Burnout, Sleep, and Sleepiness during Day and Night Shifts in Transition from 8- to 12-Hour Shift Rosters among Airline Ground Crew Managers

 ,
, 

Abstract
:1. Introduction
2. Results
2.1. Background Variables
2.2. Confounding Variables: Napping and Caffeine
2.2.1. Napping during the 12-h Night Shift
2.2.2. Caffeine Intake during 8/12-h Night Shifts
2.3. Burnout
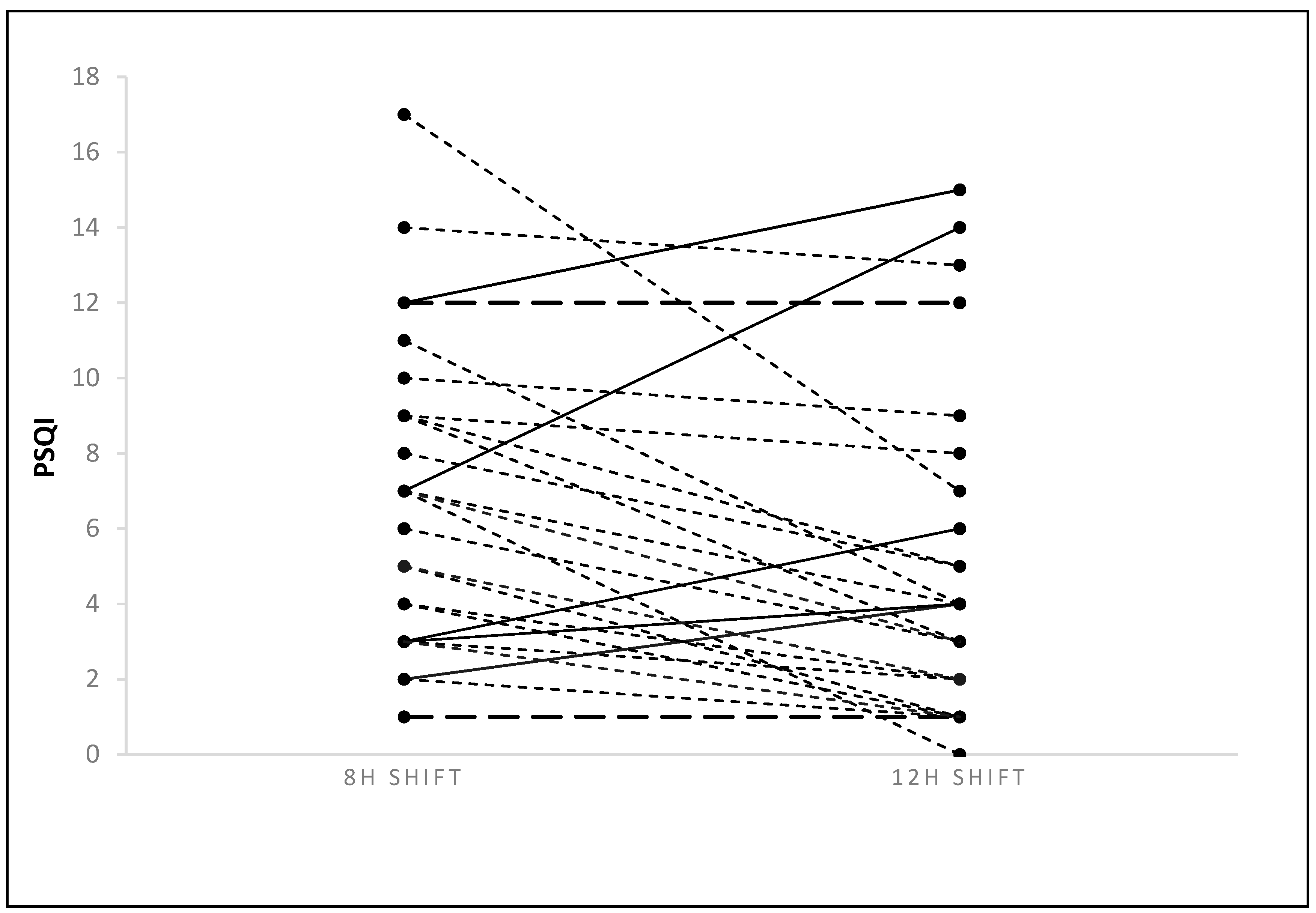
2.4. Sleep Quality (PSQI and Actigraphy)
2.5. Sleepiness
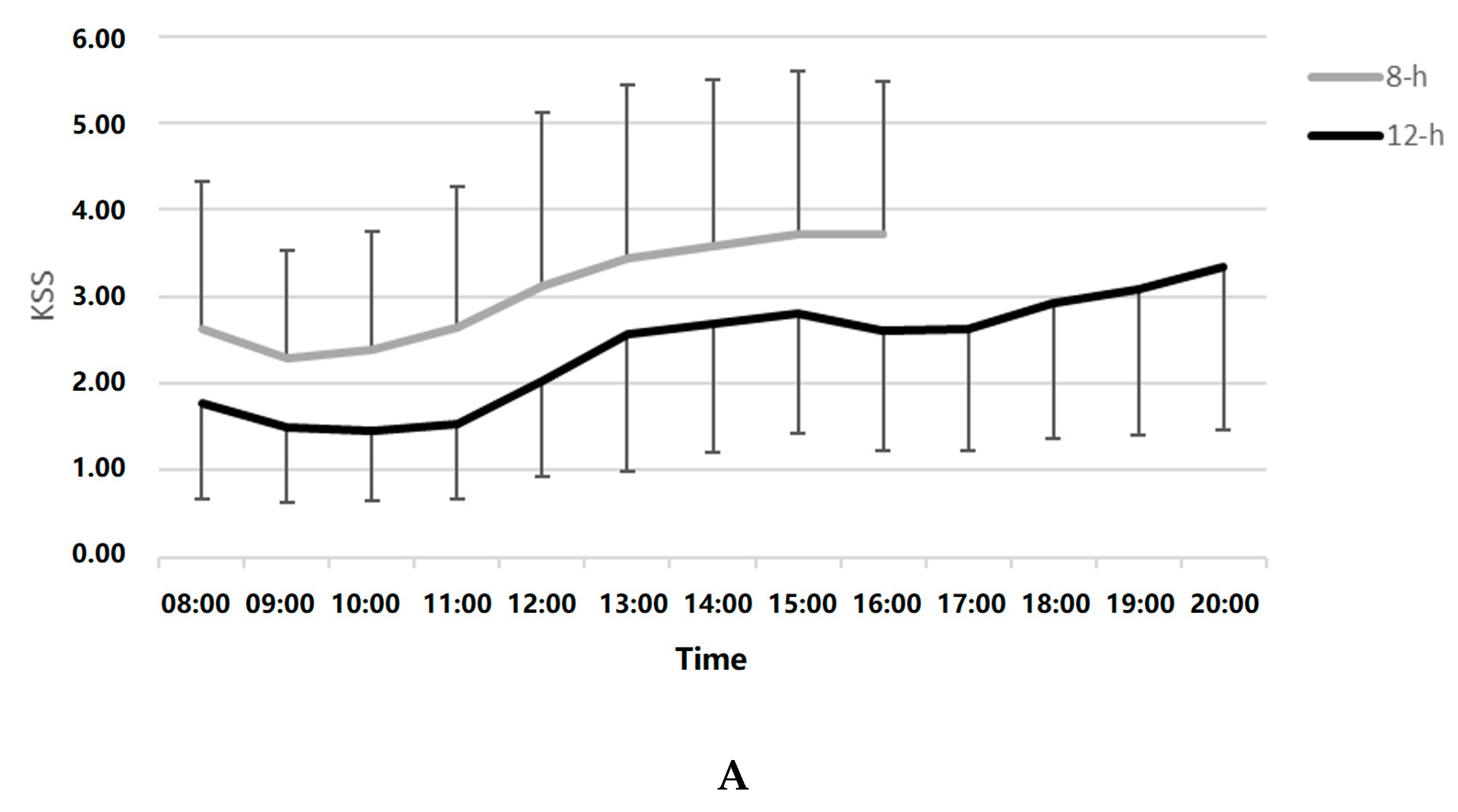
2.5.1. Day Shift Sleepiness by Shift and Hour
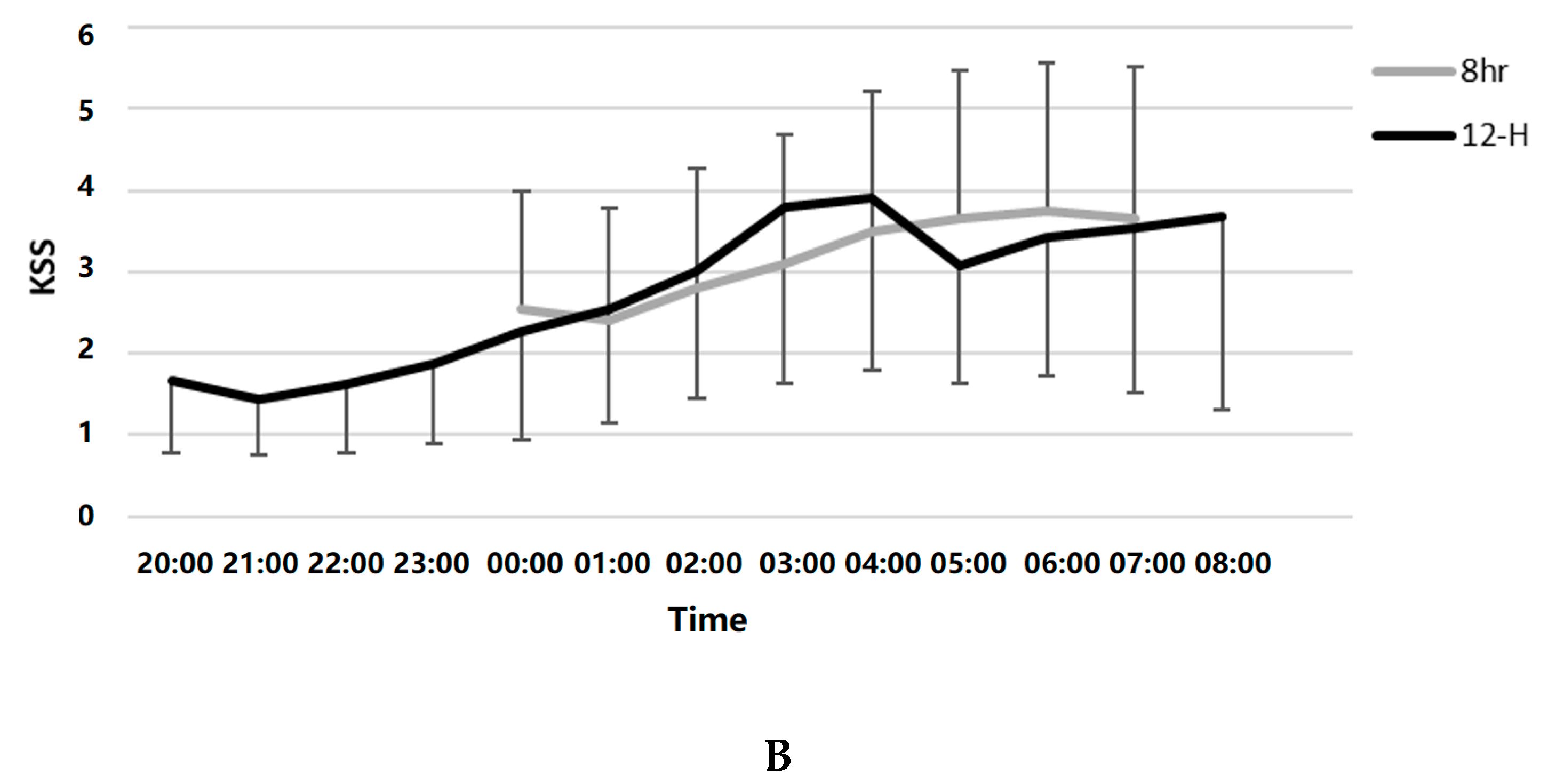
2.5.2. Night Shift Sleepiness by Shift and Hour
Night Shift Sleepiness by Shift, Hour, Nap, and Caffeine
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Participants
4.3. Measures
4.4. Procedure
4.5. Data Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| 8-h | 8-hour |
| 12-h | 12-hour |
| SMBM | Shirom-Melamed Burnout Measure |
| PSQI | Pittsburgh Sleep Quality Index |
| KSS | Karolinska Sleepiness Scale |
References
- Reid, K.J.; Weng, J.; Ramos, A.R.; Zee, P.C.; Daviglus, M.; Mossavar-Rahmani, Y.; Sotres-Alvarez, D.; Gallo, L.C.; Chirinos, D.A.; Patel, S.R. Impact of Shift Work Schedules on Actigraphy-Based Measures of Sleep in Hispanic Workers: Results from the Hispanic Community Health Study/Study of Latinos Ancillary Sueño Study. Sleep 2018, 41, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Voinescu, B.I. Common Sleep, Psychiatric, and Somatic Problems According to Work Schedule: An Internet Survey in an Eastern European Country. Int. J. Behav. Med. 2018, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Vedaa, Ø.; Mørland, E.; Larsen, M.; Harris, A.; Erevik, E.; Sivertsen, B.; Bjorvatn, B.; Waage, S.; Pallesen, S. Sleep Detriments Associated