Abstract
In keeping with the trend worldwide, in Portugal, more than 60% of newly diagnosed patients with cancer are aged 65 years or older, which makes older adults the most common population seen in an oncology practice. This study’s objectives were to assess geriatric oncology practices in Portugal and investigate medical professionals’ current needs and perceptions on the treatment of elderly cancer patients. Methods: A cross-sectional study was conducted using a web-based survey of healthcare providers treating elderly patients. Results: There were 222 responses: 62.6% of physicians reported the absence of geriatric oncology and/or geriatrics consultations in their institutions, 14.9% had guidelines for the management of older patients with cancer and 4.5% had physicians dedicated to geriatric oncology. The reported use of geriatric assessment tools was 23.4%. Medical oncologists and physicians from medical specialties (p = 0.009) and those practicing in the south of Portugal (p = 0.054) were more likely to use geriatric assessment. Education and training in geriatric oncology was identified by 95.0% of respondents as an unmet need. The inquiries identified that geriatric assessment could be useful to define a therapeutic strategy (85.1%), detect frailty (77.5%), predict toxicity and improve quality of life (73.4%). Conclusions: There is a paucity of expertise and training in geriatric oncology in Portugal but an increasing perception of the value of geriatric assessment and the demand for education. In the next years, Portugal will progress in this area with the aid of the recently created Geriatric Oncology Working Group.
1. Introduction
Aging is one of the strongest and most predictable risk factors for the development of cancer. The pool of patients over the age of 65 years being diagnosed with and surviving their cancer is rapidly expanding [1]. According to GLOBOCAN 2020, in Portugal, more than 60% of patients who are newly diagnosed with cancer are aged 65 years or older, which makes this the most common population seen in an oncology practice [1]. Older adults with cancer are heterogeneous and have wide variability in their health status and social support; therefore, they require a personalized approach to cancer therapy. As healthcare systems remain single-disease focused, the optimal healthcare pathway for multimorbid patients is very complex [2]. Optimal delivery of care in this population faces multiple hurdles related to high cost, lack of logistical resources and lack of evidence-based care [2,3,4,5]. These challenges often lead to over-treatment, under-treatment or suboptimal outcomes. Aging is an individual process with increasing variation in comorbid disease. Therefore, chronological age, used for older patient stratification in oncology, often poorly correlates with biological age and functional status in this population. Geriatric assessment (GA) of older adults with cancer before the initiation of anticancer treatments is recommended by international guidelines [6,7].
GA is a multidimensional, interdisciplinary diagnostic process with a focus on medical, physiological, functional and psycho-social domains, employed in older vulnerable or frail patient populations, in order to identify impairments that are not routinely detected during usual oncology consultations. It also includes a coordinated and integrated plan for treatment and follow-up [8,9]. Identifying impairments through GA allows the implementation of personalized interventions resulting in several substantial benefits and improved outcomes [9]. A multidisciplinary consultative GA, a geriatrician embedded within an oncology clinic and primary management by a dual-trained geriatric oncologist are just a few examples of the various models for integrating geriatrics into oncology care that exist (reviewed in [5]). The ideal model does not exist, and GA should be flexible and tailored to the resources available. Multiple randomized controlled trials unequivocally demonstrated the benefits of GA and GA-guided interventions in reducing the toxicity of systemic treatments and improving patients’ health-related quality of life [10,11,12,13,14]. Whether and how often cancer providers use GA tools when treating older adults is not known, but a strong association was found between awareness of the ASCO Guidelines and the use of GA in practice [4,7]. GA is considered complex and resource demanding. Thus, the implementation is a challenge, especially in areas and practices with limited time, training and resources. In addition, relatively few geriatric specialized care providers exist to facilitate such assessments [15]. In Europe, there are countries where geriatrics is a specialty or a sub-specialty and others where it is a competence. In Portugal, geriatrics is a competence, and few geriatricians exist [16].
The aim of this work was to examine the position of geriatric oncology practice in Portugal and analyze medical professional’s current needs and perceptions in the management of older adults with cancer in our country.
