
Cardiac Magnetic Resonance Imaging in Immune Check-Point Inhibitor Myocarditis: A Systematic Review

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
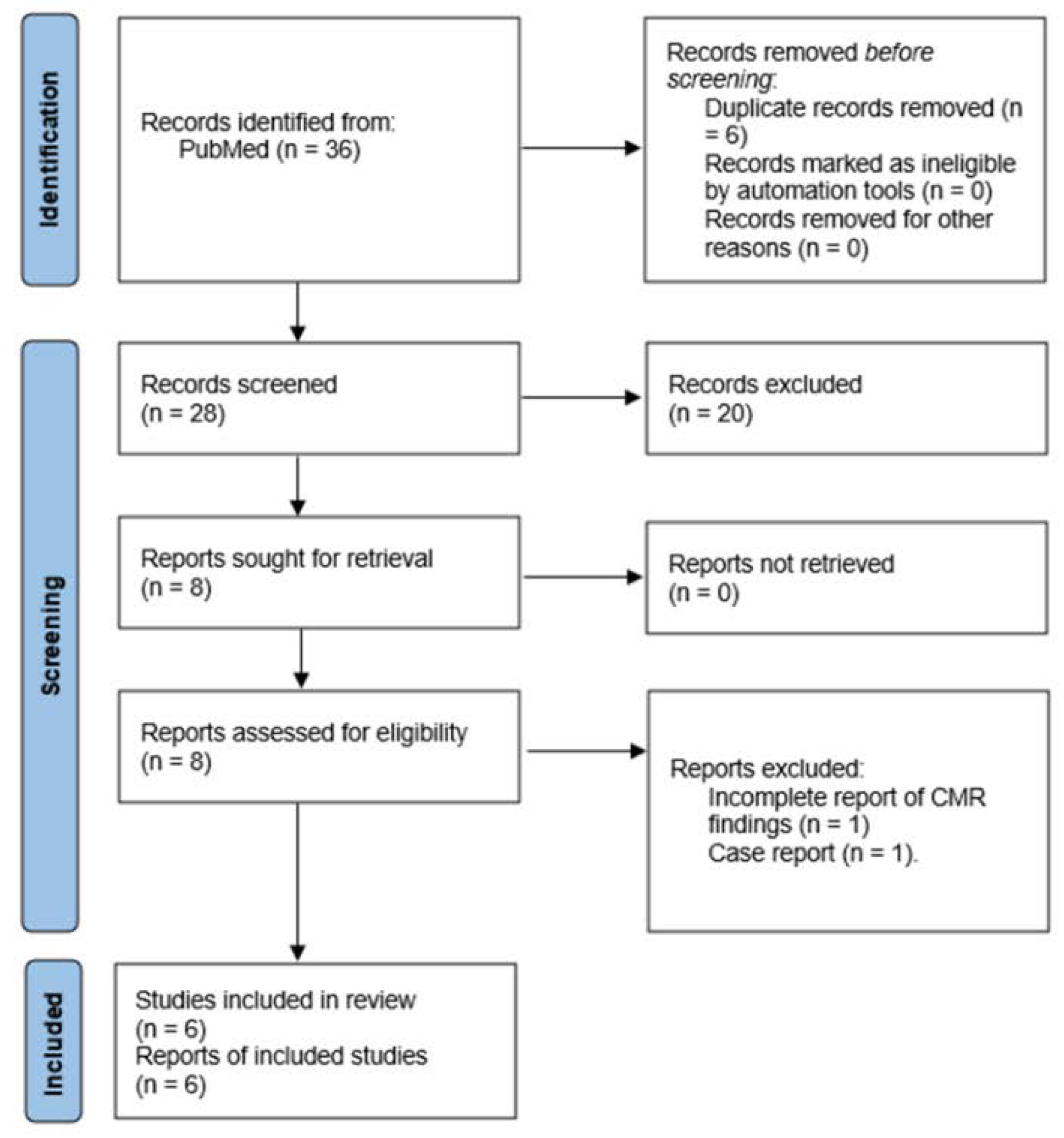
2. Materials and Methods
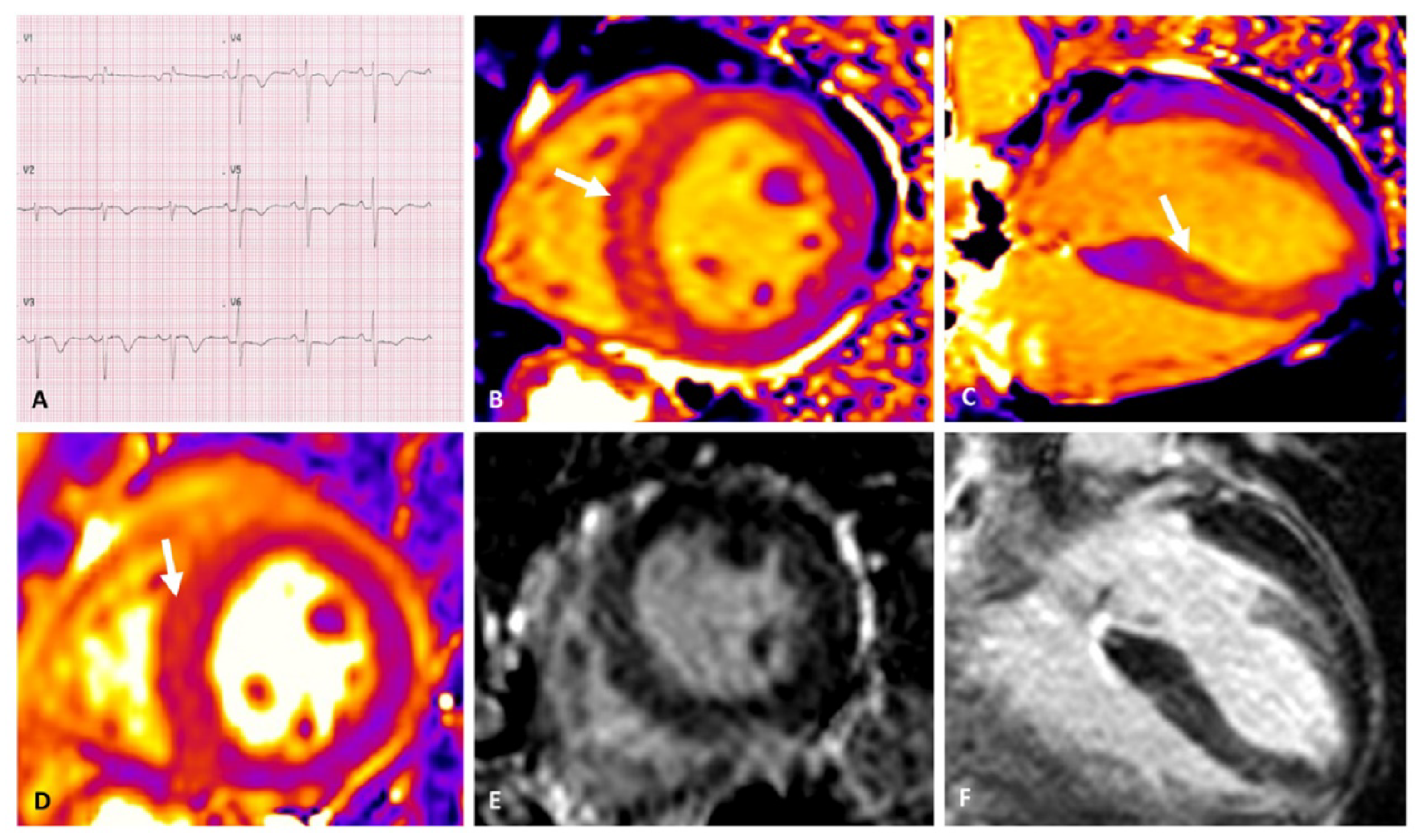
3. Cardiac Magnetic Resonance Findings
3.1. Left Ventricular Function
3.2. Edema
3.3. Fibrosis
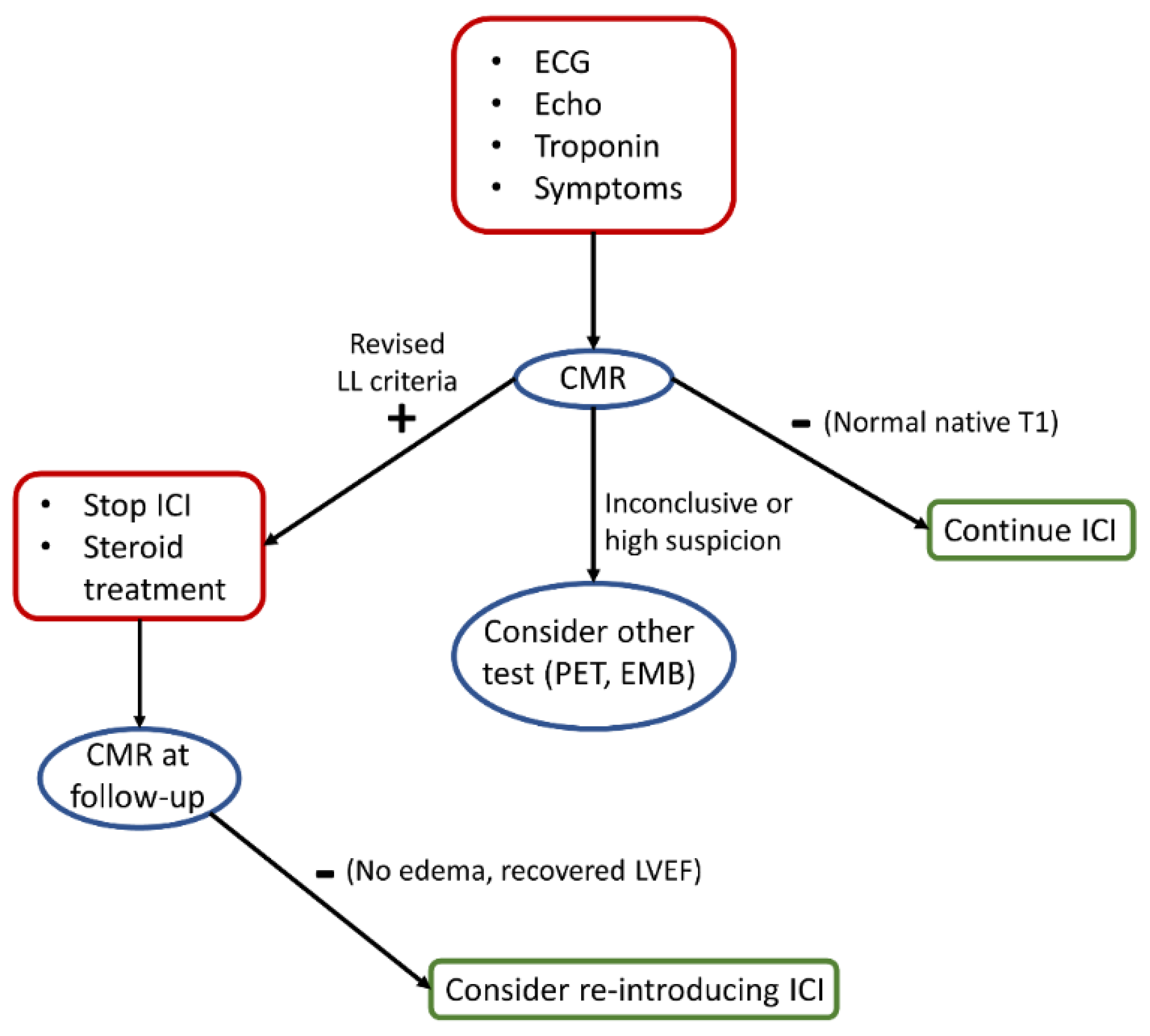
4. Clinical Implications
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wolchok, J.D. Bench to Bedside PD-1 Blockers. Cell 2015, 162, 937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Postow, M.A.; Callahan, M.K.; Wolchok, J.D. Immune Checkpoint Blockade in Cancer Therapy. J. Clin. Oncol. 2015, 33, 1974–1982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spallarossa, P.; Meliota, G.; Brunelli, C.; Arboscello, E.; Ameri, P.; Dessalvi, C.C.; Grossi, F.; Deidda, M.; Mele, D.; Sarocchi, M.; et al. Potential cardiac risk of immune-checkpoint blockade as anticancer treatment: What we know, what we do not know, and what we can do to prevent adverse effects. Med. Res. Rev. 2018, 38, 1447–1468. [Google Scholar] [CrossRef] [PubMed]
- Spallarossa, P.; Sarocchi, M.; Tini, G.; Arboscello, E.; Toma, M.; Ameri, P.; Porto, I. How to Monitor Cardiac Complications of Immune Checkpoint Inhibitor Therapy. Front. Pharmacol. 2020, 11, 972. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.R.; Florido, R.; Lipson, E.J.; Naidoo, J.; Ardehali, R.; Tocchetti, C.G.; Lyon, A.R.; Padera, R.F.; Johnson, D.B.; Moslehi, J. Cardiovascular toxicities associated with immune checkpoint inhibitors. Cardiovasc. Res. 2019, 115, 854–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salem, J.E.; Manouchehri, A.; Moey, M.; Lebrun-Vignes, B.; Bastarache, L.; Pariente, A.; Gobert, A.; Spano, J.-P.; Balko, J.M.; Bonaca, M.P.; et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: An observational, retrospective, pharmacovigilance study. Lancet Oncol. 2018, 19, 1579–1589. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef]
