





J. Cardiovasc. Dev. Dis. 2026, 13(4), 163; https://doi.org/10.3390/jcdd13040163 (registering DOI) - 9 Apr 2026
Abstract
Background: Risk stratification in patients with bicuspid aortic valve (BAV) and severe aortic stenosis (AS) remains challenging. Valvulo-arterial impedance (Zva), an integrated marker of global left ventricular (LV) afterload, has shown prognostic value in tricuspid AS; however, data in BAV are limited. This
[...] Read more.
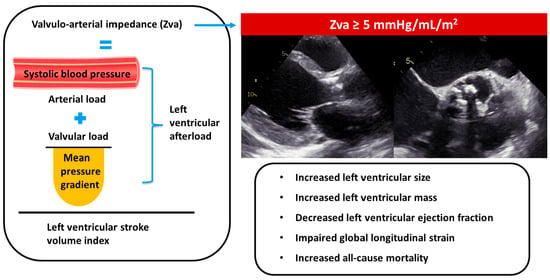
Background: Risk stratification in patients with bicuspid aortic valve (BAV) and severe aortic stenosis (AS) remains challenging. Valvulo-arterial impedance (Zva), an integrated marker of global left ventricular (LV) afterload, has shown prognostic value in tricuspid AS; however, data in BAV are limited. This study aimed to evaluate the association of Zva with LV remodeling, symptoms, and all-cause death in patients with BAV and severe AS. Methods: In this retrospective, two-center cohort study, 147 patients with severe AS and BAV were included. Zva was calculated at the time of the first echocardiographic diagnosis of severe AS. The study endpoint was all-cause mortality. Results: Over a median follow-up of 9.8 years, 24 patients (16%) died. A Zva threshold of 5 mmHg/mL/m2 was identified as optimal by ROC analysis. Patients with Zva ≥ 5 mmHg/mL/m2 showed higher mortality rates (29% vs. 10%; p = 0.003), more advanced symptoms (NYHA III-IV: 41% vs. 9%; p < 0.001), adverse LV remodeling, lower LVEF (60% (IQR 36–66) vs. 66% (IQR 61–71); p = 0.001), and worse LV global longitudinal strain (14.8% ± 2.7 vs. 16.5% ± 3.0; p = 0.016). Zva ≥ 5 mmHg/mL/m2 was independently associated with worse long-term survival after adjustment (HR 2.885; 95% CI 1.119–7.438; p = 0.028). Conclusions: Among patients with BAV and severe AS, an increased Zva was associated with more advanced symptoms, adverse LV remodeling, impaired LV systolic function, and worse long-term survival, and might therefore help in risk stratification of these patients.
Full article
(This article belongs to the Special Issue The Role of Echocardiography in Cardiovascular Diseases)
►
Show Figures
Graphical abstract


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}