2. Materials and Methods
2.1. Survey Development and Setting
A 10-question, online, web-based survey was prepared using the free server Google Forms (https://docs.google.com/forms, accessed on 13 August 2022) (Table 1 and Table S1). The questionnaire was anonymous and did not collect personal data other than age and gender. From September to October 2019, the survey was shared by the Portuguese Oncology Society mailing list, which included 700 members from different medical specialties at that time. First, a brief introduction outlining the main goals of the survey was presented. In order to submit the survey and be included, responses to all 10 questions were required. Respondents who provided consent to participate and responded to the full questionnaire were included.

Table 1.
Survey questions.
Questionnaire domains included the following respondent characteristics (gender, age, work geographic location, medical specialty). No financial incentives were offered to respondents. The time to complete the survey was on average 5 min.
2.2. Data Analysis
Descriptive analyses were conducted for responses to survey questions. When the questionnaires were sent in by the respondents, data were automatically saved in an Excel sheet (each question in separate columns) providing a database for analysis. Data were analyzed using IBM® SPSS v24.0. Descriptive statistics were presented as frequencies (n) and percentages (%) for categorical variables and as medians and range for continuous variables. A chi-square (χ2) test of independence was performed to examine the relationship between geographic differences and answering to “No” to questions 1 to 3. Age, location and gender differences were also explored for questions 5–8 using the χ2 test. p < 0.05 was considered as statistically significant.
3. Results
3.1. Facts and Figures—Policies for Older Adults with Cancer
A total of 222 physicians from different medical specialties completed the survey; the majority of respondents were medical oncologists (n = 119, 53.6%) (Table 2). There was a good geographical representation of the country (Table 2). When questioned about the existence of specific consultations or specialists for the care of elderly cancer patients, as well as management protocols for this population, 62.6% of physicians stated their institutions did not offer consultations in geriatric oncology and/or geriatrics (Figure 1A), and among the 12.6% of cases that did, geriatrics made up the majority (12.1%) (Figure 1A). Only 4.5% of respondents reported the existence of a physician dedicated to geriatric oncology in their hospitals (Figure 1B), and 14.9% of institutions provided specific guidelines for the management of older patients with cancer (Figure 1C). The majority of respondents (92.8%) perceived an increase, in clinical practice, in number of elderly cancer patients, and almost all (98.2%) admitted that older adults with cancer require different care than younger ones (Figure S1). A significant association between the absence of geriatric oncology practices and location of the practice within the country was found, with 77.1% of physicians from the north of the country answering “No” to the first three questions vs. 62.0% in the south, where the Portuguese capital is located (p = 0.033).
Table 2.
Respondent characteristics.
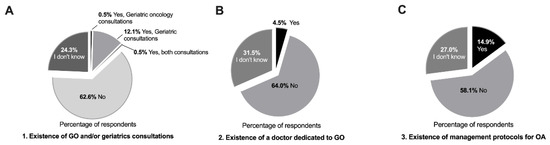
Figure 1.
Geriatric oncology situation in Portuguese hospitals. (A) Frequency of geriatric oncology and/or geriatrics care in Portuguese hospitals. (B) Medical oncology departments with physicians practicing geriatric oncology. (C) Existence of specific management protocols for the care of elderly cancer patients. (A–C) Values are expressed as percentages, total number of answers (n = 222). Abbreviations: GO—geriatric oncology; OA—older adults.
3.2. Geriatric Assessment and Screening
To support treatment decisions and evaluate older adults, 82.4% of clinicians sense a need for additional scales other than ECOG-Performance Status (ECOG-PS) and Karnofsky Performance Scale (KPS), and 12.6% have never thought about this subject (Figure S1). When asked about the use, in clinical practice, of geriatric assessment/screening tools to evaluate elderly patients, only 23.4% (n = 52) reported using these tools (Figure 2A). Medical oncologists and physicians from medical specialties (p = 0.009) and those practicing in the south of Portugal (p = 0.054) were more likely to report performing a GA (Table 3). The most listed tools reported by the respondents were the geriatric screening tools, Geriatric 8 (G8) questionnaire [17] and Vulnerable Elders Survey-13 (VES-13) [18,19] (n = 18 out of 47 responses), and tools to assess activities of daily living and instrumental activities of daily living (with Barthel and Katz indexes, respectively) (n = 13 out of 47) (Figure 2B). Almost all the professionals (95.0%) considered that there is a need for more education regarding geriatric oncology as well as additional training in this field, and 5.0% had never thought about this subject. In terms of age or gender, we found a high homogeneity among answers to questions 5 to 8, with no significant differences.
