Abstract
Ginseng is one of the most valuable and commonly used Chinese medicines not only in ancient China but also worldwide. Ginsenosides, also known as saponins or triterpenoids, are thought to be responsible for the beneficial effects of ginseng. In this review, we summarize recent publications on anti-diabetic studies of ginseng extracts and ginsenosides in cells, animals, and humans. It seems that the anti-diabetic effect of ginseng is positive for type 2 diabetic patients but has no significant impact on prediabetes or healthy adults. Regulation of insulin secretion, glucose uptake, anti-oxidative stress, and anti-inflammatory pathways may be the mechanisms involved with ginseng’s anti-diabetic effects. Taken together, this summary provides evidence for the anti-diabetes effects of ginseng extracts and ginsenosides as well as the underlying mechanisms of their impact on diabetes.
1. Introduction
The main type of diabetes is type 1 diabetes, which is caused by insulin deficiency, and type 2 diabetes, which is characterized by insulin resistance [1]. The majority of diabetes is type 2 diabetes, and it is a formidable challenge for public health [2]. According to the International Diabetes Federation statistics, 463 million people aged 20–79 years worldwide had type 2 diabetes in 2019, and this number is estimated to reach 700 million by 2045 [3]. There is also a huge population with prediabetes, which is very likely to develop into type 2 diabetes [4]. Without proper management, diabetes can cause serious health problems, especially diabetic complications. For example, it can damage eyes, kidneys, and nerves, and it also causes heart disease, stroke, and can even necessitate limb removal [5]. Thus, proper treatment of diabetes is important. Although many researchers are looking at ways to reduce insulin resistance to treat type 2 diabetes, type 2 diabetes is still a severe disease and cannot be cured [6]. Currently, management of diabetes mainly focuses on insulin or its peptide derivatives, anti-diabetic oral drugs, and diet control [7]. Insulin and its peptide derivative treatments need to be injected via vein every day, leading to inconvenience and burdens for patients [8]. Long-term oral administration of chemical drugs can be harmful for many diabetic patients because of drug toxicities [8]. Researchers are exploring the possibilities offered by complementary and alternative medicine, such as traditional herbal medicine.
There has been increasing popularity in Chinese medicine, especially since the 2015 Nobel Prize was awarded to Tu Youyou, who discovered that artemisinin from traditional Chinese medicine can treat malaria [9]. This popularity indicates that even in modern times, ancient Chinese herbal remedies can be valuable as an alternative therapy for relieving serious diseases. One of the Chinese medicinal herbs with promising anti-diabetic effects is ginseng [10]. In fact, ginseng has long been used to treat diabetes in China. In the Song Dynasty (1078 A.D.), official documentation (Formularies of the Bureau of People’s Welfare Pharmacies) recorded that ginseng was employed to cure Xiaoke disease, which is nowadays known as diabetes [10]. As a medicinal intervention management to diabetes, the Asian (Panax ginseng) and American (Panax quinquefolius L.) ginsengs are the two most widely used varieties and have recently attracted a lot of attention from those trying to understand the molecular mechanisms of ginseng’s anti-diabetic effects.
Ginseng contains diversified components, including saponins, polysaccharides, polyacetylenes, phenols, and alkaloids. Ginseng saponins, known as ginsenosides, are an important class of natural triterpene saponins, which are thought to be responsible for the anti-diabetic effect in ginseng. So far, nearly two hundred ginsenosides have been detected from ginseng plants and heat-processed ginseng products [11]. Most known ginsenosides are classified as members of the dammarane family, and consist of a four-ring, steroid-like structure, such as ginsenosides Rb1, Rg3, Re, and Rg1 (structures shown in Figure 1). Increasing studies suggest that ginseng extracts, processed ginseng extracts, and ginsenosides show anti-diabetic effects, although the mechanism of action is still not clear. A systematic summary of anti-diabetic studies of ginseng will be helpful to explore its anti-diabetic mechanism.
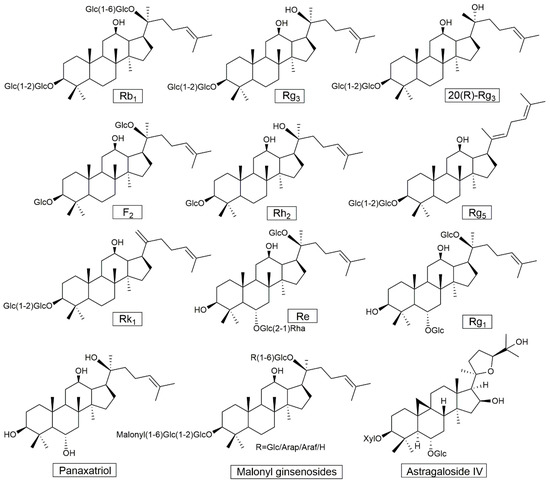
Figure 1.
Chemical structures of triterpenoid saponins mentioned in this study. Glc, Rha, Arap, Araf, and Xyl refer to β-d-glucopyranosyl, α-l-rhamnopranosyl, α-l-arabinopyranosyl, α-l-arabinofuranosyl, and β-d-xylopyranosyl, respectively.
Until 2011, there were eleven publications (twelve human trials) about ginseng extracts being used for diabetes intervention. Four of them studied American ginseng root extracts, five of them studied Asian ginseng root extracts, two used ginsenosides (Rb1 and Rg1, Re), and one tested eight types of ginseng (American, American-wild, Asian, Asian-red, Vietnamese-wild, Siberian, Japanese-rhizome, and Sanchi ginseng) on acute postprandial glycemic indices in healthy humans. Through summarizing these twelve human trials, along with in vitro cell studies and in vivo animal studies, the authors deduced that ginseng may modulate insulin production/secretion, glucose metabolism and uptake, or inflammatory pathway to exert anti-diabetic effects [12]. Recently, many studies, including human studies, in vitro and in vivo studies have been conducted on diabetes intervention with ginseng extracts or ginsenoside. In order to better know the progress and basis for the evaluation of the anti-diabetic effects of ginseng, this current review summarizes the research into type 2 diabetes intervention with ginseng extracts or ginsenosides conducted in human trials, in vivo animal studies, and in vitro cell studies since 2012.
