
SARS-CoV-2 Vaccine Breakthrough Reinfections in Fully Vaccinated Healthcare Workers in Davao City, Philippines: A Retrospective Cohort Study

 , ,
, ,
Abstract
1. Introduction
2. Methodology
2.1. Study Design
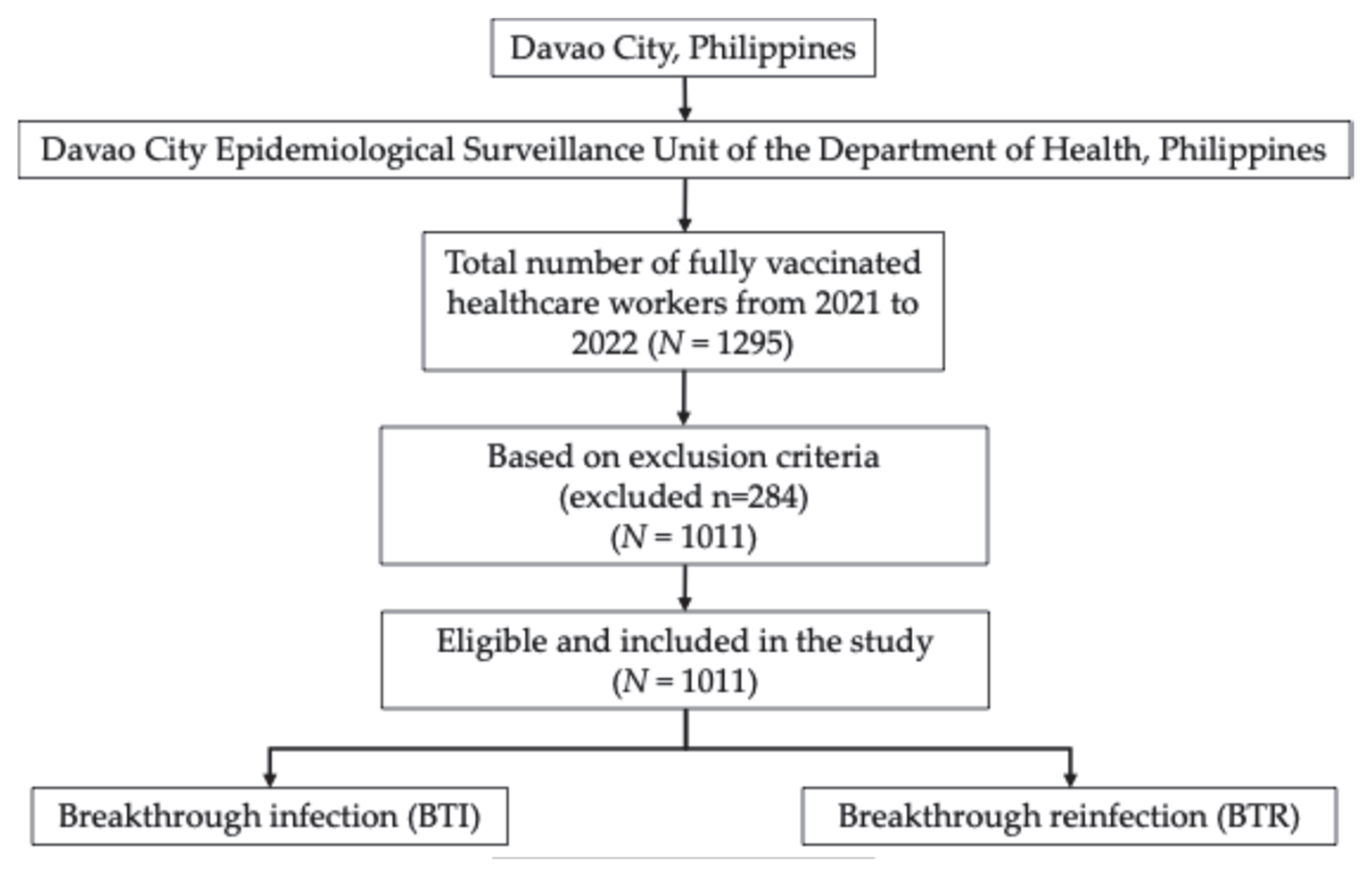
2.2. Study Population
- Fully vaccinated HCWs;
- Complete and accurate vaccination records for both first and second doses.
