Abstract
Background: The management of symptomatic uterine fibroids in women of reproductive age remains a clinical challenge, with uterine preservation being a primary objective in order to safeguard fertility. To date, no clear consensus has been established in the literature regarding the optimal treatment strategy, as therapeutic choices largely depend on individual patient characteristics. In selected cases, the use of preoperative measures aimed at minimizing the risk of major intraoperative hemorrhage has been associated with an increased likelihood of adopting a more conservative surgical approach. Case presentation: We report the case of a young patient treated at our institution who presented large uterine fibroids and underwent Preoperative Uterine Artery Embolization (PUAE) before planned open myomectomy with positive outcomes. In our case, this approach provided excellent intraoperative hemostatic control, minimizing blood loss. At post-discharge follow-up, the patient showed marked symptom relief and improved quality of life. Long-term follow-up will assess sustained treatment efficacy. Conclusions: PUAE should be considered a valuable therapeutic option in patients with symptomatic uterine fibroids at high risk of surgical bleeding. When integrated into a multidisciplinary treatment plan, PUAE may enhance surgical safety, support fertility preservation, and broaden the range of conservative options available for women with complex fibroid disease.
1. Introduction
Uterine fibroids, also known as leiomyomas or myomas, are benign smooth muscle tumors of the uterus that originate from the myometrium. Histologically, they are composed of extracellular matrix rich in collagen, fibronectin, and proteoglycans.
Uterine fibroids represent the most common benign gynecological neoplasms, affecting up to 70% of women of reproductive age [1]. Risk factors for fibroid development include reproductive age, African ancestry, nulliparity, genetic predisposition, caffeine and alcohol consumption, early menarche, and the presence of comorbidities such as obesity and hypertension [2].
Fibroids are typically classified based on their anatomical location as submucosal, intramural, or subserosal. The most widely adopted classification systems are those proposed by the FIGO (International Federation of Gynecology and Obstetrics) and the ESGE (European Society for Gynecological Endoscopy).
Although often asymptomatic, approximately one-third of cases present with clinical symptoms including abnormal uterine bleeding (metrorrhagia), dysmenorrhea, pelvic pain, infertility, or recurrent pregnancy loss, as well as urinary or bowel disturbances [3]. In symptomatic patients, medical or surgical intervention is often required to improve quality of life and reproductive outcomes.
Diagnosis is primarily based on clinical examination and transvaginal ultrasound, the current gold standard. Additional diagnostic tools include sonohysterography, hysteroscopy, and MRI.
Available treatment options include medical therapy, myomectomy (via laparoscopy, laparotomy, or hysteroscopy), hysterectomy, Uterine Artery Embolization (UAE), and thermal ablation techniques [4]. The choice of treatment depends not only on fibroid characteristics (number, size, and location) but also on the patient’s age, desire for fertility preservation, and preference regarding invasive procedures [4]. In fact, no clear consensus has been established regarding the optimal therapeutic choice. In young women with complex and symptomatic disease, intervention is often unavoidable and whenever feasible, the most conservative approach should be adopted. Myomectomy and UAE remain the standard alternatives to hysterectomy, though uterine preservation may be challenging. To minimize intraoperative risks, the combination of those procedures can be considered. Nevertheless, it is important to note that although conservative approaches offer advantages in terms of uterus preservation, they are not risk-free and have been linked to miscarriages and obstetric complications [5,6].
These considerations underscore the complexity of the decision and highlight the necessity of an individualized risk–benefit assessment and a patient-centered approach.
The purpose of this case report is to describe the clinical utility of Preoperative Uterine Artery Embolization (PUAE) as an adjunct to conservative surgical management in a young woman with symptomatic and highly vascularized fibroids, highlighting its role in reducing intraoperative blood loss and facilitating a uterus-preserving approach.
