An Insight into Knowledge, Perspective, and Practices of Indian Optometrists towards Childhood Myopia


Abstract
1. Introduction
2. Methods
2.1. Practitioner’s Survey
Sample Size
2.2. Questionnaire Design
- Understanding of the natural history and ocular complications associated with myopia.
- Clinical practice behavior related to the diagnosis and management of myopia in children aged 16 years or younger.
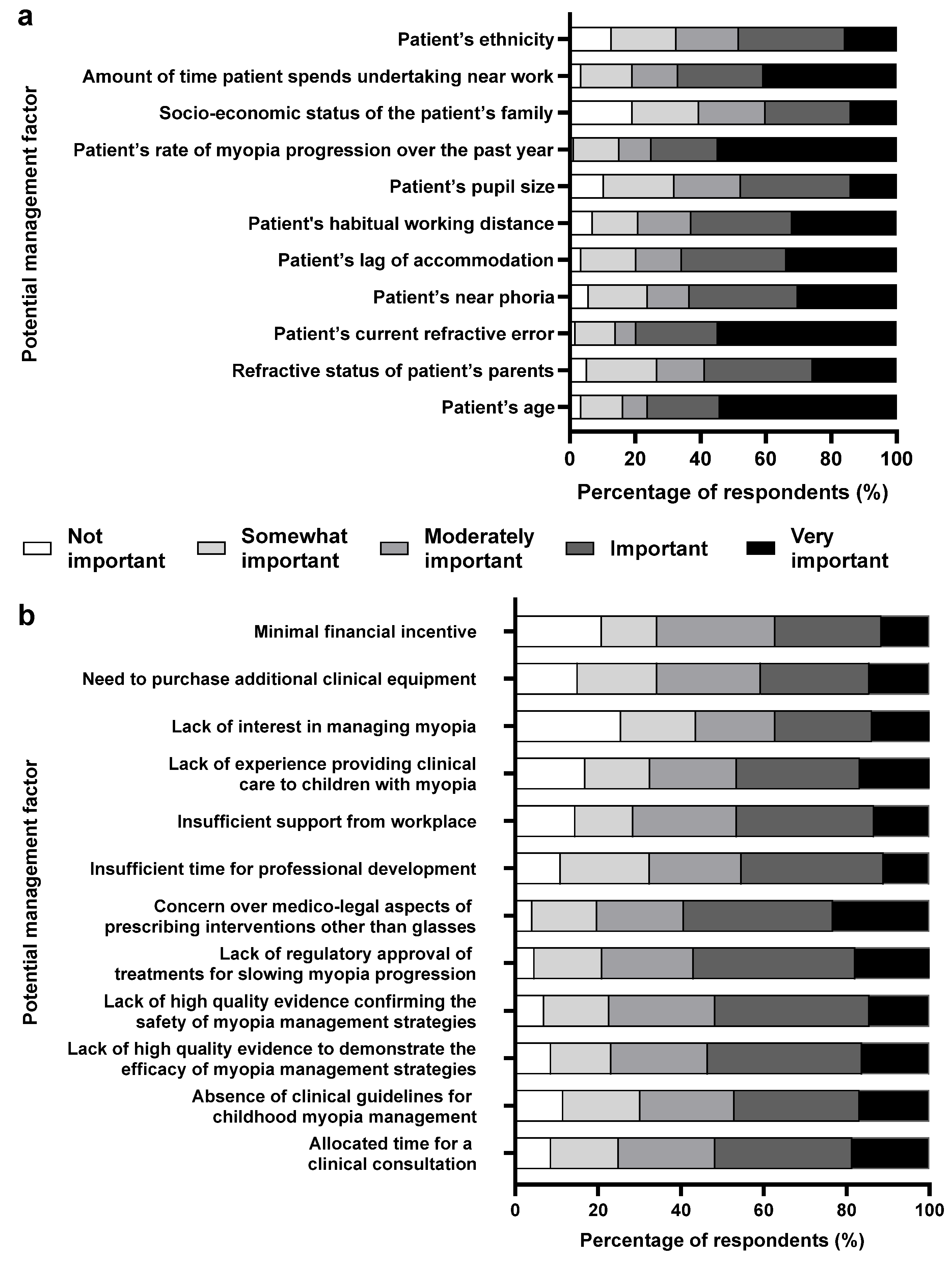
- Potential barriers to providing optimal myopia care.
- Source of evidence that clinicians use as a guide to their practice.
- Extent to which adult caregivers are involved during the decision-making process in treating childhood myopia.
2.3. Data Analysis
3. Results
3.1. Knowledge of Childhood Myopia and Its Complications
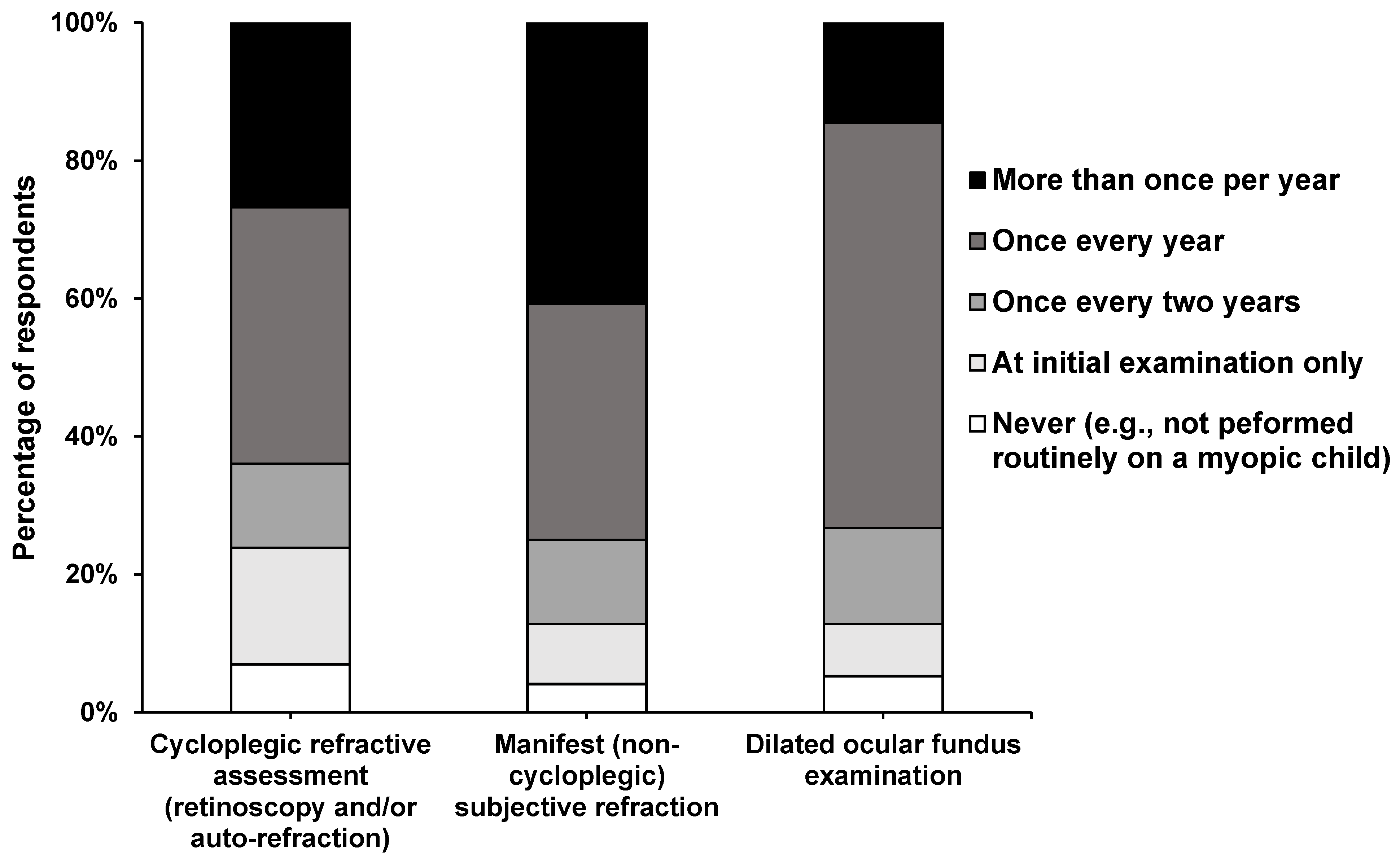
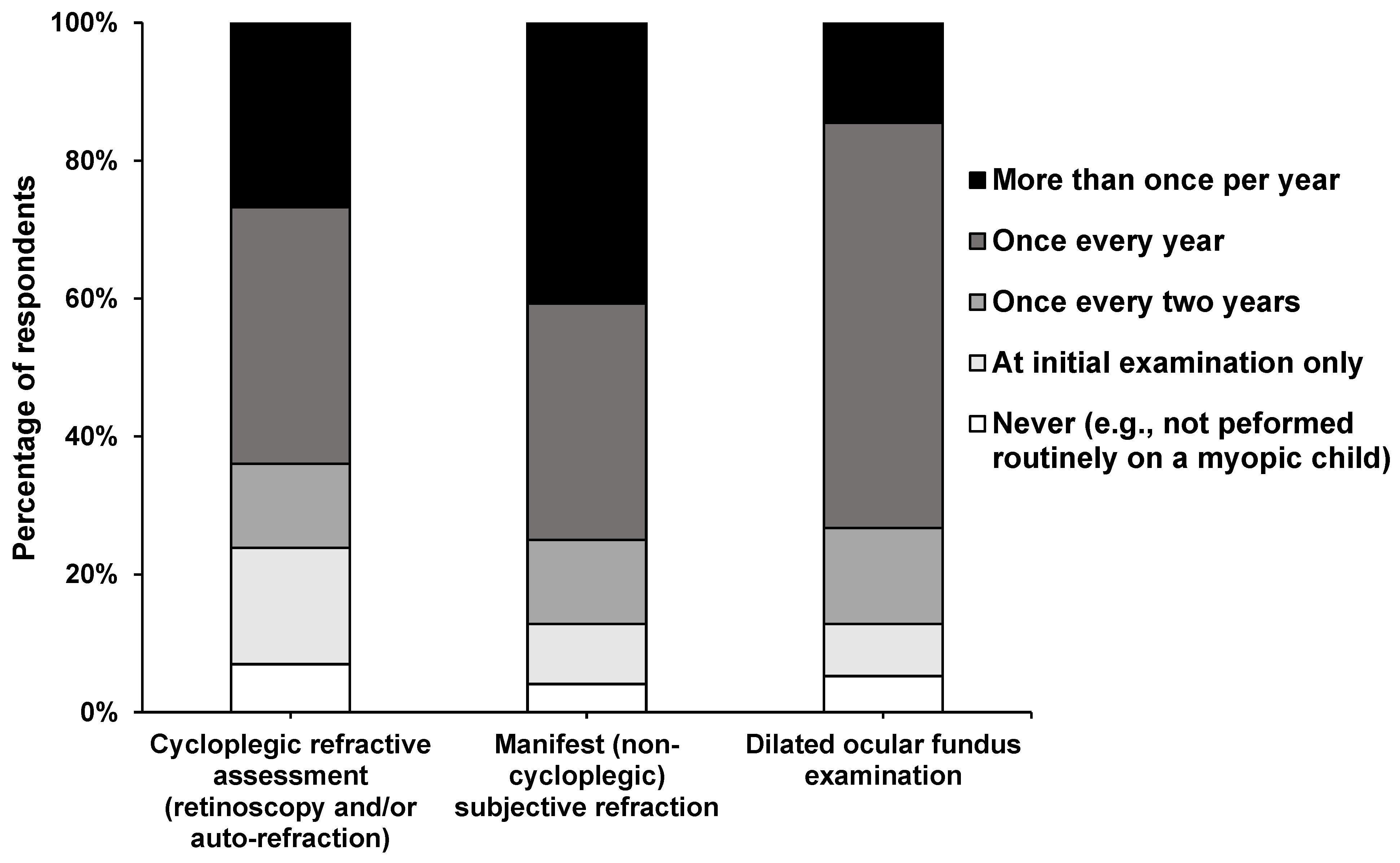
3.2. Clinical Workup and Diagnosis of Childhood Myopia
3.3. Perception on Intervention
3.4. Influential Factors on Management Approach
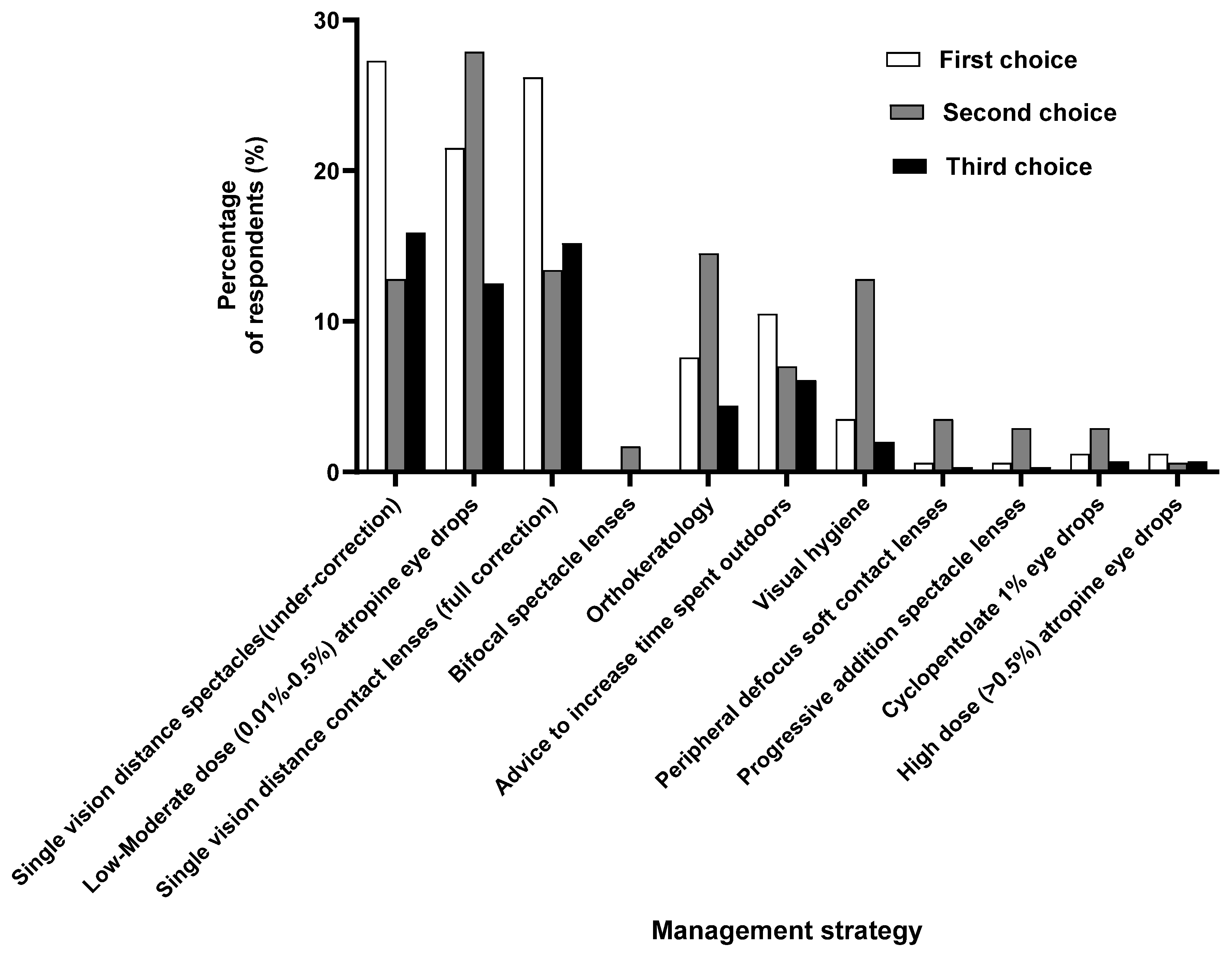