with Quick Returns in Rotating Shift Work. J. Occup. Environ. Med. 2017, 59, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Åkerstedt, T.; Kecklund, G. What Work Schedule Characteristics Constitute a Problem to the Individual? A Representative Study of Swedish Shift Workers. Appl. Ergon. 2017, 59, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Ihlström, J.; Kecklund, G.; Anund, A. Split-Shift Work in Relation to Stress, Health and Psychosocial Work Factors among Bus Drivers. Work 2017, 56, 531–538. [Google Scholar] [CrossRef]
- Dall’Ora, C.; Griffiths, P.; Ball, J.; Simon, M.; Aiken, L.H. Association of 12 h Shifts and Nurses’ Job Satisfaction, Burnout and Intention to Leave: Findings from a Cross-Sectional Study of 12 European Countries. BMJ Open 2015, 5, e008331. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, S.A.; Dawson, D. 12-h or 8-h Shifts? It Depends. Sleep Med. Rev. 2012, 16, 519–528. [Google Scholar] [CrossRef]
- Tucker, P.; Macdonald, I.; Folkard, S.; Smith, L. The Impact of Early and Late Shift Changeovers on Sleep, Health, and Well-Being in 8- and 12-Hour Shift Systems. J. Occup. Health Psychol. 1998, 3, 265–275. [Google Scholar] [CrossRef]
- Smith, L.; Folkard, S.; Tucker, P.; Macdonald, I. Work Shift Duration: A Review Comparing Eight Hour and 12 Hour Shift Systems. Occup. Environ. Med. 1998, 55, 217–229. [Google Scholar] [CrossRef]
- Mitchell, R.J.; Williamson, A.M. Evaluation of an 8 Hour versus a 12 Hour Shift Roster on Employees at a Power Station. Appl. Ergon. 2000, 31, 83–93. [Google Scholar] [CrossRef]
- Oh, J.-I.; Yim, H.W. Association between Rotating Night Shift Work and Metabolic Syndrome in Korean Workers: Differences between 8-Hour and 12-Hour Rotating Shift Work. Ind. Health 2018, 56, 40–48. [Google Scholar] [CrossRef]
