Keywords:
Urethra; carcinoma; squamous cell; urinary retention; urethral stricture; penile neoplasms Primary urethral squamous cell carcinomas (SCCs) are rare, with a variable clinical presentation, and occur infrequently in patients younger than 45 years of age [1,2,3]. The surgical management for advanced urethral SCCs remains challenging, given it occurs in less than 1 in 100 000 men [1,4]. We describe the diagnosis and management of urethral SCC in a 37-year-old male presenting with urinary retention.
The patient initially presented to our emergency department with fevers, perineal pain on voiding, and high post-void residuals. His history included recurrent bulbar urethral strictures, UTIs, smoking, and intra- venous drug use. His urethral stricture was previously endoscopically managed with dilatation, but the patient had been lost to follow-up.
An initial pelvic ultrasound revealed a complex peri- neal mass inferior to the prostate and contiguous with the urethra. Pelvic MRI subsequently revealed 2 lesions in the perineum (Figure 1). FDGPET-scan demon- strated avid lesions in the right inguinal and meso-rectal nodes with no distal metastatic disease. Urine cytology suggested malignant cells suspicious for SCC. On pelvic examination, 2 distinct masses were palpable in the bulbar urethra and rectum. Cystoscopy demonstrated an obliterated urethra that could not be cannulated with a wire, thus a suprapubic catheter was placed.
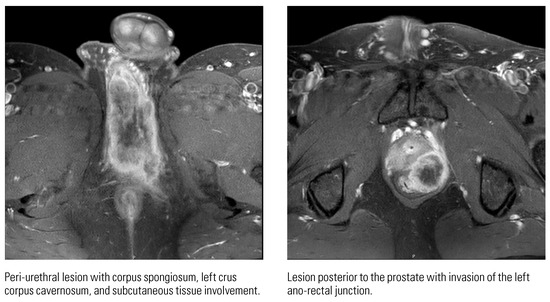
Figure 1.
Pelvic MRI demonstrating 2 lesions in the perineum.
Because of the severity of local symptoms, the patient was discussed in a multi-disciplinary team meeting and transferred to a specialist centre for pelvic exenteration. Before adjuvant chemo-radiotherapy was begun, the patient was identified to have significant local disease recurrence and opted instead for palliative treatment.
Primary urethral SCCs are a rare cause for advanced cancer in young men. This case exhibits the need for considering neoplasms as a differential diagnosis for young patients presenting with urinary retention and perineal pain. It also highlights the need for close follow-up of recurrent urethral stricture patients to ensure there are no complications of their disease.
Conflicts of Interest
None declared.
Patient Consent
Obtained.
References
- Hakenberg, O.W.; Compérat, E.; Minhas, S.; Necchi, A.; Protzel, C.; Watkin, N.; et al. EAU guidelines on penile cancer.2019. Available online: http:// uroweb.org/guideline/penile-cancer/ (accessed on 11 January 2022).
- Antwerpen, I.; Gstrein, L.; Moskovszky, L.; Gissler, H.M.; Möltgen, T.; Kwiatkowski, M.; et al. Primary urethral squamous cell carcinoma: a unique manifestation of a penile tumor. J Int Med Res. 2019, 47, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Castiglione, F.; Alnajjar, H.M.; Christodoulidou, M.; Albersen, M.; Parnham, A.; Freeman, A.; et al. Primary squamous cell carcinoma of the male proximal urethra: outcomes from a single centre. Eur Urol Focus 2021, 7, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Janisch, F.; Abufaraj, M.; Fajkovic, H.; Kimura, S.; Iwata, T.; Nyirady, P.; et al. Current disease management of primary urethral carcinoma. Eur Urol Focus 2019, 5, 722–734. [Google Scholar] [CrossRef] [PubMed]
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2022 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.