

The Alarmin Triad—IL-25, IL-33, and TSLP—Serum Levels and Their Clinical Implications in Chronic Spontaneous Urticaria
 , ,
, ,  and
and 
Abstract
1. Introduction
2. Results
2.1. Collection and Presentation of Clinical and Paraclinical Data
2.2. Serum Alarmin Levels and ROC Analysis in CSU Patients versus Controls
2.2.1. Analysis of IL-25, IL-33, and TSLP Serum Levels in CSU Patients and Healthy Controls
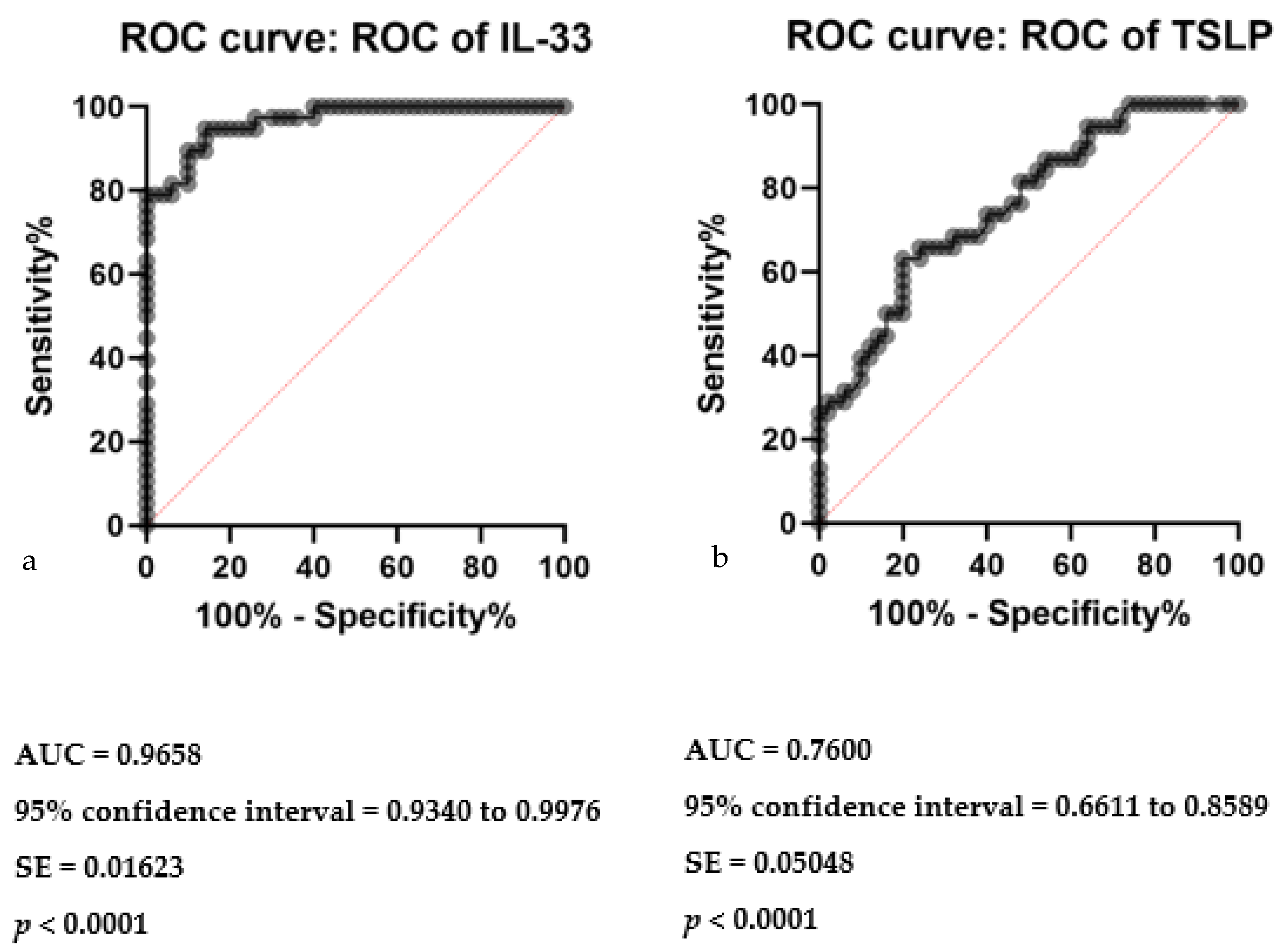
2.2.2. Diagnostic Performance of Serum Alarmins in CSU: ROC Curve Assessment
2.3. Inter-Alarmin Correlations in Serum
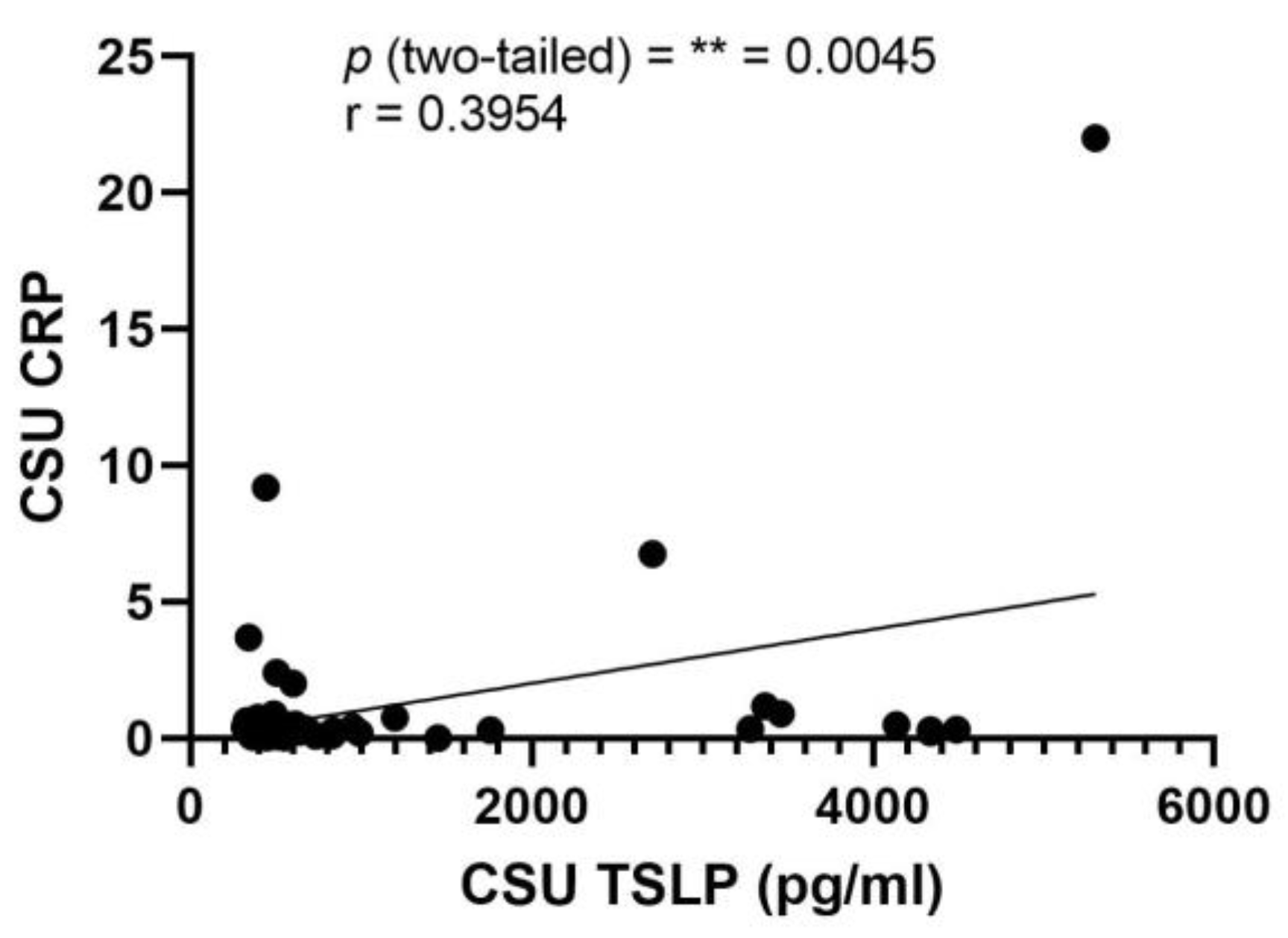
2.4. Correlation Analysis of Serum Alarmin Levels with Inflammatory Markers in CSU
2.5. Correlation between Clinical Tools (UAS7 and DLQI) in CSU
2.6. Correlation between Serum Alarmin Levels and UAS7 in CSU
2.6.1. Analysis of Serum IL-25 and TSLP Levels and Their Correlation with UAS7
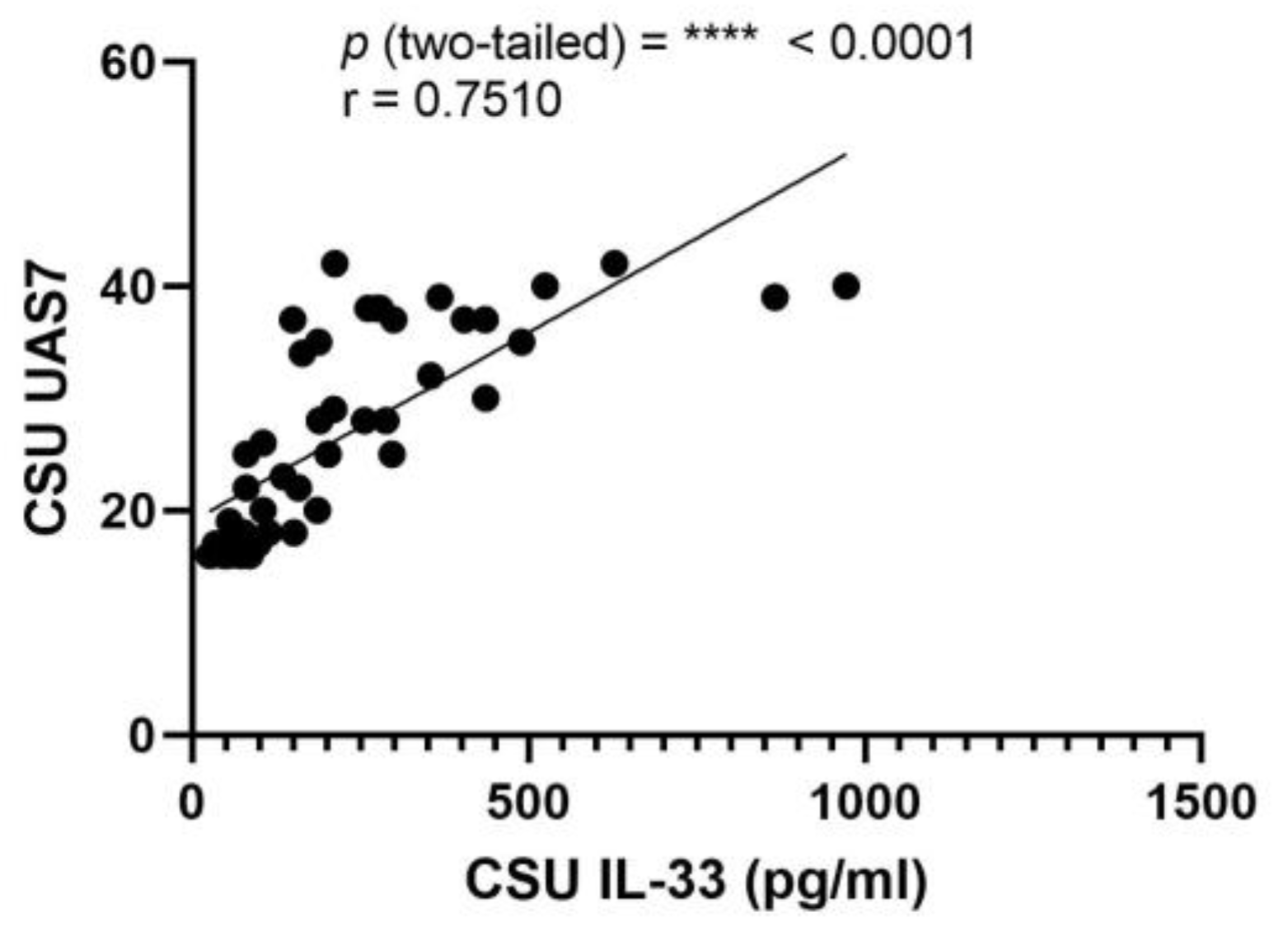
2.6.2. Analysis of Serum IL-33 Levels and Their Correlation with UAS7
2.7. Correlation between Serum Alarmin Levels and DLQI in CSU
2.7.1. Analysis of Serum IL-25 and TSLP Levels and Their Correlation with DLQI
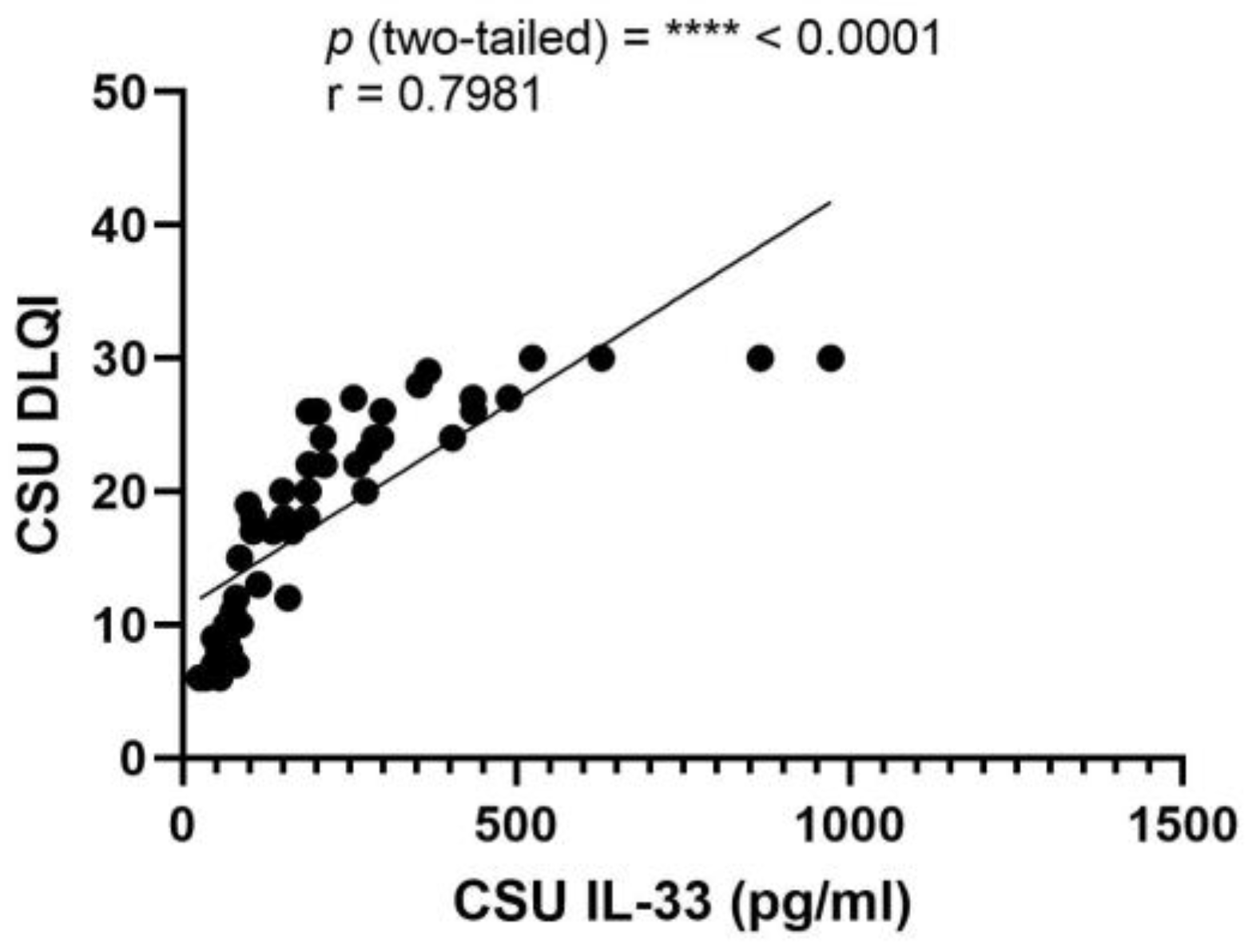
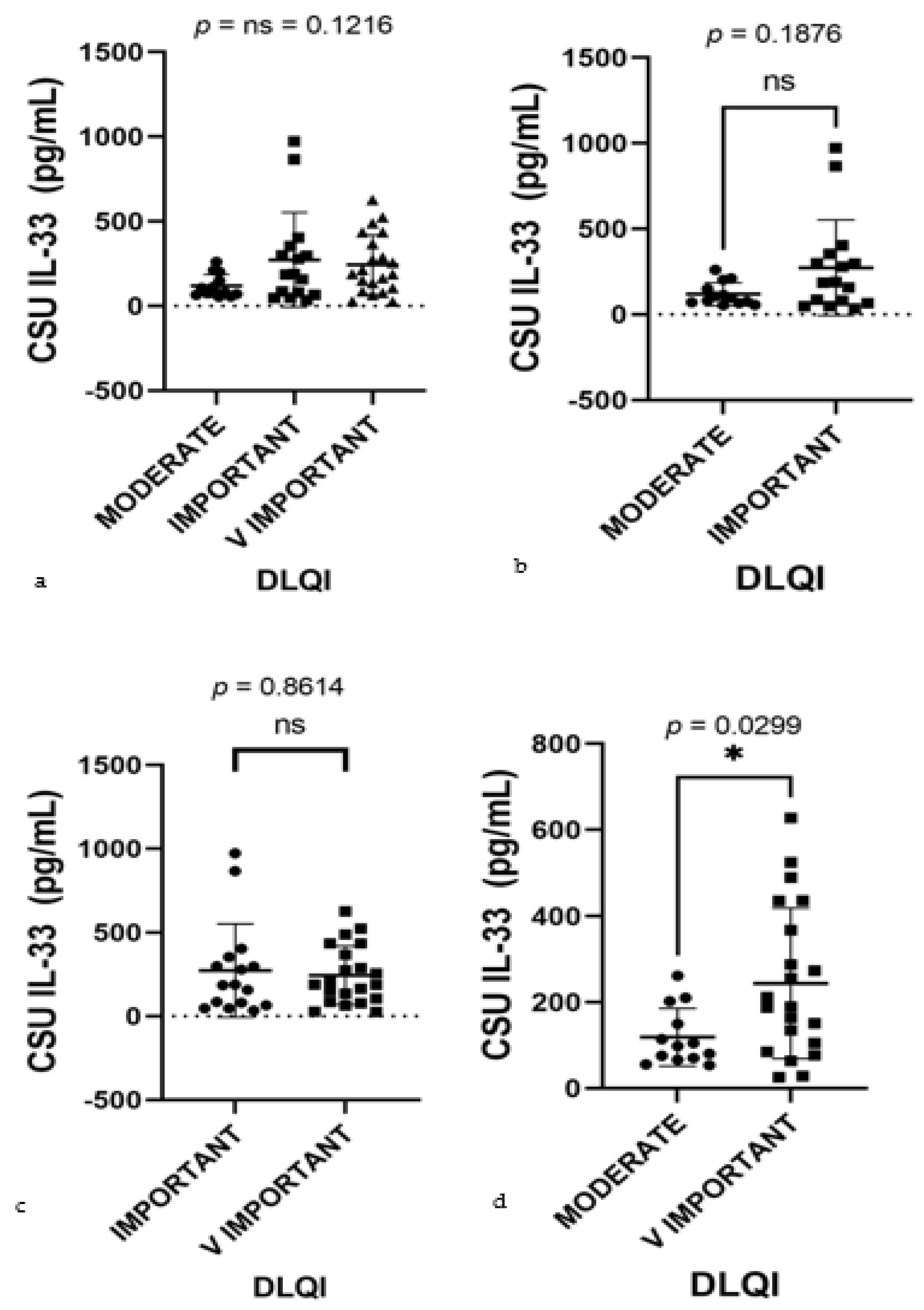
2.7.2. Analysis of Serum IL-33 Levels and Their Correlation with DLQI
3. Discussion
Strengths and Limitations
4. Materials and Methods
Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zuberbier, T.; Latiff, A.H.A.; Abuzakouk, M.; Aquilina, S.; Asero, R.; Baker, D.; Ballmer-Weber, B.; Bangert, C.; Ben-Shoshan, M.; Bernstein, J.A.; et al. The international EAACI/GA2LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy 2021, 77, 734–766. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.; Eyerich, K.; Eyerich, S.; Ferrer, M.; Gutermuth, J.; Hartmann, K.; Jakob, T.; Kapp, A.; Kolkhir, P.; Larenas-Linnemann, D.; et al. Urticaria: Collegium Internationale Allergologicum (CIA) Update 2020. Int. Arch. Allergy Immunol. 2020, 181, 321–333. [Google Scholar] [CrossRef]