- Winau, L.; Hinojar Baydes, R.; Braner, A.; Drott, U.; Burkhardt, H.; Sangle, S.; D’Cruz, D.P.; Carr-White, G.; Marber, M.; Schnoes, K.; et al. High-sensitive troponin is associated with subclinical imaging biosignature of inflammatory cardiovascular involvement in systemic lupus erythematosus. Ann. Rheum. Dis. 2018, 77, 1590–1598. [Google Scholar] [CrossRef]
- de Leuw, P.; Arendt, C.T.; Haberl, A.E.; Froadinadl, D.; Kann, G.; Wolf, T.; Stephan, C.; Schuettfort, G.; Vasquez, M.; Arcari, L.; et al. Myocardial Fibrosis and Inflammation by CMR Predict Cardiovascular Outcome in People Living With HIV. JACC Cardiovasc. Imaging 2021, 14, 1548–1557. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Escudier, M.; Cautela, J.; Malissen, N.; Ancedy, Y.; Orabona, M.; Pinto, J.; Monestier, S.; Grob, J.-J.; Scemama, U.; Jacquier, A.; et al. Clinical features, management, and outcomes of immune checkpoint inhibitor-related cardiotoxicity. Circulation 2017, 136, 2085–2087. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.W.; Alexander, M.; Dib, Y.; Lau, P.K.H.; Weppler, A.M.; Au-Yeung, G.; Lee, B.; Khoo, C.; Mooney, D.; Joshi, S.B.; et al. A closer look at immune-mediated myocarditis in the era of combined checkpoint blockade and targeted therapies. Eur. J. Cancer 2020, 124, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, A.Y.; Arbune, A.; Soufer, A.; Ragheb, E.; Kwan, J.M.; Lamy, J.; Henry, M.; Cuomo, J.R.; Charifa, A.; Gallegos, C.; et al. Left ventricular myocardial strain and tissue characterization by cardiac magnetic resonance imaging in immune checkpoint inhibitor associated cardiotoxicity. PLoS ONE 2021, 16, e0246764. [Google Scholar] [CrossRef]
- Zhang, L.; Awadalla, M.; Mahmood, S.S.; Nohria, A.; Hassan, M.Z.O.; Thuny, F.; Zlotoff, D.A.; Murphy, S.P.; Stone, J.R.; Golden, D.L.A.; et al. Cardiovascular magnetic resonance in immune checkpoint inhibitor-associated myocarditis. Eur. Heart J. 2020, 41, 1733–1743. [Google Scholar] [CrossRef] [PubMed]
- Thavendiranathan, P.; Zhang, L.; Zafar, A.; Drobni, Z.D.; Mahmood, S.S.; Cabral, M.; Awadalla, M.; Nohria, A.; Zlotoff, D.A.; Thuny, F.; et al. Myocardial T1 and T2 Mapping by Magnetic Resonance in Patients With Immune Checkpoint Inhibitor–Associated Myocarditis. J. Am. Coll. Cardiol. 2021, 77, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- Faron, A.; Isaak, A.; Mesropyan, N.; Reinert, M.; Schwab, K.; Sirokay, J.; Sprinkart, A.M.; Bauernfeind, F.