2. Case Presentation
2.1. Patient Information
We present the case of Ms. R.J.C., a 34-year-old woman from Madagascar, known to have a history of left breast fibroadenoma and chronic iron-deficiency anemia under long-term treatment. Her family history is notable for a father who died of prostate carcinoma, one sister with uterine fibromatosis, and another with ovarian cysts, with no known hereditary gynecologic malignancies. She has no prior surgical history, no history of blood transfusions, and no known drug allergies. Her BMI was 21.7 kg/m2, and she reported no tobacco or alcohol use. Gynecologically, the patient experienced menarche at age 14, reported regular 28-day menstrual cycles, denied prior pelvic inflammatory disease or genital infections, and had a negative Pap smear in 2025. She was sexually inactive (virgo) and nulligravid (G0P0). Her blood pressure values were consistently normal. Table 1 presents a summary of the patient’s demographic and clinical characteristics.

Table 1.
Summary of patient demographic and clinical characteristics.
2.2. Clinical Course
In November 2024, a 34-year-old woman presented to her general practitioner with the subjective perception of an abdominal mass. She reported chronic fatigue and a history of iron-deficiency anemia, which had worsened in recent months and was now associated with dizziness. Laboratory findings dated 19 June 2024 revealed Hb 13.6 g/dL, serum iron 70 µg/dL, and ferritin 18 ng/mL. She had never undergone a gynecological examination. An abdominal ultrasound and updated blood tests were requested. Oral iron therapy, already ongoing, was continued.
By December 2024, the patient reported pelvic pain, metrorrhagia, a progressive increase in the size of the abdominal mass, and the onset of mild constipation. No urinary symptoms were reported. Blood tests revealed Hb 12.3 g/dL, iron 37 µg/dL, ferritin 13 ng/mL, and transferrin saturation 9%.
On 27 December 2024, an abdominal ultrasound performed at Parini Hospital (Aosta, Italy) identified a large pelvic solid mass (~9 cm maximum longitudinal diameter) (Figure 1), with a heterogeneous appearance, predominantly peripheral vascularization, and multinodular morphology, likely of uterine origin (fundal). Urgent gynecologic evaluation was recommended. Table 2 presents a timeline of the patient’s clinical course.
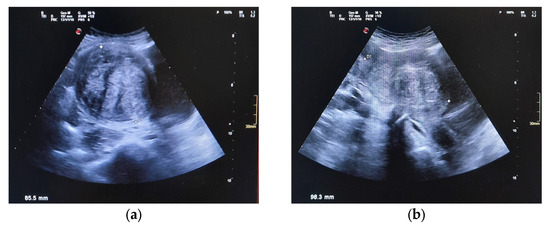
Figure 1.
Abdominal US, showing large uterine fibroids in transverse (a) and longitudinal (b) view. The mass displaced the right margin of the bladder. No free fluid was detected.
Table 2.
Timeline of the patient’s clinical course.
Subsequent laboratory evaluations in January and February 2025 showed stabilization of hematologic parameters under iron therapy (Hb up to 14.3 g/dL), with no elevation in tumor markers (CA125: 20.1 U/mL, CA15.3: 16.4 U/mL, CA19-9: 25 U/mL, CEA: 2 ng/mL; β-hCG: negative).
On 28 February 2025, she underwent her first gynecological examination at Beauregard Hospital (Aosta, Italy) for symptomatic recurrent metrorrhagia (heavy menstrual bleeding) in the setting of a fibroid uterus. Transabdominal ultrasound showed an anteverted and fibroid uterus, measuring 150 × 87 × 70 mm with an endometrial thickness of 4 mm and the presence of a fundal intramural fibroid (approximately 65 × 35 mm) and a large corporal intramural fibroid (approximately 87 × 77 mm), both with predominantly peripheral vascularization (CS2). Both ovaries were normal in morphology and location, and no free fluid was seen in the Douglas pouch.
Given the patient’s age and the desire to preserve fertility, while also addressing the progressively worsening symptoms, a conservative approach was proposed. Preoperative medical therapy with Ryeqo® (relugolix 40 mg, estradiol 1 mg, norethisterone acetate 0.5 mg; Gedeon Richter) was prescribed and promptly initiated. The patient reported partial symptom improvement and reduced bleeding in April 2025.