- Dobrican, C.-T.; Muntean, I.A.; Pintea, I.; Petricău, C.; Deleanu, D.-M.; Filip, G.A. Immunological signature of chronic spontaneous urticaria (Review). Exp. Ther. Med. 2022, 23, 381. [Google Scholar] [CrossRef] [PubMed]
- Bansal, C.J.; Bansal, A.S. Stress, Pseudoallergens, Autoimmunity, Infection and Inflammation in Chronic Spontaneous Urticaria. Allergy Asthma Clin. Immunol. 2019, 15, 56. [Google Scholar] [CrossRef] [PubMed]
- Muntean, I.A.; Pintea, I.; Bocsan, I.C.; Dobrican, C.T.; Deleanu, D. COVID-19 Disease Leading to Chronic Spontaneous Urticaria Exacerbation: A Romanian Retrospective Study. Healthcare 2021, 9, 1144. [Google Scholar] [CrossRef]
- MacGlashan, D. Autoantibodies to IgE and FcϵRI and the Natural Variability of Spleen Tyrosine Kinase Expression in Basophils. J. Allergy Clin. Immunol. 2019, 143, 1100–1107.e11. [Google Scholar] [CrossRef]
- Rauber, M.M.; Pickert, J.; Holiangu, L.; Möbs, C.; Pfützner, W. Functional and Phenotypic Analysis of Basophils Allows Determining Distinct Subtypes in Patients with Chronic Urticaria. Allergy 2017, 72, 1904–1911. [Google Scholar] [CrossRef]
- Zhou, B.; Li, J.; Liu, R.; Zhu, L.; Peng, C. The Role of Crosstalk of Immune Cells in Pathogenesis of Chronic Spontaneous Urticaria. Front. Immunol. 2022, 13, 879754. [Google Scholar] [CrossRef]
- Church, M.K.; Kolkhir, P.; Metz, M.; Maurer, M. The role and relevance of mast cells in urticaria. Immunol. Rev. 2018, 282, 232–247. [Google Scholar] [CrossRef]
- Yanase, Y.; Takahagi, S.; Ozawa, K.; Hide, M. The Role of Coagulation and Complement Factors for Mast Cell Activation in the Pathogenesis of Chronic Spontaneous Urticaria. Cells 2021, 10, 1759. [Google Scholar] [CrossRef]
