







Lymphatics 2024, 2(1), 1-9; https://doi.org/10.3390/lymphatics2010001 - 1 Jan 2024
Viewed by 2896
Abstract
►
Show Figures
Radiation therapy is a key contributor to positive outcomes in hematological malignancies. However, this is contingent on minimizing the exposure of critical normal organs. The introduction of computed tomography (CT) for radiation treatment planning and the development of sophisticated dose calculation algorithms has
[...] Read more.
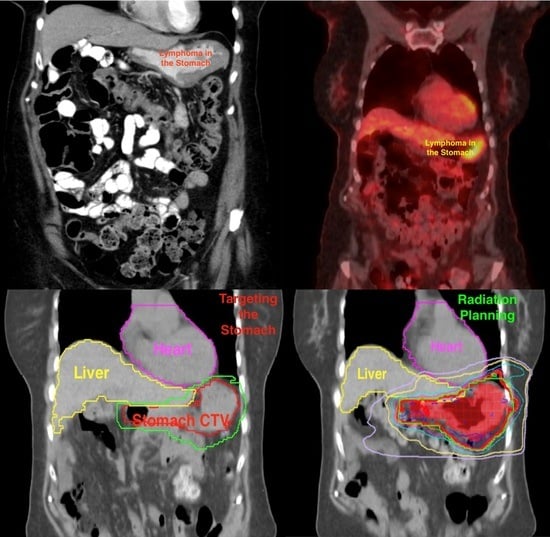
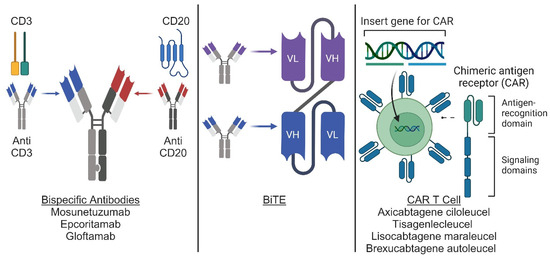
Radiation therapy is a key contributor to positive outcomes in hematological malignancies. However, this is contingent on minimizing the exposure of critical normal organs. The introduction of computed tomography (CT) for radiation treatment planning and the development of sophisticated dose calculation algorithms has transformed the radiation therapy field and made it possible to transition from conventional involved-field radiation to modern involved-site radiation therapy. Thanks to rapid advances in drug discovery, treatment strategies for many hematological malignancies have evolved to incorporate targeted and cellular therapies, in some cases even allowing the replacement of chemotherapy. As a result, new opportunities have been created for radiation to address relapses after more lines of therapy, identify disease-involving sanctuary sites, and bridge to the subsequent therapy. When considering radiation in patients receiving novel therapies, who may also be more heavily pretreated, respecting the critical and normal structures at all costs is imperative. In this document, we will describe modern techniques used to deliver state-of-the-art radiation therapy and practical considerations to ensure the accurate treatment of the target while avoiding normal organs at risk.
Full article
Graphical abstract
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}