A pelvic MRI performed on 15 April 2025 confirmed a globular and enlarged uterus (16 × 8 × 7 cm) (Figure 2), due to multiple intramural and submucosal fibroids. Two dominant fibroids were located at the fundus and corpus: these appeared hypointense on T2, with well-defined margins, no signs of hemorrhagic or necrotic degeneration, and mild homogeneous contrast enhancement; additional small subserosal fibroids were noted. The endometrium and ovaries appeared normal, with the absence of ascites. The bladder was compressed and displaced.
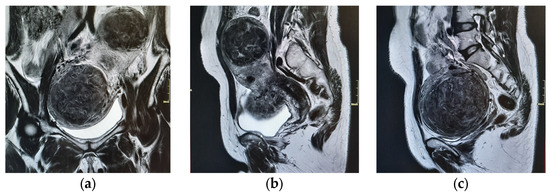
Figure 2.
MRI images in coronal (a) and sagittal (b,c) planes. The images demonstrate the patient’s pelvis, almost completely deformed due to the mass effect of the fibroids, with the cranial one measuring 67 × 60 × 67.5 cm and the caudal one 92.5 × 91 × 84 cm.
At the gynecological consultation on 9 May, informed consent was obtained for a planned open multiple myomectomy, and to minimize the risk of intraoperative hemorrhage, a Preoperative Uterine Artery Embolization (PUAE) was scheduled following a multidisciplinary discussion with interventional radiologists. The decision to proceed with open surgery was justified by the large size of the fibroids and their intramural location.
On 5 June 2025, the patient underwent selective PUAE at Parini Hospital (Figure 3). Via right femoral access, angiography showed marked hypervascularization of both myomas, especially of the most cranial one. Both uterine arteries were embolized with 800-micron non-absorbable particles followed by gelfoam emulsion. At the end of the procedure, adequate devascularization of both lesions was observed. Beyond their application in the treatment of uterine fibroids, the embolic agents used during PUAE—including gelfoam—are also widely employed in the management of other gynecologic vascular pathologies. In particular, gelfoam slurry has demonstrated efficacy in controlling bleeding from uterine and pelvic pseudoaneurysms and has been used as part of conservative treatment strategies for cervical and select non-tubal ectopic pregnancies, where prompt devascularization is essential to avoid major hemorrhage.
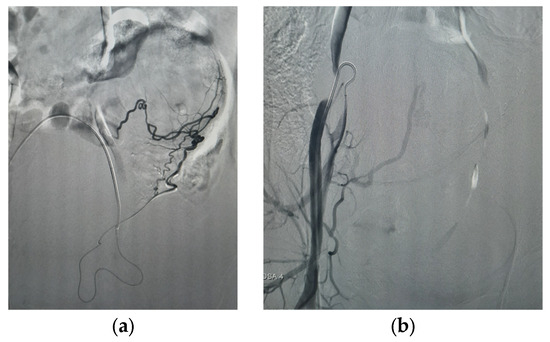
Figure 3.
Effects of embolization of the left uterine artery, supplying the fundal fibroid (a), and of the right uterine artery, supplying the anterior fibroid (b). These post-procedure images show low vascularization of both fibroids as the contrast agent is taken up only by the few remaining vessels supplying the lesions.
On the same day at Beauregard Hospital, the patient underwent a longitudinal laparotomic multiple myomectomy, with bilateral occlusion of the uterine and the utero-ovarian vessels using vascular clamps (maintained for roughly one hour). Upon opening the abdominal cavity, the uterus was immediately visualized as enlarged and deformed by the presence of multiple fibroids, primarily by the two dominant ones previously identified through preoperative diagnostic imaging. The procedure lasted about 85 min, with both fibroids successfully excised without complications (Figure 4). A double-layer uterine closure was performed, with the second layer being imbricating, using an absorbable monofilament suture USP 0 with a 32 mm curved needle. Although two units of blood products were requested preoperatively, no transfusions were administered, as blood loss was limited (approximately 100 cc).
