Abstract
Self-regulated learning (SRL) is a fundamental competence for academic transition and success in higher education, especially in health sciences, where autonomy and learning management are essential. This systematic review analyzed the relationship between SRL, academic performance, and student well-being among undergraduate health sciences students. Following the PRISMA protocol, 39 articles published between 2015 and 2025 on Web of Science, Scopus, and PubMed databases were selected. The consolidated sample consisted of 24,835 participants. The methodological quality of the selected studies was assessed using the Newcastle–Ottawa scale (NOS). A predominantly positive association was found between high levels of SRL and academic performance (GPA) (with correlation coefficients ranging from r = 0.11 to r = 0.55 in the primary studies). Furthermore, evidence from standardized self-report questionnaires in the reviewed literature indicates that several studies report female students showed higher levels of organization and planning, but these findings were not consistently observed across all studies. SRL acts as a key protective factor against stress, anxiety, and academic burnout. However, a “stagnation paradox” was identified: SRL skills do not always evolve linearly, often showing regression or stagnation in advanced clinical years due to the high cognitive load and insufficient support structure in those environments. Regarding sociodemographic variables, female students reported higher levels of planning and responsibility. SRL does not develop spontaneously with academic progress. Therefore, higher-education institutions must implement systematic and intentional pedagogical strategies from the early years of training to foster student well-being and the development of resilient professionals.
1. Introduction
Entering higher education involves a challenging academic transition [1] that demands adaptation from students due to the autonomy required by the process and the necessary higher cognitive skills [2]. Due to this, students are expected to be able to manage their learning, which will directly influence their ability to adapt to university life [3].
A suitable educational environment can foster the development of these skills that not all students have before entering university [4], so the concept of self-regulated learning or SRL in higher education has become relevant as a measure to promote essential skills, facilitating integration into university life, and improving academic performance [5].
The SRL is fundamental to the university process and to lifelong learning, essential for a more sustainable and equitable society [6,7].
SRL is defined as the conscious ability to direct one’s own learning behavior [8], constituting a dynamic and self-directed process where control resides in the student for the development of academic skills [9,10].
SRL encompasses cognitive, motivational, and affective factors, involving self-generated thoughts, feelings, and behaviors oriented towards achieving a purpose [11]. Its objective is for students to actively participate in their learning process, setting goals and strategies based on external and internal resources [12].
The development of SRL generates better academic performance by being a specific process that must be adapted to each task, and not an intrinsic personal trait [11,12].
Within the SRL process, certain transversal characteristics can be described, which would be:
- SRL is dynamic, dependent on the academic environment, and can be controlled by the student. Therefore, learning skills can be acquired over time [13].
- The student has an active role in the SRL, managing their academic training instead of being a passive recipient [3].
- External factors (academic and social context) and internal (executive functions and motivation) influence the development of SRL and can be regulated by students. The university environment and interaction with peers/professors favor SRL [3,5,14].
- The development of the SRL is imperative for continuous learning and professional performance, since its skills transcend the academic [3,5].
- The motivational and strategic components of SRL can be measured quantitatively using standardized instruments [3].
Two SRL models stand out. The first is proposed by Zimmerman [12], which proposes three cyclical phases: (i) planning: analysis of the task, goals, resources, and self-motivation; (ii) performance: self-control, application of strategies and self-observation, recording actions and time spent; and (iii) self-reflection: self-evaluation of the process and emotional analysis.
On the other hand, Pintrich postulates a similar model with four cyclical phases [11] (i) planning: review of objectives, goal orientation, time planning, perceptions of difficulty and academic context; (ii) monitoring: metacognition of the process, motivation, effort, use of time and need for help; (iii) control: review of the effectiveness of cognitive and metacognitive strategies and volitional control used to adjust strategies; and (iv) reaction–reflection: self-evaluation of the effectiveness of the strategies used.
Although there are similarities, both authors agree that SRL is a cyclical and dynamic process, whose phases are not necessarily sequential and can occur in parallel [11,12].
SRL plays a fundamental role in higher education because it predicts better academic performance and grades [15,16]. It facilitates the transition and adaptation to university life, increasing satisfaction and acting as a protective factor against dropout [7]. Moreover, it fosters higher-order thinking skills and empowers students to autonomously manage their educational process, promoting motivation, self-efficacy, and proactive behavior [9]. This autonomy positively influences well-being, where time management is a protective factor against academic burnout [1]. Finally, SRL contributes to holistic development by fostering transversal skills such as critical thinking and strategic learning [2]. Therefore, SRL is fundamental to academic performance, adaptation to the university environment, and comprehensive professional development.
Also, following global trends in Curriculum harmonization, such as the Credit System in Latin America, the aim is to measure and harmonize student workload, declaring hours of direct instruction and independent work for the achievement of Expected Learning Outcomes and the Graduate Profile. This regulated context highlights the importance of students developing adequate SRL.
SRL is crucial for student well-being, acting as a protective factor against depression, stress, anxiety, and burnout [17]. SRL is negatively correlated with depression, promoting coping with stress [18] and contributing to its management [19]. Additionally, it reduces anxiety by facilitating clinical decision-making, where poor performance is associated with increased stress and SRL difficulties [20]. Similarly, SRL prevents burnout [1], while low academic well-being negatively impacts SRL, professional identity, and burnout in students [21]. In summary, SRL is essential for preventing these problems and for successful university adjustment.
Empirical evidence points to the critical importance of SRL in university students and the need for its systematic development from the beginning of their studies. Implementing early SRL pedagogical strategies and support programs would improve academic performance and curricular progress, while also acting as a preventative measure against demotivation, stress, and dropout. Therefore, promoting SRL is essential to foster persistence, successful completion of studies, and development of competent professionals.