2. Anti-Diabetic Effects of Ginseng in Human Trials
Although ginseng has been used as a natural herb medicine for a long time in East Asia, interest in the anti-diabetic efficacy of ginseng has drawn increased attention from modern medicine. An increasing number of human trials are exploring the efficacy of ginseng intervention in diabetes. Shishtar et al. found ginseng significantly reduced fasting blood glucose compared to the control (−0.31 mmol/L [95% CI: −0.59 to −0.03], p = 0.03) based on a meta-analysis of sixteen randomized controlled clinical trials; there was no significant effect on fasting plasma insulin and glycated hemoglobin [13]. Another meta-analysis included eight trials that suggested ginseng supplementation showed significant differences on fasting glucose (−0.306 mmol/L [95% CI: −0.539 to −0.074], p = 0.01), postprandial insulin (−2.132 mmol/L [95% CI: −3.706 to −0.558], p = 0.008), and HOMA-IR (−0.397 mmol/L [95% CI: −0.679 to −0.115], p = 0.006) compared to the control group; there was no significant difference on postprandial glucose and fasting insulin between ginseng treatment and control groups [14]. Since 2012, there have been 13 human trials published that have focused on the anti-diabetic effect of ginseng (Asian ginseng (Panax ginseng) and American ginseng (Panax quinquefolius L.)). Different ginseng extracts or differently processed ginseng products exhibited varied impact on diabetic patients. The information of ginseng extracts mentioned in this study is shown in Table 1.

Table 1.
Ginseng materials mentioned in this study.
Ten clinical trials on Asian ginseng have been reported in recent years. In one trial, thirty-six diabetic patients were randomized to receive 1.5 g/day of ginsam, which is enriched ginsenoside Rg3, though a vinegar extraction from P. ginseng, or a daily placebo for eight weeks. HbA1c levels and fasting blood glucose in the ginsam-treated group significantly reduced by 0.56% and 21.40 mg/dL compared to the placebo group [15]. Park et al. reported that 23 impaired fasting glucose participants were randomly administrated with 960 mg/day of hydrolyzed Asian ginseng extract or a placebo for eight weeks. The hydrolyzed ginseng extract, containing 7.54 mg/g of Rg1, 6.30 mg/g of compound K, 5.42 mg/g of Rb1, 1.87 mg/g of Re, 0.70 mg/g of Rd, 0.36 mg/g of Rb2, and 0.29 mg/g of Rc, significantly decreased fasting plasma glucose (p = 0.017) and postprandial glucose (p = 0.01) compared to the placebo but there were no significant differences in fasting plasma insulin and postprandial insulin between the groups [16]. These results showed that hydrolyzed ginseng extract cut the absorption of glucose in the intestinal lumen. Further large-scale and long-term studies are needed to fully evaluate whether it can decrease insulin secretion.
The ginseng berry has a different ginsenoside composition and contains more plentiful ginsenosides than its root [17]. An in vivo study using ob/ob diabetic mice reported that after being treated with 150 mg/kg ginseng berry extract, fasting blood glucose significantly decreased to 150 mg/dL on day 5 and 129 mg/dL on day 12. The same experiment was carried out with ginseng root extract. Although the same dose of ginseng root extract significantly reduced the fasting blood glucose to 143 mg/dL on day 5, the fasting blood glucose had not decreased by day 12 (155 mg/dL) [18]. This study showed that ginseng berry extract exhibited more potent anti-hyperglycemic effects compared to ginseng root extract administrated at the same concentrations using ob/ob diabetic mice. Recently, a 12-week, randomized, double-blind, placebo-controlled clinical trial was completed with 72 participants with a fasting glucose level ranging from 100–140 mg/dL. The study showed that ginseng berry extract significantly reduced fasting blood glucose and postprandial glucose at 60 min in an oral glucose tolerance test after a 12-week treatment, but it did not regulate serum glucose to normal levels [19], indicating that the ginseng berry extract failed to show anti-hyperglycemic effects in this human study. It should be noted that the participants in this study were prediabetes rather than type 2 diabetic patients. The anti-hyperglycemic effect was observed in the ob/ob diabetic mice model [18]. Maybe the anti-hyperglycemic effect of ginseng berry extract is positive for type 2 diabetes rather than prediabetes. Further investigation of people with type 2 diabetes is needed to test this hypothesis.
Participants with impaired fasting glucose, impaired glucose tolerance, or type 2 diabetes consuming 5 g/day Korean red ginseng (KRG) extract were found to have significantly reduced blood glucose. Specifically, −1.23 ± 0.59 mmol/L of serum glucose and –0.97 ± 0.30 mmol/L of whole blood glucose were decreased at a 30 min oral glucose tolerance test after a 12-week intervention [20]. The plasma insulin sensitivity index increased by 33% compared to the placebo group in this 12-week randomized, double-blind and placebo-controlled trial [20].
In a randomized, double-blind, placebo-controlled trial involving forty-two subjects, 2.7 g/day of fermented red ginseng given for four weeks significantly increased postprandial insulin of subjects with impaired fasting glucose or type 2 diabetes (35.5 µU/mL in the placebo group vs. 56.3 µU/mL in the ginseng group, p = 0.040). Moreover, in the ginseng treatment group, their postprandial glucose and glucose area under curves (AUC) significantly reduced by 17.2% (p = 0.0001) and 27.4% (p = 0.002) compared to the baseline values. However, the ginseng treated group did not show a remarkable difference in fasting blood glucose and insulin relative to the placebo [21]. It is known that fermentation can increase the bioavailability (absorption and bioactivity) of ginseng due to small ginsenosides (ginsenoside Rg3, compound K, etc.) produced through the fermentation process. As reported by Bang et al. in the clinical trial [20], 5 g/day of Korean red ginseng can reduce fast blood glucose and glucose AUC. However, in this study [21], the fermented red ginseng only modulated postprandial glucose and insulin, not fasting glucose and insulin. The short period of time (four weeks) may be responsible for the lack of significant differences in fasting glucose and insulin because the improvement of fasting glucose and insulin is usually expected over a long-term treatment, while postprandial glucose and insulin are more sensitive to slight interventions in glycemic control. Long-term clinical trials for fermented red ginseng are needed.
These studies suggest that different Asian ginseng extracts consistently reduce the fasting blood glucose or postprandial glucose in type 2 diabetic patients and could be considered as an optional therapy for managing type 2 diabetes. However, other results from human studies cast doubts about this view.
Sixty-eight obese subjects without diabetes were administrated 6 g/day of KRG (orally) or a placebo for 12 weeks in a randomized, double-blind, and placebo-controlled trial. This study showed that there was no significant effect on the insulin level and the insulin sensitivity index between the ginseng treatment group and placebo group [22]. Another randomized, double-blind, placebo-controlled 8-week trial conducted among fifty obese women found that there were significant improvements in the obesity index between before and after treatment with 6 g/day KRG, but no significant difference between the KRG treatment group and the placebo group [23]. Both of these studies indicate that KRG does not enhance insulin sensitivity in obese people without diabetes. In both trials, the regulation of glucose homeostasis was not observed in the prediabetes situation for subjects who were obese without diabetes, impaired glucose tolerance or mild type 2 diabetes. Recently, a multicenter, double-blind, randomized, and placebo-controlled trial was conducted on 1000 healthy adults. The test group consumed 2 g/day of KRG for 24 weeks, which was found to be safe and well-tolerated in healthy adults, and there were no significant abnormal changes from anthropometric, laboratory, and vital sign measurements between the KRG group and the placebo group [24]. Therefore, it seems that the anti-diabetic effect of Asian ginseng is positive for type 2 diabetic patients, but there has no significant effect on prediabetes or healthy adults.