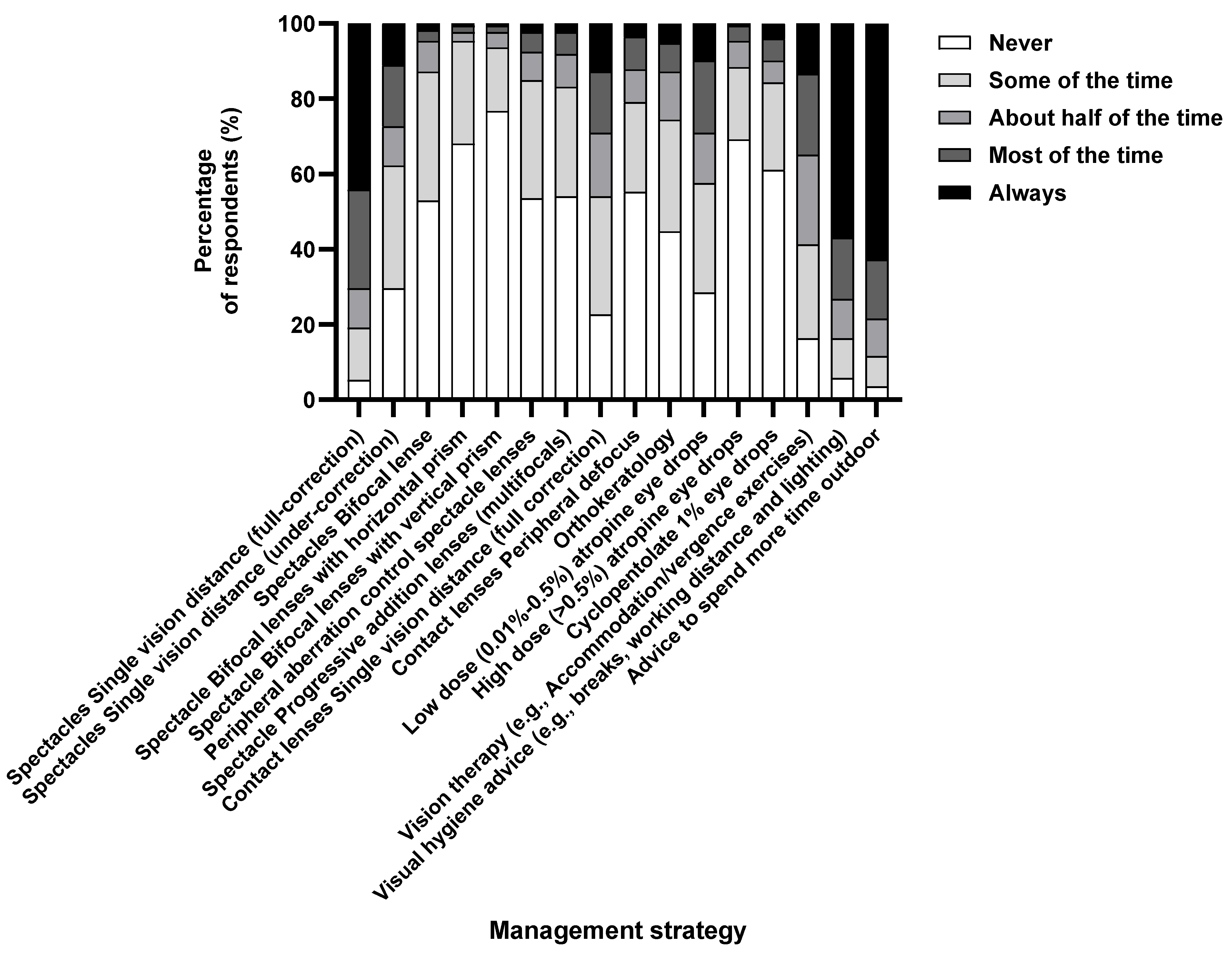
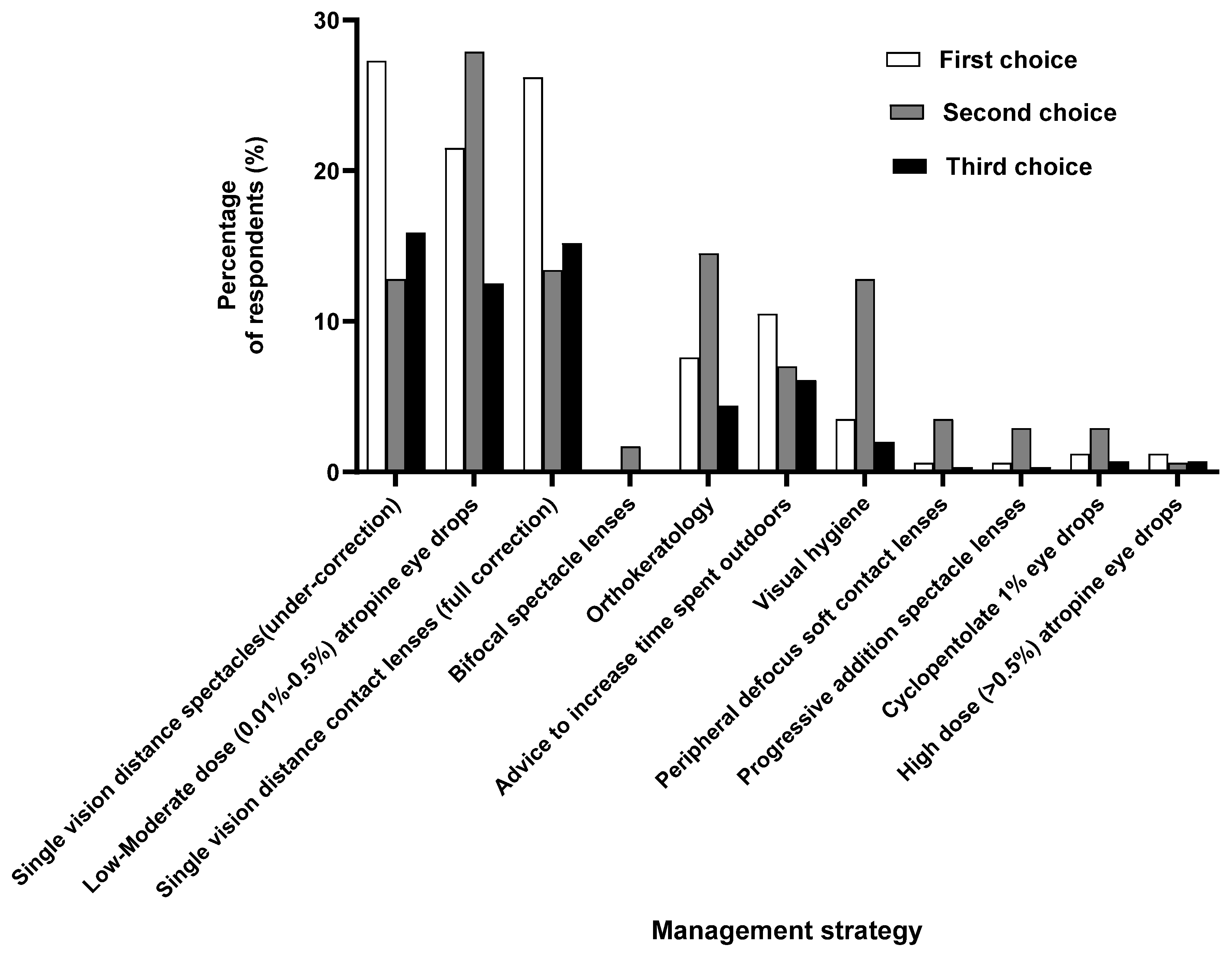
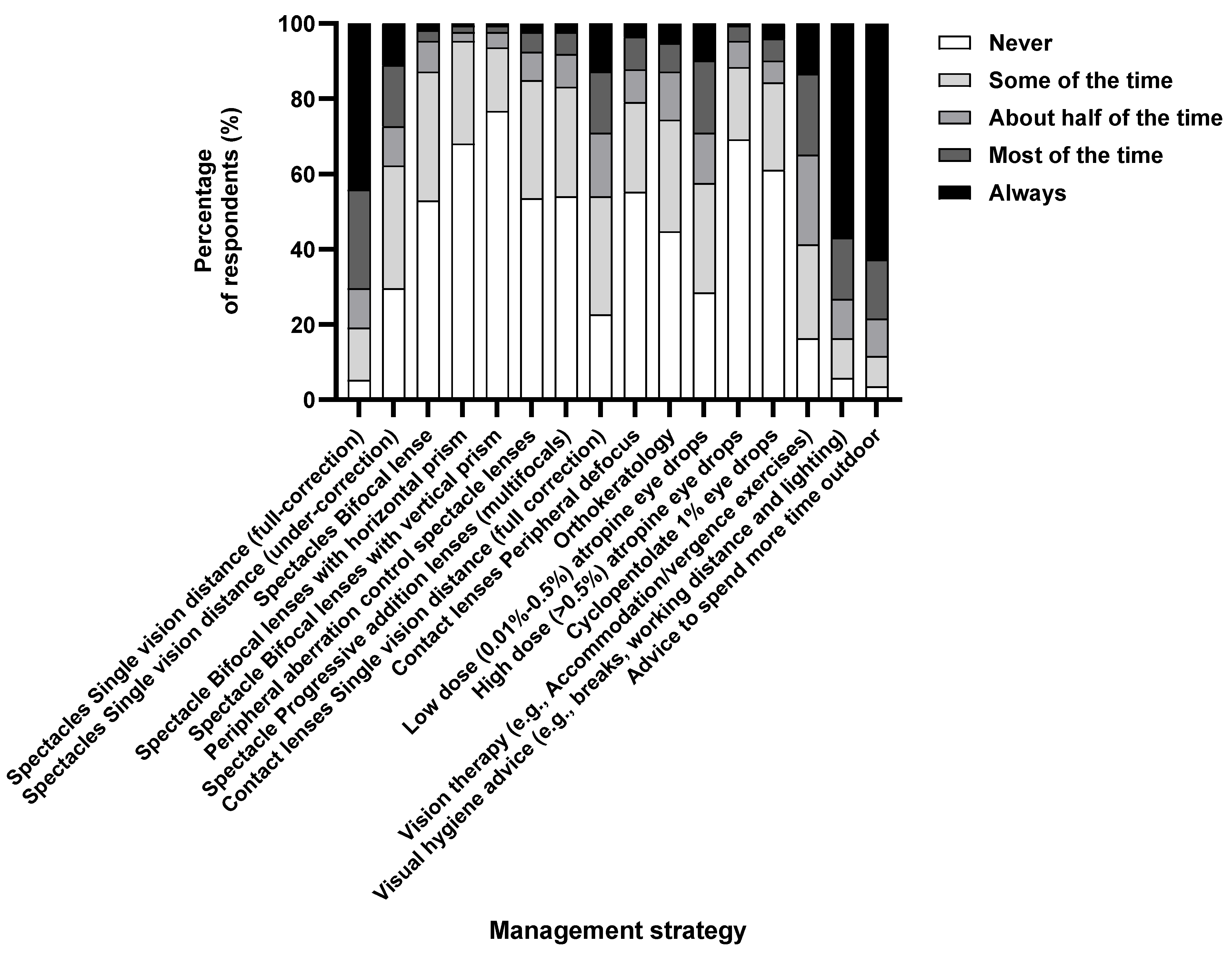
3.5. Management Approaches to Myopia in Children
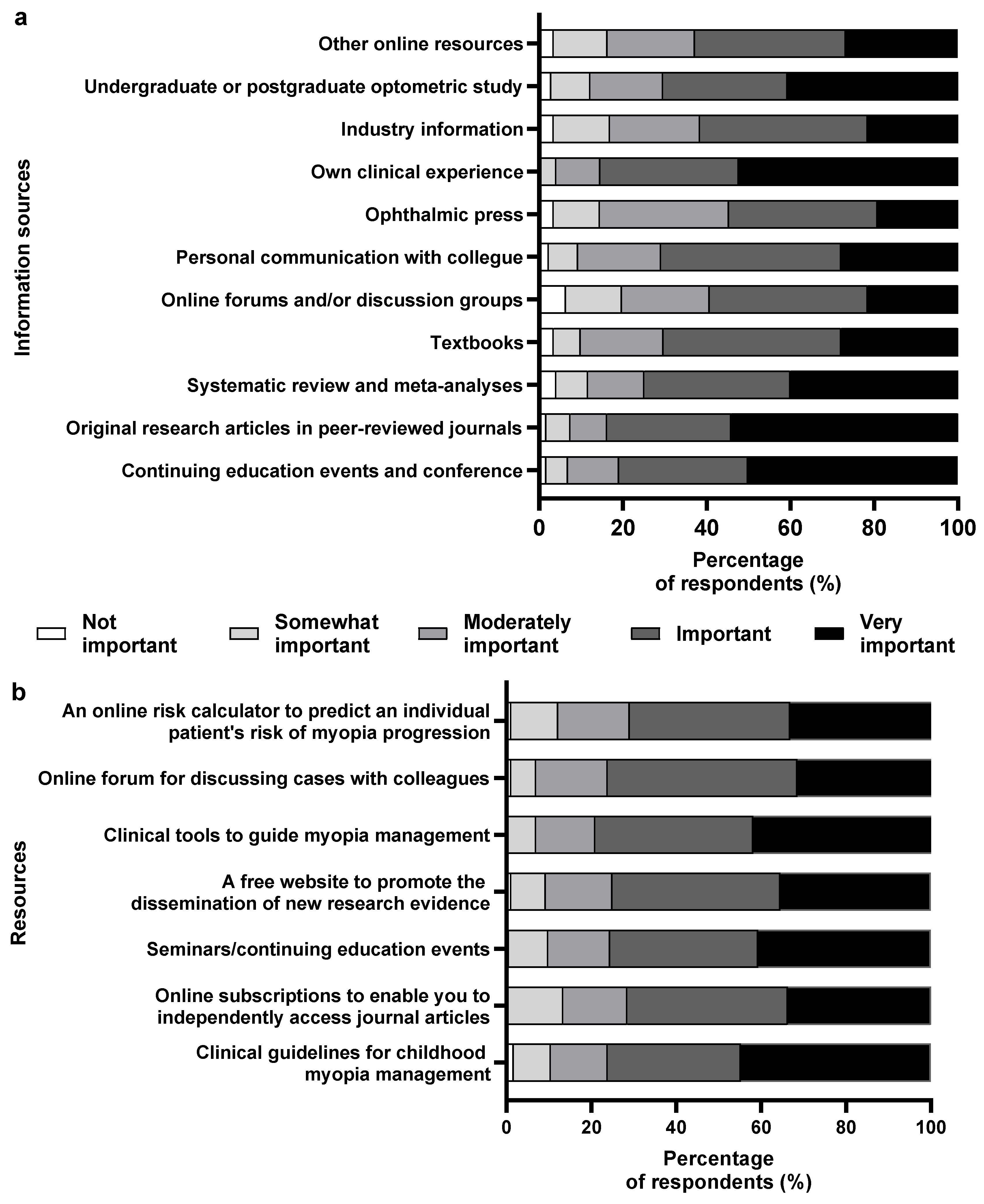
3.6. Source of Information
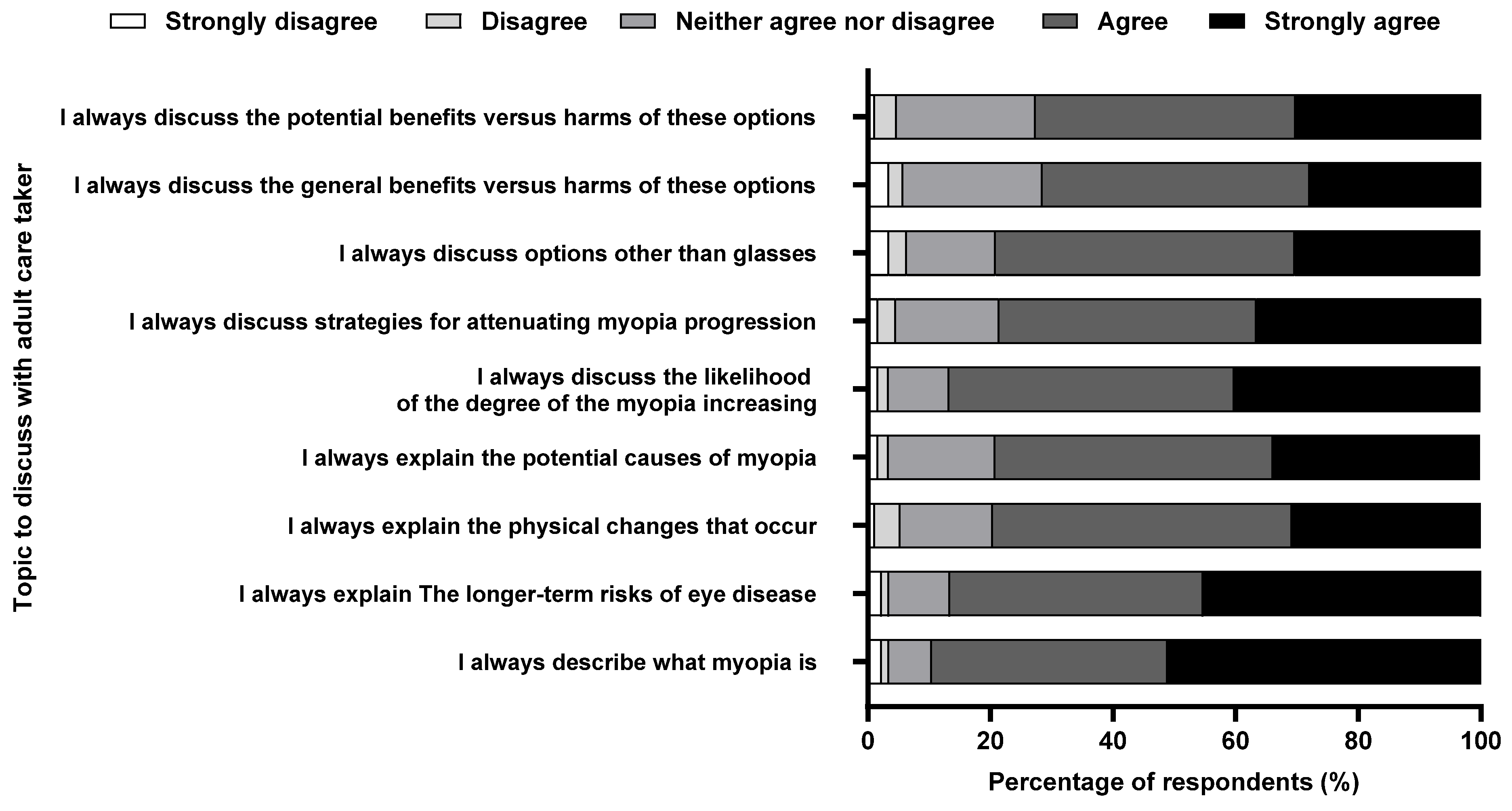
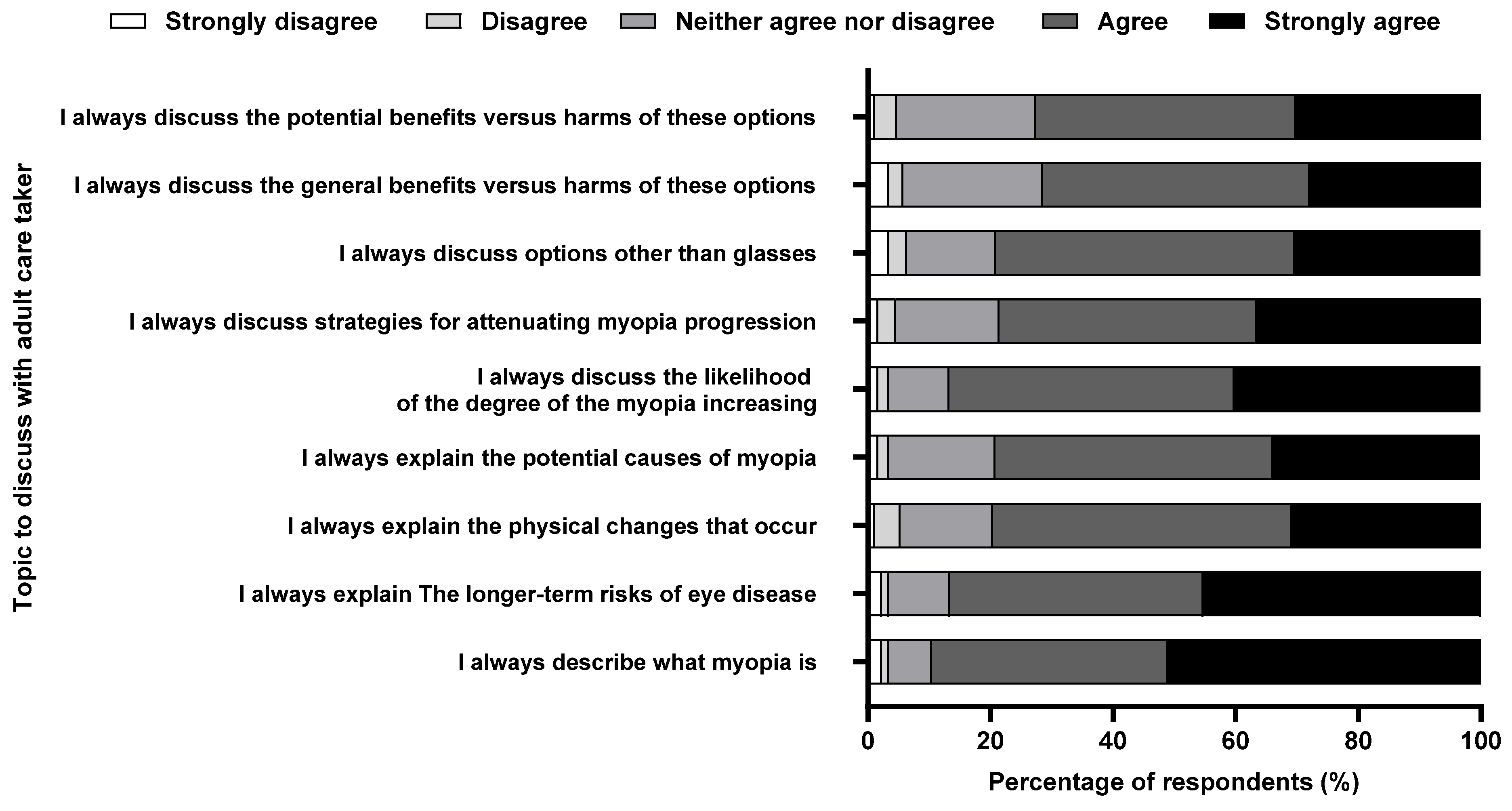
3.7. Engagement with Caregivers
4. Discussion
4.1. Complications of High Myopia
4.2. Risk Factors
4.3. Clinical Assessment
4.4. Management
4.5. Cessation
4.6. Source of Information
4.7. Caregiver
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sankaridurg, P.; Tahhan, N.; Kandel, H.; Naduvilath, T.; Zou, H.; Frick, K.D.; Marmamula, S.; Friedman, D.S.; Lamoureux, E.; Keeffe, J.; et al. IMI Impact of Myopia. Investig. Ophthalmol. Vis. Sci. 2021, 62, 2. [Google Scholar] [CrossRef] [PubMed]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Priscilla, J.J.; Verkicharla, P.K. Time trends on the prevalence of myopia in India—A prediction model for 2050. Ophthalmic Physiol. Opt. 2021, 41, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Ohno-Matsui, K.; Wu, P.C.; Yamashiro, K.; Vutipongsatorn, K.; Fang, Y.; Cheung, C.M.G.; Lai, T.Y.Y.; Ikuno, Y.; Cohen, S.Y.; Gaudric, A.; et al. IMI Pathologic Myopia. Investig. Ophthalmol. Vis. Sci. 2021, 62, 5. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.; Jhanji, V.; Leung, C.K. Prevalence of Glaucoma in Myopic Corneal Refractive Surgery Candidates in Hong Kong China. J. Refract. Surg. (1995) 2016, 32, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Chua, S.Y.; Sabanayagam, C.; Cheung, Y.B.; Chia, A.; Valenzuela, R.K.; Tan, D.; Wong, T.Y.; Cheng, C.Y.; Saw, S.M. Age of onset of myopia predicts risk of high myopia in later childhood in myopic Singapore children. Ophthalmic Physiol. Opt. 2016, 36, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Wolffsohn, J.S.; Whayeb, Y.; Logan, N.S.; Weng, R. IMI-Global Trends in Myopia Management Attitudes and Strategies in Clinical Practice-2022 Update. Investig. Ophthalmol. Vis. Sci. 2023, 64, 6. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.; El Kareh, A.; Qureshi, M.; Lee, D.M.X.; Sun, C.H.; Lam, J.S.H.; Saw, S.M.; Najjar, R.P. The influence of the environment and lifestyle on myopia. J. Physiol. Anthropol. 2024, 43, 7. [Google Scholar] [CrossRef] [PubMed]
- Gifford, K.L.; Richdale, K.; Kang, P.; Aller, T.A.; Lam, C.S.; Liu, Y.M.; Michaud, L.; Mulder, J.; Orr, J.B.; Rose, K.A.; et al. IMI—Clinical Management Guidelines Report. Investig. Ophthalmol. Vis. Sci. 2019, 60, M184–M203. [Google Scholar] [CrossRef]
- Bullimore, M.A.; Richdale, K. Myopia Control 2020: Where are we and where are we heading? Ophthalmic Physiol. Opt. 2020, 40, 254–270. [Google Scholar] [CrossRef]
- Muralidharan, A.R.; Lança, C.; Biswas, S.; Barathi, V.A.; Wan Yu Shermaine, L.; Seang-Mei, S.; Milea, D.; Najjar, R.P. Light and myopia: From epidemiological studies to neurobiological mechanisms. Ther. Adv. Ophthalmol. 2021, 13, 25158414211059246. [Google Scholar] [CrossRef] [PubMed]