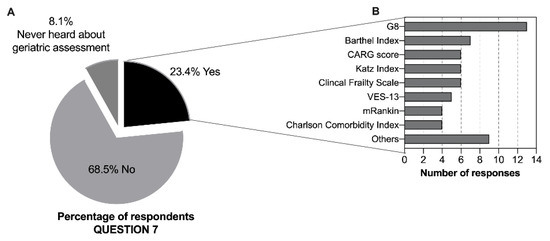
Figure 2.
Geriatric assessment awareness and use of GA tools. (A) Reported use, in clinical practice, of GA/geriatric screening to evaluate elderly cancer patients (n = 222, values are expressed as percentages). (B) Geriatric assessment or screening tools used (n = 47 respondents, absolute values are reported). Abbreviations: G8 (Geriatric 8); CARG (Cancer and Aging Research Group); VES-13 (Vulnerable Elderly Survey-13); mRankin (modified Rankin) scale; others include: Timed Up and Go Test (TUG), Mini Mental State Examination, ePrognosis, Geriatric Depression Scale (GDS), Palliative Prognostic Index (PPI), Lawton–Brody Scale.
Table 3.
Characteristics associated with the reported use of geriatric assessment.
3.3. Decision-Making and Active Aging Initiatives and Policies
The majority of the respondents (85.1%) considered that GA could be useful in guiding/defining a therapeutic strategy: 77.5% to detect frailty and 73.4% to predict toxicity and improve quality of life (Table 4). Regarding what is important to develop in the field of geriatric oncology in the country, 80.2% considered that GA should be done systematically at oncology departments. Education and training on the needs of elderly cancer patients, both at the undergraduate level and in advanced training, was identified as essential by 70.3%. Other suggestions were regarding geriatricians being a part of multidisciplinary teams (47.7%) and the creation of study groups and/or geriatric oncology units (45.9% and 30.6%, respectively).
Table 4.
Advantages of geriatric assessment and potential areas for the development of geriatric oncology.
4. Discussion
In this study, we set out to explore the current geriatric oncology practices in Portugal and analyze medical professionals’ current needs and perceptions in the management of older cancer patients. To our knowledge, this is the first survey of its kind in our country, as there were no data reported on this subject so far. Other countries, where knowledge and practices in geriatric oncology were examined by nationwide surveys, revealed a high demand for education, with an overall acceptance that the GA is an evidence-based way to evaluate older adults with cancer, though it is still less frequently used than anticipated [4,20,21,22].
Interestingly, 62.6% of respondents stated that there was no geriatric oncology care in their hospitals, and only a few (12.6%) reported having care in geriatrics. There was also a limited number of institutions that provided specific guidelines for the management of older patients with cancer. One of the possible explanations is the limited number of geriatricians available in the country (n = 64) [16]. In Portugal, geriatrics is not recognized as a medical specialty but as a competence by the Portuguese Medical Association, and this recognition is relatively recent (since 2014) [16]. As a consequence, the number of older adults per geriatrician in Portugal is considerable and estimated to be 31.590 [23]. In Spain, according to the Spanish Society of Geriatrics and Gerontology, there are approximately 2456 physicians involved in geriatric care (970 are geriatricians), and 33 accredited centers to train geriatricians [23,24].
According to Statistics Portugal, there was a 4.4% increase in the last 10 years in the population aged 65 years or older in Portugal, and considering the 2.1% decrease in the total population, the absolute number of older adults is larger, making Portugal one of the most aged countries in Europe [23,25]. This is in line with respondents’ perceptions, as the majority (92.8%) reported an increase in the number of elderly cancer patients in clinical practice.