Despite the evidence, SRL models in health sciences require special attention due to the theoretical-practical nature of their training. Understanding how SRL is integrated into these programs, considering curricular variability, is crucial to mitigate academic risks and ensure student well-being and adequate professional training. Therefore, this systematic review analyzed the relationship between SRL, academic performance, and student well-being among undergraduate health sciences students.
Understanding this phenomenon is highly relevant in the current academic panorama to design effective educational interventions. Therefore, to address this gap, this systematic review analyzed the relationship between SRL, academic performance, and student well-being. To achieve this goal, we implemented a rigorous systematic search strategy following PRISMA guidelines across Web of Science, Scopus, and PubMed, aiming to synthesize the most current evidence and provide a clear overview for future educational policies.
2. Methods
2.1. Design and Sources of Information
This systematic review, conducted according to the 2020 PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [22], examined the relationship between SRL, academic performance, and student well-being among undergraduate health sciences students. Systematic searches were performed in three broad-spectrum academic databases—Web of Science, Scopus, and PubMed—selected for their comprehensive coverage of the social science, education, psychology, and health. The final search was completed on 30 July 2025. In addition, the reference lists of included studies were manually reviewed to identify potentially relevant publications that were not captured by the automated search. This systematic review was not registered in PROSPERO. A formal protocol was not prepared; however, the review strictly adhered to PRISMA 2020 guidelines.
A ten-year time frame (2015–2025) was defined for the analysis to capture current and robust empirical evidence while avoiding biases arising from the COVID-19 lockdown period. This context significantly altered teaching and learning processes and patterns of SRL in students [23], which could affect the comparative validity of the results. This methodological decision aligns with the recommendations of the PRISMA framework, which allows for defining the search period whenever there is a clear theoretical and contextual justification [22].
2.2. Search Strategy
The literature search was carried out in accordance with the PRISMA protocol (see Figure 1) for systematic reviews and meta-analyses [22]. Searches were conducted across each database using the title, abstract, and keyword fields of every article. The following keywords were combined with Boolean operators (OR/AND): [(“academic self-regulation” OR “academic self regulation” OR “self-regulated learning”) AND (“Health students” OR “Healthcare students” OR “Health professions students” OR “medical students” OR “nursing students” OR “allied health students”)].
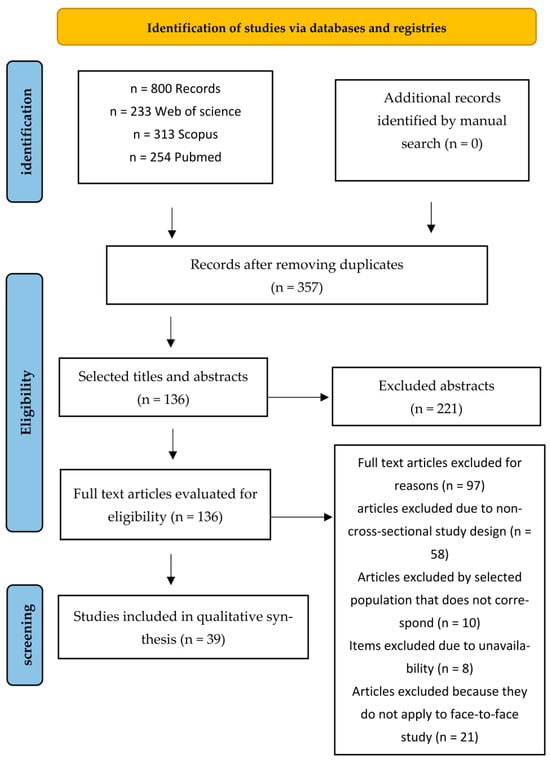
Figure 1.
Search strategy for selected studies.
2.3. Eligibility Criteria
Before reviewing the full content of each article, the titles and abstracts were checked for relevance. The initial screening of titles and abstracts was conducted manually and independently by the authors, without the use of artificial intelligence assistants. Reference management software Mendeley (version 2.142.0) was used to detect and eliminate duplicates. The process of reading and filtering titles and abstracts took approximately six months.
Studies were selected based on the following criteria: (1) cross-sectional design; (2) study population comprising undergraduate health sciences students; (3) studies conducted with students attending face-to-face classes; and (4) studies written in English and Spanish.
The following exclusion criteria were established: (1) exclusively qualitative studies; (2) postgraduate or medical specialty students; (3) studies where the SRL variable was not directly related to the central focus of the study, and (4) studies with students attending online or hybrid classes. The extraction process was carried out independently by two reviewers, and a third reviewer acted as an external verifier in case of disagreement. Discrepancies were resolved through discussion and consensus.
Qualitative studies were excluded because this review aimed to synthesize quantitative evidence on the statistical link between self-regulated learning (SRL) and academic performance and well-being outcomes. Although valuable for understanding SRL experiences, qualitative studies do not offer the effect estimates needed for quantitative comparison across different studies.
2.4. Quality Assessment
The Newcastle–Ottawa Scale (NOS), modified for cross-sectional studies, was employed to assess the study quality [24]. NOS assesses quality by examining content, structure, and interpretation, demonstrating high reliability and validity, and performing better than other scales. Its main dimensions include outcomes, comparability, and selection. Seven categories evaluate aspects such as sample representativeness, justification for sample size, comparability between respondents and non-respondents, exposure estimates, comparability based on study design or analysis, the evaluation of results, and the adequacy of statistical analysis.
If the study satisfies these criteria, a maximum of ten stars can be awarded overall. Up to three stars are allocated for the selection dimension, four stars for comparability, and three stars for the outcome dimension [24].
However, it is important to acknowledge that NOS has certain limitations: it was initially designed for observational studies, which may lead to some subjectivity when applying it to different study designs. To address this, two independent reviewers evaluated each article, and in cases of disagreement, a third researcher reviewed the article.