- Peacock, B.; Glube, R.; Miller, M.; Clune, P. Police Officers’ Responses to 8 and 12 Hour Shift Schedules. Ergonomics 1983, 26, 479–493. [Google Scholar] [CrossRef]
- Rosa, R.R.; Colligan, M.J.; Lewis, P. Extended Workdays: Effects of 8-Hour and 12-Hour Rotating Shift Schedules on Performance, Subjective Alertness, Sleep Patterns, and Psychosocial Variables. Work Stress 1989, 3, 21–32. [Google Scholar] [CrossRef]
- Rosa, R.R. Performance, Alertness, and Sleep after 3·5 Years of 12 h Shifts: A Follow-up Study. Work Stress 1991, 5, 107–116. [Google Scholar] [CrossRef]
- Rosa, R.R.; Bonnet, M.H. Performance and Alertness on 8 h and 12 h Rotating Shifts at a Natural Gas Utility. Ergonomics 1993, 36, 1177–1193. [Google Scholar] [CrossRef]
- Williamson, A.M.; Gower, C.G.I.I.; Clarke, B.C. Changing the Hours of Shiftwork: A Comparison of 8- and 12-Hour Shift Rosters in a Group of Computer Operators∗. Ergonomics 1994, 37, 287–298. [Google Scholar] [CrossRef]
- Stimpfel, A.W.; Sloane, D.M.; Aiken, L.H. The Longer The Shifts For Hospital Nurses, The Higher The Levels Of Burnout And Patient Dissatisfaction. Health Aff. 2012, 31, 2501–2509. [Google Scholar] [CrossRef]
- Estryn-Béhar, M.; Van Der Heijden, B.I.J.M. Effects of Extended Work Shifts on Employee Fatigue, Health, Satisfaction, Work/Family Balance, and Patient Safety. Work 2012, 41 (Suppl. 1), 4283–4290. [Google Scholar]
- Stone, P.W.; Du, Y.; Cowell, R.; Amsterdam, N.; Thomas, A.; Linn, R.W.; Gladstein, A.; Walsh, M.; Mojica, L.A. Comparison of Nurse, System and Quality Patient Care Outcomes in 8-Hour and 12-Hour Shifts. Med. Care 2016, 44, 1099–1106. [Google Scholar] [CrossRef]