Almost all the respondents (98.2%) admitted that older adults with cancer require different care than younger patients, and 82.4% of clinicians recognized that ECOG-PS and KPS, used in clinical practice to support treatment decisions, are not enough. These findings are significant because there is increasing evidence that conducting a GA can lead to adaptations in clinical management and improved outcomes for older adults with cancer [26]. However, only a small percentage of respondents (23.4%) reported using GA and/or geriatric screening tools to assess elderly patients in clinical practice, and surprisingly, 8.1% had never heard of GA. The proportion of physicians who reported performing a GA is comparable to that found in other studies, such as in a survey of cancer providers in the United States (U.S.) (21%) [4] or a nationwide survey in Mexico (18.9%) [20]. Studies from European countries, such as Spain, revealed a 31% use of GA in clinical practice [21], and an older study from the Netherlands showed that 60% of healthcare professionals performed some sort of geriatric evaluation [27]. Because Europe has the largest population share of older adults worldwide, the increasing awareness of the need for geriatric oncology practices in this continent is not surprising.
In the south of Portugal, where Lisbon the capital is located, there was a significantly higher percentage of physicians reporting the use of GA, which might be related to the relative higher number of geriatric and geriatric oncology practices and/or protocols implemented, when compared to other locations in the country. This reflects that there is an urgent need to increase awareness of the growing needs of older patients with cancer and guidelines available, and to implement healthcare policies aimed to improve their care. Global geriatric oncology initiatives are revolutionizing the way elderly cancer patients are being treated [2,28], particularly in Europe, where there have been a rising number of new specialized clinics, initiatives to enroll in clinical trials and joint initiatives to develop clinical trials for older adults with cancer [3].
Despite its uncommon usage, the majority of respondents considered that GA would be helpful for guiding treatment decisions, identifying frailty, predicting toxicity and improving quality of life. Thus, GA must serve as the focal point of the decision-making process [29].
The most crucial issues identified, in terms of what needs to advance and improve in the field of geriatric oncology in the country, were GA systematically performed at oncology services (80.2%) and improvement in education and training on the needs of elderly patients (70.3%). Other suggestions included geriatricians being a part of multidisciplinary teams and the creation of study groups and/or geriatric oncology units. Most of the needs in geriatric oncology identified by Portuguese respondents are common among European countries, as recently revealed by an ESMO–SIOG Joint Working Group short survey on the management of older patients with cancer [30].
In Portugal, there are four centers offering postgraduate geriatrics training, although there are no specific programs toward training in geriatric oncology. There is also a lack of training at the undergraduate level. Therefore, there is a need to disseminate knowledge and integrate geriatric oncology in the curricula for healthcare professionals’ education, in order to develop a workforce in the field and in the context of a broader implementation of active aging-related policies and initiatives.
As a consequence of this growing need, in 2020, the Portuguese Oncology Society established the Geriatric Oncology Working Group (GTOG), with the aim to improve knowledge and develop cooperative clinical, educational and research initiatives in geriatric oncology [31]. Several partnerships have been established so far, with the International Society of Geriatric Oncology (SIOG), Oncogeriatrics Group of the Spanish Society of Medical Oncology (SEOM) and with the Geriatric Study Group of the Portuguese Internal Medicine Society. These groups need to cooperate in order to provide training and funding for scientific initiatives, as these objectives can only be accomplished with collaborative work.
Six Portuguese oncologists have taken part in the SIOG Advanced Course in Geriatric Oncology since this survey was performed (in addition to three more who had completed this course previously), and others were/are being trained in centers with geriatric oncology expertise in Europe, in addition to the educational sessions promoted by GTOG in the last two years.
The incorporation of geriatric evaluation into routine clinical practice is hampered by a number of factors, including a lack of time, a shortage of geriatricians and the absence of a national plan. However, we must not forget that a GA can change oncologic treatment plans, lead to non-oncologic interventions, increase the likelihood that a patient will complete their treatment, minimize the risk of complications and toxicity and improve their physical health and quality of life [26]. Accordingly, GA must serve as the focal point of any intervention and be used as part of the standard of care for older patients with cancer since it is just as crucial as recommending an oncologic therapy. This study also serves as a reminder that there is still more work to be done in order to put active aging-related policies and initiatives into practice.
