Global Cognitive Impairment Prevalence and Incidence in Community Dwelling Older Adults—A Systematic Review


Abstract
1. Introduction
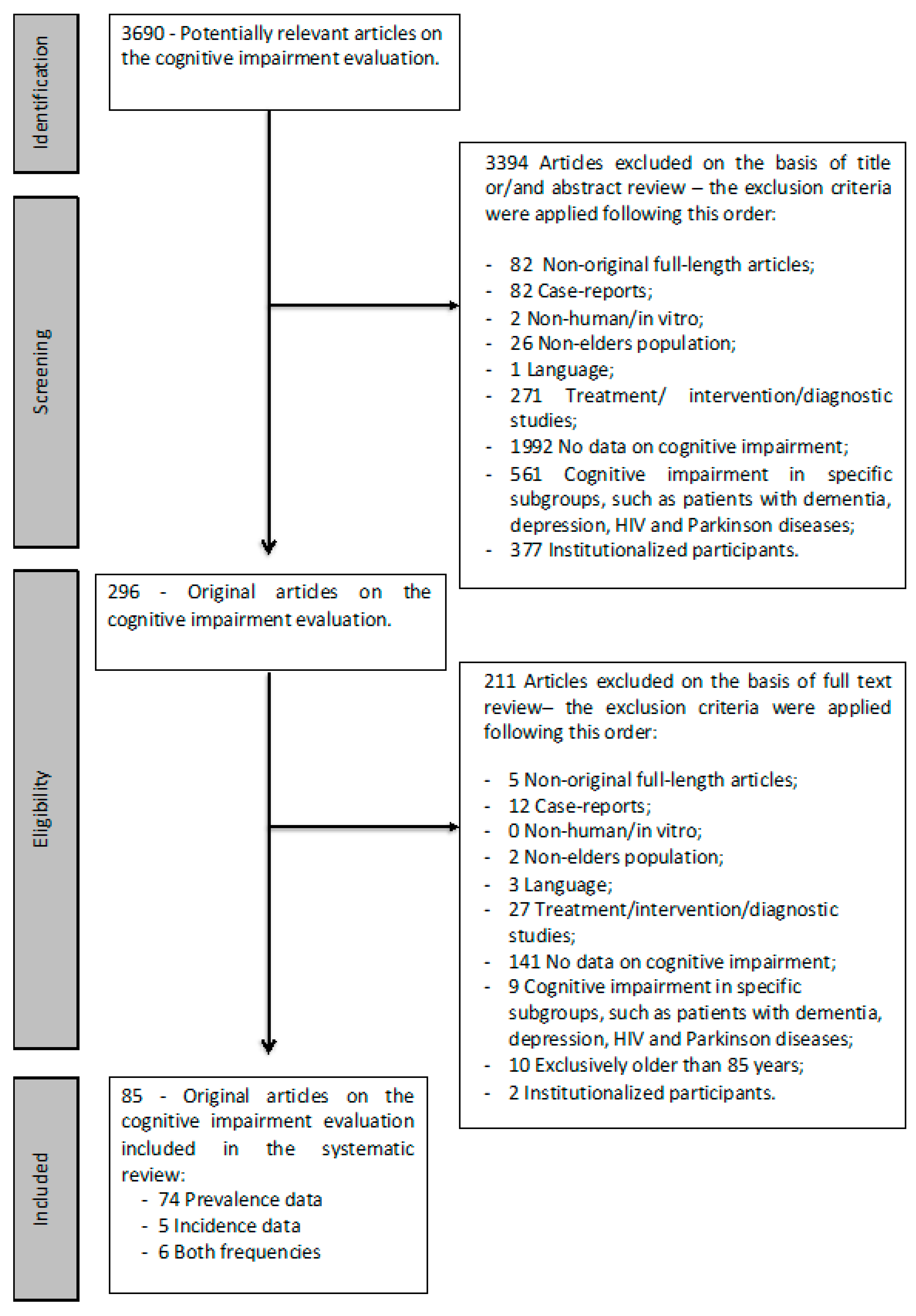
2. Materials and Methods
2.1. Statistical Analysis
2.2. Data Analysis
3. Results
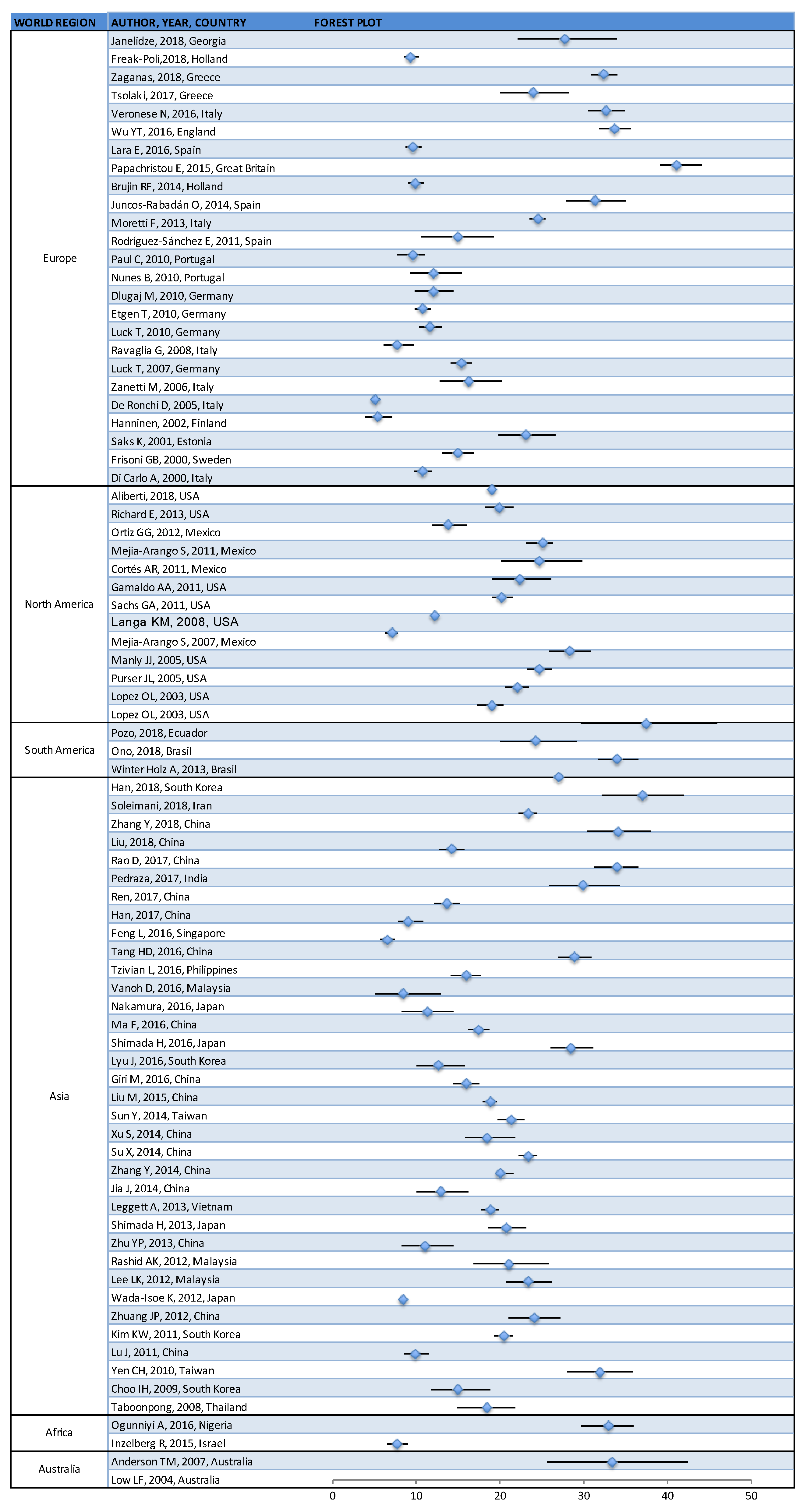
3.1. Prevalence of Cognitive Impairment
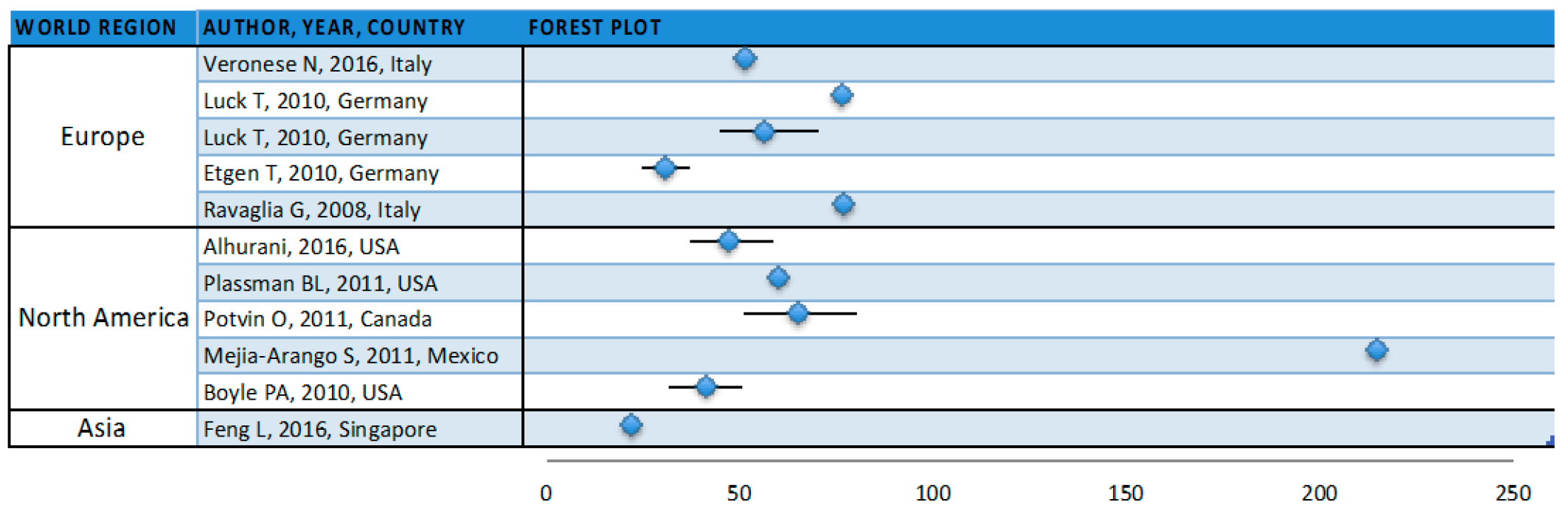
3.2. Incidence of Cognitive Impairment
4. Discussion
4.1. Methodological Considerations
4.2. Future Directions
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- UN. World Population Ageing 2015; United Nations: San Francisco, CA, USA, 2015. [Google Scholar]
- Crimmins, E.M.; Kim, J.K.; Langa, K.M.; Weir, D.R. Assessment of cognition using surveys and neuropsychological assessment: The Health and Retirement Study and the Aging, Demographics, and Memory Study. J. Gerontol. B Psychol. Sci. Soc. Sci. 2011, 66 (Suppl. 1), i162–i171. [Google Scholar] [CrossRef]
- ICD-10. International Statistical Classification of Diseases and Related Health Problems 10th Revision. Available online: http://apps.who.int/classifications/icd10/browse/2010/en#/F06.7 (accessed on 10 January 2013).