- Saini, S.S.; Paterniti, M.; Vasagar, K.; Gibbons, S.P., Jr.; Sterba, P.M.; Vonakis, B.M. Cultured Peripheral Blood Mast Cells From Chronic Idiopathic Urticaria Patients Spontaneously Degranulate Upon IgE Sensitization: Relationship to Expression of Syk and SHIP-2. Clin. Immunol. 2009, 132, 342–348. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, J.C.; Azor, M.H.; Nojima, V.Y.; Lourenço, F.D.; Prearo, E.; Maruta, C.W.; Rivitti, E.A.; da Silva Duarte, A.J.; Sato, M.N. Increased Circulating Pro-inflammatory Cytokines and Imbalanced Regulatory T-cell Cytokines Production in Chronic Idiopathic Urticaria. Int. Immunopharmacol. 2008, 8, 1433–1440. [Google Scholar] [CrossRef]
- Bonnekoh, H.; Maurer, M.; Krause, K. Interleukin-1-related cytokines as potential biomarkers in autoinflammatory skin diseases. Pediatr. Rheumatol. 2015, 13 (Suppl. 1), P197. [Google Scholar] [CrossRef][Green Version]
- Kuna, M.; Štefanović, M.; Ladika Davidović, B.; Mandušić, N.; Birkić Belanović, I.; Lugović-Mihić, L. Chronic Urticaria Biomarkers IL-6, ESR and CRP in Correlation with Disease Severity and Patient Quality of Life—A Pilot Study. Biomedicines 2023, 11, 2232. [Google Scholar] [CrossRef]
- Lin, W.; Zhou, Q.; Liu, C.; Ying, M.; Xu, S. Increased plasma IL-17, IL-31, and IL-33 levels in chronic spontaneous urticaria. Sci. Rep. 2017, 7, 17797. [Google Scholar] [CrossRef]
- Dobrican-Băruța, C.-T.; Deleanu, D.M.; Muntean, I.A.; Pintea, I.; Florea, C.M.; Filip, G.A. IL-31—Pruritus Interleukin: Serum Values and Clinical Impact in Chronic Spontaneous Urticaria—A Romanian Retrospective Study. J. Clin. Med. 2023, 12, 5957. [Google Scholar] [CrossRef]