Besides the human trials using Asian ginseng, there have been three trials using American ginseng on type 2 diabetic patients. In one study, thirty type-2 patients were involved in a randomized, placebo-controlled crossover trial. HbA1c levels were 0.31% lower (p = 0.011) after treatment with 6 g konjac-glucomannan-based fiber blended together with 3 g American ginseng per day for 12 weeks. Plasma lipids of the ginseng intervention group also significantly decreased compared to the placebo control group [25]. This study did not consider the effect of konjac-glucomannan-based fiber on diabetes. The study did not report whether the konjac-glucomannan-based fiber blend or the American ginseng was responsible for reducing the glucose levels in the trial subjects. The study could be improved by planning another group administrated with konjac-glucomannan-based fiber, or adding it to the placebo. Vuksan et al. [26] conducted a randomized, double-blind, and placebo-controlled crossover clinical study to assess the anti-diabetic efficacy and safety of American ginseng. Twenty-four individuals with well-controlled type 2 diabetes completed the study. Using a double-blind, crossover design, the participants were randomized to receive either 3 g/day of American ginseng extract or a placebo for eight weeks together with their original treatment. The efficacy was assessed by HbA1c, and safety was assessed by liver and kidney function testing. The researchers found that American ginseng significantly reduced HbA1c levels (−0.29%, p = 0.041), fasting blood glucose (−0.71 mmol/L, p = 0.008), and systolic blood pressure (−5.6 mmHg, p < 0.001) compared to the placebo. Furthermore, the beneficial changes did not affect the safety profiles. Another human study specifically tested the safety of American ginseng as an adjunct to conventional therapy in type 2 diabetes [27]. Seventy-four type 2 diabetic patients were given 3 g/day American ginseng extract or a placebo for 12 weeks. The investigators found that there was no significant difference between the ginseng treatment and the placebo in the safety parameters, such as kidney function (urates and creatinine), liver function (AST and ALT), and hemostatic function (PT and INR). These studies suggest that American ginseng extract is effective and safe as an additional treatment in the management of type 2 diabetes.
Together, these human studies show that both Asian ginseng and American ginseng do indeed decrease blood glucose in type 2 diabetics. At the same time, it should be noted that this efficacy was observed in several limited ginsenosides (6–7 ginsenosides analyzed), small sample sizes (23–94 subjects), and short-term studies (4–12 weeks). Larger scale clinical trials are needed to completely illuminate the long-term benefits of this herbal supplement in the management of type 2 diabetes. The studies are summarized in Table 2.
Table 2.
Effects of ginseng on diabetes-related parameters in human studies.
3. Potential Mechanisms of the Anti-Diabetic Effect of Ginseng
Apart from the clinical evidence for the anti-diabetic effect of ginseng, there have also been animal studies conducted to explore the underlying mechanisms of the anti-diabetic effect of ginseng, along with some cell experiments in vitro. Different processed ginseng extracts and some individual ginsenosides (structures shown in Figure 1) have been reported to exhibit an anti-diabetic effect in cell and animal experiments (Table 3 and Table 4). Although the anti-diabetic mechanism of ginseng has not been entirely clarified, the available data indicate that the regulation of blood glucose by ginseng is possibly related to the following four aspects.
Table 3.
Effects of ginseng on diabetes-related parameters in animal studies.
Table 4.
Effects of ginseng on diabetes-related molecular targets in cell line studies.
First, ginseng modulates blood glucose levels by improving β-cell function and enhancing insulin sensitivity. P. ginseng berry extract increased β-cell proliferation and insulin secretion to improve glycemic control in streptozotocin (STZ) -induced diabetic mice [28]. Ginseng berry extract could also improve insulin sensitivity in C57BL/6 mice over 15 months old, likely by increasing the activation of IRS-1 and AKT [29]. Kim et al. found that 200 mg/kg of black ginseng extract inhibited β-cell apoptosis and improved islet architecture, which led to the enhancement of β-cell function and reduction of hyperglycemia in STZ-treated mice [30]. While exploring the anti-diabetic component of ginseng extracts, both PPD-type ginsenosides and PPT-type ginsenosides were investigated in animal studies. Ginsenoside Rb1, one of the main PPD-type ginsenosides, was found to reduce symptoms of decreased insulin sensitivity and elevated blood glucose caused by the high-fat diet induction of type 2 diabetic mice [31]. Using the STZ-induced diabetic rat model, researchers found that a main PPT-type ginsenoside, Rg1, can lower insulin resistance and blood glucose, and also improve the blood lipid profile and liver function [32], suggesting that Rg1 may be a potential adjuvant therapy for type 2 diabetic patients with fatty liver disease. As well as the main components in fresh ginseng extracts, heat-treated ginsenoside Rg3 has also been tested. Ginsenoside Rg3 is the main metabolite degraded from other abundant ginsenosides during heat-processing fresh ginseng to manufacture red ginseng and black ginseng. Kim et al. screened the GLP-1 release ability of 15 ginsenosides and found that Rg3 showed the strongest GLP-1 secretion (about 27 pM/mg) effect in NCI-H716 cells. In this in vivo trial, 10 µM Rg3 significantly raised production of GLP-1 and insulin to reduce blood glucose in db/db mice [33]. In mouse islet cells, insulin secretion was significant: 2.3 times higher in the 4 μM Rg3 treatment group compared to control group [34]. Taken together, Rg3 is presumably the main active anti-diabetic ingredient of ginseng, although administration with other ginsenosides has also shown hypoglycemic effects; these ginsenosides can be hydrolysed to Rg3 in the gastrointestinal tract [35] to further exert pharmacological effects.