- Luchsinger, J.A. Type 2 diabetes and cognitive impairment: Linking mechanisms. J. Alzheimers Dis. 2012, 30 (Suppl. 2), S185–S198. [Google Scholar] [CrossRef]
- Park, M.H.; Kwon, D.Y.; Jung, J.M.; Han, C.; Jo, I.; Jo, S.A. Mini-Mental Status Examination as predictors of mortality in the elderly. Acta Psychiatr. Scand. 2013, 127, 298–304. [Google Scholar] [CrossRef]
- Roberts, R.; Knopman, D.S. Classification and epidemiology of MCI. Clin. Geriatr. Med. 2013, 29, 753–772. [Google Scholar] [CrossRef] [PubMed]
- Geda, Y.E. Mild cognitive impairment in older adults. Curr. Psychiatry Rep. 2012, 14, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Millan-Calenti, J.C.; Tubio, J.; Pita-Fernandez, S.; Gonzalez-Abraldes, I.; Lorenzo, T.; Maseda, A. Prevalence of cognitive impairment: Effects of level of education, age, sex and associated factors. Dement. Geriatr. Cogn. Disord. 2009, 28, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, P.S.; Lipnicki, D.M.; Kochan, N.A.; Crawford, J.D.; Thalamuthu, A.; Andrews, G.; Brayne, C.; Matthews, F.E.; Stephan, B.C.; Lipton, R.B.; et al. The Prevalence of Mild Cognitive Impairment in Diverse Geographical and Ethnocultural Regions: The COSMIC Collaboration. PLoS ONE 2015, 10, e0142388. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung., and Blood Institute; National Institutes of Health; U.S. Department of Health and Human Services. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 27 March 2020).
- Janelidze, M.; Mikeladze, N.; Bochorishvili, N.; Dzagnidze, A.; Kapianidze, M.; Mikava, N.; Khatiashvili, I.; Mirvelashvili, E.; Shiukashvili, N.; Lynch, J.; et al. Mild Cognitive Impairment in Republic of Georgia. Gerontol. Geriatr. Med. 2018, 4, 2333721418771408. [Google Scholar] [CrossRef] [PubMed]
- Freak-Poli, R.; Licher, S.; Ryan, J.; Ikram, M.A.; Tiemeier, H. Cognitive Impairment, Sexual Activity and Physical Tenderness in Community-Dwelling Older Adults: A Cross-Sectional Exploration. Gerontology 2018, 64, 589–602. [Google Scholar] [CrossRef]
- Zaganas, I.V.; Simos, P.; Basta, M.; Kapetanaki, S.; Panagiotakis, S.; Koutentaki, I.; Fountoulakis, N.; Bertsias, A.; Duijker, G.; Tziraki, C.; et al. The Cretan Aging Cohort: Cohort Description and Burden of Dementia and Mild Cognitive Impairment. Am. J. Alzheimers Dis. Other Demen. 2019, 34, 23–33. [Google Scholar] [CrossRef]
- Tsolaki, M.; Gkioka, M.; Verykouki, E.; Galoutzi, N.; Kavalou, E.; Pattakou-Parasyri, V. Prevalence of Dementia, Depression, and Mild Cognitive Impairment in a Rural Area of the Island of Crete, Greece. Am. J. Alzheimers Dis Other Demen. 2017, 32, 252–264. [Google Scholar] [CrossRef]
- Veronese, N.; Stubbs, B.; Trevisan, C.; Bolzetta, F.; De Rui, M.; Solmi, M.; Sartori, L.; Musacchio, E.; Zambon, S.; Perissinotto, E.; et al. What physical performance measures predict incident cognitive decline among intact older adults? A 4.4year follow up study. Exp. Gerontol. 2016, 81, 110–118. [Google Scholar] [CrossRef]
- Wu, Y.T.; Prina, A.M.; Jones, A.P.; Barnes, L.E.; Matthews, F.E.; Brayne, C. Community environment, cognitive impairment and dementia in later life: Results from the Cognitive Function and Ageing Study. Age Ageing 2015, 44, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Lara, E.; Koyanagi, A.; Olaya, B.; Lobo, A.; Miret, M.; Tyrovolas, S.; Ayuso-Mateos, J.L.; Haro, J.M. Mild cognitive impairment in a Spanish representative sample: Prevalence and associated factors. Int. J. Geriatr. Psychiatry 2016, 31, 858–867. [Google Scholar] [CrossRef]
- Papachristou, E.; Ramsay, S.E.; Lennon, L.T.; Papacosta, O.; Iliffe, S.; Whincup, P.H.; Wannamethee, S.G. The relationships between body composition characteristics and cognitive functioning in a population-based sample of older British men. BMC Geriatr. 2015, 15, 172. [Google Scholar] [CrossRef]
- De Bruijn, R.F.; Akoudad, S.; Cremers, L.G.; Hofman, A.; Niessen, W.J.; van der Lugt, A.; Koudstaal, P.J.; Vernooij, M.W.; Ikram, M.A. Determinants, MRI correlates, and prognosis of mild cognitive impairment: The Rotterdam Study. J. Alzheimers Dis. 2014, 42 (Suppl. 3), S239–S249. [Google Scholar] [CrossRef] [PubMed]
