
Preparation for Residency: Effect of Formalized Patient Handover Instruction for Fourth-Year Medical Students


Abstract
1. Introduction
2. Materials and Method
2.1. Study Design and Participants
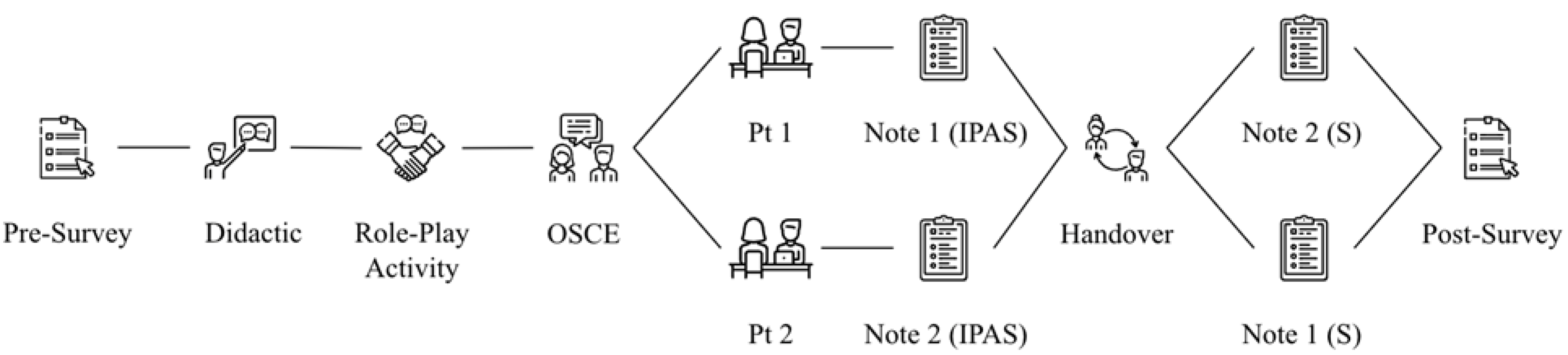
2.2. Curriculum and Intervention
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Confidence in Patient Handover and IPAS Score
3.2. Giving a Patient Handover
3.3. Receiving a Patient Handover and Comparisons Between Giver and Receiver
3.4. Student Feedback
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Summative OSCE Patient Case Scenarios I-PASS Grading Rubric
| OSCE Patient Case Scenario: Patient 1 | Points |
| Illness Severity—if correct 1 point, if incorrect/no answer 0 | |
| 1. Watcher | |
| Patient Summary—all included 1 point, some—partial (0.5 point), incorrect/none—0 | |
| |
| |
| |
| Action List—all included 1 point, some—partial (0.5 point), incorrect/none—0 | |
| |
| |
| |
| |
| Situation Awareness and Contingency Planning—all included 1 point, some—partial (0.5 point), incorrect/none—0 | |
| |
| |
| Synthesis by Receiver—all included 1 point, some—partial (0.5 point), incorrect/none—0 | |
| |
| |
| OSCE Patient Case Scenario: Patient 2 | Points |
| Illness Severity—if correct 1 point, if incorrect/no answer 0 | |
| 1. Watcher | |
| Patient Summary—all included 1 point, some—partial (0.5 point), incorrect/none—0 | |
| |
| |
| |
| Action List—all included 1 point, some—partial (0.5 point), incorrect/none—0 | |
| |
| |
| Situation Awareness and Contingency Planning—all included 1 point, some—partial (0.5 point), incorrect/none—0 | |
| |
| |
| |
| Synthesis by Receiver—all included 1 point, some—partial (0.5 point), incorrect/none—0 | |
| |
| |
References
- Starmer, A.J.; Spector, N.D.; Srivastava, R.; West, D.C.; Tse, L.L.; Allen, A.D.; Rosenbluth, G.; Dalal, A.K.; Keohane, C.A.; Lipsitz, S.R.; et al. Changes in medical errors with a handoff program. N. Engl. J. Med. 2015, 372, 490–491. [Google Scholar] [CrossRef] [PubMed]
- Joint Commission on Accreditation of Healthcare Organizations. The Joint Commission releases Improving America’s hospitals: The Joint Commission’s annual report on quality and safety 2007. Jt. Comm. Perspect. 2007, 27, 1–3. [Google Scholar]
- Horwitz, L.I.; Moin, T.; Krumholz, H.M.; Wang, L.; Bradley, E.H. Consequences of inadequate sign-out for patient care. Arch. Intern. Med. 2008, 168, 1755–1760. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.; Wisnivesky, J.; Williams, S.; McGinn, T. Medical errors related to discontinuity of care from an inpatient to an outpatient setting. J. Gen. Intern. Med. 2003, 18, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Starmer, A.J.; Spector, N.D.; Srivastava, R.; West, D.C.; Rosenbluth, G.; Allen, A.D.; Noble, E.L.; Tse, L.L.; Dalal, A.K.; Keohane, C.A.; et al. Changes in medical errors after implementation of a handoff program. N. Engl. J. Med. 2014, 371, 1803–1812. [Google Scholar] [CrossRef] [PubMed]
- Tool: I-PASS. Agency for Healthcare Research and Quality; 2023. Available online: https://www.ahrq.gov/teamstepps-program/curriculum/communication/tools/ipass.html (accessed on 3 April 2025).