-G.; Dabir, D.; Pieper, C.C.; et al. Cardiac mri depicts immune checkpoint inhibitor-induced myocarditis: A prospective study. Radiology 2021, 301, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Camastra, G.; Arcari, L.; Ciolina, F.; Danti, M.; Cacciotti, L. Cardiac magnetic resonance imaging of transient myocardial dysfunction in a patient treated with checkpoint-targeted immunotherapy. Eur. J. Cancer 2020, 144, 389–391. [Google Scholar] [CrossRef]
- Palaskas, N.L.; Segura, A.; Lelenwa, L.; Siddiqui, B.A.; Subudhi, S.K.; Lopez-Mattei, J.; Durand, J.B.; Deswal, A.; Zhao, B.; Buja, L.M.; et al. Immune checkpoint inhibitor myocarditis: Elucidating the spectrum of disease through endomyocardial biopsy. Eur. J. Heart Fail. 2021, 23, 1725–1735. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Jiménez, R.; Sánchez-González, J.; Aguero, J.; Del Trigo, M.; Galán-Arriola, C.; Fuster, V.; Ibáñez, B. Fast T2 gradient-spin-echo (T2-GraSE) mapping for myocardial edema quantification: First in vivo validation in a porcine model of ischemia/reperfusion. J. Cardiovasc. Magn. Reson. 2015, 17, 1–9. [Google Scholar] [CrossRef] [Green Version]
- McAlindon, E.J.; Pufulete, M.; Harris, J.M.; Lawton, C.B.; Moon, J.C.; Manghat, N.; Hamilton, M.C.K.; Weale, P.; Bucciarelli-Ducci, C. Measurement of Myocardium at Risk with Cardiovascular MR: Comparison of Techniques for Edema Imaging. Radiology 2015, 275, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Arcari, L.; Bucciarelli-Ducci, C.; Francone, M.; Agati, L. Myocardial Salvage Imaging: Where Are We and Where Are We Heading? A Cardiac Magnetic Resonance Perspective. Curr. Cardiovasc. Imaging Rep. 2018, 11, 8. [Google Scholar] [CrossRef] [Green Version]
- Puntmann, V.O.; Peker, E.; Chandrashekhar, Y.; Nagel, E. T1 Mapping in Characterizing Myocardial Disease. Circ. Res. 2016, 119, 277–299. [Google Scholar] [CrossRef] [PubMed]
- Arcari, L.; Engel, J.; Freiwald, T.; Zhou, H.; Zainal, H.; Gawor, M.; Buettner, S.; Geiger, H.; Hauser, I.; Nagel, E.; et al. Cardiac biomarkers in chronic kidney disease are independently associated with myocardial edema and diffuse fibrosis by cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2021, 23, 71. [Google Scholar] [CrossRef] [PubMed]