- Juncos-Rabadan, O.; Pereiro, A.X.; Facal, D.; Lojo, C.; Caamano, J.A.; Sueiro, J.; Boveda, J.; Eiroa, P. Prevalence and correlates of mild cognitive impairment in adults aged over 50 years with subjective cognitive complaints in primary care centers. Geriatr. Gerontol. Int. 2014, 14, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Moretti, F.; De Ronchi, D.; Palmer, K.; Forlani, C.; Morini, V.; Ferrari, B.; Dalmonte, E.; Atti, A.R. Prevalence and characteristics of mild cognitive impairment in the general population. Data from an Italian population-based study: The Faenza Project. Aging Ment. Health 2013, 17, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Sanchez, E.; Mora-Simon, S.; Patino-Alonso, M.C.; Garcia-Garcia, R.; Escribano-Hernandez, A.; Garcia-Ortiz, L.; Perea-Bartolome, M.V.; Gomez-Marcos, M.A. Prevalence of cognitive impairment in individuals aged over 65 in an urban area: DERIVA study. BMC Neurol. 2011, 11, 147. [Google Scholar] [CrossRef] [PubMed]
- Paul, C.; Ribeiro, O.; Santos, P. Cognitive impairment in old people living in the community. Arch. Gerontol. Geriatr. 2010, 51, 121–124. [Google Scholar] [CrossRef]
- Nunes, B.; Silva, R.D.; Cruz, V.T.; Roriz, J.M.; Pais, J.; Silva, M.C. Prevalence and pattern of cognitive impairment in rural and urban populations from Northern Portugal. BMC Neurol. 2010, 10, 42. [Google Scholar] [CrossRef] [PubMed]
- Dlugaj, M.; Weimar, C.; Wege, N.; Verde, P.E.; Gerwig, M.; Dragano, N.; Moebus, S.; Jockel, K.H.; Erbel, R.; Siegrist, J. Prevalence of mild cognitive impairment and its subtypes in the Heinz Nixdorf Recall study cohort. Dement. Geriatr. Cogn. Disord. 2010, 30, 362–373. [Google Scholar] [CrossRef]
- Etgen, T.; Sander, D.; Huntgeburth, U.; Poppert, H.; Forstl, H.; Bickel, H. Physical activity and incident cognitive impairment in elderly persons: The INVADE study. Arch. Intern. Med. 2010, 170, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Luck, T.; Riedel-Heller, S.G.; Luppa, M.; Wiese, B.; Wollny, A.; Wagner, M.; Bickel, H.; Weyerer, S.; Pentzek, M.; Haller, F.; et al. Risk factors for incident mild cognitive impairment—Results from the German Study on Ageing, Cognition and Dementia in Primary Care Patients (AgeCoDe). Acta Psychiatr. Scand. 2010, 121, 260–272. [Google Scholar] [CrossRef]
- Ravaglia, G.; Forti, P.; Montesi, F.; Lucicesare, A.; Pisacane, N.; Rietti, E.; Dalmonte, E.; Bianchin, M.; Mecocci, P. Mild cognitive impairment: Epidemiology and dementia risk in an elderly Italian population. J. Am. Geriatr. Soc. 2008, 56, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Luck, T.; Riedel-Heller, S.G.; Kaduszkiewicz, H.; Bickel, H.; Jessen, F.; Pentzek, M.; Wiese, B.; Koelsch, H.; van den Bussche, H.; Abholz, H.H.; et al. Mild cognitive impairment in general practice: Age-specific prevalence and correlate results from the German study on ageing, cognition and dementia in primary care patients (AgeCoDe). Dement. Geriatr. Cogn. Disord. 2007, 24, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Zanetti, M.; Ballabio, C.; Abbate, C.; Cutaia, C.; Vergani, C.; Bergamaschini, L. Mild cognitive impairment subtypes and vascular dementia in community-dwelling elderly people: A 3-year follow-up study. J. Am. Geriatr. Soc. 2006, 54, 580–586. [Google Scholar] [CrossRef]
- De Ronchi, D.; Berardi, D.; Menchetti, M.; Ferrari, G.; Serretti, A.; Dalmonte, E.; Fratiglioni, L. Occurrence of cognitive impairment and dementia after the age of 60: A population-based study from Northern Italy. Dement. Geriatr. Cogn. Disord. 2005, 19, 97–105. [Google Scholar] [CrossRef]
- Hanninen, T.; Hallikainen, M.; Tuomainen, S.; Vanhanen, M.; Soininen, H. Prevalence of mild cognitive impairment: A population-based study in elderly subjects. Acta Neurol. Scand. 2002, 106, 148–154. [Google Scholar] [CrossRef]
- Saks, K.; Kolk, H.; Allev, R.; Soots, A.; Koiv, K.; Paju, I.; Jaanson, K.; Schneider, G. Health status of the older population in Estonia. Croat. Med. J. 2001, 42, 663–668. [Google Scholar]
- Frisoni, G.B.; Fratiglioni, L.; Fastbom, J.; Guo, Z.; Viitanen, M.; Winblad, B. Mild cognitive impairment in the population and physical health: Data on 1,435 individuals aged 75 to 95. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M322–M328. [Google Scholar] [CrossRef] [PubMed]
- Di Carlo, A.; Baldereschi, M.; Amaducci, L.; Maggi, S.; Grigoletto, F.; Scarlato, G.; Inzitari, D. Cognitive impairment without dementia in older people: Prevalence, vascular risk factors, impact on disability. The Italian Longitudinal Study on Aging. J. Am. Geriatr. Soc. 2000, 48, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, M.J.R.; Cenzer, I.S.; Smith, A.K.; Lee, S.J.; Yaffe, K.; Covinsky, K.E. Assessing Risk for Adverse Outcomes in Older Adults: The Need to Include Both Physical Frailty and Cognition. J. Am. Geriatr. Soc. 2019, 67, 477–483. [Google Scholar] [CrossRef]