3. Results
3.1. Search Results
Eight hundred (800) articles were found related to how SRL relates to the academic process of health sciences students. Of these, 443 were discarded as duplicates, and 221 were discarded after reviewing their titles and abstracts. Out of 136 full-text articles evaluated for eligibility, 97 were excluded. The main reasons for exclusion were non-cross-sectional study designs (n = 58), populations other than undergraduate health sciences students (n = 10), not applying a face-to-face modality (n = 21), and inadequate outcome data (n = 8).
3.2. Characterization of the Articles
The details of the articles and the results of this review are organized in Table 1. The sample sizes of the 39 articles range from 23 to 6546, totaling 24,835 participants across all the scientific articles analyzed. Additionally, the 39 articles were developed in different countries around the world: China (n = 7), Turkey (n = 6), the Netherlands (n = 5), Canada (n = 4), Iran (n = 3), Pakistan (n = 3), Saudi Arabia (n = 2), Australia (n = 2), USA (n = 3), Chile (n = 1), Indonesia (n = 1), Malaysia (n = 1) and Singapore (n = 1) (Figure 2).

Table 1.
Summary of Selected Works.
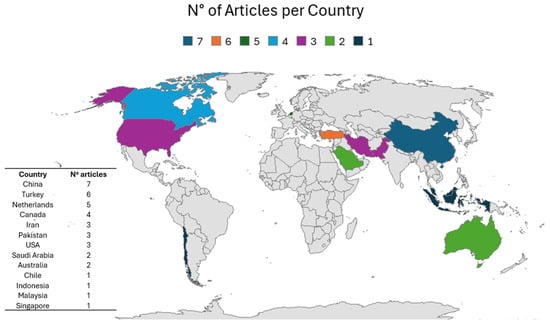
Figure 2.
Distribution of the 39 articles obtained from the PRISMA protocol.
Based on the results of this review (see Table 1), it was possible to identify five central themes associated with SRL in the academic training of university students in the health field.
Due to variations in study design, measurement instruments for SRL, and how outcomes were reported, a meta-analysis was not conducted. Instead, results were summarized through a structured narrative, categorizing studies by outcome domains like academic performance, psychological well-being, and sociodemographic factors, and describing the direction and strength of the associations found.
- 1.
- Relationship between SRL and Academic Performance
There is substantial evidence suggesting a predominantly positive association between SRL skills and the academic performance of health sciences students. Numerous studies report that students with higher Grade Point Average (GPA) scores perform significantly higher on SRL strategies and executive functions [3,25,58]. Moreover, students’ profiles characterized by high SRL and low-test anxiety have been reported to be associated with optimal academic performance [60].
While the evidence is extensive on this point, it is not uniform. Some studies did not find a significant direct association between SRL levels and GPA [36,44] or only found isolated components of SRL, such as effort regulation, that predicted academic performance in higher grades [27]. Furthermore, key mediating variables such as sense of coherence [28] and self-efficacy [43] were identified.
- 2.
- Sociodemographic Variables and Curriculum Evolution
When analyzing demographic variables, a consistent gender trend is observed, where female students frequently obtain better SRL results globally or in sub-areas such as planning and accountability, compared to male students [26,46,50], although this difference was not statistically significant in all cultural contexts analyzed [30,35]; however, findings were not entirely consistent across all included studies.
A key finding relates to the evolutionary trajectory of SRL throughout the student training process. Contrary to expectations, multiple students report a stagnation or even a decline in SRL-related skills among upper-year students compared to first-year students [29,33]. This negative trend is observed primarily in the dimensions of metacognition and help-seeking [31], which could be explained by the fact that advanced courses or clinical immersion may slow down or even inhibit the continued development of autonomy in learning.
- 3.
- Psychological Determinants: Self-efficacy, Motivation, and Emotion
Personal factors emerge as strong predictors of self-regulated behavior. Self-efficacy demonstrates a strong positive correlation with SRL capacity [48,57], frequently acting as a necessary precursor of the adoption of effective learning strategies. Intrinsic motivation, achievement orientation, and a defined professional identity also facilitate high levels of SRL [21,40,47].
However, the affective dimension plays an important regulatory role. Positive academic emotions promote the development of SRL [57], while unstable emotional variability has been negatively linked to performance in clinical reasoning [21]. Additionally, high levels of SRL act as a protective factor because they are associated with lower levels of stress and higher levels of student well-being [60].
- 4.
- Influence of the Educational Environment and Cognitive Load
The educational context exerts a decisive influence on the quality of SRL. Effective teacher feedback and a pedagogical atmosphere that meets basic psychological needs are strong predictors of the development of SRL [49,61]. On the other hand, clinical settings are often perceived as lacking in support, which hinders participation in active learning [32].
In line with the above, the characteristics of the activities moderate the self-regulatory response. Experimental and microanalysis studies indicate that cognitive load and task complexity can alter SRL processes, promoting analytical reasoning but negatively affecting the self-reflection phase and diagnostic efficiency [53,54]. This underscores the importance of designing academic activities that balance cognitive challenge with appropriate instructional support.
- 5.
- Profiles of Microanalytical Strategies and Processes
When the components of SRL are analyzed individually, a disparity is observed among health science students. On the one hand, reflection and task evaluation strategies generally show high scores [34], while frequent deficiencies are observed in critical skills such as planning, metacognitive monitoring, and seeking help [37,52,56].
Studies employing microanalysis methodologies show that, during clinical problem-solving, students frequently fail to adapt their strategies after making mistakes or do not employ higher-order reasoning processes in the planning phase [42,56]. However, specific methodologies such as the flipped classroom have demonstrated potential for improving collaborative strategies such as peer learning [39].
