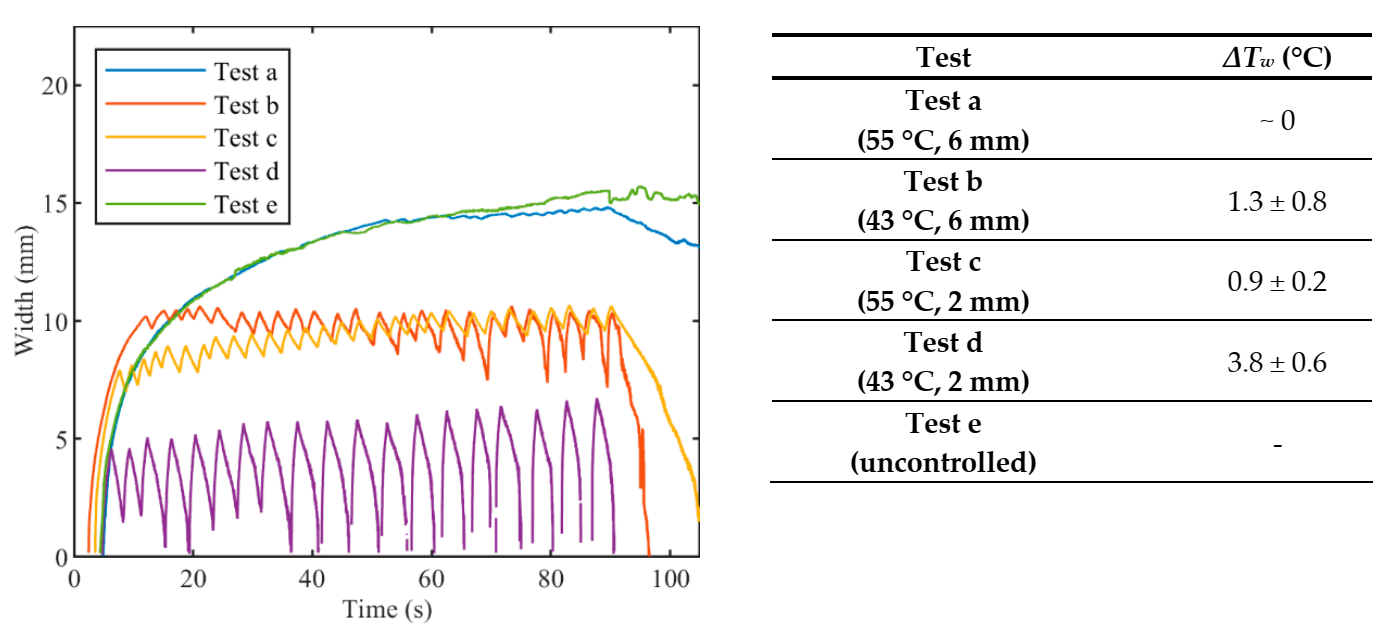
| Setting | Test a | Test b | Test c | Test d | Test e |
|---|---|---|---|---|---|
| 55 | 43 | 55 | 43 | uncontrolled | |
| rS (mm) | 6 | 6 | 2 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korganbayev, S.; Orrico, A.; Bianchi, L.; De Landro, M.; Wolf, A.; Dostovalov, A.; Saccomandi, P. Closed-Loop Temperature Control Based on Fiber Bragg Grating Sensors for Laser Ablation of Hepatic Tissue. Sensors 2020, 20, 6496. https://doi.org/10.3390/s20226496
Korganbayev S, Orrico A, Bianchi L, De Landro M, Wolf A, Dostovalov A, Saccomandi P. Closed-Loop Temperature Control Based on Fiber Bragg Grating Sensors for Laser Ablation of Hepatic Tissue. Sensors. 2020; 20(22):6496. https://doi.org/10.3390/s20226496
Chicago/Turabian StyleKorganbayev, Sanzhar, Annalisa Orrico, Leonardo Bianchi, Martina De Landro, Alexey Wolf, Alexander Dostovalov, and Paola Saccomandi. 2020. "Closed-Loop Temperature Control Based on Fiber Bragg Grating Sensors for Laser Ablation of Hepatic Tissue" Sensors 20, no. 22: 6496. https://doi.org/10.3390/s20226496
APA StyleKorganbayev, S., Orrico, A., Bianchi, L., De Landro, M., Wolf, A., Dostovalov, A., & Saccomandi, P. (2020). Closed-Loop Temperature Control Based on Fiber Bragg Grating Sensors for Laser Ablation of Hepatic Tissue. Sensors, 20(22), 6496. https://doi.org/10.3390/s20226496