- Richard, E.; Reitz, C.; Honig, L.H.; Schupf, N.; Tang, M.X.; Manly, J.J.; Mayeux, R.; Devanand, D.; Luchsinger, J.A. Late-life depression, mild cognitive impairment, and dementia. JAMA Neurol. 2013, 70, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, G.G.; Arias-Merino, E.D.; Flores-Saiffe, M.E.; Velazquez-Brizuela, I.E.; Macias-Islas, M.A.; Pacheco-Moises, F.P. Prevalence of Cognitive Impairment and Depression among a Population Aged over 60 Years in the Metropolitan Area of Guadalajara, Mexico. Curr. Gerontol. Geriatr. Res. 2012, 2012, 175019. [Google Scholar] [CrossRef]
- Mejia-Arango, S.; Gutierrez, L.M. Prevalence and incidence rates of dementia and cognitive impairment no dementia in the Mexican population: Data from the Mexican Health and Aging Study. J. Aging Health 2011, 23, 1050–1074. [Google Scholar] [CrossRef]
- Cortes, A.R.; Villarreal, E.; Galicia, L.; Martinez, L.; Vargas, E.R. Cross sectional geriatric assessment of Mexican older people. Rev. Med. Chile 2011, 139, 725–731. [Google Scholar] [CrossRef]
- Gamaldo, A.A.; Allaire, J.C.; Sims, R.C.; Whitfield, K.E. Assessing mild cognitive impairment among older African Americans. Int. J. Geriatr. Psychiatry 2010, 25, 748–755. [Google Scholar] [CrossRef]
- Sachs-Erisson, N.; Sawyer, K.; Corsentino, E.; Collins, N.; Steffens, D.C. The moderating effect of the APOE [small element of] 4 allele on the relationship between hippocampal volume and cognitive decline in older depressed patients. Am. J. Geriatr. Psychiatry 2011, 19, 23–32. [Google Scholar] [CrossRef]
- Langa, K.M.; Larson, E.B.; Karlawish, J.H.; Cutler, D.M.; Kabeto, M.U.; Kim, S.Y.; Rosen, A.B. Trends in the prevalence and mortality of cognitive impairment in the United States: Is there evidence of a compression of cognitive morbidity? Alzheimers Dement. 2008, 4, 134–144. [Google Scholar] [CrossRef]
- Mejia-Arango, S.; Miguel-Jaimes, A.; Villa, A.; Ruiz-Arregui, L.; Gutierrez-Robledo, L.M. Cognitive impairment and associated factors in older adults in Mexico. Salud. Publica Mex. 2007, 49 (Suppl. 4), S475–S481. [Google Scholar]
- Manly, J.J.; Bell-McGinty, S.; Tang, M.X.; Schupf, N.; Stern, Y.; Mayeux, R. Implementing diagnostic criteria and estimating frequency of mild cognitive impairment in an urban community. Arch. Neurol. 2005, 62, 1739–1746. [Google Scholar] [CrossRef] [PubMed]
- Purser, J.L.; Fillenbaum, G.G.; Pieper, C.F.; Wallace, R.B. Mild cognitive impairment and 10-year trajectories of disability in the Iowa Established Populations for Epidemiologic Studies of the Elderly cohort. J. Am. Geriatr. Soc. 2005, 53, 1966–1972. [Google Scholar] [CrossRef] [PubMed]
- Lopez, O.L. Classification of mild cognitive impairment in a population study. Rev. Neurol. 2003, 37, 140–144. [Google Scholar]
- Lopez, O.L.; Jagust, W.J.; DeKosky, S.T.; Becker, J.T.; Fitzpatrick, A.; Dulberg, C.; Breitner, J.; Lyketsos, C.; Jones, B.; Kawas, C.; et al. Prevalence and classification of mild cognitive impairment in the Cardiovascular Health Study Cognition Study: Part 1. Arch. Neurol. 2003, 60, 1385–1389. [Google Scholar] [CrossRef]
- Espinosa Del Pozo, P.H.; Espinosa, P.S.; Donadi, E.A.; Martinez, E.Z.; Salazar-Uribe, J.C.; Guerrero, M.A.; Moriguti, J.C.; Colcha, M.C.; Garcia, S.E.; Naranjo, R.; et al. Cognitive Decline in Adults Aged 65 and Older in Cumbaya, Quito, Ecuador: Prevalence and Risk Factors. Cureus 2018, 10, e3269. [Google Scholar] [CrossRef] [PubMed]
- Ono, L.M.; Confortin, S.C.; Figueiro, T.H.; Rech, C.R.; d’Orsi, E. Influence of instrumental activities of daily living on the cognitive impairment: EpiFloripa study. Aging Ment. Health 2018, 1–5. [Google Scholar] [CrossRef]
- Winter Holz, A.; Nunes, B.P.; Thume, E.; Lange, C.; Facchini, L.A. Prevalence of cognitive impairment and associated factors among the elderly in Bage, Rio Grande do Sul, Brazil. Rev. Bras. Epidemiol. 2013, 16, 880–888. [Google Scholar] [CrossRef]
- Han, J.W.; Kim, T.H.; Kwak, K.P.; Kim, K.; Kim, B.J.; Kim, S.G.; Kim, J.L.; Kim, T.H.; Moon, S.W.; Park, J.Y.; et al. Overview of the Korean Longitudinal Study on Cognitive Aging and Dementia. Psychiatry Investig. 2018, 15, 767–774. [Google Scholar] [CrossRef]
- Soleimani, R.; Shokrgozar, S.; Fallahi, M.; Kafi, H.; Kiani, M. An investigation into the prevalence of cognitive impairment and the performance of older adults in Guilan province. J. Med. Life 2018, 11, 247–253. [Google Scholar] [CrossRef]
- Zhang, Y.; Guan, Y.; Shi, Z.; Yue, W.; Liu, S.; Liu, S.; Lu, H.; Zhao, L.; Zhang, Y.; Su, W.; et al. Sex Differences in the Prevalence of and Risk Factors for Cognitive Impairment No Dementia among the Elderly in a Rural Area of Northern China: A Population-Based Cross-Sectional Study. Neuroepidemiology 2018, 52, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yin, X.; Tan, A.; He, M.; Jiang, D.; Hou, Y.; Lu, Y.; Mao, Z. Correlates of Mild Cognitive Impairment of Community-Dwelling Older Adults in Wuhan, China. Int. J. Environ. Res. Public Health 2018, 15, 2705. [Google Scholar] [CrossRef] [PubMed]