3.3. Analysis of Methodological Quality
Table 2 shows the results of the methodological quality analysis of the studies. Overall, the quality of the studies was satisfactory, with an average of 5.46 stars. The weakest point examined was the selection process, as most of the analyzed studies exhibited weaknesses stemming from their sample collection methods: most were non-probability, convenience, or snowball sampling methods. The highest score was seven stars, where eight articles obtained this score [21,31,38,42,47,50,60,62], and the lowest score was two stars with two works with this score [34,44].
Table 2.
Analysis of the Quality of the Articles.
4. Discussion
39 scientific studies that met the established inclusion criteria were analyzed, encompassing a cumulative sample of 24,835 undergraduate health sciences students. These cross-sectional studies were published between 2015 and 2025 and predominantly used standardized instruments such as the MSLQ, SRLPS, and SRLS-CNP to assess SRL. The evidence shows remarkable geographical diversity, with studies from 13 countries, notably China (n = 7), Turkey (n = 6), the Netherlands (n = 5), and Canada (n = 4). However, a limited representation of research from Latin American contexts was identified, with only one study conducted in Chile, highlighting a significant gap in regional scientific output. This finding opens a critical opportunity for future research in Latin America, where the study of SRL in health sciences students is still not sufficiently developed, despite its potential impact on improving academic performance and student well-being.
Regarding SRL, a consistent trend is observed with respect to gender, suggesting that female students exhibit higher level of SRL compared to males, which could be explained because women present a greater sense of responsibility and commitment to their training than men [26,44,50,63], as well as the fact that women show more goal-setting strategies, responsibility and planning, because it has been seen that they take better ownership of their training process. However, it is important to note that the gender gap is not universal across all the cultural environments analyzed, suggesting that contextual factors may mediate this relationship [30,35]. Beyond gender, other sociodemographic factors emerge as conclusive indicators of SRL behavior. Variables such as pre-university education, parents’ educational level, household income, and prior participation in occupational risk prevention training significantly influence students’ self-management skills [58]. Additionally, significant differences exist between students from different types of institutions, with public students reporting higher levels of SRL than private university students. This could be explained by two structural factors: (i) differences in admission requirements, given that public institutions tend to have more competitive selection processes, attracting students with strong academic profiles and a greater prior development of autonomy [59]. Therefore, it is suggested that SRL is not only an individual process but is directly influenced by cultural capital and the opportunities for advancement offered by the student’s socio-educational environment.
Undoubtedly, one of the most counterintuitive findings of this systematic review was the “stagnation paradox” in the development of SRL among health sciences students in their final years of study. Contrary to expectations that academic maturation would strengthen SRL competencies as students’ progress through their studies, the evidence shows that these skills do not develop linearly and may even regress during the preclinical and clinical stages [29]. Consistently, a significant decrease or even a high level of decline was observed in key dimensions such as time management, help-seeking, and metacognition in senior students compared to first-year [31,33].
This phenomenon suggests that the traditional organization of health training may be acting as an inhibitor of higher-order processes. To interpret this, the interaction between curriculum design and the demands of the clinical environment could be analyzed through the lens of cognitive load theory, which posits that working memory saturation prevents the activation of metacognitive processes [64]. Therefore, the progressive increase in the complexity of clinical tasks could not only affect diagnostic efficiency but also critically reduce the frequency of self-reflexive behaviors [54]. Moreover, when faced with highly demanding tasks, students prioritize immediate analytical reasoning to solve problems, neglecting the monitoring and evaluation processes of their own performance, which are fundamental components of self-reflective learning [53].
In addition, students often perceive clinical practice settings as spaces with little or no teaching support, which influences their ability to actively participate in their own learning [32]. This lack of external structure at preclinical and clinical levels could hinder the development of the autonomy required to complete the SRL cycle.
While more advanced students possess greater theoretical knowledge, they exhibit a notable deficiency in their ability to adapt strategies after making mistakes. Microanalytical evidence shows that less than 10% of students in clinical settings indicate that they would adjust their reasoning process in the face of future difficulties, revealing shortcomings in higher-order processes during planning [42,56].
Moreover, professional identity is positively correlated with student well-being, where SRL acts as a critical mediator in this relationship [21]. However, if SRL levels decrease, academic well-being is compromised, increasing the risk of stress and burnout, especially in the final stages of academic studies [21,60].
Therefore, the development of SRL in health science students does not evolve spontaneously, and the stagnation reported in this review highlights the need to include strategies such as the flipped classroom, which has shown satisfactory results with respect to academic performance and student satisfaction [65], and support programs that provide proper continuous development throughout professional training, to prevent the demands of the clinical environment from stifling the student’s reflective capacity.
The evidence found in this systematic review confirms that SRL promotes academic success and is a fundamental pillar for the mental health of healthcare students. A close relationship has been described where developing strategies that promote SRL act as a protective factor against the prevalence of symptoms associated with depression, stress, burnout, and anxiety [17]. In healthcare students, SRL shows a negative correlation with depression, explained by the strengthening of resilience mechanisms against stressors in the academic environment [18].
This mitigating effect occurs through various psychological and operational mechanisms identified in the analyzed studies. The first is a negative correlation between stress and SRL skills, where increased levels of perceived stress are associated with a decrease in students’ ability to develop SRL skills [19]. Furthermore, the development of SRL facilitates clinical decision-making, directly contributing to a reduction in student anxiety levels [20]. Additionally, adopting SRL strategies, such as time management, acts as a protective factor against burnout in university students [1] and even students characterized by high levels of SRL report very low levels of stress compared to those with low or even moderate metacognitive skills [60]. Similarly, academic well-being has been identified as directly influencing a student’s SRL-regulation capacity, impacting the construction of their professional identity [21]. Low levels of well-being can lead to cycles of low SRL, resulting in emotional exhaustion and difficulties in developing a professional identity [21]. Finally, self-efficacy emerges as a necessary precursor for the incorporation of effective academic strategies, demonstrating that as students’ confidence in their abilities is fostered, their SRL levels increase [48,57].