- Aquaro, G.D.; Perfetti, M.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C.; Pepe, A.; Todiere, G.; Lanzillo, C.; Scatteia, A.; et al. Cardiac MR With Late Gadolinium Enhancement in Acute Myocarditis With Preserved Systolic Function: ITAMY Study. J. Am. Coll. Cardiol. 2017, 70, 1977–1987. [Google Scholar] [CrossRef] [PubMed]
- Hinojar, R.; Foote, L.; Ucar, E.A.; Jackson, T.; Jabbour, A.; Yu, C.Y.; McCrohon, J.; Higgins, D.; Carr-White, G.; Mayr, M.; et al. Native T1 in discrimination of acute and convalescent stages in patients with clinical diagnosis of myocarditis: A proposed diagnostic algorithm using CMR. JACC Cardiovasc. Imaging 2015, 8, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Puntmann, V.O.; Isted, A.; Hinojar, R.; Foote, L.; Carr-White, G.; Nagel, E. T1 and T2 mapping in recognition of early cardiac involvement in systemic sarcoidosis. Radiology 2017, 285, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Kim, R.J.; Wu, E.; Rafael, A.; Chen, E.L.; Parker, M.A.; Simonetti, O.; Klocke, F.J.; Bonow, R.O.; Judd, R.M. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N. Engl. J. Med. 2000, 343, 1445–1453. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Ghebru Habtemicael, Y.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C. Prognostic Value of Repeating Cardiac Magnetic Resonance in Patients With Acute Myocarditis. J. Am. Coll. Cardiol. 2019, 74, 2439–2448. [Google Scholar] [CrossRef]
- Nakamori, S.; Dohi, K.; Ishida, M.; Goto, Y.; Imanaka-Yoshida, K.; Omori, T.; Goto, I.; Kumagai, N.; Fujimoto, N.; Ichikawa, Y.; et al. Native T1 Mapping and Extracellular Volume Mapping for the Assessment of Diffuse Myocardial Fibrosis in Dilated Cardiomyopathy. JACC Cardiovasc. Imaging 2018, 11, 48–59. [Google Scholar] [CrossRef]