- Portela, L.F.; Luna, C.K.; Rotenberg, L.; Silva-Costa, A.; Toivanen, S.; Araújo, T.; Griep, R.H. Job Strain and Self-Reported Insomnia Symptoms among Nurses: What about the Influence of Emotional Demands and Social Support? Biomed Res. Int. 2015, 2015, 1–8. [Google Scholar] [CrossRef]
- Dall’Ora, C.; Ball, J.; Recio-Saucedo, A.; Griffiths, P. Characteristics of Shift Work and Their Impact on Employee Performance and Wellbeing: A Literature Review. Int. J. Nurs. Stud. 2016, 57, 12–27. [Google Scholar] [CrossRef]
- Zion, N.; Drach-Zahavy, A.; Shochat, T. Who Is Sleepier on the Night Shift? The Influence of Bio-Psycho-Social Factors on Subjective Sleepiness of Female Nurses during the Night Shift. Ergonomics 2018, 61, 1004–1014. [Google Scholar] [CrossRef]
- Zion, N.; Shochat, T. Cognitive Functioning of Female Nurses during the Night Shift: The Impact of Age, Clock Time, Time Awake and Subjective Sleepiness. Chronobiol. Int. 2018, 35, 1595–1607. [Google Scholar] [CrossRef] [PubMed]
- Tremaine, R.; Dorrian, J.; Lack, L.; Lovato, N.; Ferguson, S.; Zhou, X.; Roach, G. The Relationship between Subjective and Objective Sleepiness and Performance during a Simulated Night shift with a Nap Countermeasure. Appl. Ergon. 2010, 42, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Zion, N.; Shochat, T. Let Them Sleep: The Effects of a Scheduled Nap during the Night Shift on Sleepiness and Cognition in Hospital Nurses. J. Adv. Nurs. (Acceptance). [CrossRef] [PubMed]
- Centofanti, S.; Banks, S.; Colella, A.; Dingle, C.; Devine, L.; Galindo, H.; Pantelios, S.; Brkic, G.; Dorrian, J. Coping with Shift Work-Related Circadian Disruption: A Mixed-Methods Case Study on Napping and Caffeine Use in Australian Nurses and Midwives. Chronobiol. Int. 2018, 35, 853–864. [Google Scholar] [CrossRef]