As a result, the importance of intentionally promoting the development of SRL skills from the early years of university becomes evident. This proactive approach, in addition to optimizing the educational process and curricular progress, acts as a strong protective factor against demotivation and academic dropout in demanding contexts [5,9]. Consequently, facilitating SRL is a vital strategy for developing resilient, competent healthcare professionals with enhanced adaptability skills required in higher education.
The results are conclusive regarding the predominantly positive relationship between SRL skills and the academic performance of healthcare students. A large corpus of evidence suggests that high-achieving students exhibit higher levels of SRL strategy use and greater proficiency in key executive functions such as monitoring and cognitive flexibility [3,25,58]. Additionally, profiles with high SRL capacity and low-test anxiety are reported to be associated with positive academic outcomes [60]. In this regard, a student’s ability to consciously guide their own study is fundamental, especially when control of the learning process rests with the student [10].
However, it is important to highlight that this relationship is not consistent across the analyzed literature. Some studies found no direct or significant relationship between SRL scores and academic success [36,44]. In other contexts, only specific components proved to be predictors of academic performance in later stages of the curriculum [27]. This inconsistency could be explained by the fact that the influence of SRL on grades is not linear, but rather conditioned by critical mediating variables identified in this study, such as self-sufficiency and sense of coherence [28,43]. In line with the above, self-efficacy has a preeminent precursor role in enabling students to implement effective learning strategies and achieve higher academic goals [40,48].
5. Strengths and Limitations
First, the PRISMA protocol was strictly followed to ensure transparency and replicability of the process [22]. The inclusion of 39 scientific studies allowed for the consolidation of a robust sample of 24,835 participants, providing robust statistical representativeness. Likewise, geographical diversity was achieved across multiple countries on different continents, enabling a global and transcultural perspective on the phenomenon of SRL in healthcare students (13 countries included). Finally, the Newcastle–Ottawa scale (NOS) was used for the standardized assessment of methodological quality, identifying critical gaps in the current literature [24].
The main strength of this study is that it constitutes one of the few, if not the first, systematic review that integrates and consolidates the evidence on SRL in students from different healthcare disciplines, going beyond previous reviews focused exclusively on medicine and nursing. This multidisciplinary approach allows the findings on the “stagnation paradox” to be generalized across different disciplines within the field. Additionally, the cumulative sample of 24,835 participants from 13 different countries provides adequate robustness with respect to the medical education literature, along with cross-cultural diversity of the data, strongly suggesting that the decline in SRL during clinical rotations is not an isolated finding, but rather a global systemic pattern.
Among the main limitations of this systematic review is the fact that all the included studies employed a cross-sectional design, which limits the possibility of establishing causal relationships between SRL and the variables analyzed. Also, this review did not include qualitative studies; despite the importance of these studies, they did not provide measurable and/or comparable data about the phenomenon. Longitudinal studies were not included to ensure methodological homogeneity and reduce the variability that could occur in such designs. Moreover, the overall methodological quality of the studies was rated as moderate, reinforcing the need for future research with more robust designs, such as longitudinal or quasi-experimental studies. Finally, it is worth noting that the studies relied on self-reported instruments, which may introduce biases associated with participants’ subjective perceptions and limit the external validity of the findings.
6. Conclusions
In conclusion, this systematic review synthesized evidence from 39 studies using rigorous selection criteria focused on undergraduate health sciences students across multiple global contexts. Going beyond a mere listing of findings, the integrated evidence demonstrates that SRL is a critical input that transcends academic performance, serving as an essential pillar for adapting to university life, student well-being, and the comprehensive training of healthcare professionals. It also confirms that high levels of SRL are associated with better academic performance and act as a protective factor against stress, anxiety, and burnout, especially in highly demanding environments.
However, the results revealed a “stagnation paradox”, because we suggest SRL skills may not develop spontaneously with academic progress, even declining in later years due to increased cognitive load and lack of institutional support in clinical settings. This highlights the need to develop SRL intentionally, systematically, and from the early years of the program.
In conclusion, universities in the healthcare field must implement teaching strategies that balance academic challenges with effective faculty support. Promoting lifelong learning is not only a measure to improve academic performance, but also a comprehensive way to ensure retention, well-being, and the development of competent and resilient professionals prepared for lifelong learning.
Author Contributions
Conceptualization, C.A.V. and J.M.-L.; methodology, C.A.V. and J.M.-L.; software, C.A.V. and J.M.-L.; validation C.A.V. and J.M.-L.; formal analysis, C.A.V. and J.M.-L.; investigation, C.A.V. and J.M.-L.; resources, not applicable; data curation, C.A.V. and J.M.-L.; writing—original draft preparation, C.A.V. and J.M.-L.; writing—review and editing, C.A.V. and J.M.-L.; visualization, C.A.V. and J.M.-L.; supervision, C.A.V. and J.M.-L.; project administration, C.A.V. and J.M.-L.; funding acquisition, not applicable. All authors have read and agreed to the published version of the manuscript.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare that they have no conflicts of interest in writing this article.