- Child, N.; Suna, G.; Dabir, D.; Yap, M.-L.; Rogers, T.; Kathirgamanathan, M.; Arroyo-Ucar, E.; Hinojar, R.; Mahmoud, I.; Young, C.; et al. Comparison of MOLLI, shMOLLLI, and SASHA in discrimination between health and disease and relationship with histologically derived collagen volume fraction. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 768–776. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.; Piechnik, S.K.; Dall’Armellina, E.; Karamitsos, T.D.; Francis, J.M.; Choudhury, R.P.; Friedrich, M.G.; Robson, M.D.; Neubauer, S. Non-contrast T1-mapping detects acute myocardial edema with high diagnostic accuracy: A comparison to T2-weighted cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2012, 14, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arcari, L.; Hinojar, R.; Engel, J.; Freiwald, T.; Platschek, S.; Zainal, H.; Zhou, H.; Vasquez, M.; Keller, T.; Rolf, A.; et al. Native T1 and T2 provide distinctive signatures in hypertrophic cardiac conditions–Comparison of uremic, hypertensive and hypertrophic cardiomyopathy. Int. J. Cardiol. 2020, 306, 102–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thavendiranathan, P.; Zhang, L.; Neilan, T.G. Reply: Imaging Edema in Immune Checkpoint Inhibitor Myocarditis: A Moving Target. J. Am. Coll. Cardiol. 2021, 78, 417–418. [Google Scholar] [CrossRef]
- Arcari, L.; Camastra, G.; Ciolina, F.; Danti, M.; Cacciotti, L. Imaging Edema in Immune Checkpoint Inhibitor Myocarditis: A Moving Target. J. Am. Coll. Cardiol. 2021, 78, 416–417. [Google Scholar] [CrossRef]
- Puzanov, I.; Diab, A.; Abdallah, K.; Bingham, C.O.; Brogdon, C.; Dadu, R.; Hamad, L.; Kim, S.; Lacouture, M.E.; LeBoeuf, N.R.; et al. Managing toxicities associated with immune checkpoint inhibitors: Consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J. Immunother. Cancer 2017, 5, 95. [Google Scholar] [CrossRef] [Green Version]
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; Ernstoff, M.S.; Gardner, J.M.; Ginex, P.; et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American society of clinical oncology clinical practice guideline. J. Clin. Oncol. 2018, 36, 1714–1768. [Google Scholar] [CrossRef]
- Johnson, D.B.; Balko, J.M.; Compton, M.L.; Chalkias, S.; Gorham, J.; Xu, Y.; Hicks, M.; Puzanov, I.; Alexander, M.R.; Bloomer, T.L.; et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N. Engl. J. Med. 2016, 375, 1749–1755. [Google Scholar] [CrossRef]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in Patients Treated With Immune Checkpoint Inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. [Google Scholar] [CrossRef]