- A history of pre-vaccination infection;
- Second vaccine dose administered but date not recorded;
- No record of second vaccine dose;
- Complete second dose data but incomplete first dose data;
- Missing records for both first and second doses.
2.3. Study Period
2.4. Data Source
2.5. Exposures
2.6. Outcomes
2.7. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Healthcare Workers in Davao City, Philippines
3.2. Incidence of Breakthrough Infections Among Healthcare Workers in Davao City, Philippines
3.3. Associated Risk Factors of Vaccine Breakthrough Infections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yang, Y.P.; Pan, S.J.; Zhang, M.X.; Chen, H.X.; Tung, T.H. The Impact of COVID-19 Pandemic on Healthcare Workers under the “Ten New Guidelines” in Taizhou, China. Prev. Med. Rep. 2024, 37, 102550. [Google Scholar] [CrossRef]
- Smallwood, N.; Harrex, W.; Rees, M.; Willis, K.; Bennett, C.M. COVID-19 Infection and the Broader Impacts of the Pandemic on Healthcare Workers. Respirology 2022, 27, 411–426. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Lee, J.; Ta, C.; Soroush, A.; Rogers, J.R.; Kim, J.H.; Natarajan, K.; Zucker, J.; Perl, Y.; Weng, C. Risk Factors Associated With SARS-CoV-2 Breakthrough Infections in Fully MRNA-Vaccinated Individuals: Retrospective Analysis. JMIR Public Health Surveill. 2022, 8, e35311. [Google Scholar] [CrossRef]
- Liu, C.; Lee, J.; Ta, C.; Soroush, A.; Rogers, J.R.; Kim, J.H.; Natarajan, K.; Zucker, J.; Weng, C. A Retrospective Analysis of COVID-19 MRNA Vaccine Breakthrough Infections—Risk Factors and Vaccine Effectiveness. medRxiv 2021. [Google Scholar] [CrossRef]
- Gopinath, S.; Ishak, A.; Dhawan, N.; Poudel, S.; Shrestha, P.S.; Singh, P.; Xie, E.; Tahir, P.; Marzaban, S.; Michel, J.; et al. Characteristics of COVID-19 Breakthrough Infections among Vaccinated Individuals and Associated Risk Factors: A Systematic Review. Trop. Med. Infect. Dis. 2022, 7, 81. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Theiler-Schwetz, V.; Trummer, C.; Krause, R.; Ioannidis, J.P.A. SARS-CoV-2 Reinfections: Overview of Efficacy and Duration of Natural and Hybrid Immunity. Environ. Res. 2022, 209, 112911. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Bertollini, R. Severity of SARS-CoV-2 Reinfections as Compared with Primary Infections. New Engl. J. Med. 2021, 385, 2487–2489. [Google Scholar] [CrossRef]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. COVID-19 Vaccine Coverage in Health-Care Workers in England and Effectiveness of BNT162b2 MRNA Vaccine against Infection (SIREN): A Prospective, Multicentre, Cohort Study. Lancet 2021, 397, 1725–1735. [Google Scholar] [CrossRef]
- Perez-Garcia, F.; Perez-Zapata, A.; Arcos, N.; De La Mata, M.; Ortiz, M.; Simón, E.; Hervás Fernández, I.; González Ventosa, V.; Muñoz Monte, M.; González Arroyo, J.; et al. Severe Acute Respiratory Coronavirus Virus 2 (SARS-CoV-2) Infection among Hospital Workers in a Severely Affected Institution in Madrid, Spain: A Surveillance Cross-Sectional Study. Infect. Control Hosp. Epidemiol. 2021, 42, 803–809. [Google Scholar] [CrossRef]