References
- Barbosa, J.; Silva, Á.; Ferreira, M.A.; Severo, M. Transição do ensino secundário para a escola médica: O papel do tempo de estudo e das competências de autorregulação da aprendizagem no burnout académico. Acta Medica Port. 2016, 29, 803–808. [Google Scholar] [CrossRef] [PubMed]
- Dinh, C.T.; Phuong, H.Y. Teaching Self-Regulated Learning Strategies on Efl Students in Moocs: A Case Study in Vietnam. Turk. Online J. Distance Educ. 2025, 26, 101–121. [Google Scholar] [CrossRef]
- Lepe-Martínez, N.; Pinochet-Quiroz, P.; Gálvez-Gamboa, F.; Moreno-Cerda, M.; Tapia-Castro, Y.; Durán-González, E. Executive functions and management of self-regulated learning in medical and health care students. Investig. Educ. Medica 2024, 13, 26–36. [Google Scholar] [CrossRef]
- Chan, K.M.; Tse, S.K. Graduate Attributes: Modelling the Roles of Teaching, Learning, and Communicative Factors. Creat. Educ. 2025, 16, 1017–1039. [Google Scholar] [CrossRef]
- Inzunza Melo, B.C.; Márquez Urrizola, C.; Villalobos Pérez, C. Relationship Between Self-Regulated Learning, Academic Antecedents and Sociodemographic Characteristics in Medical Students. Educación Médica Superior [Internet]. 2020. Available online: https://www.medigraphic.com/cgi-bin/new/resumenI.cgi?IDARTICULO=96950 (accessed on 26 January 2026).
- Mejeh, M.; Rehm, M. Taking adaptive learning in educational settings to the next level: Leveraging natural language processing for improved personalization. Educ. Technol. Res. Dev. 2024, 72, 1597–1621. [Google Scholar] [CrossRef]
- Theobald, M. Self-regulated learning training programs enhance university students’ academic performance, self-regulated learning strategies, and motivation: A meta-analysis. Contemp. Educ. Psychol. 2021, 66, 101976. [Google Scholar] [CrossRef]
- Wesselborg, B. Enhancing of self-regulated learning strategies for health care students to improve e-learning in the “Corona semester” as an interdisciplinary task. J. Med. Educ. 2020, 37, Doc76. [Google Scholar] [CrossRef]
- Lee, H.Y.; Chen, P.H.; Wang, W.S.; Huang, Y.M.; Wu, T.T. Empowering ChatGPT with guidance mechanism in blended learning: Effect of self-regulated learning, higher-order thinking skills, and knowledge construction. Int. J. Educ. Technol. High. Educ. 2024, 21, 16. [Google Scholar] [CrossRef]
- Ng, D.T.K.; Tan, C.W.; Leung, J.K.L. Empowering student self-regulated learning and science education through ChatGPT: A pioneering pilot study. Br. J. Educ. Technol. 2024, 55, 1328–1353. [Google Scholar] [CrossRef]
- Pintrich, P.R. A Conceptual Framework for Assessing Motivation and Self-Regulated Learning in College Students. Educ. Psychol. Rev. 2004, 16, 385–407. [Google Scholar] [CrossRef]
- Zimmerman, B.J. Becoming a self-regulated learner: An overview. In Theory into Practice; Ohio State University Press: Columbus, OH, USA, 2002; pp. 64–70. [Google Scholar] [CrossRef]
- Daura, F.T. Self-Regulated Learning and Academic Achievement among Students in the Clinical Cycle of their Medical Degree. Rev. Electrón. Investig. Educ. 2015, 17, 28–45. [Google Scholar]
- Parra-Esquivel, E.I.; Peñas-Felizzola, O.L.; Gómez-Galindo, A.M. Virtual objects for self-regulated learning of occupational therapy students. Rev. Salud Pública 2017, 19, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Allen, J.L.; Hesketh, T. The influence of individual, peer, and family factors on the educational aspirations of adolescents in rural China. Soc. Psychol. Educ. 2023, 26, 735–759. [Google Scholar] [CrossRef] [PubMed]
- Feraco, T.; Resnati, D.; Fregonese, D.; Spoto, A.; Meneghetti, C. An integrated model of school students’ academic achievement and life satisfaction. Linking soft skills, extracurricular activities, self-regulated learning, motivation, and emotions. Eur. J. Psychol. Educ. 2022, 38, 109–130. [Google Scholar] [CrossRef]
- Martínez-Líbano, J.; Torres-Vallejos, J.; Oyanedel, J.C.; González-Campusano, N.; Calderón-Herrera, G.; Yeomans-Cabrera, M.M. Prevalence and variables associated with depression, anxiety, and stress among Chilean higher education students, post-pandemic. Front. Psychiatry 2023, 14, 1139946. [Google Scholar] [CrossRef]
- Van Nguyen, H.; Laohasiriwong, W.; Saengsuwan, J.; Thinkhamrop, B.; Wright, P. The relationships between the use of self-regulated learning strategies and depression among medical students: An accelerated prospective cohort study. Psychol. Health Med. 2015, 20, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Marsch, S.; Yanagida, T.; Steinberg, E. Workplace learning: The bidirectional relationship between stress and self-regulated learning in undergraduates. BMC Med. Educ. 2024, 24, 1038. [Google Scholar] [CrossRef] [PubMed]
- Bektas, I.; Kudubes, A.A.; Ayar, D.; Bektas, M. The level of nursing students’ self-regulated learning and academic locus of control predicting self-confidence and anxiety in clinical decision-making. Nurse Educ. Today 2025, 148, 106629. [Google Scholar] [CrossRef] [PubMed]
- Zhouchen, Y.B.; Wang, S.Y.; Shen, S.L.; Zhou, Y.T.; Redding, S.R.; Ouyang, Y.Q. Impact of professional identity on learner well-being of undergraduate nursing students of “double tops” universities: Mediating effect of self-regulated learning. Nurse Educ. Today 2024, 143, 106382. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Lobos, K.; Cobo-Rendón, R.; Jofré, D.B.; Santana, J. New challenges for higher education: Self-regulated learning in blended learning contexts. Front. Educ. 2024, 9, 1457367. [Google Scholar] [CrossRef]