- Kay, A.B.; Clark, P.; Maurer, M.; Ying, S. Elevations in T-helper-2-initiating cytokines (interleukin-33, interleukin-25, and thymic stromal lymphopoietin) in lesional skin from chronic spontaneous (‘idiopathic’) urticaria. Br. J. Dermatol. 2015, 172, 1294–1302. [Google Scholar] [CrossRef]
- Hueber, A.J.; Alves-Filho, J.C.; Asquith, D.L.; Michels, C.; Millar, N.L.; Reilly, J.H.; Graham, G.J.; Liew, F.Y.; Miller, A.M.; McInnes, I.B. IL-33 induces skin inflammation with mast cell and neutrophil activation. Eur. J. Immunol. 2011, 41, 2229–2237. [Google Scholar] [CrossRef]
- Drube, S.; Grimlowski, R.; Deppermann, C.; Fröbel, J.; Kraft, F.; Andreas, N.; Stegner, D.; Dudeck, J.; Weber, F.; Rödiger, M.; et al. The Neurobeachin-like 2 Protein Regulates Mast Cell Homeostasis. J. Immunol. 2017, 199, 2948–2957. [Google Scholar] [CrossRef] [PubMed]
- Borgia, F.; Custurone, P.; Li Pomi, F.; Vaccaro, M.; Alessandrello, C.; Gangemi, S. IL-33 and IL-37: A Possible Axis in Skin and Allergic Diseases. Int. J. Mol. Sci. 2023, 24, 372. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, A.; Katsoulis-Dimitriou, K.; Edler, H.J.; Dudeck, J.; Drube, S.; Dudeck, A. Mast cells initiate the vascular response to contact allergens by sensing cell stress. J. Allergy Clin. Immunol. 2020, 145, 1476–1478. [Google Scholar] [CrossRef]
- Kaplan, A.; Lebwohl, M.; Giménez-Arnau, A.M.; Hide, M.; Armstrong, A.W.; Maurer, M. Chronic spontaneous urticaria: Focus on pathophysiology to unlock treatment advances. Allergy 2022, 78, 389–401. [Google Scholar] [CrossRef]
- Pedersen, N.H.; Sørensen, J.A.; Ghazanfar, M.N.; Zhang, D.G.; Vestergaard, C.; Thomsen, S.F. Biomarkers for Monitoring Treatment Response of Omalizumab in Patients with Chronic Urticaria. Int. J. Mol. Sci. 2023, 24, 11328. [Google Scholar] [CrossRef]
- Asero, R.; Ferrucci, S.M.; Calzari, P.; Consonni, D.; Cugno, M. Thyroid Autoimmunity in CSU: A Potential Marker of Omalizumab Response? Int. J. Mol. Sci. 2023, 24, 7491. [Google Scholar] [CrossRef]
