


Neonatal Airway Management
A special issue of Children (ISSN 2227-9067). This special issue belongs to the section "Pediatric Neonatology".
Deadline for manuscript submissions: closed (25 April 2023) | Viewed by 32577
Special Issue Editor

Interests: quality and safety in neonatal airway management; focusing on intubation and unplanned extubation; newborn resuscitation; neonatal epidemiology
Special Issue Information
Dear Colleagues,
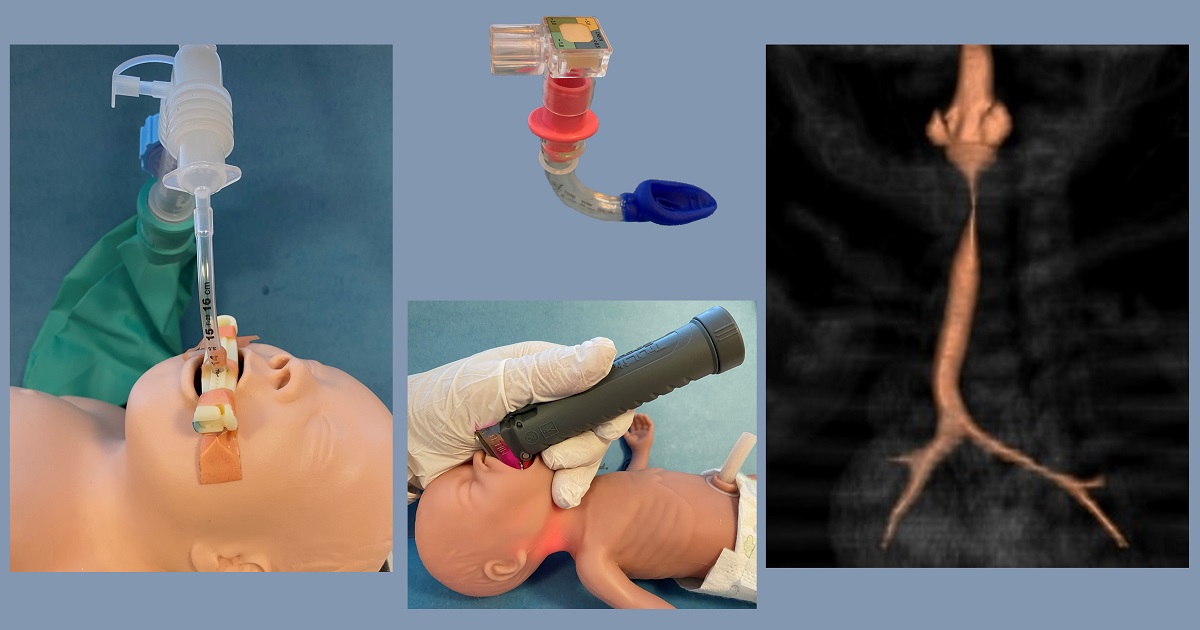
Neonates needing assisted ventilation often require an artificial airway. The normal neonatal airway is intrinsically difficult to manage due to its small dimensions and anatomical relationships, which also vary widely between extremely preterm and full-term newborns. Neonates are often physiologically unstable, and some have airway anomalies. Airway-management devices are typically designed for use in adults and are subsequently downsized for newborns. Consequently, tracheal intubation of neonates has a relatively low success rate, and it is associated with acute risks and long-term complications. Additionally, unplanned extubations occur more frequently in newborns than any other age group. These problems are currently addressed by single-center and collaborative efforts, using clinical research, quality improvement and patient safety methodologies. Finally, devices are being increasingly developed to support less-invasive respiratory support of neonates, and to facilitate airway management with reduced technical expertise required of neonatal caregivers.
This Special Issue of Children will address current topics in neonatal airway management, including normal and anomalous development and injury, tracheal intubation and its associated complications, as well as devices and techniques used in airway instrumentation. Original research, quality improvement reports, or review papers will be considered for publication. We look forward to receiving your individual or collaborative contributions on these topics.
Dr. Joaquim M. B. Pinheiro
Guest Editor
Manuscript Submission Information
Manuscripts should be submitted online at www.mdpi.com by registering and logging in to this website. Once you are registered, click here to go to the submission form. Manuscripts can be submitted until the deadline. All submissions that pass pre-check are peer-reviewed. Accepted papers will be published continuously in the journal (as soon as accepted) and will be listed together on the special issue website. Research articles, review articles as well as short communications are invited. For planned papers, a title and short abstract (about 250 words) can be sent to the Editorial Office for assessment.
Submitted manuscripts should not have been published previously, nor be under consideration for publication elsewhere (except conference proceedings papers). All manuscripts are thoroughly refereed through a single-blind peer-review process. A guide for authors and other relevant information for submission of manuscripts is available on the Instructions for Authors page. Children is an international peer-reviewed open access monthly journal published by MDPI.
Please visit the Instructions for Authors page before submitting a manuscript. The Article Processing Charge (APC) for publication in this open access journal is 2400 CHF (Swiss Francs). Submitted papers should be well formatted and use good English. Authors may use MDPI's English editing service prior to publication or during author revisions.
Keywords
- Neonatal airway development
- Neonatal intubation
- Difficult airways in newborns
- Intubation safety
- Endotracheal tubes
- Laryngeal mask/supraglottic airway devices
- Adverse events in neonatal ventilation
- Unplanned extubation
Benefits of Publishing in a Special Issue
- Ease of navigation: Grouping papers by topic helps scholars navigate broad scope journals more efficiently.
- Greater discoverability: Special Issues support the reach and impact of scientific research. Articles in Special Issues are more discoverable and cited more frequently.
- Expansion of research network: Special Issues facilitate connections among authors, fostering scientific collaborations.
- External promotion: Articles in Special Issues are often promoted through the journal's social media, increasing their visibility.
- Reprint: MDPI Books provides the opportunity to republish successful Special Issues in book format, both online and in print.
Further information on MDPI's Special Issue policies can be found here.