- Van Dongen, H.P.A.; Baynard, M.D.; Maislin, G.; Dinges, D.F. Systematic Interindividual Differences in Neurobehavioral Impairment from Sleep Loss: Evidence of Trait-Like Differential Vulnerability. Sleep 2004, 27, 423–433. [Google Scholar]
- Van Dongen, H.P.A.; Caldwell, J.A.; Caldwell, J.L. Investigating Systematic Individual Differences in Sleep-Deprived Performance on a High-Fidelity Flight Simulator. Behav. Res. Methods 2006, 38, 333–343. [Google Scholar] [CrossRef]
- Shirom, A.; Melamed, S. A Comparison of the Construct Validity of Two Burnout Measures in Two Groups of Professionals. Int. J. Stress Manag. 2006, 13, 176–200. [Google Scholar] [CrossRef]
- Armon, G.; Shirom, A.; Shapira, I.; Melamed, S. On the Nature of Burnout–insomnia Relationships: A Prospective Study of Employed Adults. J. Psychosom. Res. 2008, 65, 5–12. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Shochat, T.; Tzischinsky, O.; Oksenberg, A.; Peled, R. Validation of the Pittsburgh Sleep Quality Index Hebrew Translation (PSQI-H) in a Sleep Clinic Sample. Isr. Med. Assoc. J. 2007, 9, 853–856. [Google Scholar]
- Åkerstedt, T.; Gillberg, M. Subjective and Objective Sleepiness in the Active Individual. Int. J. Neurosci. 1990, 52, 29–37. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 8-h Shift | 12-h Shift | Statistic, p-Value, Effect Size | |||
|---|---|---|---|---|---|
| Burnout | |||||
| Physical strength | 3.91 (1.36) | 2.88 (1.15) | F(1,30) = 13.55 | p = 0.001 | η2 = 0.93 |
| Vitality thinking | 2.61 (1.11) | 2.06 (1.00) | F(1,30) = 6.46 | p = 0.016 | η2 = 0.89 |
| Mental energy | 2.37 (1.13) | 1.82 (0.93) | F(1,30) = 5.79 | p = 0.022 | η2 = 0.15 |
| Total score | 3.12 (1.04) | 2.34 (0.96) | t = 3.88 | p = 0.002 | η2 = 0.25 |
| Sleep Quality (Pittsburgh Sleep Quality Index; PSQI) | |||||
| Total score | 6.51 (3.88) | 4.61 (4.07) | t = 3.19 | p = 0.003 | η2 = 0.25 |