Second, ginseng can enhance glucose uptake by up-regulating the expression of glucose transporters (GLUT). One percent Fermented red ginseng (FRG) significantly decreased the body weight of ob/ob mice compared with the controls after 4 weeks of administration during the 16-week treatment period; blood glucose was also significantly reduced after 16-weeks treatment with FRG [44]. Furthermore, the study found that the expressions of GLUT1 and GLUT4 were significantly up-regulated by FRG in liver and muscle. This suggests that FRG may decrease blood glucose through enhancing glucose uptake in skeletal muscle. Similar results were also observed in db/db mice treated with ginseng extracts. 0.5 g/kg fermented steam-dried ginseng berry (FSGB) [45] significantly decreased body weight and blood glucose in db/db mice during a 35-day treatment; furthermore, the plasma insulin in the FSGB treated group (17.05 ± 0.49 ng/mL) significantly increased almost double compared to the untreated db/db group (8.21 ± 0.60 ng/mL). GLUT1 mRNA expression was up-regulated by FSGB in the L6 skeletal muscle cells. During an 8-week treatment with 0.1% fermented ginseng extract (FGE) in db/db mice, the body weight, fasting blood glucose, and HbA1c level significantly (p < 0.05) decreased compared to control groups [46]. FGE intervention significantly enhanced the mRNA expression of GLUT2 and lowered the glucose-6-phosphotase (G6Pase) expression in liver tissues [46]. G6Pase plays an important role in glucose homeostasis because it is a main enzyme of gluconeogenesis and glycogenolysis in the liver. The reduction of G6Pase and increase of GLUT2 expressions mean FGE may improve the transport of blood glucose into the liver, which leads to decreasing the blood glucose level in db/db mice. Moreover, the FGE group exhibited a higher level of insulin secretion than the control group in the islet primary cell culture; the FGE treated group had weaker damage and inflammation than the control group in vivo hematoxylin–eosin staining assay [46]. These suggest that FGE has a protective effect on the pancreas and improves the production/secretion of insulin. Kang et al. found that 900 mg/kg black ginseng ethanol extract (GBG05-FF) significantly reduced fasting blood glucose, glucose tolerance, and plasma HbA1c after four weeks of treatment. Furthermore, GBG05-FF up-regulated the expressions of GLUT2 in the liver and GLUT4 in the muscles [43], indicating that black ginseng can enhance glucose uptake in surrounding tissues to regulate blood glucose levels. In addition, other beneficial physiological changes, such as a reduction of total cholesterol and triglycerides, and increased PPAR-γ and PEPCK were also observed after administration with fermented ginseng berry [46] or black ginseng [43]. Ginsenosides Rg1 [66] and Re [67] increased expressions of GLUT4 through AMPK pathways in C2CI2 muscle cells and via increasing PPAR-γ activity in 3T3-L1 cells, respectively. Furthermore, KRG at a dose of 0.2 g/kg/d for a 12-week treatment period enhanced insulin action and secretion in diabetic Goto-Kakizaki rats by up-regulating the GLUT4 expression in adipose tissue and down-regulating the expressions of UCP2 and PARP in the pancreas, and PTP-1B in adipose tissue and skeletal muscle [40].
Third, suppression of oxidative stress through increasing SOD activity and decreasing MDA production was reported to occur in treatment with either ginseng polysaccharides in STZ-induced ICR diabetic mice [50], or ginsenoside Rg1 in STZ-induced diabetic rats [57]. Administration of GS-E3D (pectin lyase-modified red ginseng extract) for six weeks significantly decreased urinary levels of albumin, 8-hydroxy-2′-deoxyguanosine (8-OHdG), and advanced glycation end-products (AGEs) in STZ-induced diabetic rats. Moreover, all symptoms of diabetic nephropathy were improved by GS-E3D treatment via suppressing renal accumulation of AGEs and oxidative stress [47]. Tissue culture raised mountain ginseng adventitious root (TCMGARs) extracts at dosage levels of 250, and 500 mg/kg significantly reduced the blood glucose, total cholesterol, and triglyceride content in STZ-induced diabetic rats [38]. In an LDL-/- mouse model, Rg3-enriched red ginseng extract (44.91 mg/g, 66.6% occupy for total ginsenosides) significantly decreased the levels of glucose, triglyceride, low-density lipoprotein, alanine aminotransferase and aspartate aminotransferase compared to the control [48]. In a high-fat induced C57BL/6 mouse model, ginsenoside Re significantly reduced fasting blood glucose levels and related biochemical parameters, including cholesterol, low-density lipoprotein cholesterol, total triglyceride, glutamic-pyruvic transaminase, and glutamic-oxaloacetic transaminase. Re also regulated the level of ACh, AChE, and oxidative stress-related parameters (MDA, SOD, GSH) via the JNK pathway [55].
In addition to the above three potential anti-diabetic mechanisms, ginseng can also show anti-diabetic activity through other pathways. Several animal studies have found that ginseng processed products or individual ginsenosides regulate blood glucose in diabetic mouse or rat models, accompanied by regulating the expression of TNF-α, eNOS [46,53,56], suggesting that diabetes is associated with inflammation, and effective modulation by ginseng on inflammation may be able to prevent the development of insulin resistance. Recently, Shen et al. reported that Rg1 released in brain tissue using nano-drug delivery systems reduced the volume of cerebral infarction and improved neural recovery in diabetic rats with cerebral infarction [59], indicating that the hypoglycemic effect of Rg1 may be regulated through the central nervous system. Additionally, in an STZ-induced type 1 diabetic rat model, ginsenoside Rh2 reduced fasting blood glucose and improved cardiac function via enhancing PPAR-δ signaling in diabetic rats with cardiac fibrosis [60]. In the 3T3-L1 cells, researchers that found ginsenoside F2 [68], and a ginsenosides Rg5 + Rk1 mixture [69] could reduce lipid accumulation and down-regulate expression of PPAR-γ.
Based on studies on diabetes intervention with ginseng in vivo and in vitro, the potential mechanism of ginseng extracts (ginsenosides) on type 2 diabetes is summarized in Figure 2.
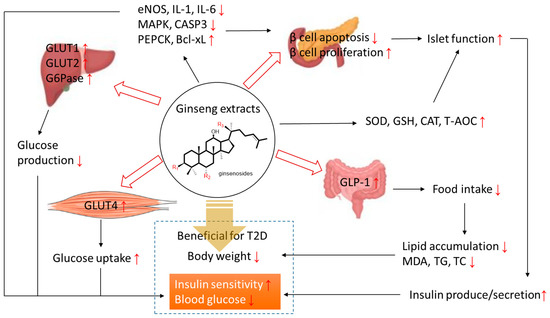
Figure 2.
The potential mechanism of ginseng extracts (ginsenosides) on type 2 diabetes. Bcl-xL: B-cell lymphoma-extra-large; CASP3: caspase-3; CAT: catalase; eNOS: endothelial nitric oxide synthase; G6Pase: glucose-6-phosphotase; GLP-1: glucagon-like peptide-1; GLUT: glucose transporter protein; GSH (-PX): glutathione peroxidase; IL: interleukin; MAPK: mitogen-activated protein kinase; MDA: malondialdehyde; PEPCK: phosphoenolpyruvate carboxykinase; SOD: superoxide dismutase; T-AOC: total anti-oxidative capacity; TC: total cholesterol; TG: triglycerides.