5. Limitations
Limitations to this study that may be addressed in future research include the relatively small sample size, which does not allow a generalization of the conclusions. Although comparable to other studies of this kind, the low response rate (31.7%) makes it difficult to rule out a potential response bias in favor of individuals with an interest in geriatric oncology. The variations and similarities between the Portuguese setting and other European nations should be compared, especially with regard to how each nation develops its aging policies while taking into account international guidelines. Differences in the type of clinical practice (academic/university hospital, comprehensive cancer center or general hospital) were not evaluated in this questionnaire. Another limitation is the need to combine the perceptions and needs in geriatric oncology identified by healthcare professionals in the survey with a mapping of cancer and aging policies in Portugal. The Portuguese Oncology Society’s Geriatric Oncology Working Group will play a significant role in this area.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/geriatrics7050091/s1: Figure S1: Perceptions and challenging factors in the management of older patients with cancer. Table S1: Survey questions and response options.
Author Contributions
All authors met the ICMJE authorship criteria. Conceptualization, methodology and validation, J.M. and S.C.; formal analysis, investigation, resources, data curation and writing—original draft preparation, J.M.; writing—review and editing, J.M. and S.C. supervision, J.M. and S.C.; project administration, J.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
In light of the observational nature, no ethical approval was required.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors acknowledge all the participants who answered the survey and the Portuguese Oncology Society for supporting and sharing the survey.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kanesvaran, R.; Mohile, S.; Soto-Perez-De-Celis, E.; Singh, H. The Globalization of Geriatric Oncology: From Data to Practice. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, e107–e115. [Google Scholar] [CrossRef] [PubMed]
- Soto-Perez-De-Celis, E.; de Glas, N.A.; Hsu, T.; Kanesvaran, R.; Steer, C.; Navarrete-Reyes, A.P.; Battisti, N.M.L.; Chavarri-Guerra, Y.; O’Donovan, A.; Avila-Funes, J.A.; et al. Global geriatric oncology: Achievements and challenges. J. Geriatr. Oncol. 2017, 8, 374–386. [Google Scholar] [CrossRef]
- Dale, W.; Williams, G.R.; MacKenzie, A.R.; Soto-Perez-De-Celis, E.; Maggiore, R.J.; Merrill, J.K.; Katta, S.; Smith, K.T.; Klepin, H.D. How Is Geriatric Assessment Used in Clinical Practice for Older Adults With Cancer? A Survey of Cancer Providers by the American Society of Clinical Oncology. JCO Oncol. Pr. 2021, 17, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Chapman, A.E.; Elias, R.; Plotkin, E.; Lowenstein, L.M.; Swartz, K. Models of Care in Geriatric Oncology. J. Clin. Oncol. 2021, 39, 2195–2204. [Google Scholar] [CrossRef]