- Bostan, O.C.; Damadoglu, E.; Sarac, B.E.; Kilic, B.; Sahiner, M.; Karaaslan, C.; Karakaya, G.; Kalyoncu, A.F. Cytokine Profiles of Chronic Urticaria Patients and The Effect of Omalizumab Treatment. Dermatol. Pract. Concept. 2023, 13, e2023272. [Google Scholar] [CrossRef]
- Metz, M.; Maurer, M. Use of Biologics in Chronic Spontaneous Urticaria—Beyond Omalizumab Therapy? Allergol. Select 2021, 5, 89–95. [Google Scholar] [CrossRef]
- Metz, M.; Kolkhir, P.; Altrichter, S.; Siebenhaar, F.; Levi-Schaffer, F.; Youngblood, B.A.; Church, M.K.; Maurer, M. Mast cell silencing: A novel therapeutic approach for urticaria and other mast cell-mediated diseases. Allergy 2023, 79, 37–51. [Google Scholar] [CrossRef]
- Manti, S.; Giallongo, A.; Papale, M.; Parisi, G.F.; Leonardi, S. Monoclonal antibodies in treating chronic spontaneous urticaria: New drugs for an old disease. J. Clin. Med. 2022, 11, 4453. [Google Scholar] [CrossRef]
- Puxeddu, I.; Italiani, P.; Giungato, P.; Pratesi, F.; Panza, F.; Bartaloni, D.; Rocchi, V.; Del Corso, I.; Boraschi, D. Free IL-18 and IL-33 cytokines in chronic spontaneous urticaria. Cytokine 2013, 61, 741–743. [Google Scholar] [CrossRef]
- Cayrol, C.; Girard, J.P. Interleukin-33 (IL-33): A critical review of its biology and the mechanisms involved in its release as a potent extracellular cytokine. Cytokine 2022, 156, 155891. [Google Scholar] [CrossRef]
- Trier, A.M.; Ver Heul, A.M.; Fredman, A.; Kropski, J.A.; Dai, R.; Mitchell, D.; Serezani, A.P.; Guttman-Yassky, E.; Richmond, J.; Gilfillan, A.M.; et al. IL-33 potentiates histaminergic itch. J. Allergy Clin. Immunol. 2023. [Google Scholar] [CrossRef]