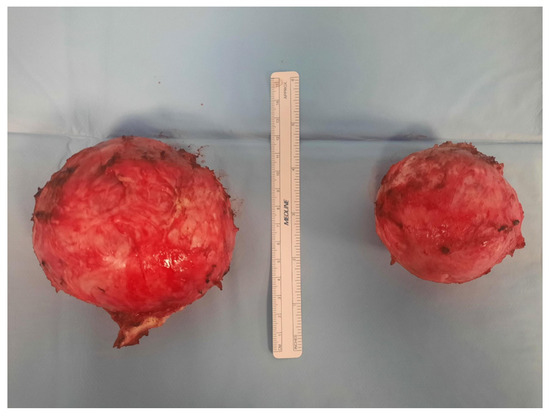
Figure 4.
The image shows the two main fibroids removed during the surgery, measuring approximately 9 and 7 cm in diameter.
The postoperative course was uneventful, with Hb 13 g/dL and stable vital signs. The patient was discharged on postoperative day 3 in stable and good general condition, with the recommendation to continue treatment with Ryeqo® for one month and to avoid attempting conception for at least 12 months following surgery.
At the follow-up evaluation, performed 40 days after surgery, the patient was in good general condition, with a marked improvement in symptoms. Ultrasound examination was within normal limits. No active genital bleeding was observed. The patient no longer reported or exhibited pelvic pain during the visit and urinary symptoms were no longer reported. Resumption of the menstrual cycle could not be assessed yet, as the patient has been in amenorrhea since starting Ryeqo® therapy.
The histopathological examination of the surgical specimens confirmed the diagnosis of leiomyomas.
3. Discussion
To date, UAE and myomectomy have been the primary conservative treatments used as alternatives to hysterectomy in complex fibroid cases. Their relevance as therapeutic options stems from the need to always consider the possibility of conservative approaches, particularly when managing women of reproductive age [7,8,9].
Regarding the combined use of these techniques, findings across studies are heterogeneous and there is no clear consensus. As reported by Russ et al. (2022) [10], the rationale behind the use of PUAE is that it should reduce the blood flow and subsequently reduce blood loss when scarring the uterus during myomectomy, with the additional long-term advantage of inducing atrophy in any possible residual small fibroids. The primary advantages acknowledged for the combined use of PUAE and myomectomy are a reduced risk of intraoperative hemorrhage [10,11,12,13,14,15] and a decreased need for blood transfusion [10,11,14,16,17]. As reported by Ghiaroni et al. (2013) [16], PUAE is additionally associated with the possibility of a smaller incision, increasing the chance of preserving the uterus. Furthermore, as shown in Dumousset et al. (2008)’s [13] retrospective study, PUAE has been reported to improve intraoperative visibility by reducing vascularization, thereby facilitating the surgical procedure.
Nonetheless, it should be noted that some studies demonstrate that hemoglobin values do not differ significantly between patients undergoing PUAE and those receiving surgery alone [11,12].
The available evidence suggests that combining PUAE and surgical intervention can be considered in specific cases: it is especially recommended for patients with symptomatic fibroids [10], significantly enlarged uteri [10,18,19], or those at high risk of hemorrhage [15], where traditional surgery alone may pose technical or hemodynamic difficulties.
Although some studies have demonstrated the effectiveness of PUAE/UAE in achieving the benefits, its use has also been associated with an increased risk of complications. These approaches indeed spare patients from a radical intervention that results in a permanent loss of reproductive capacity. However, it should not be overlooked that these procedures are not without risks, particularly regarding fertility preservation: UAE may, in the long term, lead to increased reproductive challenges (e.g., it can raise the risk of IUAs and reduced endometrial thickness, resulting in changes in the ER during the ovulation day and a subsequent higher incidence of miscarriage [5,11,20,21]), as well as myomectomy (also associated with an increased risk of IUAs, as well as obstetric complications such as a higher risk of uterine rupture and placenta accreta [6,22]). Conservative approaches also present a greater likelihood of requiring reintervention due to fibroid recurrence or regrowth [23].