- Loh, K.P.; Soto-Perez-De-Celis, E.; Hsu, T.; De Glas, N.A.; Battisti, N.M.L.; Baldini, C.; Rodrigues, M.; Lichtman, S.M.; Wildiers, H. What Every Oncologist Should Know About Geriatric Assessment for Older Patients With Cancer: Young International Society of Geriatric Oncology Position Paper. J. Oncol. Pr. 2018, 14, 85–94. [Google Scholar] [CrossRef]
- Mohile, S.G.; Dale, W.; Somerfield, M.R.; Hurria, A. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology Summary. J. Oncol. Pr. 2018, 14, 442–446. [Google Scholar] [CrossRef]
- Outlaw, D.; Abdallah, M.; A Gil-Jr, L.; Giri, S.; Hsu, T.; Krok-Schoen, J.L.; Liposits, G.; Madureira, T.; Marinho, J.; Subbiah, I.M.; et al. The Evolution of Geriatric Oncology and Geriatric Assessment over the Past Decade. Semin. Radiat. Oncol. 2022, 32, 98–108. [Google Scholar] [CrossRef]
- Li, D.; Soto-Perez-De-Celis, E.; Hurria, A. Geriatric Assessment and Tools for Predicting Treatment Toxicity in Older Adults With Cancer. Cancer J. 2017, 23, 206–210. [Google Scholar] [CrossRef]
- Lund, C.M.; Vistisen, K.K.; Olsen, A.P.; Bardal, P.; Schultz, M.; Dolin, T.G.; Rønholt, F.; Johansen, J.S.; Nielsen, D.L. The effect of geriatric intervention in frail older patients receiving chemotherapy for colorectal cancer: A randomised trial (GERICO). Br. J. Cancer 2021, 124, 1949–1958. [Google Scholar] [CrossRef]
- Soo, W.-K.; King, M.; Pope, A.; Parente, P.; Darzins, P.; Davis, I.D. Integrated geriatric assessment and treatment (INTEGERATE) in older people with cancer planned for systemic anticancer therapy. J. Clin. Oncol. 2020, 38, 12011. [Google Scholar] [CrossRef]
- Nipp, R.D.; Qian, C.L.; Knight, H.P.; Ferrone, C.R.; Kunitake, H.; Castillo, C.F.-D.; Lanuti, M.; Qadan, M.; Ricciardi, R.; Lillemoe, K.D.; et al. Effects of a perioperative geriatric intervention for older adults with Cancer: A randomized clinical trial. J. Geriatr. Oncol. 2022, 13, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Mohile, S.G.; Mohamed, M.R.; Xu, H.; Culakova, E.; Loh, K.P.; Magnuson, A.; A Flannery, M.; Obrecht, S.; Gilmore, N.; Ramsdale, E.; et al. Evaluation of geriatric assessment and management on the toxic effects of cancer treatment (GAP70+): A cluster-randomised study. Lancet 2021, 398, 1894–1904. [Google Scholar] [CrossRef]
- Li, D.; Sun, C.-L.; Kim, H.; Soto-Perez-De-Celis, E.; Chung, V.; Koczywas, M.; Fakih, M.; Chao, J.; Chien, L.C.; Charles, K.; et al. Geriatric Assessment–Driven Intervention (GAIN) on Chemotherapy-Related Toxic Effects in Older Adults With Cancer. JAMA Oncol. 2021, 7, e214158. [Google Scholar] [CrossRef]
- Williams, G.R.; Weaver, K.E.; Lesser, G.J.; Dressler, E.; Winkfield, K.M.; Neuman, H.B.; Kazak, A.E.; Carlos, R.; Gansauer, L.J.; Kamen, C.S.; et al. Capacity to Provide Geriatric Specialty Care for Older Adults in Community Oncology Practices. Oncologist 2020, 25, 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- EuGMS—European Geriatric Medicine Society. Available online: https://www.eugms.org/our-members/national-societies/portugal.html (accessed on 10 August 2022).