- Gualdi-Russo, E.; Zaccagni, L. The Newcastle–Ottawa Scale for Assessing the Quality of Studies in Systematic Reviews. Publications 2026, 14, 4. [Google Scholar] [CrossRef]
- Jouhari, Z.; Haghani, F.; Changiz, T. Assessment of medical students’ learning and study strategies in self-regulated learning. J. Adv. Med. Educ. Prof. 2016, 4, 72–79. [Google Scholar] [PubMed]
- Demirören, M.; Turan, S.; Öztuna, D. Medical students’ self-efficacy in problem-based learning and its relationship with self-regulated learning. Med. Educ. Online 2016, 21, 30049. [Google Scholar] [CrossRef] [PubMed]
- Lucieer, S.M.; Jonker, L.; Visscher, C.; Rikers, R.M.J.P.; Themmen, A.P.N. Self-regulated learning and academic performance in medical education. Med. Teach. 2016, 38, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Salamonson, Y.; Ramjan, L.M.; van den Nieuwenhuizen, S.; Metcalfe, L.; Chang, S.; Everett, B. Sense of coherence, self-regulated learning and academic performance in first year nursing students: A cluster analysis approach. Nurse Educ. Pract. 2016, 17, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Lucieer, S.M.; van der Geest, J.N.; Elói-Santos, S.M.; de Faria, R.M.D.; Jonker, L.; Visscher, C.; Rikers, R.M.J.P.; Themmen, A.P.N. The development of self-regulated learning during the pre-clinical stage of medical school: A comparison between a lecture-based and a problem based curriculum. Adv. Health Sci. Educ. 2015, 21, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Denat, Y.; Dikmen, Y.; Arslan, G.G.; Karalar, D.; Yilmaz, G. Factors Affecting Self-Regulated Learning in Nursing Students in Turkey. Oxid. Commun. 2017, 40, 973. [Google Scholar]
- Cho, K.K.; Marjadi, B.; Langendyk, V.; Hu, W. Medical student changes in self-regulated learning during the transition to the clinical environment. BMC Med. Educ. 2017, 17, 59. [Google Scholar] [CrossRef] [PubMed]
- Berkhout, J.J.; Teunissen, P.W.; Helmich, E.; van Exel, J.; van der Vleuten, C.P.M.; Jaarsma, D.A.D.C. Patterns in clinical students’ self-regulated learning behavior: A Q-methodology study. Adv. Health Sci. Educ. 2017, 22, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Cheema, M.K.; Nadeem, A.; Aleem, M. Motivation, Cognitive and Resource Management Skills: Association of Self-Regulated Learning Domains with Gender, Clinical Transition and Academic Performance of Undergraduate Medical Students. Med. Sci. Educ. 2019, 29, 79–86. [Google Scholar] [CrossRef]
- Siddiqui, F.; Malik, A.A. Promoting self-regulated learning skills in medical students is the need of time. J. Taibah Univ. Med. Sci. 2019, 14, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Qaiser, A.; Waqqar, S.; Noor, A.A.; Zakaria, M.; Iqbal, F. Barrier Faced by Undergraduate Medical Students to Become Self-Regulated Learner. Pak. J. Med. Health Sci. 2020, 14, 1297–1300. [Google Scholar]
- Demirören, M.; Turan, S.; Teker, G.T. Determinants of self-regulated learning skills: The roles of tutors and students. Adv. Physiol. Educ. 2020, 44, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Samarasekera, D.D.; Sim, J.H.; Hong, W.H.; Foong, C.C.; Pallath, V.; Vadivelu, J. Exploring the Cultivation of Self-Regulated Learning (SRL) Strategies Among Pre-Clinical Medical Students in Two Medical Schools. Med. Sci. Educ. 2020, 30, 271–280. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, G.; Huang, R.; Yan, P.; Hu, P.; Huang, L.; Meng, T.; Zhang, J.; Liu, R.; Zeng, Y.; et al. Nomograms Predicting Self-Regulated Learning Levels in Chinese Undergraduate Medical Students. Front. Psychol. 2020, 10, 2858. [Google Scholar] [CrossRef]
- Zheng, B.; Zhang, Y. Self-regulated learning: The effect on medical student learning outcomes in a flipped classroom environment. BMC Med. Educ. 2020, 20, 100. [Google Scholar] [CrossRef] [PubMed]
- Ghorbani Yekta, B.; Doost Mohammadi, A.; Saeed Parvar, T. The Relationship Between Self-Regulated Learning Components and Achievement Motivation in Students of Islamic Azad University, Tehran Medical Branch. Strides Dev. Med. Educ. 2020, 17, 91550. [Google Scholar] [CrossRef]
- Zheng, J.; Li, S.; Lajoie, S.P. The Role of Achievement Goals and Self-regulated Learning Behaviors in Clinical Reasoning. Technol. Knowl. Learn. 2020, 25, 541–556. [Google Scholar] [CrossRef]
- Gandomkar, R.; Yazdani, K.; Fata, L.; Mehrdad, R.; Mirzazadeh, A.; Jalili, M.; Sandars, J. Using multiple self-regulated learning measures to understand medical students’ biomedical science learning. Med. Educ. 2020, 54, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Zheng, B.; Chang, C.; Lin, C.-H.; Zhang, Y. Academic Motivation, and Self-Regulation: How Do They Predict Academic Achievement for Medical Students? Med. Sci. Educ. 2021, 31, 125–130. [Google Scholar] [CrossRef]
- Elfakki, F.A.M.; Alamri, M.M.; Ashraful, I.; Elnimeiri, M.; Frah, E. Self-Regulated Learning in the University of Tabuk: Gender Differences in Strategy and Outcomes. Rwanda J. Med. Health Sci. 2021, 4, 151–165. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zheng, J.; Lajoie, S.P. The Frequency of Emotions and Emotion Variability in Self-regulated Learning: What Matters to Task Performance? Front. Learn. Res. 2021, 9, 76–91. [Google Scholar] [CrossRef]