Although it could be an excellent therapeutic option, it should be emphasized that PUAE combined with myomectomy remains a complex treatment strategy, inherently limited to tertiary centers with interventional radiology integrated with gynecologic surgery teams. As demonstrated, in high-income countries (such as the UK, North America, and Western Europe), the procedure is available but used only in selected cases. In middle- and low-income settings, access is highly variable and could become extremely rare due to infrastructural and personnel limitations.
From an economic perspective, specific cost-effectiveness data for PUAE combined with myomectomy are scarce: the addition of an interventional radiology step increases initial costs, and the cost–benefit balance depends heavily on actual operating room savings, local reintervention rates, and the health system’s capacity to integrate multidisciplinary services.
The clinical course described in this report supports the idea that PUAE should be considered a valuable therapeutic tool for reducing intraoperative hemorrhage risk and increasing the chances of a conservative surgical option. Indeed, in our case, the use of PUAE allowed for a successful laparotomic myomectomy with minimal blood loss and no need for transfusions, despite the large fibroid burden and increased vascularization.
In conclusion, the role of PUAE as a potential risk-reducing strategy is widely supported and sometimes even demonstrated as more effective than surgery alone [14], but the paucity of comprehensive studies addressing combined treatment approaches highlights the need for further investigations to better define the indications, efficacy, patient selection criteria, and reproductive outcomes associated with such integrated strategies [24,25,26]. Therefore, PUAE is most likely justified—both clinically and economically—in high-volume centers with well-established infrastructure. Table 3 summarizes the included articles in the literature review.
Table 3.
Literature review.
Author Contributions
Conceptualization, B.B. and A.L.; methodology, L.L.; validation, A.L.; formal analysis, A.L. and M.N.; investigation, A.L.; resources, A.M., A.L. and R.T.; data curation, B.B.; writing—original draft preparation, B.B. and R.T.; writing—review and editing, L.L. and A.L.; visualization, L.L.; supervision, R.T. and A.L.; project administration, L.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. No Ethics Committee or institutional review board statement were required, due to the nature of the case report (single patient who consented for publication). This is also in agreement with HIPAA (Health Insurance Portability and Accountability Act): “a case report is an activity to develop information to be shared for medical/educational purposes. Although the use of protected health information to prepare, the paper does not require IRB review”.
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| CCT | Controlled Clinical Trial |
| MRI | Magnetic Resonance Imaging |
| PUAE | Preoperative Uterine Artery Embolization |
| RCS | Retrospective Cohort Study |
| RCTs | Randomized Controlled Trials |
| RR | Retrospective Review |
| RS | Retrospective Study |
| SR/MA | Systematic Review and Meta-analysis |
| UA | Uterine Artery |
| UAE | Uterine Artery Embolization |
| ER | Endometrial receptivity |