- Rao, D.; Luo, X.; Tang, M.; Shen, Y.; Huang, R.; Yu, J.; Ren, J.; Cheng, X.; Lin, K. Prevalence of mild cognitive impairment and its subtypes in community-dwelling residents aged 65 years or older in Guangzhou, China. Arch. Gerontol. Geriatr. 2018, 75, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Pedraza, O.L.; Montes, A.M.S.; Sierra, F.A.; Montalvo, M.C.; Munoz, Y.; Diaz, J.M.; Lozano, A.; Pineros, C. Mild cognitive impairment (MCI) and dementia in a sample of adults in the city of Bogota. Dement. Neuropsychol. 2017, 11, 262–269. [Google Scholar] [CrossRef]
- Ren, L.; Zheng, Y.; Wu, L.; Gu, Y.; He, Y.; Jiang, B.; Zhang, J.; Zhang, L.; Li, J. Investigation of the prevalence of Cognitive Impairment and its risk factors within the elderly population in Shanghai, China. Sci. Rep. 2018, 8, 3575. [Google Scholar] [CrossRef]
- Han, R.; Tang, Z.; Ma, L. Related factors of cognitive impairment in community-dwelling older adults in Beijing Longitudinal Study of Aging. Aging Clin. Exp. Res. 2018. [CrossRef]
- Feng, L.; Nyunt, M.S.; Gao, Q.; Feng, L.; Lee, T.S.; Tsoi, T.; Chong, M.S.; Lim, W.S.; Collinson, S.; Yap, P.; et al. Physical Frailty, Cognitive Impairment, and the Risk of Neurocognitive Disorder in the Singapore Longitudinal Ageing Studies. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 369–375. [Google Scholar] [CrossRef]
- Tang, H.D.; Zhou, Y.; Gao, X.; Liang, L.; Hou, M.M.; Qiao, Y.; Ma, J.F.; Chen, S.D. Prevalence and Risk Factor of Cognitive Impairment were Different between Urban and Rural Population: A Community-Based Study. J. Alzheimers Dis. 2016, 49, 917–925. [Google Scholar] [CrossRef]
- Tzivian, L.; Dlugaj, M.; Winkler, A.; Weinmayr, G.; Hennig, F.; Fuks, K.B.; Vossoughi, M.; Schikowski, T.; Weimar, C.; Erbel, R.; et al. Long-Term Air Pollution and Traffic Noise Exposures and Mild Cognitive Impairment in Older Adults: A Cross-Sectional Analysis of the Heinz Nixdorf Recall Study. Environ. Health Perspect. 2016, 124, 1361–1368. [Google Scholar] [CrossRef]
- Vanoh, D.; Shahar, S.; Din, N.C.; Omar, A.; Vyrn, C.A.; Razali, R.; Ibrahim, R.; Hamid, T.A. Predictors of poor cognitive status among older Malaysian adults: Baseline findings from the LRGS TUA cohort study. Aging Clin. Exp. Res. 2017, 29, 173–182. [Google Scholar] [CrossRef]
- Nakamura, K.; Kitamura, K.; Watanabe, Y.; Shinoda, H.; Sato, H.; Someya, T. Rural-urban differences in the prevalence of cognitive impairment in independent community-dwelling elderly residents of Ojiya city, Niigata Prefecture, Japan. Environ. Health Prev. Med. 2016, 21, 422–429. [Google Scholar] [CrossRef]
- Ma, F.; Wu, T.; Zhao, J.; Ji, L.; Song, A.; Zhang, M.; Huang, G. Prevalence of Mild Cognitive Impairment and Its Subtypes among Chinese Older Adults: Role of Vascular Risk Factors. Dement. Geriatr. Cogn. Disord. 2016, 41, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Makizako, H.; Doi, T.; Tsutsumimoto, K.; Lee, S.; Suzuki, T. Cognitive Impairment and Disability in Older Japanese Adults. PLoS ONE 2016, 11, e0158720. [Google Scholar] [CrossRef] [PubMed]
- Lyu, J.; Kim, H.Y. Gender-Specific Incidence and Predictors of Cognitive Impairment among Older Koreans: Findings from a 6-Year Prospective Cohort Study. Psychiatry Investig. 2016, 13, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Giri, M.; Chen, T.; Yu, W.; Lu, Y. Prevalence and correlates of cognitive impairment and depression among elderly people in the world’s fastest growing city, Chongqing, People’s Republic of China. Clin. Interv. Aging 2016, 11, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; He, Y.; Jiang, B.; Wu, L.; Wang, J.; Yang, S.; Wang, Y. Association between metabolic syndrome and mild cognitive impairment and its age difference in a Chinese community elderly population. Clin. Endocrinol. (Oxf.) 2015, 82, 844–853. [Google Scholar] [CrossRef]
- Sun, Y.; Lee, H.J.; Yang, S.C.; Chen, T.F.; Lin, K.N.; Lin, C.C.; Wang, P.N.; Tang, L.Y.; Chiu, M.J. A nationwide survey of mild cognitive impairment and dementia, including very mild dementia, in Taiwan. PLoS ONE 2014, 9, e100303. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Xie, B.; Song, M.; Yu, L.; Wang, L.; An, C.; Zhu, Q.; Han, K.; Zhao, X.; Zhang, R.; et al. High prevalence of mild cognitive impairment in the elderly: A community-based study in four cities of the hebei province, china. Neuroepidemiology 2014, 42, 123–130. [Google Scholar] [CrossRef]