- Hospitals and Health Systems: Advance Your Institution’s Patient Safety Culture. I-PASS Patient Safety Institute. n.d. Available online: https://www.ipassinstitute.com/hospitals-and-health-systems (accessed on 3 April 2025).
- Weiss, K.B.; Bagian, J.P.; Wagner, R. CLER Pathways to Excellence: Expectations for an Optimal Clinical Learning Environment (Executive Summary). J. Grad. Med. Educ. 2014, 6, 610–611. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Terndrup, C.; Phan, P.H.; Zaeh, S.E.; Atsina, K.; Minkove, N.; Billioux, A.; Chatterjee, S.; Montague, I.; Clark, B.; et al. A Randomized Cohort Controlled Trial to Compare Intern Sign-Out Training Interventions. J. Hosp. Med. 2017, 12, 979–983. [Google Scholar] [CrossRef] [PubMed]
- Clements, K. High-reliability and the I-pass communication tool. Nurs. Manag. 2017, 48, 12–13. [Google Scholar] [CrossRef] [PubMed]
- Patient Handoff Templates: An Executive Guide to Safer Transitions. American Data Network. 6 March 2025. Available online: https://www.americandatanetwork.com/patient-safety/patient-handoff-template-safety-transitions (accessed on 3 April 2025).
- Liston, B.W.; Tartaglia, K.M.; Evans, D.; Walker, C.; Torre, D. Handoff practices in undergraduate medical education. J. Gen. Intern. Med. 2014, 29, 765–769. [Google Scholar] [CrossRef] [PubMed]
- Solet, D.J.; Norvell, J.M.; Rutan, G.H.; Frankel, R.M. Lost in translation: Challenges and opportunities in physician-to-physician communication during patient handoffs. Acad. Med. J. Assoc. Am. Med. Coll. 2005, 80, 1094–1099. [Google Scholar] [CrossRef] [PubMed]
- Association of American Medical Colleges. Medical Education: The Core Entrustable Professional Activities (EPAs) for Entering Residency. Available online: https://www.aamc.org/what-we-do/mission-areas/medical-education/cbme/core-epas (accessed on 31 March 2025).
- Cleland, J.A.; Ross, S.; Miller, S.C.; Patey, R. “There is a chain of Chinese whispers ...”: Empirical data support the call to formally teach handover to prequalification doctors. Qual. Saf. Health Care 2009, 18, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Holt, N.; Crowe, K.; Lynagh, D.; Hutcheson, Z. Is there a need for formal undergraduate patient handover training and could an educational workshop effectively provide this? A proof-of-concept study in a Scottish Medical School. BMJ Open 2020, 10, e034468. [Google Scholar] [CrossRef] [PubMed]
- Miller, G.E. The assessment of clinical skills/competence/performance. Acad Med. 1990, 65, s63–s67. [Google Scholar] [CrossRef] [PubMed]
- Pangaro, L. A new vocabulary and other innovations for improving descriptive in-training evaluations. Acad Med. 1999, 74, 1203–1207. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| I-PASS Element | Description |
|---|---|
| I: Illness severity |
|
| P: Patient summary |
|
| A: Action list |
|
| S: Situation awareness and contingency planning |
|
| S: Synthesis by receiver |
|
| Survey Item | Prior Experience in Giving and/or Receiving Patient Handover | n | % for Each Likert-Scale Rating | χ2 | p Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| SD | D | Neutral | A | SA | |||||
| I am confident in giving a patient handover | Experience BOTH giving and receiving | 60 | 1.7 | 11.7 | 16.7 | 63.3 | 6.7 | 25.3 | 0.001 |
| Experience giving OR receiving | 19 | 5.3 | 26.3 | 26.3 | 42.1 | 0.0 | |||
| No experience | 19 | 15.8 | 42.1 | 31.6 | 10.5 | 0.0 | |||