- Moslehi, J.J.; Salem, J.E.; Sosman, J.A.; Lebrun-Vignes, B.; Johnson, D.B. Increased reporting of fatal immune checkpoint inhibitor-associated myocarditis. Lancet 2018, 391, 933. [Google Scholar] [CrossRef] [Green Version]
- PCaforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef] [PubMed]
- Spallarossa, P.; Tini, G.; Sarocchi, M.; Arboscello, E.; Grossi, F.; Queirolo, P.; Zoppoli, G.; Ameri, P. Identification and Management of Immune Checkpoint Inhibitor-Related Myocarditis: Use Troponin Wisely. J. Clin. Oncol. 2019, 37, 2201–2205. [Google Scholar] [CrossRef] [Green Version]
- Januzzi, J.L.; Filippatos, G.; Nieminen, M.; Gheorghiade, M. Troponin elevation in patients with heart failure: On behalf of the third Universal Definition of Myocardial Infarction Global Task Force: Heart Failure Section. Eur. Heart J. 2012, 33, 2265–2271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turan, A.; Cohen, B.; Rivas, E.; Liu, L.; Pu, X.; Maheshwari, K.; Farag, E.; Onal, O.; Wang, J.; Ruetzler, K.; et al. Association between postoperative haemoglobin and myocardial injury after noncardiac surgery: A retrospective cohort analysis. Br. J. Anaesth. 2021, 126, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Arcari, L.; Luciani, M.; Cacciotti, L.; Pucci, M.; Musumeci, M.B.; Pietropaolo, L.; Spuntarelli, V.; Negro, A.; Camastra, G.; Bentivegna, E.; et al. Coronavirus disease 2019 in patients with cardiovascular disease: Clinical features and implications on cardiac biomarkers assessment. J. Cardiovasc. Med. 2021, 22, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Sarocchi, M.; Grossi, F.; Arboscello, E.; Bellodi, A.; Genova, C.; Dal Bello, M.G.; Rijavec, E.; Barletta, G.; Biello, F.; Ghigliotti, G.; et al. Serial Troponin for Early Detection of Nivolumab Cardiotoxicity in Advanced Non-Small Cell Lung Cancer Patients. Oncologist 2018, 23, 936–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palaskas, N.; Lopez-Mattei, J.; Durand, J.B.; Iliescu, C.; Deswal, A. Immune Checkpoint Inhibitor Myocarditis: Pathophysiological Characteristics, Diagnosis, and Treatment. J. Am. Heart Assoc. 2020, 9, e013757. [Google Scholar] [CrossRef]