| PSQI > 5 | 75.0% | 42.1% | X2 = 5.56 | p = 0.02 | McNemar = 0.02 |
| 8-h Shift | 12-h Shift | Statistic, p-Value, Effect Size | |||
|---|---|---|---|---|---|
| Day sleep after night shift | |||||
| Time in Bed (hours) | (1.34) 5.34 | (1.51) 4.59 | F(1,21) = 3.38 | p = 0.08 | η2 = 0.139 |
| Total Sleep Time (hours) | (1.16) 4.44 | (1.47) 3.87 | F(1,21) = 2.29 | p = 0.14 | η2 = 0.098 |
| Sleep Efficiency (%) | (9.13) 82.94 | (8.19) 83.72 | F(1,21) = 0.14 | p = 0.71 | η2 = 0.007 |
| Night sleep after day shift | |||||
| Time in Bed (hours) | (1.26) 6.34 | (1.31) 6.55 | F(1,13) = 0.204 | p = 0.65 | η2 = 0.015 |
| Total Sleep Time (hours) | (1.25) 5.44 | (1.18) 5.42 | F(1,13) = 0.002 | p = 0.96 | η2 = 0.0 |
| Sleep Efficiency (%) | (6.20) 82.60 | (6.88) 82.63 | F(1,13) = 0.001 | p = 0.98 | η2 = 0.0 |
| Naps (other than main sleep period) during the roster | |||||
| Time in Bed (hours) | (0.71) 2.1 | (0.74) 2.59 | F(1,9) = 5.7 | p = 0.04 | η2 = 0.388 |
| Total Sleep Time (hours) | (0.51) 1.6 | (0.73) 2.08 | F(1,9) = 6.47 | p = 0.03 | η2 = 0.418 |
| Sleep Efficiency (%) | (7.41) 72.61 | (9.47) 79.78 | F(1,9) = 7.57 | p = 0.02 | η2 = 0.457 |
| Mean | SE | F(df) | p | |
|---|---|---|---|---|
| Shift | 184.50 (1,226) | <0.001 | ||
| 8-h | 3.09 | 0.14 | ||
| 12-h | 0.47 | 0.20 | ||
| Hour | 2.13 (7,355) | p = 0.04 | ||
| 00:00 | 1.52 | 0.15 | ||
| 01:00 | 1.43 | 0.16 | ||
| 02:00 | 1.61 | 0.16 | ||
| 03:00 | 1.75 | 0.17 | ||
| 04:00 | 1.94 | 0.17 | ||
| 05:00 | 1.99 | 0.16 | ||
| 06:00 | 2.05 | 0.17 | ||
| 07:00 | 1.97 | 0.17 | ||
| Nap | 9.81 (1,78) | p = 0.002 | ||
| Nappers | 2.19 | 0.20 | ||
| Non-nappers | 1.37 | 0.16 | ||
| Caffeine Intake | 0.91* | 0.05 | 17.7 (438) | <0.001 |