- Su, X.; Shang, L.; Xu, Q.; Li, N.; Chen, J.; Zhang, L.; Zhang, L.; Hua, Q. Prevalence and predictors of mild cognitive impairment in Xi’an: A community-based study among the elders. PLoS ONE 2014, 9, e83217. [Google Scholar] [CrossRef]
- Zhang, Y.; Shi, Z.; Liu, M.; Liu, S.; Yue, W.; Liu, S.; Xiang, L.; Lu, H.; Liu, P.; Wisniewski, T.; et al. Prevalence of cognitive impairment no dementia in a rural area of Northern China. Neuroepidemiology 2014, 42, 197–203. [Google Scholar] [CrossRef]
- Jia, J.; Zhou, A.; Wei, C.; Jia, X.; Wang, F.; Li, F.; Wu, X.; Mok, V.; Gauthier, S.; Tang, M.; et al. The prevalence of mild cognitive impairment and its etiological subtypes in elderly Chinese. Alzheimers Dement. 2014, 10, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Leggett, A.; Zarit, S.H.; Hoang, C.N.; Nguyen, H.T. Correlates of cognitive impairment in older Vietnamese. Aging Ment. Health 2013, 17, 915–923. [Google Scholar] [CrossRef]
- Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Ito, T.; Lee, S.; Park, H.; et al. Combined prevalence of frailty and mild cognitive impairment in a population of elderly Japanese people. J. Am. Med. Dir. Assoc. 2013, 14, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.P.; Chen, M.F.; Shen, B.H. A prevalence study on mild cognitive impairment among elderly populations in Zhejiang province. Zhonghua Liu Xing Bing Xue Za Zhi 2013, 34, 475–477. [Google Scholar] [PubMed]
- Rashid, A.K.; Azizah, A.M.; Rohana, S. Cognitive impairment among the elderly Malays living in rural Malaysia. Med. J. Malays. 2012, 67, 186–189. [Google Scholar]
- Lee, L.K.; Shahar, S.; Chin, A.V.; Mohd Yusoff, N.A.; Rajab, N.; Aziz, S.A. Prevalence of gender disparities and predictors affecting the occurrence of mild cognitive impairment (MCI). Arch. Gerontol. Geriatr. 2012, 54, 185–191. [Google Scholar] [CrossRef]
- Wada-Isoe, K.; Uemura, Y.; Nakashita, S.; Yamawaki, M.; Tanaka, K.; Yamamoto, M.; Shimokata, H.; Nakashima, K. Prevalence of Dementia and Mild Cognitive Impairment in the Rural Island Town of Ama-cho, Japan. Dement. Geriatr. Cogn. Dis Extra 2012, 2, 190–199. [Google Scholar] [CrossRef]
- Zhuang, J.P.; Wang, G.; Cheng, Q.; Wang, L.L.; Fang, R.; Liu, L.H.; Xiong, R.; Zhang, Y.; Gui, Y.X.; Kang, W.Y.; et al. Cognitive impairment and the associated risk factors among the elderly in the Shanghai urban area: A pilot study from China. Transl. Neurodegener. 2012, 1, 22. [Google Scholar] [CrossRef]
- Kim, K.W.; Park, J.H.; Kim, M.H.; Kim, M.D.; Kim, B.J.; Kim, S.K.; Kim, J.L.; Moon, S.W.; Bae, J.N.; Woo, J.I.; et al. A nationwide survey on the prevalence of dementia and mild cognitive impairment in South Korea. J. Alzheimers Dis. 2011, 23, 281–291. [Google Scholar] [CrossRef]
- Lu, J.; Li, D.; Li, F.; Zhou, A.; Wang, F.; Zuo, X.; Jia, X.F.; Song, H.; Jia, J. Montreal cognitive assessment in detecting cognitive impairment in Chinese elderly individuals: A population-based study. J. Geriatr. Psychiatry Neurol. 2011, 24, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.H.; Yeh, C.J.; Wang, C.C.; Liao, W.C.; Chen, S.C.; Chen, C.C.; Liang, J.; Lai, T.J.; Lin, H.S.; Lee, S.H.; et al. Determinants of cognitive impairment over time among the elderly in Taiwan: Results of the national longitudinal study. Arch. Gerontol. Geriatr. 2010, 50 (Suppl. 1), S53–S57. [Google Scholar] [CrossRef]
- Choo, I.H.; Lee, D.Y.; Lee, J.H.; Kim, K.W.; Jhoo, J.H.; Ju, Y.S.; Yoon, J.C.; Kim, S.G.; Ha, J.; Woo, J.I. The prevalence of cognitive impairment with no dementia in older people: The Seoul study. Int. J. Geriatr. Psychiatry 2009, 24, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Taboonpong, S.; Chailungka, P.; Aassanangkornchai, S. Factors related to cognitive status among elders in southern Thailand. Nurs. Health Sci. 2008, 10, 188–194. [Google Scholar] [CrossRef]
- Ogunniyi, A.; Adebiyi, A.O.; Adediran, A.B.; Olakehinde, O.O.; Siwoku, A.A. Prevalence estimates of major neurocognitive disorders in a rural Nigerian community. Brain Behav. 2016, 6, e00481. [Google Scholar] [CrossRef] [PubMed]
- Inzelberg, R.; Massarwa, M.; Schechtman, E.; Strugatsky, R.; Farrer, L.A.; Friedland, R.P. Estimating the risk for conversion from mild cognitive impairment to Alzheimer’s disease in an elderly Arab community. J. Alzheimers Dis. 2015, 45, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Anderson, T.M.; Sachdev, P.S.; Brodaty, H.; Trollor, J.N.; Andrews, G. Effects of sociodemographic and health variables on Mini-Mental State Exam scores in older Australians. Am. J. Geriatr. Psychiatry 2007, 15, 467–476. [Google Scholar] [CrossRef]