- Jothi Balaji, J.; Viswanathan, S. Practice patterns in managing myopia differs among Indian eye care practitioners. Indian J. Ophthalmol. 2022, 70, 1848–1849. [Google Scholar] [CrossRef] [PubMed]
- Nti, A.N.; Owusu-Afriyie, B.; Osuagwu, U.L.; Kyei, S.; Ovenseri-Ogbomo, G.; Ogbuehi, K.C.; Ouzzani, M.; Agho, K.E.; Mashige, K.P.; Ekure, E.; et al. Trends in myopia management attitudes and strategies in clinical practice: Survey of eye care practitioners in Africa. Contact Lens Anterior Eye J. Br. Contact Lens Assoc. 2023, 46, 101597. [Google Scholar] [CrossRef] [PubMed]
- Douglass, A.; Keller, P.R.; He, M.; Downie, L.E. Knowledge, perspectives and clinical practices of Australian optometrists in relation to childhood myopia. Clin. Exp. Optom. 2020, 103, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Di Pierdomenico, J.; González-González, R.; Valiente-Soriano, F.J.; Galindo-Romero, C.; García-Ayuso, D. Attitudes and knowledge of myopia management by Spanish optometrists. Int. Ophthalmol. 2023, 43, 4247–4261. [Google Scholar] [CrossRef] [PubMed]
- Chaurasiya, R.K.; Sutar, S.; Gupta, A.; Pandey, R.; Agarwal, P. Knowledge, attitude, and practice of childhood myopia among Indian optometrists: A questionnaire-based study. Indian J. Ophthalmol. 2023, 71, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Thite, N.; Jaggernath, J.; Chinanayi, F.; Bharadwaj, S.; Kunjeer, G. Pattern of Optometry Practice and Range of Services in India. Optom. Vis. Sci. 2015, 92, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Kotrlik, J.; Higgins, C. Organizational research: Determining appropriate sample size in survey research appropriate sample size in survey research. Inf. Technol. Learn. Perform. J. 2001, 19, 43. [Google Scholar]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- India Vision Institute. Optometry in India. An Overview of Optometry Services in India in Terms of Optical Outlets, Eye Hospitals and Educational Institutes. 2016. Available online: https://www.indiavisioninstitute.org/resources-files/1730Optometry%20in%20India%20report_February%202016.pdf (accessed on 1 October 2023).
