A 95-year-old female presented to hospital with a 3-day history of worsening right-sided flank pain, on background of recent heavy lifting. The pain was dull in nature and centred over a bulge at her right flank. It was not associated with any subjective fevers, bowel disturbance, or urinary symptoms. Examination identified an uncomfortable but haemodynically normal patient. Abdominal examination revealed a soft abdomen with a tender, palpable mass over the right flank in line with a surgical scar. The mass was reducible but would spontaneously re-herniate on cessation of pressure.
The patient had a significant history of a right- sided minimally invasive lateral transpsoas L1-5 spinal fusion (also known as a direct lateral inter- body fusion [DLIF]) 6-years earlier. Other significant history included atrial fibrillation on anticoagulation, cerebrovascular attack on aspirin, breast cancer, and recurrent urinary tract infections. She lived at home independently.
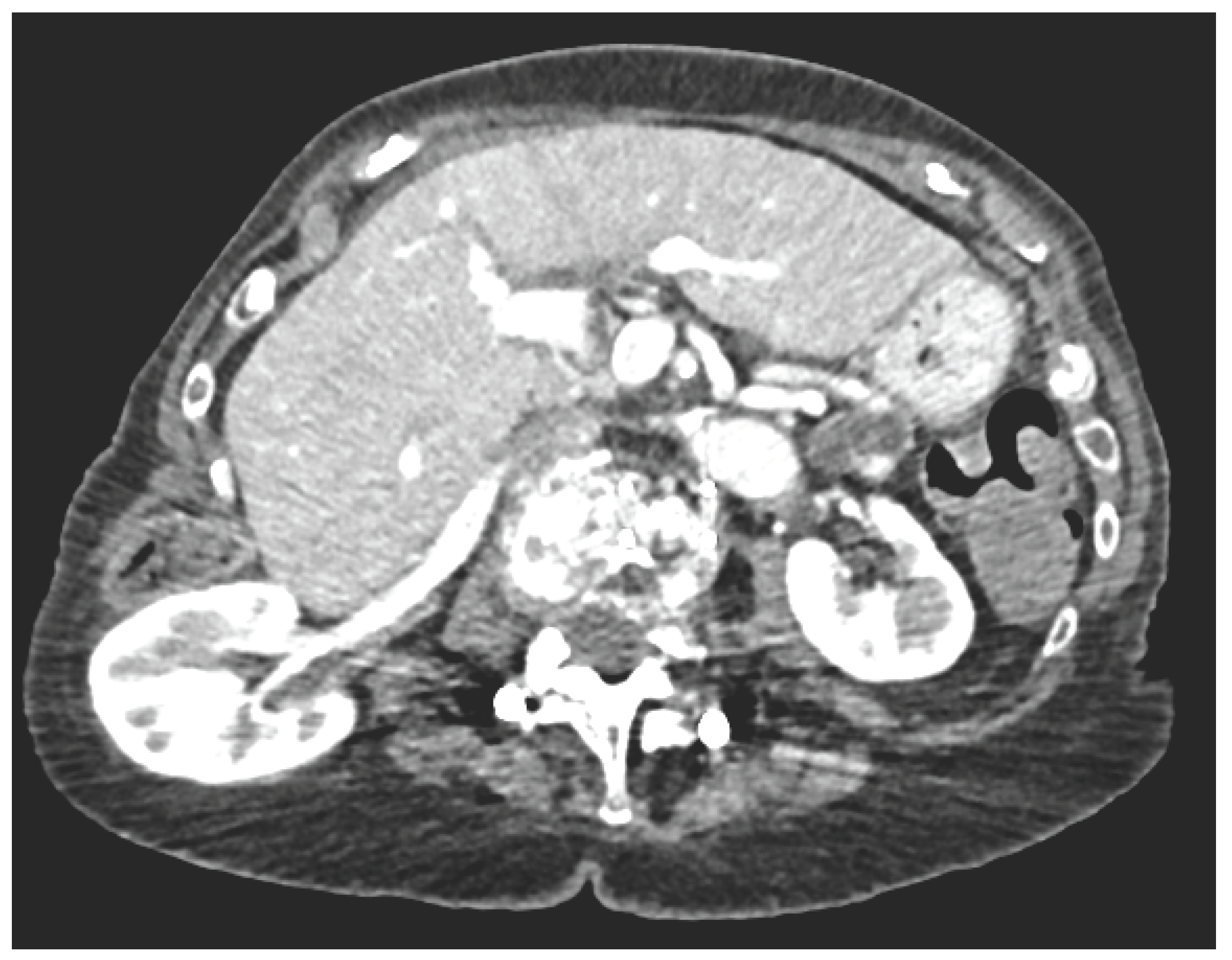
Biochemistry and inf lammatory markers were normal. CT imaging demonstrated a right renal flank hernia through the retroperitoneum into the subcutaeneous tissue (Figure 1A,B). The renal artery and vein were significantly stretched, without evidence of acute pathology. There was no evidence of hydronephrosis or delayed nephrogram.
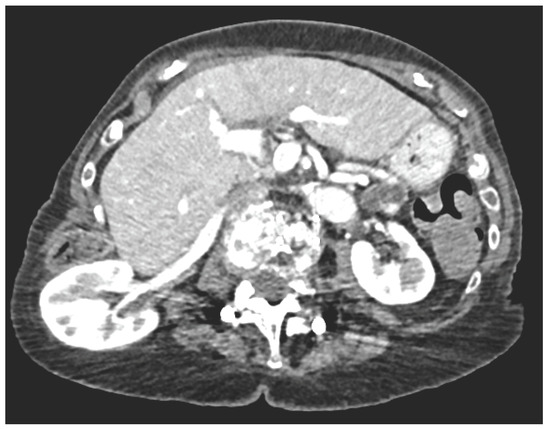

Figure 1.
A. Axial CT. B. Sagittal CT.
The patient was monitored overnight and discharged on simple analgesia. After follow-up discussion with the patient, and given her age and comorbidities, the decision at this stage has been to take a conservative approach with use of a body vest to keep the kidney within the retroperitoneum.
Patient Consent
Obtained.
Conflicts of Interest
None declared.

This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2022 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.