- Low, L.F.; Brodaty, H.; Edwards, R.; Kochan, N.; Draper, B.; Trollor, J.; Sachdev, P. The prevalence of “cognitive impairment no dementia” in community-dwelling elderly: A pilot study. Aust. N. Z. J. Psychiatry 2004, 38, 725–731. [Google Scholar] [CrossRef]
- Luck, T.; Luppa, M.; Briel, S.; Riedel-Heller, S.G. Incidence of mild cognitive impairment: A systematic review. Dement. Geriatr. Cogn. Disord. 2010, 29, 164–175. [Google Scholar] [CrossRef]
- Luck, T.; Luppa, M.; Briel, S.; Matschinger, H.; Konig, H.H.; Bleich, S.; Villringer, A.; Angermeyer, M.C.; Riedel-Heller, S.G. Mild cognitive impairment: Incidence and risk factors: Results of the leipzig longitudinal study of the aged. J. Am. Geriatr. Soc. 2010, 58, 1903–1910. [Google Scholar] [CrossRef]
- Alhurani, R.E.; Vassilaki, M.; Aakre, J.A.; Mielke, M.M.; Kremers, W.K.; Machulda, M.M.; Geda, Y.E.; Knopman, D.S.; Peterson, R.C.; Roberts, R.O. Decline in Weight and Incident Mild Cognitive Impairment: Mayo Clinic Study of Aging. JAMA Neurol. 2016, 73, 439–446. [Google Scholar] [CrossRef]
- Plassman, B.L.; Langa, K.M.; McCammon, R.J.; Fisher, G.G.; Potter, G.G.; Burke, J.R.; Steffens, D.C.; Foster, N.L.; Giordani, B.; Unverzagt, F.W.; et al. Incidence of dementia and cognitive impairment, not dementia in the United States. Ann. Neurol. 2011, 70, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Leurgans, S.E.; Bennett, D.A. Physical frailty is associated with incident mild cognitive impairment in community-based older persons. J. Am. Geriatr. Soc. 2010, 58, 248–255. [Google Scholar] [CrossRef]
- Potvin, O.; Forget, H.; Grenier, S.; Preville, M.; Hudon, C. Anxiety, depression, and 1-year incident cognitive impairment in community-dwelling older adults. J. Am. Geriatr. Soc. 2011, 59, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Satya-Murti, S.; Lockhart, J. Recognizing and reducing cognitive bias in clinical and forensic neurology. Neurol. Clin. Pract. 2015, 5, 389–396. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Number of Papers | With Cognitive Impairment Median (25–75 Percentile) | p Value | |
|---|---|---|---|
| Inclusion Age | |||
| 50–59 | 15 | 12.0 (9.60–17.65) | 0.062 |
| 60–69 | 57 | 20.10 (14.20–24.70) | |
| ≥70 | 9 | 19.0 (15.0–29.90) | |
| Participants Number | |||
| <1001 | 26 | 22.75 (14.90–31.40) | 0.386 |
| 1001–2500 | 22 | 15.95 (11.60–28.50) | |
| 2501–5000 | 18 | 13.75 (9.60–21.30) | |
| >5000 | 14 | 20.24 (18.80–24.10) | |
| Diagnostic Method | |||
| Neurologist evaluation | 9 | 15.40 (11.30–23.40) | 0.737 |
| Neurological tests | 62 | 18.90 (12.20–24.70) | |
| Neurologist evaluation and tests | 8 | 21.30 (12.0–28.90) | |
| Region | |||
| Europe | 25 | 12.10 (9.94–23.90) | 0.110 |
| North America | 13 | 20.10 (19.0–24.70) | |
| South America | 3 | 34.0 (29.15–35.75) | |
| Asia | 35 | 19.44 (13.25–25.55) | |
| Africa | 2 | 25.70 (18.40–33.0) | |
| Australia | 2 | 20.50 (7.70–33.30) | |
| Studies | With Cognitive Impairment Median (25–75 Percentile) | p Value | |
|---|---|---|---|
| Inclusion Age | |||
| 50–59 | 3 | 30.70 (26.35–36.24) | 0.035 * |
| 60–69 | 4 | 71.11 (58.44–145.98) | |
| ≥70 | 4 | 58.45 (51.84–68.45) | |
| Participants Number | |||
| <1001 | 2 | 51.09 (41.77–60.40) | 0.693 |
| 1001–2500 | 5 | 56.50 (41.19–76.50) | |
| 2501–5000 | 3 | 51.45 (41.08–58.44) | |
| >5000 | 1 | 215 | |
| Diagnostic Method | |||
| Neurologist evaluation | 3 | 76.50 (59.14–145.75) | 0.737 |
| Neurological tests | 5 | 51.45 (30.70–60.40) | |
| Neurologist evaluation and tests | 3 | 56.50 (51.82–60.96) | |
| Region | |||
| Europe | 5 | 56.50 (51.45–76.50) | 0.285 |
| North America | 5 | 60.40 (47.19–65.42) | |
| Asia | 1 | 22 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pais, R.; Ruano, L.; P. Carvalho, O.; Barros, H. Global Cognitive Impairment Prevalence and Incidence in Community Dwelling Older Adults—A Systematic Review. Geriatrics 2020, 5, 84. https://doi.org/10.3390/geriatrics5040084
Pais R, Ruano L, P. Carvalho O, Barros H. Global Cognitive Impairment Prevalence and Incidence in Community Dwelling Older Adults—A Systematic Review. Geriatrics. 2020; 5(4):84. https://doi.org/10.3390/geriatrics5040084
Chicago/Turabian StylePais, Ricardo, Luís Ruano, Ofélia P. Carvalho, and Henrique Barros. 2020. "Global Cognitive Impairment Prevalence and Incidence in Community Dwelling Older Adults—A Systematic Review" Geriatrics 5, no. 4: 84. https://doi.org/10.3390/geriatrics5040084
APA StylePais, R., Ruano, L., P. Carvalho, O., & Barros, H. (2020). Global Cognitive Impairment Prevalence and Incidence in Community Dwelling Older Adults—A Systematic Review. Geriatrics, 5(4), 84. https://doi.org/10.3390/geriatrics5040084