- Buonafine, C.P.; Paiatto, B.N.M.; Leal, F.B.; de Matos, S.F.; de Morais, C.O.; Guerra, G.G.; Martuchelli, M.V.V.; Oliveira, D.B.L.; Durigon, E.L.; Soares, C.P.; et al. High Prevalence of SARS-CoV-2 Infection among Symptomatic Healthcare Workers in a Large University Tertiary Hospital in São Paulo, Brazil. BMC Infect. Dis. 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Stead, D.; Adeniyi, O.V.; Singata-Madliki, M.; Abrahams, S.; Batting, J.; Jelliman, E.; Parrish, A. Cumulative Incidence of SARS-CoV-2 and Associated Risk Factors among Healthcare Workers: A Cross-Sectional Study in the Eastern Cape, South Africa. BMJ Open 2022, 12, e058761. [Google Scholar] [CrossRef] [PubMed]
- Dzinamarira, T.; Mhango, M.; Dzobo, M.; Ngara, B.; Chitungo, I.; Makanda, P.; Atwine, J.; Nkambule, S.J.; Musuka, G. Risk Factors for COVID-19 among Healthcare Workers. A Protocol for a Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0250958. [Google Scholar] [CrossRef]
- Cordero, D.A. “Leaving” Resilience for the Future? Exploring the Difficulty of Achieving Herd Immunity against COVID-19 in the Philippines. J. Public Health 2022, 44, e652–e653. [Google Scholar] [CrossRef] [PubMed]
- Cedeño, T.D.D.; Rocha, I.C.N.; Miranda, A.V.; Lim, L.T.S.; Buban, J.M.A.; Cleofas, J.V. Achieving Herd Immunity against COVID-19 in the Philippines. Public Health Chall. 2023, 2, e61. [Google Scholar] [CrossRef]
- Hasan, D.A.; Maulud, S.Q.; Jalal, P.J.; Priyanka; Choudhary, O.P. SARS-CoV-2 Vaccine Breakthrough Reinfection in a Health-Care Worker of Iraq: A Case Report. Hum. Vaccin Immunother. 2022, 18, 2055947. [Google Scholar] [CrossRef]
- Shastri, J.; Parikh, S.; Aggarwal, V.; Agrawal, S.; Chatterjee, N.; Shah, R.; Devi, P.; Mehta, P.; Pandey, R. Severe SARS-CoV-2 Breakthrough Reinfection With Delta Variant After Recovery From Breakthrough Infection by Alpha Variant in a Fully Vaccinated Health Worker. Front. Med. 2021, 8, 737007. [Google Scholar] [CrossRef] [PubMed]
- Skrzat-Klapaczyńska, A.; Bieńkowski, C.; Kowalska, J.; Paciorek, M.; Puła, J.; Krogulec, D.; Stengiel, J.; Pawełczyk, A.; Perlejewski, K.; Osuch, S.; et al. The Beneficial Effect of the COVID-19 Vaccine Booster Dose among Healthcare Workers in an Infectious Diseases Center. Vaccines 2022, 10, 552. [Google Scholar] [CrossRef]
- Oster, Y.; Benenson, S.; Nir-Paz, R.; Buda, I.; Cohen, M.J. The Effect of a Third BNT162b2 Vaccine on Breakthrough Infections in Health Care Workers: A Cohort Analysis. Clin. Microbiol. Infect. 2022, 28, 735.e1–735.e3. [Google Scholar] [CrossRef]
- Spitzer, A.; Angel, Y.; Marudi, O.; Zeltser, D.; Saiag, E.; Goldshmidt, H.; Goldiner, I.; Stark, M.; Halutz, O.; Gamzu, R.; et al. Association of a Third Dose of BNT162b2 Vaccine with Incidence of SARS-CoV-2 Infection among Health Care Workers in Israel. JAMA 2022, 327, 341. [Google Scholar] [CrossRef]