| IUAs | Intrauterine adhesions |
References
- Stewart, E.A.; Cookson, C.L.; Gandolfo, R.A.; Schulze-Rath, R. Epidemiology of uterine fibroids: A systematic review. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 1501–1512. [Google Scholar] [CrossRef]
- Donnez, J.; Dolmans, M.M. Uterine fibroid management: From the present to the future. Hum. Reprod. Update 2016, 22, 665–686. [Google Scholar] [CrossRef]
- De La Cruz, M.S.; Buchanan, E.M. Uterine Fibroids: Diagnosis and Treatment. Am. Fam. Physician 2017, 95, 100–107. [Google Scholar] [PubMed]
- Micić, J.; Macura, M.; Andjić, M.; Ivanović, K.; Dotlić, J.; Micić, D.D.; Arsenijević, V.; Stojnić, J.; Bila, J.; Babić, S.; et al. Currently Available Treatment Modalities for Uterine Fibroids. Medicina 2024, 60, 868. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.; Pereira, L.; Berghella, V. Pregnancy After Uterine Artery Embolization. Obstet. Gynecol. 2002, 100, 869–872. [Google Scholar] [PubMed]
- Lee, S.J.; Ko, H.S.; Na, S.; Bae, J.Y.; Seong, W.J.; Kim, J.W.; Shin, J.; Cho, H.J.; Choi, G.Y.; Kim, J.; et al. Nationwide population-based cohort study of adverse obstetric outcomes in pregnancies with myoma or following myomectomy: Retrospective cohort study. BMC Pregnancy Childbirth 2020, 20, 716. [Google Scholar] [CrossRef]
- Xu, F.; Deng, L.; Zhang, L.; Hu, H.; Shi, Q. The comparison of myomectomy, UAE and MRgFUS in the treatment of uterine fibroids: A meta analysis. Int. J. Hyperth. 2021, 38, 24–29. [Google Scholar] [CrossRef]
- Manyonda, I.T.; Bratby, M.; Horst, J.S.; Banu, N.; Gorti, M.; Belli, A.M. Uterine artery embolization versus myomectomy: Impact on quality of life—Results of the FUME (Fibroids of the Uterus: Myomectomy versus Embolization) Trial. Cardiovasc. Interv. Radiol. 2012, 35, 530–536. [Google Scholar] [CrossRef]
- Daniels, J.; Middleton, L.J.; Cheed, V.; McKinnon, W.; Rana, D.; Sirkeci, F.; Manyonda, I.; Belli, A.M.; Lumsden, M.A.; Moss, J.; et al. Uterine artery embolisation versus myomectomy for premenopausal women with uterine fibroids wishing to avoid hysterectomy: The FEMME RCT. Health Technol. Assess. 2022, 26, 1–74. [Google Scholar] [CrossRef]
- Russ, M.; Hees, K.A.; Kemmer, M.; Richter, R.; Kroncke, T.; Schnapauff, D.; Heimann, U.; David, M. Preoperative Uterine Artery Embolization in Women Undergoing Uterus-Preserving Myomectomy for Extensive Fibroid Disease: A Retrospective Analysis. Gynecol. Obstet. Investig. 2022, 87, 38–45. [Google Scholar] [CrossRef]
- Bula Ibula, D.; Balestra, A.; Tanos, P.; Nisolle, M.; Karampelas, S. Uterine artery embolization before myomectomy: Is it worth the trouble? J. Minim. Invasive Gynecol. 2025, 32, 386–394. [Google Scholar] [CrossRef]
- Butori, N.; Tixier, H.; Filipuzzi, L.; Mutamba, W.; Guiu, B.; Cercueil, J.P.; Douvier, S.; Sagot, P.; Krausé, D.; Loffroy, R. Interest of uterine artery embolization with gelatin sponge particles prior to myomectomy for large and/or multiple fibroids. Eur. J. Radiol. 2011, 79, 1–6. [Google Scholar] [CrossRef]
- Dumousset, E.; Chabrot, P.; Rabischong, B.; Mazet, N.; Nasser, S.; Darcha, C.; Garcier, J.M.; Mage, G.; Boyer, L. Preoperative uterine artery embolization (PUAE) before uterine fibroid myomectomy. Cardiovasc. Interv. Radiol. 2008, 31, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Ustünsöz, B.; Uğurel, M.S.; Bozlar, U.; Duru, N.K.; Ustünsöz, A. Is Uterine Artery Embolization Prior to Myomectomy for Giant Fibroids Helpful? Diagn. Interv. Radiol. 2007, 13, 210–212. [Google Scholar] [PubMed]