4. Conclusions
Human, animal, and cell studies have shown that different processed ginseng extracts and specific ginsenosides possess beneficial effects on diabetes, especially type 2 diabetes. Most studies of individual ginsenosides have focused on Rb1, Re, or Rg1, which are the main components of ginseng and are easily obtained. However, these ginsenosides have a large molecule structure, resulting in poor systemic bioavailability. Reeds et al. reported on overweight and obese participants with impaired glucose tolerance or newly diagnosed type 2 diabetes who consumed ginseng root extract (8 g/day), ginsenoside Re (250–500 mg/day), or placebo for 30 days; ginsenosides Rb1, Rb2, and Re were not detected in plasma after treatment with ginseng root extract or ginsenoside Re [70]. However, another study conducted in healthy volunteers showed that ginsenoside Re and its potential metabolites (including Rg2, F1, Rh1, and PPT) were detected in plasma after oral administration of ginsenoside Re [71]. It seems that the large molecule ginsenosides (Rb1, Rc, Re) may be a form of storage for saponins in ginseng plants rather than the active form in vivo. The related but smaller molecule ginsenosides (Rg3, Rh1) may be the ingredient that exerts therapeutic effects. This is also supported by the evidence found in experiments with red ginseng, fermented ginseng, and black ginseng. Therefore, the metabolic ginsenosides (Rg3, Rh1) need to be investigated to determine the active form of ginsenosides in vivo.
Another concern is that the results from clinical data for different processed ginseng extracts are inconsistent; some studies showed that the ginseng extracts possessed anti-hyperglycemic or diabetes-related effects, while others did not. These results could be caused by subject factors and/or drug reasons. The physical activity, body weight, diabetic degree, and sample size of volunteers may affect the outcomes of clinical trials. Another influencing factor is the variability of ginseng extracts. Different sources, species, or extraction processes lead to different ginseng ingredients. Even when using the same species and the same extraction process, different batches of ginseng can have various components, which influence the curative effect. Thus, characteristic detection and quality control are needed for ginseng products in clinical applications.
Author Contributions
W.C. and D.G.P. conceived the structure of this review; W.C. collected literature, analyzed data from literature, and wrote the original manuscript; P.B. and D.G.P. reviewed and edited the manuscript.
Funding
This work was supported by funding from the Alpha-Massey Natural Nutraceutical Research Centre.
Acknowledgments
We would like to acknowledge Ceire Hopley (librarian) for her help in literature searching and analysis.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chen, Q.; Zhu, L.; Tang, Y.; Zhao, Z.; Yi, T.; Chen, H. Preparation-related structural diversity and medical potential in the treatment of diabetes mellitus with ginseng pectins. Ann. N. Y. Acad. Sci. 2017, 1401, 75–89. [Google Scholar] [CrossRef] [PubMed]
- Aurora, R.N.; Punjabi, N.M. Obstructive sleep apnoea and type 2 diabetes mellitus: A bidirectional association. Lancet Respir. Med. 2013, 1, 329–338. [Google Scholar] [CrossRef]
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; IDF: Brussels, Belgium, 2019. [Google Scholar]
- Li, Z.; Jin, H.; Chen, W.; Sun, Z.; Jing, L.; Zhao, X.; Zhu, S.; Guo, X.; Study Group, C.N. Influencing Factors of Knowledge, Attitude, and Practice regarding Medical Nutrition Therapy in Patients with Diabetes: A National Cross-Sectional Study in Urban China. J. Diabetes Res. 2017, 2017, 8948452. [Google Scholar] [CrossRef] [PubMed]
- Forbes, J.M.; Cooper, M.E. Mechanisms of diabetic complications. Physiol. Rev. 2013, 93, 137–188. [Google Scholar] [CrossRef] [PubMed]
- Warren, R.E. The stepwise approach to the management of type 2 diabetes. Diabetes Res. Clin. Pr. 2004, 65S, S3–S8. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Shin, B.C.; Lee, M.S.; Lee, H.; Ernst, E. Red ginseng for type 2 diabetes mellitus: A systematic review of randomized controlled trials. Chin. J. Integr. Med. 2011, 17, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Che, J.Y.; Lu, D. Rethink Of Diabetes Treatment and Drug Development. Cell Dev. Biol. 2014, 3, e125. [Google Scholar]
- Tu, Y. Artemisinin-A Gift from Traditional Chinese Medicine to the World (Nobel Lecture). Angew. Chem. Int. Ed. Engl. 2016, 55, 10210–10226. [Google Scholar] [CrossRef]
- Bai, L.; Gao, J.; Wei, F.; Zhao, J.; Wang, D.; Wei, J. Therapeutic Potential of Ginsenosides as an Adjuvant Treatment for Diabetes. Front. Pharm. 2018, 9, 423. [Google Scholar] [CrossRef]
- Chen, W.; Balan, P.; Popovich, D.G. Chapter 6-Comparison of the ginsenoside composition of Asian ginseng (Panax ginseng) and American ginseng (Panax quinquefolius L.) and their transformation pathways. Stud. Nat. Prod. Chem. 2019, 63, 161–195. [Google Scholar]
- Yuan, H.D.; Kim, J.T.; Kim, S.H.; Chung, S.H. Ginseng and diabetes: The evidences from in vitro, animal and human studies. J. Ginseng Res. 2012, 36, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Shishtar, E.; Sievenpiper, J.L.; Djedovic, V.; Cozma, A.I.; Ha, V.; Jayalath, V.H.; Jenkins, D.J.; Meija, S.B.; de Souza, R.J.; Jovanovski, E.; et al. The effect of ginseng (the genus panax) on glycemic control: A systematic review and meta-analysis of randomized controlled clinical trials. PLoS ONE 2014, 9, e107391. [Google Scholar] [CrossRef] [PubMed]