- Schneider, B.J.; Naidoo, J.; Santomasso, B.D.; Lacchetti, C.; Adkins, S.; Anadkat, M.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; et al. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: ASCO Guideline Update. J. Clin. Oncol. 2021, 39, 4073–4126. [Google Scholar] [CrossRef]
- Power, J.R.; Alexandre, J.; Choudhary, A.; Ozbay, B.; Hayek, S.; Asnani, A.; Tamura, Y.; Aras, M.; Cautela, J.; Thuny, F.; et al. Electrocardiographic Manifestations of Immune Checkpoint Inhibitor Myocarditis. Circulation 2021, 144, 1521–1523. [Google Scholar] [CrossRef]
- Ederhy, S.; Devos, P.; Pinna, B.; Funck-Brentano, E.; Abbar, B.; Fenioux, C.; Cohen, A.A.; Moslehi, J.; Bretagne, M.; Allenbach, Y.; et al. 18F-fluorodeoxyglucose positron emission tomography/computed tomography imaging for the diagnosis of immune checkpoint inhibitor-associated myocarditis. Arch. Cardiovasc. Dis. 2022, 115, 114–116. [Google Scholar] [CrossRef]
- Ederhy, S.; Fenioux, C.; Cholet, C.; Rouvier, P.; Redheuil, A.; Cohen, A.; Salem, J.-E. Immune Checkpoint Inhibitor Myocarditis With Normal Cardiac Magnetic Resonance Imaging: Importance of Cardiac Biopsy and Early Diagnosis. Can. J. Cardiol. 2021, 37, 1654–1656. [Google Scholar] [CrossRef] [PubMed]
- Ida, M.; Nakamori, S.; Ishida, M.; Dohi, K. Management of immune checkpoint inhibitor myocarditis: A serial cardiovascular magnetic resonance T2 mapping approach. Eur. Heart J. 2021, 42, 2869. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Nakamori, S.; Watanabe, S.; Nishikawa, K.; Inoue, T.; Imanaka-Yoshida, K.; Ishida, M.; Sakuma, H.; Ito, M.; Dohi, K. Monitoring of the Evolution of Immune Checkpoint Inhibitor Myocarditis with Cardiovascular Magnetic Resonance. Circ. Cardiovasc. Imaging 2020, 13, 10633. [Google Scholar] [CrossRef] [PubMed]
- Haslbauer, J.D.; Lindner, S.; Valbuena-Lopez, S.; Zainal, H.; Zhou, H.; D’Angelo, T.; Pathan, F.; Arendt, C.A.; Bug, G.; Serve, H.; et al. CMR imaging biosignature of cardiac involvement due to cancer-related treatment by T1 and T2 mapping. Int. J. Cardiol. 