- Garcovich, S.; Maurelli, M.; Gisondi, P.; Peris, K.; Yosipovitch, G.; Girolomoni, G. Pruritus as a Distinctive Feature of Type 2 Inflammation. Vaccines 2021, 9, 303. [Google Scholar] [CrossRef]
- Murdaca, G.; Greco, M.; Tonacci, A.; Negrini, S.; Borro, M.; Puppo, F.; Gangemi, S. IL-33/IL-31 Axis in Immune-Mediated and Allergic Diseases. Int. J. Mol. Sci. 2019, 20, 5856. [Google Scholar] [CrossRef]
- Hasegawa, T.; Oka, T.; Demehri, S. Alarmin Cytokines as Central Regulators of Cutaneous Immunity. Front. Immunol. 2022, 13, 876515. [Google Scholar] [CrossRef]
- Stanbery, A.G.; Smita, S.; von Moltke, J.; Tait Wojno, E.D.; Ziegler, S.F. TSLP, IL-33, and IL-25: Not just for allergy and helminth infection. J. Allergy Clin. Immunol. 2022, 150, 1302–1313. [Google Scholar] [CrossRef]
- Hoy, S.M. Tezepelumab: First Approval. Drugs 2022, 82, 461–468. [Google Scholar] [CrossRef]
- Wang, S.-H.; Zuo, Y.-G. Thymic Stromal Lymphopoietin in Cutaneous Immune-Mediated Diseases. Front. Immunol. 2021, 12, 698522. [Google Scholar] [CrossRef]
- Damask, C.C.; Ryan, M.W.; Casale, T.B.; Castro, M.; Franzese, C.B.; Lee, S.E.; Levy, J.M.; Lin, S.Y.; Lio, P.A.; Peters, A.T.; et al. Targeted Molecular Therapies in Allergy and Rhinology. Otolaryngol.-Head Neck Surg. 2021, 164, S1–S21. [Google Scholar] [CrossRef]
- Hashimoto, T.; Rosen, J.D.; Sanders, K.M.; Yosipovitch, G. Possible roles of basophils in chronic itch. Exp. Dermatol. 2019, 28, 1373–1379. [Google Scholar] [CrossRef]
- Treudler, R.; Simon, J.-C. Developments and perspectives in allergology. J. Der Dtsch. Dermatol. Ges. 2023, 21, 399–403. [Google Scholar] [CrossRef]
- Metz, M.; Krull, C.; Maurer, M. Histamine, TNF, C5a, IL-6, -9, -18, -31, -33, TSLP, neopterin, and VEGF are not elevated in chronic spontaneous urticaria. J. Dermatol. Sci. 2013, 70, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, P.; Russo, D.; Attanasi, M.; Di Pillo, S.; Chiarelli, F. Immunological Targets of Biologic Drugs in Allergic Skin Diseases in Children. Biomedicines 2021, 9, 1615. [Google Scholar] [CrossRef] [PubMed]