- Gui, Q.F.; Xu, Z.R.; Xu, K.Y.; Yang, Y.M. The Efficacy of Ginseng-Related Therapies in Type 2 Diabetes Mellitus: An Updated Systematic Review and Meta-analysis. Medicine (Baltim.) 2016, 95, e2584. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.W.; Kang, S.M.; Vassy, J.L.; Shin, H.; Lee, Y.H.; Ahn, H.Y.; Choi, S.H.; Park, K.S.; Jang, H.C.; Lim, S. Efficacy and safety of ginsam, a vinegar extract from Panax ginseng, in type 2 diabetic patients: Results of a double-blind, placebo-controlled study. J. Diabetes Investig. 2012, 3, 309–317. [Google Scholar] [CrossRef]
- Park, S.H.; Oh, M.R.; Choi, E.K.; Kim, M.G.; Ha, K.C.; Lee, S.K.; Kim, Y.G.; Park, B.H.; Kim, D.S.; Chae, S.W. An 8-wk, randomized, double-blind, placebo-controlled clinical trial for the antidiabetic effects of hydrolyzed ginseng extract. J. Ginseng Res. 2014, 38, 239–243. [Google Scholar] [CrossRef]
- Kim, Y.K.; Yoo, D.S.; Xu, H.; Park, N.I.; Kim, H.H.; Choi, J.E.; Park, S.U. Ginsenoside content of berries and roots of three typical Korean ginseng (Panax ginseng) cultivars. Nat. Prod. Commun. 2009, 4, 903–906. [Google Scholar] [CrossRef]
- Dey, L.; Xie, J.T.; Wang, A.; Wu, J.; Maleckar, S.A.; Yuan, C.S. Anti-hyperglycemic effects of ginseng: Comparison between root and berry. Phytomedicine 2003, 10, 600–605. [Google Scholar] [CrossRef]
- Choi, H.S.; Kim, S.; Kim, M.J.; Kim, M.S.; Kim, J.; Park, C.W.; Seo, D.; Shin, S.S.; Oh, S.W. Efficacy and safety of Panax ginseng berry extract on glycemic control: A 12-wk randomized, double-blind, and placebo-controlled clinical trial. J. Ginseng Res. 2018, 42, 90–97. [Google Scholar] [CrossRef]
- Bang, H.; Kwak, J.H.; Ahn, H.Y.; Shin, D.Y.; Lee, J.H. Korean red ginseng improves glucose control in subjects with impaired fasting glucose, impaired glucose tolerance, or newly diagnosed type 2 diabetes mellitus. J. Med. Food 2014, 17, 128–134. [Google Scholar] [CrossRef]
- Oh, M.R.; Park, S.H.; Kim, S.Y.; Back, H.I.; Kim, M.G.; Jeon, J.Y.; Ha, K.C.; Na, W.T.; Cha, Y.S.; Park, B.H.; et al. Postprandial glucose-lowering effects of fermented red ginseng in subjects with impaired fasting glucose or type 2 diabetes: A randomized, double-blind, placebo-controlled clinical trial. BMC Complement. Altern. Med. 2014, 14, 237. [Google Scholar] [CrossRef]
- Cho, Y.H.; Ahn, S.C.; Lee, S.Y.; Jeong, D.W.; Choi, E.J.; Kim, Y.J.; Lee, J.G.; Lee, Y.H.; Shin, B.C. Effect of Korean red ginseng on insulin sensitivity in non-diabetic healthy overweight and obese adults. Asia Pac. J. Clin. Nutr. 2013, 22, 365–371. [Google Scholar] [PubMed]
- Kwon, D.H.; Bose, S.; Song, M.Y.; Lee, M.J.; Lim, C.Y.; Kwon, B.S.; Kim, H.J. Efficacy of Korean Red Ginseng by Single Nucleotide Polymorphism in Obese Women: Randomized, Double-blind, Placebo-controlled Trial. J. Ginseng Res. 2012, 36, 176–189. [Google Scholar] [CrossRef] [PubMed]
- Song, S.W.; Kim, H.N.; Shim, J.Y.; Yoo, B.Y.; Kim, D.H.; Lee, S.H.; Park, J.S.; Kim, M.J.; Yoo, J.H.; Cho, B.; et al. Safety and tolerability of Korean Red Ginseng in healthy adults: A multicenter, double-blind, randomized, placebo-controlled trial. J. Ginseng Res. 2018, 42, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, A.L.; Morgan, L.M.; Bishop, J.; Jovanovski, E.; Jenkins, D.J.A.; Vuksan, V. Co-administration of a konjac-based fibre blend and American ginseng (Panax quinquefolius L.) on glycaemic control and serum lipids in type 2 diabetes: A randomized controlled, cross-over clinical trial. Eur. J. Nutr. 2018, 57, 2217–2225. [Google Scholar] [CrossRef]
- Vuksan, V.; Xu, Z.Z.; Jovanovski, E.; Jenkins, A.L.; Beljan-Zdravkovic, U.; Sievenpiper, J.L.; Mark Stavro, P.; Zurbau, A.; Duvnjak, L.; Li, M.Z.C. Efficacy and safety of American ginseng (Panax quinquefolius L.) extract on glycemic control and cardiovascular risk factors in individuals with type 2 diabetes: A double-blind, randomized, cross-over clinical trial. Eur. J. Nutr. 2019, 58, 1237–1245. [Google Scholar] [CrossRef]
- Mucalo, I.; Jovanovski, E.; Vuksan, V.; Bozikov, V.; Romic, Z.; Rahelic, D. American Ginseng Extract (Panax quinquefolius L.) Is Safe in Long-Term Use in Type 2 Diabetic Patients. Evid. Based Complement. Altern. Med. 2014, 2014, 9168. [Google Scholar] [CrossRef]
- Park, E.Y.; Kim, H.J.; Kim, Y.K.; Park, S.U.; Choi, J.E.; Cha, J.Y.; Jun, H.S. Increase in Insulin Secretion Induced by Panax ginseng Berry Extracts Contributes to the Amelioration of Hyperglycemia in Streptozotocininduced Diabetic Mice. J. Ginseng Res. 2012, 36, 153–160. [Google Scholar] [CrossRef]
- Seo, E.; Kim, S.; Lee, S.J.; Oh, B.C.; Jun, H.S. Ginseng berry extract supplementation improves age-related decline of insulin signaling in mice. Nutrients 2015, 7, 3038–3053. [Google Scholar] [CrossRef]
- Kim, J.H.; Pan, J.H.; Cho, H.T.; Kim, Y.J. Black Ginseng Extract Counteracts Streptozotocin-Induced Diabetes in Mice. PLoS ONE 2016, 11, e0146843. [Google Scholar] [CrossRef]
- Song, B.; Ding, L.; Zhang, H.; Chu, Y.; Chang, Z.; Yu, Y.; Guo, D.; Zhang, S.; Liu, X. Ginsenoside Rb1 increases insulin sensitivity through suppressing 11beta-hydroxysteroid dehydrogenase type I. Am. J. Transl. Res. 2017, 9, 1049–1057. [Google Scholar]