| I am confident in receiving a patient handover | Experience BOTH giving and receiving | 60 | 0.0 | 8.3 | 15.0 | 53.3 | 23.3 | 31.9 | 0.000 |
| Experience giving OR receiving | 19 | 15.8 | 15.8 | 42.1 | 26.3 | 0.0 | |||
| No experience | 19 | 15.8 | 31.6 | 21.1 | 31.6 | 0.0 | |||
| I am confident in knowing what pertinent information to include in a patient handover | Experience BOTH giving and receiving | 60 | 1.7 | 3.3 | 16.7 | 70.0 | 8.3 | 36.3 | 0.000 |
| Experience giving OR receiving | 19 | 10.5 | 15.8 | 10.5 | 63.2 | 0.0 | |||
| No experience | 19 | 10.5 | 42.1 | 36.8 | 10.5 | 0.0 | |||
| Survey Item | Transition to Residency Course (TTR) | n | % for Each Likert-Scale Rating | χ2 | p Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| SD | D | Neutral | A | SA | |||||
| I am confident in giving a patient handover | Pre-Course | 98 | 5.1 | 20.4 | 21.4 | 49.0 | 4.1 | 44.6 | 0.000 |
| Post-Course | 93 | 0.0 | 1.1 | 5.4 | 74.2 | 19.4 | |||
| I am confident in receiving a patient handover | Pre-Course | 98 | 6.1 | 14.3 | 21.4 | 43.9 | 14.3 | 31.9 | 0.000 |
| Post-Course | 93 | 0.0 | 2.2 | 5.4 | 61.3 | 31.2 | |||
| I am confident in knowing what pertinent information to include in a patient handover | Pre-Course | 98 | 5.1 | 13.3 | 19.4 | 57.1 | 5.1 | 27.4 | 0.000 |
| Post-Course | 93 | 0.0 | 1.1 | 9.7 | 68.8 | 20.4 | |||
| Patient 1 Handover Write-Up (n = 47) | Patient 2 Handover Write-Up (n = 46) | |||
|---|---|---|---|---|
| Illness Severity Answer | # correctly listed | Illness Severity Answer | # correctly listed | |
| 30 |
| 36 | |
| Patient Summary Answers | # correctly listed | Patient Summary Answers | # correctly listed | |
| 47 |
| 46 | |
| 25 46 | |||
| 36 | |||
| 45 | |||
| 43 44 | |||
| 39 | |||
| 38 | |||
| 7 | |||
| 18 | |||
| 31 |
| 12 | |
| 30 |
| 33 | |
| 12 | |||
| 15 | |||
| 7 | |||
| 32 | |||
| 4 | |||
| Patient 1 Handover Write-Up (n = 47) | Patient 2 Handover Write-Up (n = 46) | ||
|---|---|---|---|
| Action List Answers | # correctly listed | Action List Answers | # correctly listed |
| 45 |
| 45 |
| 25 |
| 35 |
| 40 | ||
| Situation Awareness and Contingency Planning Answers | # correctly listed | Situation Awareness and Contingency Planning Answers | # correctly listed |
| 23 |
| 32 |
| 42 | ||
| 8 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Academic Society for International Medical Education. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kazmi, M.; Wong, S.; Conklin, P.; Cohen, D.; Wackett, A.; Lu, W.-H. Preparation for Residency: Effect of Formalized Patient Handover Instruction for Fourth-Year Medical Students. Int. Med. Educ. 2025, 4, 10. https://doi.org/10.3390/ime4020010
Kazmi M, Wong S, Conklin P, Cohen D, Wackett A, Lu W-H. Preparation for Residency: Effect of Formalized Patient Handover Instruction for Fourth-Year Medical Students. International Medical Education. 2025; 4(2):10. https://doi.org/10.3390/ime4020010
Chicago/Turabian StyleKazmi, Masooma, Stacey Wong, Perrilynn Conklin, David Cohen, Andrew Wackett, and Wei-Hsin Lu. 2025. "Preparation for Residency: Effect of Formalized Patient Handover Instruction for Fourth-Year Medical Students" International Medical Education 4, no. 2: 10. https://doi.org/10.3390/ime4020010
APA StyleKazmi, M., Wong, S., Conklin, P., Cohen, D., Wackett, A., & Lu, W.-H. (2025). Preparation for Residency: Effect of Formalized Patient Handover Instruction for Fourth-Year Medical Students. International Medical Education, 4(2), 10. https://doi.org/10.3390/ime4020010