- Mathias, S.D.; Crosby, R.D.; Zazzali, J.L.; Maurer, M.; Saini, S.S. Evaluating the minimally important difference of the urticaria activity score and other measures of disease activity in patients with chronic idiopathic urticaria. Ann. Allergy Asthma Immunol. 2012, 108, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Hawro, T.; Ohanyan, T.; Schoepke, N.; Metz, M.; Peveling-Oberhag, A.; Staubach, P.; Maurer, M.; Weller, K. The urticaria activity score-validity, reliability, and responsiveness. J. Allergy Clin. Immunol. Pract. 2018, 6, 1185–1190.e1. [Google Scholar] [CrossRef]
- Baiardini, I.; Braido, F.; Bindslev-Jensen, C.; Bousquet, P.J.; Brzoza, Z.; Canonica, G.W.; Compalati, E.; Fiocchi, A.; Fokkens, W.; Gerth van Wijk, R.; et al. Recommendations for assessing patient-reported outcomes and health-related quality of life in patients with urticaria: A GA^2LEN taskforce position paper. Allergy 2011, 66, 840–844. [Google Scholar] [CrossRef]
- Weller, K.; Groffik, A.; Magerl, M.; Tohme, N.; Martus, P.; Krause, K.; Metz, M.; Staubach, P.; Maurer, M. Development and construct validation of the angioedema quality of life questionnaire. Allergy 2012, 67, 1289–1298. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Controls | CSU Patients | p-Values (Mann–Whitney U) |
|---|---|---|---|
| Total Participants (n) | 33 | 50 | N/A |
| Average Age (yrs. ± SD) | 44.32 ± 9.23 | 50.14 ± 16.10 | N/A |
| Gender Distribution (F/M) | 26/12 | 36/14 | N/A |
| Atopy Status (Atopic/Non-atopic) | 10/28 | 14/36 | N/A |
| IL-25 (pg/mL ± SD) | 105.03 ± 89.21 | 140.27 ± 100.16 | 0.0823 |
| TSLP (pg/mL ± SD) | 434.57 ± 169.43 | 1200.42 ± 1348.36 | <0.0001 |