2019, 275, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Peleg Hasson, S.; Salwen, B.; Sivan, A.; Shamai, S.; Geva, R.; Merimsky, O.; Raphael, A.; Shmilovich, H.; Moshkovits, Y.; Kapusta, L.; et al. Re-introducing immunotherapy in patients surviving immune checkpoint inhibitors-mediated myocarditis. Clin. Res. Cardiol. 2020, 110, 50–60. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Study (First Author) | Patients | LVEF (%) | Edema (%) | T1 and T2 Mapping | LGE (%) | Prognostic Assessment |
|---|---|---|---|---|---|---|
| Escudier et al. | n = 15 | 35 (15, 73) | 5/15 (33) | No | 3/13 (23) | No |
| Guo et al. | n = 6 | 55 (31, 60) | 3/6 (50) | No | 5/6 (83) | No |
| Higgins et al. | n = 20 | 53 (39, 60) | 12/20 (60) | T2 in n = 3 | 14 (70) | No |
| Zhang et al. | n = 103 | 49 ± 15 | 28/103 (27) | No | 49/103 (48) | Yes |
| Thavendiranathan et al. | n = 86 | 51 ± 14 | 42/79 (34) | T1 (n = 86), T2 (n = 79) | 48/86 (56) | Yes |
| Faron et al. | n = 22 | 59 ± 14 | 2 (9) | Yes | 9 (41) | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arcari, L.; Tini, G.; Camastra, G.; Ciolina, F.; De Santis, D.; Russo, D.; Caruso, D.; Danti, M.; Cacciotti, L. Cardiac Magnetic Resonance Imaging in Immune Check-Point Inhibitor Myocarditis: A Systematic Review. J. Imaging 2022, 8, 99. https://doi.org/10.3390/jimaging8040099
Arcari L, Tini G, Camastra G, Ciolina F, De Santis D, Russo D, Caruso D, Danti M, Cacciotti L. Cardiac Magnetic Resonance Imaging in Immune Check-Point Inhibitor Myocarditis: A Systematic Review. Journal of Imaging. 2022; 8(4):99. https://doi.org/10.3390/jimaging8040099
Chicago/Turabian StyleArcari, Luca, Giacomo Tini, Giovanni Camastra, Federica Ciolina, Domenico De Santis, Domitilla Russo, Damiano Caruso, Massimiliano Danti, and Luca Cacciotti. 2022. "Cardiac Magnetic Resonance Imaging in Immune Check-Point Inhibitor Myocarditis: A Systematic Review" Journal of Imaging 8, no. 4: 99. https://doi.org/10.3390/jimaging8040099
APA StyleArcari, L., Tini, G., Camastra, G., Ciolina, F., De Santis, D., Russo, D., Caruso, D., Danti, M., & Cacciotti, L. (2022). Cardiac Magnetic Resonance Imaging in Immune Check-Point Inhibitor Myocarditis: A Systematic Review. Journal of Imaging, 8(4), 99. https://doi.org/10.3390/jimaging8040099