| Day Shift | Day Shift | Day Shift | Night Shift | Night Shift | Night Shift | Free Day | Free Day | Evening Shift | Evening Shift | Evening Shift |
|---|---|---|---|---|---|---|---|---|---|---|
| Start of roster | Day assessment | Night 1 assessment | Night 2 assessment | End of roster |
| Day Shift | Night Shift | Free Day | Free Day | Day Shift | Night Shift | Free Day |
|---|---|---|---|---|---|---|
| Start of roster | Night 1 assessment | Day assessment | Night 2 assessment | End of roster |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shochat, T.; Hadish-Shogan, S.; Banin Yosipof, M.; Recanati, A.; Tzischinsky, O. Burnout, Sleep, and Sleepiness during Day and Night Shifts in Transition from 8- to 12-Hour Shift Rosters among Airline Ground Crew Managers. Clocks & Sleep 2019, 1, 226-239. https://doi.org/10.3390/clockssleep1020020
Shochat T, Hadish-Shogan S, Banin Yosipof M, Recanati A, Tzischinsky O. Burnout, Sleep, and Sleepiness during Day and Night Shifts in Transition from 8- to 12-Hour Shift Rosters among Airline Ground Crew Managers. Clocks & Sleep. 2019; 1(2):226-239. https://doi.org/10.3390/clockssleep1020020
Chicago/Turabian StyleShochat, Tamar, Satanay Hadish-Shogan, Michal Banin Yosipof, Ayelet Recanati, and Orna Tzischinsky. 2019. "Burnout, Sleep, and Sleepiness during Day and Night Shifts in Transition from 8- to 12-Hour Shift Rosters among Airline Ground Crew Managers" Clocks & Sleep 1, no. 2: 226-239. https://doi.org/10.3390/clockssleep1020020
APA StyleShochat, T., Hadish-Shogan, S., Banin Yosipof, M., Recanati, A., & Tzischinsky, O. (2019). Burnout, Sleep, and Sleepiness during Day and Night Shifts in Transition from 8- to 12-Hour Shift Rosters among Airline Ground Crew Managers. Clocks & Sleep, 1(2), 226-239. https://doi.org/10.3390/clockssleep1020020