- Moosavi, S.; Namdar, P.; Moghaddam Zeabadi, S.; Akbari Shahrestanaki, Y.; Ghalenoei, M.; Amerzadeh, M.; Kalhor, R. Healthcare Workers Exposure Risk Assessment in the Context of the COVID-19: A Survey among Frontline Workers in Qazvin, Iran. BMC Health Serv. Res. 2023, 23, 1–7. [Google Scholar] [CrossRef]
- Atnafie, S.A.; Anteneh, D.A.; Yimenu, D.K.; Kifle, Z.D. Assessment of Exposure Risks to COVID-19 among Frontline Health Care Workers in Amhara Region, Ethiopia: A Cross-Sectional Survey. PLoS ONE 2021, 16, e0251000. [Google Scholar] [CrossRef] [PubMed]
- Wilson, K.S.; Ntlebi, V.; Made, F.; Sanabria, N.; Vetten, M.; Joseph, J.; Chin, G.; Jones, D.; Tlotleng, N. COVID-19 Cases among Medical Laboratory Services Staff in South Africa, 2020–2021: A Cohort Study. PLoS ONE 2022, 17, e0268998. [Google Scholar] [CrossRef] [PubMed]
- Issah, M.A.; Atinga, R.A.; Baku, A.A. Adherence to COVID-19 Protocols: A Comparative Study of Public and Private Hospitals in Ghana. Public. Health Pract. 2024, 7, 100463. [Google Scholar] [CrossRef]
- Sarapultseva, M.; Hu, D.; Sarapultsev, A. SARS-CoV-2 Seropositivity among Dental Staff and the Role of Aspirating Systems. JDR Clin. Trans. Res. 2021, 6, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Conway Morris, A.; Sharrocks, K.; Bousfield, R.; Kermack, L.; Maes, M.; Higginson, E.; Forrest, S.; Pereira-Dias, J.; Cormie, C.; Old, T.; et al. The Removal of Airborne SARS-CoV-2 and Other Microbial Bioaerosols by Air Filtration on COVID-19 Surge Units. Clin. Infect. Dis. 2021, 75, e97–e101. [Google Scholar] [CrossRef]
- Lindsley, W.G.; Derk, R.C.; Coyle, J.P.; Martin, S.B.; Mead, K.R.; Blachere, F.M.; Beezhold, D.H.; Brooks, J.T.; Boots, T.; Noti, J.D. Efficacy of Portable Air Cleaners and Masking for Reducing Indoor Exposure to Simulated Exhaled SARS-CoV-2 Aerosols—United States, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 972–976. [Google Scholar] [CrossRef]
- Dingemans, J.; van der Veer, B.M.J.W.; Gorgels, K.M.F.; Hackert, V.; den Heijer, C.D.J.; Hoebe, C.J.P.A.; Savelkoul, P.H.M.; van Alphen, L.B. Investigating SARS-CoV-2 Breakthrough Infections per Variant and Vaccine Type. Front. Microbiol. 2022, 13, 1027271. [Google Scholar] [CrossRef]
- Evans, J.P.; Zeng, C.; Carlin, C.; Lozanski, G.; Saif, L.J.; Oltz, E.M.; Gumina, R.J.; Liu, S.L. Neutralizing Antibody Responses Elicited by SARS-CoV-2 MRNA Vaccination Wane over Time and Are Boosted by Breakthrough Infection. Sci. Transl. Med. 2022, 14, eabn8057. [Google Scholar] [CrossRef]
- Chivu-economescu, M.; Vremera, T.; Ruta, S.M.; Grancea, C.; Leustean, M.; Chiriac, D.; David, A.; Matei, L.; Diaconu, C.C.; Gatea, A.; et al. Assessment of the Humoral Immune Response Following COVID-19 Vaccination in Healthcare Workers: A One Year Longitudinal Study. Biomedicines 2022, 10, 1526. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. Covid-19 Breakthrough Infections in Vaccinated Health Care Workers. New Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Sabnis, R.; Patil, A.; Shete, N.; Rastogi, A.K. Break-through COVID-19 Infection Rate with Indian Strain in Single-Center Healthcare Workers—A Real World Data 2021. MedRxiv 2021. [Google Scholar] [CrossRef]