| IL-33 (pg/mL ± SD) | 21.70 ± 22.68 | 220.67 ± 201.17 | <0.0001 |
| Total IgE (IU/L ± SD) | 41.23 ± 27.08 | 168.63 ± 178.99 | <0.0001 |
| Eos (×1000 cells/µL ± SD) | 0.163 ± 0.102 | 0.495 ± 0.704 | 0.1015 |
| RF (IU/mL ± SD) | 10.75 ± 2.82 | 14.02 ± 1.58 | <0.0001 |
| ESR (mm/h ± SD) | 12 ± 6.71 | 14.29 ± 9.89 | 0.8074 |
| CRP (mg/dL ± SD) | 0.36 ± 0.33 | 0.36 ± 0.27 | 0.7408 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrican-Băruța, C.-T.; Deleanu, D.M.; Muntean, I.A.; Nedelea, I.; Bălan, R.-G.; Filip, G.A.; Procopciuc, L.M. The Alarmin Triad—IL-25, IL-33, and TSLP—Serum Levels and Their Clinical Implications in Chronic Spontaneous Urticaria. Int. J. Mol. Sci. 2024, 25, 2026. https://doi.org/10.3390/ijms25042026
Dobrican-Băruța C-T, Deleanu DM, Muntean IA, Nedelea I, Bălan R-G, Filip GA, Procopciuc LM. The Alarmin Triad—IL-25, IL-33, and TSLP—Serum Levels and Their Clinical Implications in Chronic Spontaneous Urticaria. International Journal of Molecular Sciences. 2024; 25(4):2026. https://doi.org/10.3390/ijms25042026
Chicago/Turabian StyleDobrican-Băruța, Carmen-Teodora, Diana Mihaela Deleanu, Ioana Adriana Muntean, Irena Nedelea, Radu-Gheorghe Bălan, Gabriela Adriana Filip, and Lucia Maria Procopciuc. 2024. "The Alarmin Triad—IL-25, IL-33, and TSLP—Serum Levels and Their Clinical Implications in Chronic Spontaneous Urticaria" International Journal of Molecular Sciences 25, no. 4: 2026. https://doi.org/10.3390/ijms25042026
APA StyleDobrican-Băruța, C.-T., Deleanu, D. M., Muntean, I. A., Nedelea, I., Bălan, R.-G., Filip, G. A., & Procopciuc, L. M. (2024). The Alarmin Triad—IL-25, IL-33, and TSLP—Serum Levels and Their Clinical Implications in Chronic Spontaneous Urticaria. International Journal of Molecular Sciences, 25(4), 2026. https://doi.org/10.3390/ijms25042026