- Jong, M.; Sankaridurg, P.; Li, W.; Resnikoff, S.; Naidoo, K.; He, M. Reduced vision in highly myopic eyes without ocular pathology: The ZOC-BHVI high myopia study. Clin. Exp. Optom. 2018, 101, 77–83. [Google Scholar] [CrossRef]
- Fryer, L.K.; Shum, A.; Lee, A.; Lau, P. Mapping students’ interest in a new domain: Connecting prior knowledge, interest, and self-efficacy with interesting tasks and a lasting desire to reengage. Learn. Instr. 2021, 75, 101493. [Google Scholar] [CrossRef]
- Morgan, I.G.; Wu, P.C.; Ostrin, L.A.; Tideman, J.W.L.; Yam, J.C.; Lan, W.; Baraas, R.C.; He, X.; Sankaridurg, P.; Saw, S.M.; et al. IMI Risk Factors for Myopia. Investig. Ophthalmol. Vis. Sci. 2021, 62, 3. [Google Scholar] [CrossRef]
- Luong, T.Q.; Shu, Y.H.; Modjtahedi, B.S.; Fong, D.S.; Choudry, N.; Tanaka, Y.; Nau, C.L. Racial and Ethnic Differences in Myopia Progression in a Large, Diverse Cohort of Pediatric Patients. Investig. Ophthalmol. Vis. Sci. 2020, 61, 20. [Google Scholar] [CrossRef]
- Mutti, D.O.; Mitchell, G.L.; Moeschberger, M.L.; Jones, L.A.; Zadnik, K. Parental myopia, near work, school achievement, and children’s refractive error. Investig. Ophthalmol. Vis. Sci. 2002, 43, 3633–3640. [Google Scholar]
- He, X.; Sankaridurg, P.; Wang, J.; Chen, J.; Naduvilath, T.; He, M.; Zhu, Z.; Li, W.; Morgan, I.G.; Xiong, S.; et al. Time Outdoors in Reducing Myopia: A School-Based Cluster Randomized Trial with Objective Monitoring of Outdoor Time and Light Intensity. Ophthalmology 2022, 129, 1245–1254. [Google Scholar] [CrossRef]
- Martínez-Pérez, C.; Villa-Collar, C.; Santodomingo-Rubido, J.; Wolffsohn, J.S. Strategies and attitudes on the management of myopia in clinical practice in Spain. J. Optom. 2023, 16, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Wolffsohn, J.S.; Kollbaum, P.S.; Berntsen, D.A.; Atchison, D.A.; Benavente, A.; Bradley, A.; Buckhurst, H.; Collins, M.; Fujikado, T.; Hiraoka, T.; et al. IMI—Clinical Myopia Control Trials and Instrumentation Report. Investig. Ophthalmol. Vis. Sci. 2019, 60, M132–M160. [Google Scholar] [CrossRef] [PubMed]
- Jonas, J.B.; Ohno-Matsui, K.; Holbach, L.; Panda-Jonas, S. Retinal pigment epithelium cell density in relationship to axial length in human eyes. Acta Ophthalmol. 2017, 95, e22–e28. [Google Scholar] [CrossRef]
- Alanazi, M.K.; Almutleb, E.S.; Badawood, Y.S.; Kudam, M.A.; Liu, M. Perspectives and clinical practices of optometrists in Saudi Arabia concerning myopia in children. Int. J. Ophthalmol. 2023, 16, 267–273. [Google Scholar] [CrossRef]
- Wan Omar, W.E.; Cruickshank, F.; Radhakrishnan, H. UK Optometrists’ Professional Learning Needs Toward Engaging with Myopia Control Interventions. Br. Ir. Orthopt. J. 2024, 20, 69–84. [Google Scholar] [CrossRef]
- Yang, A.; Pang, B.Y.; Vasudevan, P.; Drobe, B. Eye Care Practitioners Are Key Influencer for the Use of Myopia Control Intervention. Front. Public Health 2022, 10, 854654. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.; Mohidin, N.; O’Leary, D.J. Undercorrection of myopia enhances rather than inhibits myopia progression. Vis. Res. 2002, 42, 2555–2559. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.-R.; Wang, J.-H.; Huang, H.-K.; Chen, T.-L.; Chen, P.-W.; Chiu, C.-J. Efficacy of atropine, orthokeratology, and combined atropine with orthokeratology for childhood myopia: A systematic review and network meta-analysis. J. Formos. Med. Assoc. 2022, 121, 2490–2500. [Google Scholar] [CrossRef]
- Karthikeyan, S.K.; Ashwini, D.L.; Priyanka, M.; Nayak, A.; Biswas, S. Physical activity, time spent outdoors, and near work in relation to myopia prevalence, incidence, and progression: An overview of systematic reviews and meta-analyses. Indian J. Ophthalmol. 2022, 70, 728–739. [Google Scholar] [CrossRef] [PubMed]
- Tsugawa, Y.; Newhouse, J.P.; Zaslavsky, A.M.; Blumenthal, D.M.; Jena, A.B. Physician age and outcomes in elderly patients in hospital in the US: Observational study. BMJ (Clin. Res. Ed.) 2017, 357, j1797. [Google Scholar] [CrossRef] [PubMed]
- Berntsen, D.A.; Sinnott, L.T.; Mutti, D.O.; Zadnik, K. A randomized trial using progressive addition lenses to evaluate theories of myopia progression in children with a high lag of accommodation. Investig. Ophthalmol. Vis. Sci. 2012, 53, 640–649. [Google Scholar] [CrossRef] [PubMed]
- Bullimore, M.A.; Lee, S.S.; Schmid, K.L.; Rozema, J.J.; Leveziel, N.; Mallen, E.A.H.; Jacobsen, N.; Iribarren, R.; Verkicharla, P.K.; Polling, J.R.; et al. IMI-Onset and Progression of Myopia in Young Adults. Investig. Ophthalmol. Vis. Sci. 2023, 64, 2. [Google Scholar] [CrossRef] [PubMed]
- Heiwe, S.; Kajermo, K.N.; Tyni-Lenné, R.; Guidetti, S.; Samuelsson, M.; Andersson, I.L.; Wengström, Y. Evidence-based practice: Attitudes, knowledge and behaviour among allied health care professionals. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 2011, 23, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Brennan, N.A.; Toubouti, Y.M.; Cheng, X.; Bullimore, M.A. Efficacy in myopia control. Prog. Retin. Eye Res. 2021, 83, 100923. [Google Scholar] [CrossRef]
- Downie, L.E.; Keller, P.R.; Vingrys, A.J. An evidence-based analysis of Australian optometrists’ dry eye practices. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2013, 90, 1385–1395. [Google Scholar] [CrossRef]
- Downie, L.E.; Keller, P.R. The self-reported clinical practice behaviors of Australian optometrists as related to smoking, diet and nutritional supplementation. PLoS ONE 2015, 10, e0124533. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.; Logan, N.S.; Davies, L.N.; Sheppard, A.L.; Wolffsohn, J.S. Assessing the utility of ChatGPT as an artificial intelligence-based large language model for information to answer questions on myopia. Ophthalmic Physiol. Opt. 2023, 43, 1562–1570. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.; Davies, L.N.; Sheppard, A.L.; Logan, N.S.; Wolffsohn, J.S. Utility of artificial intelligence-based large language models in ophthalmic care. Ophthalmic Physiol. Opt. 2024, 44, 641–671. [Google Scholar] [CrossRef] [PubMed]
- Glasman, L.R.; Albarracín, D. Forming attitudes that predict future behavior: A meta-analysis of the attitude-behavior relation. Psychol. Bull. 2006, 132, 778–822. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Guo, L.; Zhang, J.; Zhao, F.; Hu, Y.; Guo, Y.; Du, X.; Zhang, S.; Yang, X.; Lu, C. Effect of School-Based Family Health Education via Social Media on Children’s Myopia and Parents’ Awareness: A Randomized Clinical Trial. JAMA Ophthalmol. 2021, 139, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Wen, L.M.; Rissel, C. Associations of parental influences with physical activity and screen time among young children: A systematic review. J. Obes. 2015, 2015, 546925. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, K.S.; Govender-Poonsamy, P.; Morjaria, P.; Block, S.; Chan, V.F.; Yong, A.C.; Bilotto, L. Global mapping of optometry workforce. Afr. Vis. Eye Health 2023, 82, 850. [Google Scholar] [CrossRef]