- Akhter, M.; Roy, S.K.; Khair, A.; Karim, M.R.; Mojlish, U.K.F.K.; Ahmed, M.U.; Ali, L. SARS-COV-2 Breakthrough Infection and Its Covariates among Healthcare Providers of a Hospital in Bangladesh during the Omicron Wave. Heliyon 2024, 10, e37287. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | N (%) | Fully vaccinated, with BTRs n(%) | Fully Vaccinated, No BTR n(%) | p Value |
|---|---|---|---|---|
| Gender | ||||
| Male | 304 (30.07) | 26 (8.55) | 278 (91.45) | 0.3076 |
| Female | 707 (69.93) | 76 (10.75) | 631 (89.25) | |
| Age | ||||
| Less than 40 | 815 (80.61) | 87 (10.67) | 728 (89.33) | 0.3574 |
| Above 40 | 196 (19.39) | 16 (8.16) | 180 (91.84) | |
| Occupation | ||||
| Physician | 230 (22.75) | 31 (13.38) | 199 (86.52) | 0.0002 |
| Nurse/Nurse Aid | 424 (41.94) | 43 (10.14) | 381 (89.86) | |
| Medical Technologist | 76 (7.52) | 17 (22.37) | 59 (77.63) | |
| Other healthcare workers | 127 (12.56) | 5 (3.94) | 122 (96.06) | |
| Other occupation (non-clinical) | 154 (15.23) | 9 (5.84) | 145 (94.16) | |
| Type of Health Institution | ||||
| Public hospitals and health facilities | 408 (40.36) | 49 (12) | 359 (88) | 0.0041 |
| Private Hospitals | 478 (47.28) | 37 (7.74) | 441 (92.26) | |
| Outpatient centers and non-medical institutions | 125 (12.36) | 4 (3.2) | 121 (96.8) | |
| Type of vaccine | ||||
| Sinovac | 680 (67.26) | 72 (10.59) | 608 (89.41) | 0.5185 |
| Pfizer-BioNTech | 135 (13.35) | 14 (10.37) | 121 (89.63) | |
| AstraZeneca | 169 (16.72) | 14 (8.28) | 155 (91.72) | |
| Others | 27 (2.67) | 4 (14.81) | 23 (85.19) | |
| Boster shot | ||||
| Without booster | 805 (79.62) | 90 (11.18) | 715 (88.82) | 0.0267 |
| With booster | 206 (20.38) | 12 (5.83) | 194 (94.17) | |
| Type of booster | ||||
| Homologous | 52 (25.24) | 5 (9.62) | 47 (90.38) | 0.1834 |
| Heterologous | 154 (74.76) | 7 (4.55) | 147 (95.45) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hinay, A.A., Jr.; Reyes, J.A.H.; Servillon, R.J.T.; Sarabia, A.R.C. SARS-CoV-2 Vaccine Breakthrough Reinfections in Fully Vaccinated Healthcare Workers in Davao City, Philippines: A Retrospective Cohort Study. COVID 2025, 5, 106. https://doi.org/10.3390/covid5070106
Hinay AA Jr., Reyes JAH, Servillon RJT, Sarabia ARC. SARS-CoV-2 Vaccine Breakthrough Reinfections in Fully Vaccinated Healthcare Workers in Davao City, Philippines: A Retrospective Cohort Study. COVID. 2025; 5(7):106. https://doi.org/10.3390/covid5070106
Chicago/Turabian StyleHinay, Alfredo A., Jr., Jennifer Ashley H. Reyes, Rvin John T. Servillon, and Ace Ronald C. Sarabia. 2025. "SARS-CoV-2 Vaccine Breakthrough Reinfections in Fully Vaccinated Healthcare Workers in Davao City, Philippines: A Retrospective Cohort Study" COVID 5, no. 7: 106. https://doi.org/10.3390/covid5070106
APA StyleHinay, A. A., Jr., Reyes, J. A. H., Servillon, R. J. T., & Sarabia, A. R. C. (2025). SARS-CoV-2 Vaccine Breakthrough Reinfections in Fully Vaccinated Healthcare Workers in Davao City, Philippines: A Retrospective Cohort Study. COVID, 5(7), 106. https://doi.org/10.3390/covid5070106