- Bellera, C.A.; Rainfray, M.; Mathoulin-Pélissier, S.; Mertens, C.; Delva, F.; Fonck, M.; Soubeyran, P.L. Screening older cancer patients: First evaluation of the G-8 geriatric screening tool. Ann. Oncol. 2012, 23, 2166–2172. [Google Scholar] [CrossRef]
- Carneiro, F.; Sousa, N.; Azevedo, L.; Saliba, D. Vulnerability in elderly patients with gastrointestinal cancer—translation, cultural adaptation and validation of the European Portuguese version of the Vulnerable Elders Survey (VES-13). BMC Cancer 2015, 15, 723. [Google Scholar] [CrossRef]
- Saliba, D.; Elliott, M.; Rubenstein, L.Z.; Solomon, D.H.; Young, R.T.; Kamberg, C.J.; Roth, R.C.; MacLean, C.H.; Shekelle, P.G.; Sloss, E.M.; et al. The Vulnerable Elders Survey: A Tool for Identifying Vulnerable Older People in the Community. J. Am. Geriatr. Soc. 2001, 49, 1691–1699. [Google Scholar] [CrossRef]
- Verduzco-Aguirre, H.C.; Guerra, L.M.B.; Culakova, E.; Chargoy, J.M.; Martínez-Said, H.; Beulo, G.Q.; Mohile, S.G.; Soto-Perez-De-Celis, E. Barriers and Facilitators for the Implementation of Geriatric Oncology Principles in Mexico: A Mixed-Methods Study. JCO Glob. Oncol. 2022, 8, e2100390. [Google Scholar] [CrossRef]
- Gironés, R.; On behalf of the Spanish Working Group on Geriatric Oncology of the Spanish Society of Medical Oncology (SEOM); Morilla, I.; Guillen-Ponce, C.; Torregrosa, M.D.; Paredero, I.; Bustamante, E.; del Barco, S.; Soler, G.; Losada, B.; et al. Geriatric oncology in Spain: Survey results and analysis of the current situation. Clin. Transl. Oncol. 2018, 20, 1087–1092. [Google Scholar] [CrossRef]
- To, T.H.; Soo, W.K.; Lane, H.; Khattak, A.; Steer, C.; Devitt, B.; Dhillon, H.M.; Booms, A.; Phillips, J. Utilisation of geriatric assessment in oncology—A survey of Australian medical oncologists. J. Geriatr. Oncol. 2019, 10, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Soto-Perez-De-Celis, E.; Cordoba, R.; Gironés, R.; Karnakis, T.; Paredero, I.; Chavarri-Guerra, Y.; Navarrete-Reyes, A.P.; Avila-Funes, J.A. Cancer and aging in Ibero-America. Clin. Transl. Oncol. 2018, 20, 1117–1126. [Google Scholar] [CrossRef]
- EuGMS—European Geriatric Medicine Society. Available online: https://www.eugms.org/our-members/national-societies/spain-segg.html (accessed on 10 August 2022).
- INE. Censos: INE Statistics Portugal. 2021. Available online: https://www.ine.pt/scripts/db_censos_2021.html (accessed on 10 August 2022).
- Hamaker, M.; Lund, C.; Molder, M.T.; Soubeyran, P.; Wildiers, H.; van Huis, L.; Rostoft, S. Geriatric assessment in the management of older patients with cancer—A systematic review (update). J. Geriatr. Oncol. 2022, 13, 761–777. [Google Scholar] [CrossRef] [PubMed]
- Jonker, J.; Smorenburg, C.; Schiphorst, A.; Van Rixtel, B.; Portielje, J.; Hamaker, M. Geriatric oncology in the Netherlands: A survey of medical oncology specialists and oncology nursing specialists. Eur. J. Cancer Care 2014, 23, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Extermann, M.; Brain, E.; Canin, B.; Cherian, M.N.; Cheung, K.-L.; de Glas, N.; Devi, B.; Hamaker, M.; Kanesvaran, R.; Karnakis, T.; et al. Priorities for the global advancement of care for older adults with cancer: An update of the International Society of Geriatric Oncology Priorities Initiative. Lancet Oncol. 2021, 22, e29–e36. [Google Scholar] [CrossRef]
- Dumontier, C.; Loh, K.P.; Bain, P.A.; Silliman, R.A.; Hshieh, T.; Abel, G.A.; Djulbegovic, B.; Driver, J.A.; Dale, W. Defining Undertreatment and Overtreatment in Older Adults With Cancer: A Scoping Literature Review. J. Clin. Oncol. 2020, 38, 2558–2569. [Google Scholar] [CrossRef] [PubMed]
- Baldini, C.; Brain, E.; Rostoft, S.; Biganzoli, L.; Goede, V.; Kanesvaran, R.; Quoix, E.; Steer, C.; Papamichael, D.; Wildiers, H. 1827P European Society for Medical Oncology (ESMO)/International Society of Geriatric Oncology (SIOG) Joint Working Group (WG) survey on management of older patients with cancer. Ann. Oncol. 2021, 32, S1237–S1238. [Google Scholar] [CrossRef]
- Portuguese Oncology Society. Available online: https://www.sponcologia.pt/pt/grupos-de-trabalho/ (accessed on 10 August 2022).


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).