- McCrann, S.; Flitcroft, I.; Loughman, J. Is optometry ready for myopia control? Education and other barriers to the treatment of myopia. HRB Open Res. 2019, 2, 30. [Google Scholar] [CrossRef]
- Main, P.A.E.; Anderson, S. Evidence for continuing professional development standards for regulated health practitioners in Australia: A systematic review. Hum. Resour. Health 2023, 21, 23. [Google Scholar] [CrossRef]
- Karas, M.; Sheen, N.J.L.; North, R.V.; Ryan, B.; Bullock, A. Continuing professional development requirements for UK health professionals: A scoping review. BMJ Open 2020, 10, e032781. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S.no | Description | Survey Report |
|---|---|---|
| 1 | Survey development | A prevalidated questionnaire was revised after a focus group discussion among four optometrists to finalize the questionnaire’s items. |
| 2 | Number and nature of items in the questionnaire | A 26-item questionnaire with a mix of open- and closed-ended questions. |
| 3 | Reliability | Not determined. |
| 4 | Mode of survey | Internet-based. |
| 5 | Survey period | 27 March 2020 to 27 September 2022. |
| 6 | Sample frame | Open survey: Open for all optometrists across India. |
| 7 | Target population | Optometrists practicing in India. |
| 8 | Recruitment process | Open invitations over social media, namely, Facebook, WhatsApp, E-Newsletter, and Telegram, in a target group with reminder messages every 2 weeks. |
| 9 | Participation | Voluntary participation. |
| 10 | Survey administration | Sequential questions administered using Google Forms. |
| 11 | Informed consent | E-consent. |
| 12 | Incentives | None. |
| 13 | Randomization of items or questionnaires | No randomization of items or questions. |
| 14 | Use of adoptive questions | Yes. |
| 15 | Number of screens | 5. |
| 16 | Review step | Review with a back button, no alteration was possible after submission. |
| 17 | Preventing multiple entries from a single respondent, e.g., cookies used | Limited to one response per email and one item in the questions asked for their previous participation in the survey. |
| 18 | Data capturing | Automatic conversion into a spreadsheet. |
| 19 | Data analysis | Proportions of each response were calculated, and the odds were determined (p value of <0.05 was considered statistically significant). |
| 20 | Software used for statistical analysis | GraphPad Prism (version 6.04 for Windows, GraphPad Software, La Jolla, CA, USA and IBM SPSS Statistics for Windows, Version 28.0, IBM Corp. |
| Characteristic | Respondents (n = 393) | p-Value * |
|---|---|---|
| Sex (male/female): n (%) | 194/199 (49.4%/50.6%) | - |
| Optometric practice experience: n (%) | ||
| 0–5 years | 200 (50.9%) | <0.001 |
| 5–10 years | 62 (15.8%) | |
| 10–15 years | 40 (10.2%) | |
| 15–20 years | 44 (11.2%) | |
| >20 years | 47 (12.0%) | |
| Primary place of optometric practice: n (%) | ||
| Hospital | 159 (40.4%) | <0.001 |
| Academic Institution | 63 (16.0%) | |
| Independent (private) practice | 82 (20.9%) | |
| Corporate practice | 52 (13.2%) | |
| Optometrist pursuing post-graduation | 37 (9.5%) | |
| Possess a clinical or research interest in managing childhood myopia (yes/no): n (%) | 352/41 (89.6%/10.4%) | |
| Number of myopic patients under 16 years of age provided care to in a typical week: n (%) | ||
| 158 (40.2%) 114 (29.0%) 46 (11.7%) 16 (4.1%) 18 (4.6%) 9 (2.3%) 32 (8.1%) | <0.001 |
| Ocular Conditions | Percentage of Respondents (%) |
|---|---|
| Retinal breaks | 67.4 |
| Rhegmatogenous retinal detachment | 45.3 |
| Cataract | 44.8 |
| Exudative retinal detachment | 30.8 |
| Primary open angle glaucoma | 29.7 |
| Primary angle closure glaucoma | 18.6 |
| Age-related macular degeneration | 16.9 |
| Diabetic retinopathy | 7.6 |
| Clinical Procedures | Percentage of Respondents (%) |
|---|---|
| Cycloplegic retinoscopy | 86.6 |
| Note patient family history of myopia | 83.7 |
| Dilated retinal fundus examination | 76.7 |
| Cover test (distance and near phoria) | 75.0 |
| Cycloplegic subjective refraction | 70.9 |
| Noncycloplegic retinoscopy | 62.8 |
| Noncycloplegic subjective refraction | 62.2 |
| Cycloplegic autorefraction | 52.3 |
| Intraocular pressure | 47.1 |
| Axial length measurement | 46.5 |
| Dynamic retinoscopy (e.g., MEM, NOTT retinoscopy) | 39.5 |
| AC/A ratio | 35.5 |
| Noncycloplegic autorefraction and stereopsis | 34.3 |
| Measurement of pupil size | 32.6 |
| Corneal topography | 21.5 |
| Retinal fundus photography—posterior pole | 14.5 |
| Retinal fundus photography—periphery | 11.6 |
| Peripheral defocus | 8.7 |
| Others | 11.2 |
| Myopia Management Option | Percentage of Respondents (%) |
|---|---|
| Advice to increase time spent outdoors | 73.8 |
| Low- to moderate-dose (0.01–0.5%) atropine eye drops | 68.6 |
| Visual hygiene (e.g., taking regular breaks with prolonged near work | |
| Maintaining appropriate working distance and good lighting | 66.3 |
| Orthokeratology | 52.9 |
| Single-vision distance spectacles (undercorrection) | 36.6 |
| Progressive addition spectacle lenses (multifocal) | 27.9 |
| Peripheral defocus soft contact lenses (e.g., distance-center multifocal soft contact lenses) | 26.7 |
| Bifocal spectacle lenses | 20.3 |
| Cyclopentolate 1% eye drops | 11.6 |
| Bifocal spectacle lenses with prism | 9.3 |
| High-dose (>0.5%) atropine eye drops | 5.8 |
| Others | 4.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naik, A.; Karthikeyan, S.K.; Ramesh, J.J.; Bhaskar, S.; Ganapathi, C.A.; Biswas, S. An Insight into Knowledge, Perspective, and Practices of Indian Optometrists towards Childhood Myopia. Vision 2024, 8, 22. https://doi.org/10.3390/vision8020022
Naik A, Karthikeyan SK, Ramesh JJ, Bhaskar S, Ganapathi CA, Biswas S. An Insight into Knowledge, Perspective, and Practices of Indian Optometrists towards Childhood Myopia. Vision. 2024; 8(2):22. https://doi.org/10.3390/vision8020022
Chicago/Turabian StyleNaik, Archana, Siddharth K. Karthikeyan, Jivitha Jyothi Ramesh, Shwetha Bhaskar, Chinnappa A. Ganapathi, and Sayantan Biswas. 2024. "An Insight into Knowledge, Perspective, and Practices of Indian Optometrists towards Childhood Myopia" Vision 8, no. 2: 22. https://doi.org/10.3390/vision8020022
APA StyleNaik, A., Karthikeyan, S. K., Ramesh, J. J., Bhaskar, S., Ganapathi, C. A., & Biswas, S. (2024). An Insight into Knowledge, Perspective, and Practices of Indian Optometrists towards Childhood Myopia. Vision, 8(2), 22. https://doi.org/10.3390/vision8020022