- Kurt, E.; Eskimez, Z. Examining self-regulated learning of nursing students in clinical practice: A descriptive and cross-sectional study. Nurse Educ. Today 2022, 109, 105242. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.Y.; Liu, Y.J.; Shu, T.; Xiang, M.; Feng, Z.C. Factors associated with medical students’ self-regulated learning and its relationship with clinical performance: A cross-sectional study. BMC Med. Educ. 2022, 22, 128. [Google Scholar] [CrossRef] [PubMed]
- Dogu, O.; Karadas, A.; Bacaksiz, F.E. The relationships between self-regulated learning in clinical nursing practice and self-efficacy: A cross-sectional study among nursing students. Perspect. Psychiatr. Care 2022, 58, 2107–2115. [Google Scholar] [CrossRef] [PubMed]
- Stoffels, M.; Koster, A.S.; van der Burgt, S.M.E.; de Bruin, A.B.H.; Daelmans, H.E.M.; Peerdeman, S.M.; Kusurkar, R.A. Basic psychological needs satisfaction as a mediator between clinical learning climate, self-regulated learning and perceived learning in the nursing education context. Med. Teach. 2023, 45, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Subaş, F.; Karaçay, P. Factors associated with nursing students’ self-regulated learning in clinical practicum: A descriptive cross-sectional study. Nurs. Health Sci. 2023, 25, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhu, M.-L.; Shi, Y.-Q.; Yang, L.-L. Influencing factors of self-regulated learning of medical-related students in a traditional Chinese medical university: A cross-sectional study. BMC Med. Educ. 2023, 23, 87. [Google Scholar] [CrossRef] [PubMed]
- Romli, M.H.; Yunus, F.W.; Hamzah, S.A.; Abas, R.; Foong, C.C. Self-Regulated Learning of Nursing Students: A Cross-Sectional Study. Educ. Med. J. 2023, 15, 15–27. [Google Scholar] [CrossRef]
- Wang, T.; Li, S.; Huang, X.; Lajoie, S.P. Task complexity affects temporal characteristics of self-regulated learning behaviours in an intelligent tutoring system. Educ. Technol. Res. Dev. 2023, 71, 991–1011. [Google Scholar] [CrossRef]
- Wang, T.; Li, S.; Lajoie, S. The Interplay Between Cognitive Load and Self-Regulated Learning in a Technology-Rich Learning Environment. Educ. Technol. Soc. 2023, 26, 50–62. [Google Scholar] [CrossRef]
- Faisal, E. Understanding the interplay of self-regulated learning strategies in medical education: A cross-sectional structural equation modeling study. Health Sci. Rep. 2023, 6, e1689. [Google Scholar] [CrossRef] [PubMed]
- Andrews, M.A.; Okuliar, C.A.; Whelton, S.A.; Windels, A.O.; Kruse, S.R.; Nachnani, M.G.; Topol, D.A.; McBee, E.C.; Stein, M.T.; Singaraju, R.C.; et al. Using Self-Regulated Learning Microanalysis to Examine Regulatory Processes in Clerkship Students Engaged in Practice Questions. Perspect. Med. Educ. 2023, 12, 385–398. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Xiong, H.; Chung, L.Y.F.; Wang, Y.; Wang, P.; Fang, L.; Han, L.; Yang, Y. What affects self-regulated learning ability in undergraduate nursing students: A structural equation modelling approach. Nurs. Open 2023, 10, 5728–5740. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Huang, C.; Qin, J.; Huang, K. Factors influencing self-regulated learning ability among Medical undergraduates in China: A cross-sectional study. BMC Med. Educ. 2024, 24, 1235. [Google Scholar] [CrossRef] [PubMed]
- Findyartini, A.; Greviana, N.; Hanum, C.; Wiyarta, E.; Novarianto, J.K.; Nugroho Supranoto, Y.T.; Ayusha, M.A.R.; Oktaria, D.; Sueningrum, A.S.; Pratiwi, Y.S.; et al. “How is social media used for learning?”: Relationships between social media use by medical students with their self-regulated learning skills. BMC Med. Educ. 2024, 24, 235. [Google Scholar] [CrossRef] [PubMed]
- Broks, V.M.A.; Dijk, S.W.; Van den Broek, W.W.; Stegers-Jager, K.M.; Woltman, A.M. Self-regulated learning profiles including test anxiety linked to stress and performance: A latent profile analysis based across multiple cohorts. Med. Educ. 2024, 58, 544–555. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.; Hui, Z.; Lei, H. The impact of teacher feedback on medical students’ self-regulated learning: A serial mediation model of teacher-student interaction and sense of school belonging. BMC Med. Educ. 2025, 25, 303. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zheng, J.; Lajoie, S.P.; Li, H.; Pu, D.; Wu, H. The Relationship Between Self-Regulated Learning Competency and Clinical Reasoning Tendency in Medical Students. Med. Sci. Educ. 2023, 33, 1335–1345. [Google Scholar] [CrossRef]
- Pajares, F. Gender and perceived self-efficacy in self-regulated learning. Theory Pract. 2002, 41, 116–125. [Google Scholar] [CrossRef]
- Young, J.Q.; Van Merrienboer, J.; Durning, S.; Cate, O.T. Cognitive Load Theory: Implications for medical education. Med. Teach. 2014, 36, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Spaic, D.; Bukumiric, Z.; Rajovic, N.; Markovic, K.; Savic, M.; Milin-Lazovic, J.; Grubor, N.; Milic, N.; Stanisavljevic, D.; Despotovic, A.; et al. The Flipped Classroom in Medical Education: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2025, 27, e60757. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Published by MDPI on behalf of the Academic Society for International Medical Education. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.