- Tian, W.; Chen, L.; Zhang, L.; Wang, B.; Li, X.B.; Fan, K.R.; Ai, C.H.; Xia, X.; Li, S.D.; Li, Y. Effects of ginsenoside Rg1 on glucose metabolism and liver injury in streptozotocin-induced type 2 diabetic rats. Genet. Mol. Res. 2017, 16, gmr16019463. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Jung Yang, H.; Lee, I.S.; Kim, K.H.; Park, J.; Jeong, H.S.; Kim, Y.; Ahn, K.S.; Na, Y.C.; Jang, H.J. The aglycone of ginsenoside Rg3 enables glucagon-like peptide-1 secretion in enteroendocrine cells and alleviates hyperglycemia in type 2 diabetic mice. Sci. Rep. 2015, 5, 18325. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.S.; Jang, H.J.; Oh, M.Y.; Eom, D.W.; Kang, K.S.; Kim, Y.J.; Lee, J.H.; Ham, J.Y.; Choi, S.Y.; Wee, Y.M.; et al. Ginsenoside Rg3 enhances islet cell function and attenuates apoptosis in mouse islets. Transpl. Proc. 2014, 46, 1150–1155. [Google Scholar] [CrossRef] [PubMed]
- Karikura, M.; Miyase, T.; Tanizawa, H.; Taniyama, T. Studies on Absorption, Distribution, Excretion and Metabolism of Ginseng Saponins. VII. Comparison of the Decomposition Modes of Ginsenoside-Rb1 and -Rb2 in the Digestive Tract of Rats. Chem. Pharm. Bull. 1991, 39, 2357–2361. [Google Scholar] [CrossRef] [PubMed]
- Moon, H.-K.; Kim, K.-S.; Chung, S.-K.; Kim, J.-K. Effect of wild Korean ginseng (Panax ginseng) extract on blood glucose and serum lipid contents in rats with multiple low-dose streptozotocin-induced diabetes. Food Sci. Biotechnol. 2015, 24, 1505–1511. [Google Scholar] [CrossRef]
- Shishtar, E.; Jovanovski, E.; Jenkins, A.; Vuksan, V. Effects of Korean White Ginseng (Panax Ginseng C.A. Meyer) on Vascular and Glycemic Health in Type 2 Diabetes: Results of a Randomized, Double Blind, Placebo-controlled, Multiple-crossover, Acute Dose Escalation Trial. Clin. Nutr. Res. 2014, 3, 89–97. [Google Scholar] [CrossRef]
- Murthy, H.N.; Dandin, V.S.; Lee, E.J.; Paek, K.Y. Efficacy of ginseng adventitious root extract on hyperglycemia in streptozotocin-induced diabetic rats. J. Ethnopharmacol. 2014, 153, 917–921. [Google Scholar] [CrossRef]
- Nam, S.J.; Han, Y.J.; Lee, W.; Kang, B.; Choi, M.K.; Han, Y.H.; Song, I.S. Effect of Red Ginseng Extract on the Pharmacokinetics and Efficacy of Metformin in Streptozotocin-Induced Diabetic Rats. Pharmaceutics 2018, 10, 80. [Google Scholar] [CrossRef]
- Kim, H.Y.; Kim, K. Regulation of signaling molecules associated with insulin action, insulin secretion and pancreatic beta-cell mass in the hypoglycemic effects of Korean red ginseng in Goto-Kakizaki rats. J. Ethnopharmacol. 2012, 142, 53–58. [Google Scholar] [CrossRef]
- Hong, B.N.; Ji, M.G.; Kang, T.H. The efficacy of red ginseng in type 1 and type 2 diabetes in animals. Evid. Based Complement. Altern. Med. 2013, 2013, 593181. [Google Scholar] [CrossRef]
- Yoo, K.M.; Lee, C.; Lo, Y.M.; Moon, B. The hypoglycemic effects of American red ginseng (Panax quinquefolius L.) on a diabetic mouse model. J. Food Sci 2012, 77, H147–H152. [Google Scholar] [CrossRef] [PubMed]
- Kang, O.H.; Shon, M.Y.; Kong, R.; Seo, Y.S.; Zhou, T.; Kim, D.Y.; Kim, Y.S.; Kwon, D.Y. Anti-diabetic effect of black ginseng extract by augmentation of AMPK protein activity and upregulation of GLUT2 and GLUT4 expression in db/db mice. BMC Complement. Altern. Med. 2017, 17, 341. [Google Scholar] [CrossRef] [PubMed]
- Cheon, J.M.; Kim, D.I.; Kim, K.S. Insulin sensitivity improvement of fermented Korean Red Ginseng (Panax ginseng) mediated by insulin resistance hallmarks in old-aged ob/ob mice. J. Ginseng Res. 2015, 39, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.T.; Kim, H.B.; Lee, K.H.; Choi, Y.R.; Kim, H.J.; Shin, I.S.; Gyoung, Y.S.; Joo, S.S. Steam-dried ginseng berry fermented with Lactobacillus plantarum controls the increase of blood glucose and body weight in type 2 obese diabetic db/db mice. J. Agric. Food Chem. 2012, 60, 5438–5445. [Google Scholar] [CrossRef]
- Jeon, W.J.; Oh, J.S.; Park, M.S.; Ji, G.E. Anti-hyperglycemic effect of fermented ginseng in type 2 diabetes mellitus mouse model. Phytother. Res. 2013, 27, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.S.; Jo, K.; Kim, J.S.; Pyo, M.K.; Kim, J. GS-E3D, a new pectin lyase-modified red ginseng extract, inhibited diabetes-related renal dysfunction in streptozotocin-induced diabetic rats. BMC Complement. Altern. Med. 2017, 17, 430. [Google Scholar] [CrossRef]
- Saba, E.; Kim, S.H.; Kim, S.D.; Park, S.J.; Kwak, D.; Oh, J.H.; Park, C.K.; Rhee, M.H. Alleviation of diabetic complications by ginsenoside Rg3-enriched red ginseng extract in western diet-fed LDL(-/-) mice. J. Ginseng Res. 2018, 42, 352–355. [Google Scholar] [CrossRef]
- Yang, H.; Son, G.W.; Park, H.R.; Lee, S.E.; Park, Y.S. Effect of Korean Red Ginseng treatment on the gene expression profile of diabetic rat retina. J. Ginseng Res. 2016, 40, 1–8. [Google Scholar] [CrossRef]
- Sun, C.; Chen, Y.; Li, X.; Tai, G.; Fan, Y.; Zhou, Y. Anti-hyperglycemic and anti-oxidative activities of ginseng polysaccharides in STZ-induced diabetic mice. Food Funct. 2014, 5, 845–848. [Google Scholar] [CrossRef]
- Tsai, C.C.; Chan, P.; Chen, L.J.; Chang, C.K.; Liu, Z.; Lin, J.W. Merit of ginseng in the treatment of heart failure in type 1-like diabetic rats. Biomed. Res. Int. 2014, 2014, 484161. [Google Scholar] [CrossRef]