- Tixier, H.; Grevoul, J.; Loffroy, R.; Lauferon, J.; Guiu, B.; Mutamba, W.; Filipuzzi, L.; Cercueil, J.P.; Douvier, S.; Krause, D.; et al. Preoperative embolization or ligature of the uterine arteries in preparation for conservative uterine fibroma surgery. Acta Obstet. Gynecol. Scand. 2010, 89, 1310–1315. [Google Scholar] [CrossRef] [PubMed]
- Ghiaroni, J.; Lopez, G.E.; Coutinho Junior, A.C.; Schanaider, A. Uterine artery embolization with spherical PVA-PVAc particles as preparation for surgical resection of myomas. Rev. Col. Bras. Cir. 2013, 40, 386–391. [Google Scholar] [CrossRef]
- Malartic, C.; Morel, O.; Fargeadou, Y.; Le Dref, O.; Fazel, A.; Barranger, E.; Soyer, P. Conservative two-step procedure including uterin artery embolization with embosphere and surgical myomectomy for the treatment of multiple fibroids: Preliminary experience. Eur. J. Radiol. 2012, 81, 1–5. [Google Scholar] [CrossRef]
- Goldman, K.N.; Hirshfeld-Cytron, J.E.; Pavone, M.E.; Thomas, A.P.; Vogelzang, R.L.; Milad, M.P. Uterine artery embolization immediately preceding laparoscopic myomectomy. Int. J. Gynaecol. 2012, 116, 105–108. [Google Scholar] [CrossRef]
- McLucas, B.; Voorhees, W.D., 3rd. The effectiveness of combined abdominal myomectomy and uterine artery embolization. Int. J. Gynecol. 2015, 130, 241–243. [Google Scholar] [CrossRef]
- Ouyang, Y.; Peng, Y.; Zheng, M.; Mao, Y.; Gong, F.; Li, Y.; Chen, H.; Li, X. The impact of intrauterine adhesions on endometrial receptivity in patients undergoing in vitro fertilization-embryo transfer. Front. Endocrinol. 2025, 15, 1489839. [Google Scholar] [CrossRef]
- Hiraga, H.; Hoshino, K.; Yokoyama, E.; Takahashi, Y.; Sato, T.; Takahashi, Y.; Toratani, J.; Kuga, A.; Takahashi, A.; Watanabe, Z.; et al. Fertility Complications After Uterine Artery Embolization for Postpartum Hemorrhage: A Case of Infertility and Miscarriage Following Stillbirth. Cureus 2025, 17, e82609. [Google Scholar] [CrossRef]
- Komatsu, H.; Taniguchi, F.; Harada, T. Impact of myomectomy on the obstetric complications: A large cohort study in Japan. Int. J. Gynaecol. 2023, 162, 977–982. [Google Scholar] [CrossRef]
- Van der Kooij, S.M.; Bipat, S.; Hehenkamp, W.J.K.; Ankum, W.M.; Reekers, J.A. Uterine artery embolization vs surgery in the treatment of symptomatic fibroids: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2011, 205, 513–517. [Google Scholar] [CrossRef]
- Kinariwala, D.J.; Khaja, M.S.; McCann, S.; Sheeran, D.; Park, A.W.; Stone, J.; Wilkins, L.R.; Matsumoto, A.H.; Redick, D.L. Preoperative uterine artery embolization before hysterectomy or myomectomy: A single-center review of 53 patients. Clin. Imaging 2023, 101, 121–125. [Google Scholar] [CrossRef]
- Liu, W.M.; Tzeng, C.R.; Yi-Jen, C.; Wang, P.H. Combining the uterine depletion procedure and myomectomy may be useful for treating symptomatic fibroids. Fertil. Steril. 2004, 82, 205–210. [Google Scholar] [CrossRef]
- Leo, L.; Thomasset, R.; Massaro, A.; Tinelli, R.; Masturzo, B.; Remorgida, V.; Libretti, A.; Natrella, M. A 40-year-old woman with inoperable uterine fibroids treated with combined uterine artery embolization and relugolix. Am. J. Case Rep. 2025, 26, e946334. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).