- Sen, S.; Chen, S.; Wu, Y.; Feng, B.; Lui, E.K.; Chakrabarti, S. Preventive effects of North American ginseng (Panax quinquefolius) on diabetic retinopathy and cardiomyopathy. Phytother. Res. 2013, 27, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.S.; Yin, H.J.; Guo, C.Y.; Huang, Y.; Xia, C.D.; Liu, Q. Influence of high blood glucose fluctuation on endothelial function of type 2 diabetes mellitus rats and effects of Panax Quinquefolius Saponin of stem and leaf. Chin. J. Integr. Med. 2013, 19, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Takamura, Y.; Nomura, M.; Uchiyama, A.; Fujita, S. Effects of Aerobic Exercise Combined with Panaxatriol Derived from Ginseng on Insulin Resistance and Skeletal Muscle Mass in Type 2 Diabetic Mice. J. Nutr. Sci. Vitam. 2017, 63, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Park, C.H.; Park, S.K.; Seung, T.W.; Kang, J.Y.; Ha, J.S.; Lee, D.S.; Lee, U.; Kim, D.O.; Heo, H.J. Ginsenoside Re Ameliorates Brain Insulin Resistance and Cognitive Dysfunction in High Fat Diet-Induced C57BL/6 Mice. J. Agric. Food Chem. 2017, 65, 2719–2729. [Google Scholar] [CrossRef] [PubMed]
- Yang, N.; Chen, P.; Tao, Z.; Zhou, N.; Gong, X.; Xu, Z.; Zhang, M.; Zhang, D.; Chen, B.; Tao, Z.; et al. Beneficial effects of ginsenoside-Rg1 on ischemia-induced angiogenesis in diabetic mice. Acta Biochim. Biophys. Sin. (Shanghai) 2012, 44, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.T.; Zhen, J.; Pang, B.; Gu, J.N.; Wu, S.S. Ginsenoside Rg1 ameliorates oxidative stress and myocardial apoptosis in streptozotocin-induced diabetic rats. J. Zhejiang Univ. Sci. B 2015, 16, 344–354. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Zhen, J.; Yang, Y.; Gu, J.; Wu, S.; Liu, Q. Ginsenoside Rg1 ameliorates diabetic cardiomyopathy by inhibiting endoplasmic reticulum stress-induced apoptosis in a streptozotocin-induced diabetes rat model. J. Cell Mol. Med. 2016, 20, 623–631. [Google Scholar] [CrossRef]
- Shen, J.; Zhao, Z.; Shang, W.; Liu, C.; Zhang, B.; Zhao, L.; Cai, H. Ginsenoside Rg1 nanoparticle penetrating the blood-brain barrier to improve the cerebral function of diabetic rats complicated with cerebral infarction. Int. J. Nanomed. 2017, 12, 6477–6486. [Google Scholar] [CrossRef]
- Lo, S.H.; Hsu, C.T.; Niu, H.S.; Niu, C.S.; Cheng, J.T.; Chen, Z.C. Ginsenoside Rh2 Improves Cardiac Fibrosis via PPARdelta-STAT3 Signaling in Type 1-Like Diabetic Rats. Int. J. Mol. Sci. 2017, 18, 1364. [Google Scholar] [CrossRef]
- Liu, Z.; Li, W.; Li, X.; Zhang, M.; Chen, L.; Zheng, Y.N.; Sun, G.Z.; Ruan, C.C. Antidiabetic effects of malonyl ginsenosides from Panax ginseng on type 2 diabetic rats induced by high-fat diet and streptozotocin. J. Ethnopharmacol. 2013, 145, 233–240. [Google Scholar] [CrossRef]
- Du, N.; Xu, Z.; Gao, M.; Liu, P.; Sun, B.; Cao, X. Combination of Ginsenoside Rg1 and Astragaloside IV reduces oxidative stress and inhibits TGF-beta1/Smads signaling cascade on renal fibrosis in rats with diabetic nephropathy. Drug Des. Dev. Ther. 2018, 12, 3517–3524. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Guo, G.; Xiao, J.; Sheng, X.; Zhang, X.; Tie, Y.; Cheng, Y.K.; Ji, X. Ginsenoside Rg3 stereoisomers differentially inhibit vascular smooth muscle cell proliferation and migration in diabetic atherosclerosis. J. Cell Mol. Med. 2018, 22, 3202–3214. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wu, W.; Wang, G.; Xu, W.; Zhang, F.; Wu, B.; Tian, Y. Protective effect of ginsenoside Rg3 on lung injury in diabetic rats. J. Cell Biochem. 2019, 120, 3323–3330. [Google Scholar] [CrossRef] [PubMed]
- Ha, T.S.; Lee, J.S.; Choi, J.Y.; Park, H.Y. Ginseng total saponin modulates podocyte p130Cas in diabetic condition. J. Ginseng Res. 2013, 37, 94–99. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lee, H.M.; Lee, O.H.; Kim, K.J.; Lee, B.Y. Ginsenoside Rg1 promotes glucose uptake through activated AMPK pathway in insulin-resistant muscle cells. Phytother. Res. 2012, 26, 1017–1022. [Google Scholar] [CrossRef]
- Gao, Y.; Yang, M.F.; Su, Y.P.; Jiang, H.M.; You, X.J.; Yang, Y.J.; Zhang, H.L. Ginsenoside Re reduces insulin resistance through activation of PPAR-gamma pathway and inhibition of TNF-alpha production. J. Ethnopharmacol 2013, 147, 509–516. [Google Scholar] [CrossRef]
- Siraj, F.M.; SathishKumar, N.; Kim, Y.J.; Kim, S.Y.; Yang, D.C. Ginsenoside F2 possesses anti-obesity activity via binding with PPARgamma and inhibiting adipocyte differentiation in the 3T3-L1 cell line. J. Enzym. Inhib. Med. Chem. 2015, 30, 9–14. [Google Scholar] [CrossRef]
- Yesmin Simu, S.; Ahn, S.; Castro-Aceituno, V.; Yang, D.C. Ginsenoside Rg5: Rk1 Exerts an Anti-obesity Effect on 3T3-L1 Cell Line by the Downregulation of PPARgamma and CEBPalpha. Iran. J. Biotechnol. 2017, 15, 252–259. [Google Scholar] [CrossRef]
- Reeds, D.N.; Patterson, B.W.; Okunade, A.; Holloszy, J.O.; Polonsky, K.S.; Klein, S. Ginseng and Ginsenoside Re Do Not Improve β-Cell Function or Insulin Sensitivity in Overweight and Obese Subjects With Impaired Glucose Tolerance or Diabetes. Diabetes Care 2011, 34, 1071–1076. [Google Scholar] [CrossRef]
- Liu, L.; Huang, J.; Hu, X.; Li, K.; Sun, C. Simultaneous determination of ginsenoside (G-Re, G-Rg1, G-Rg2, G-F1, G-Rh1) and protopanaxatriol in human plasma and urine by LC-MS/MS and its application in a pharmacokinetics study of G-Re in volunteers. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2011, 879, 2011–2017. [Google Scholar] [CrossRef]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).