Multi-Morbidity and Polypharmacy in Older People: Challenges and Opportunities for Clinical Practice


Abstract
1. Introduction
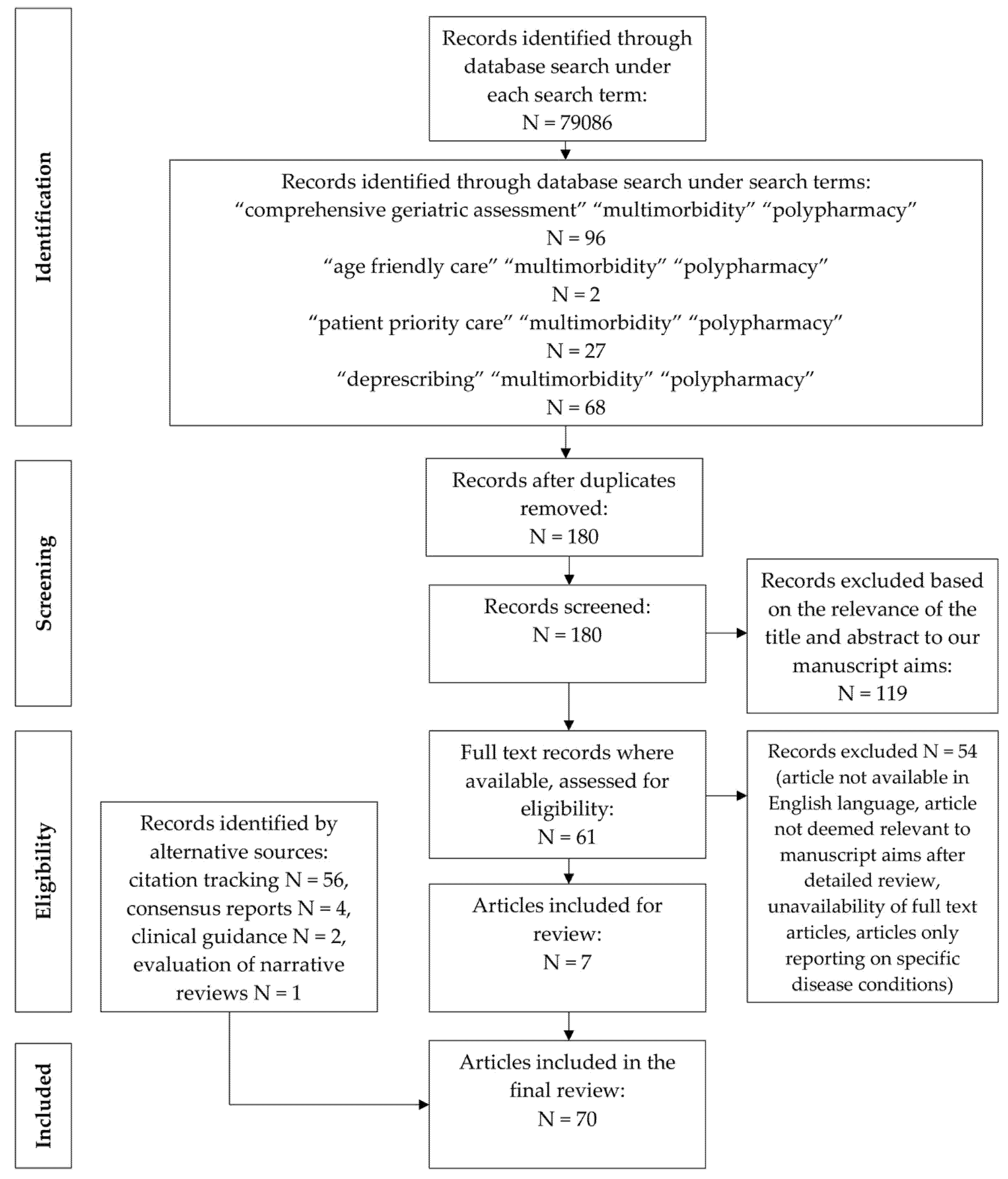
2. Methods
2.1. Multi-Morbidity
2.2. Multi-Morbidity and Frailty
2.3. Polypharmacy
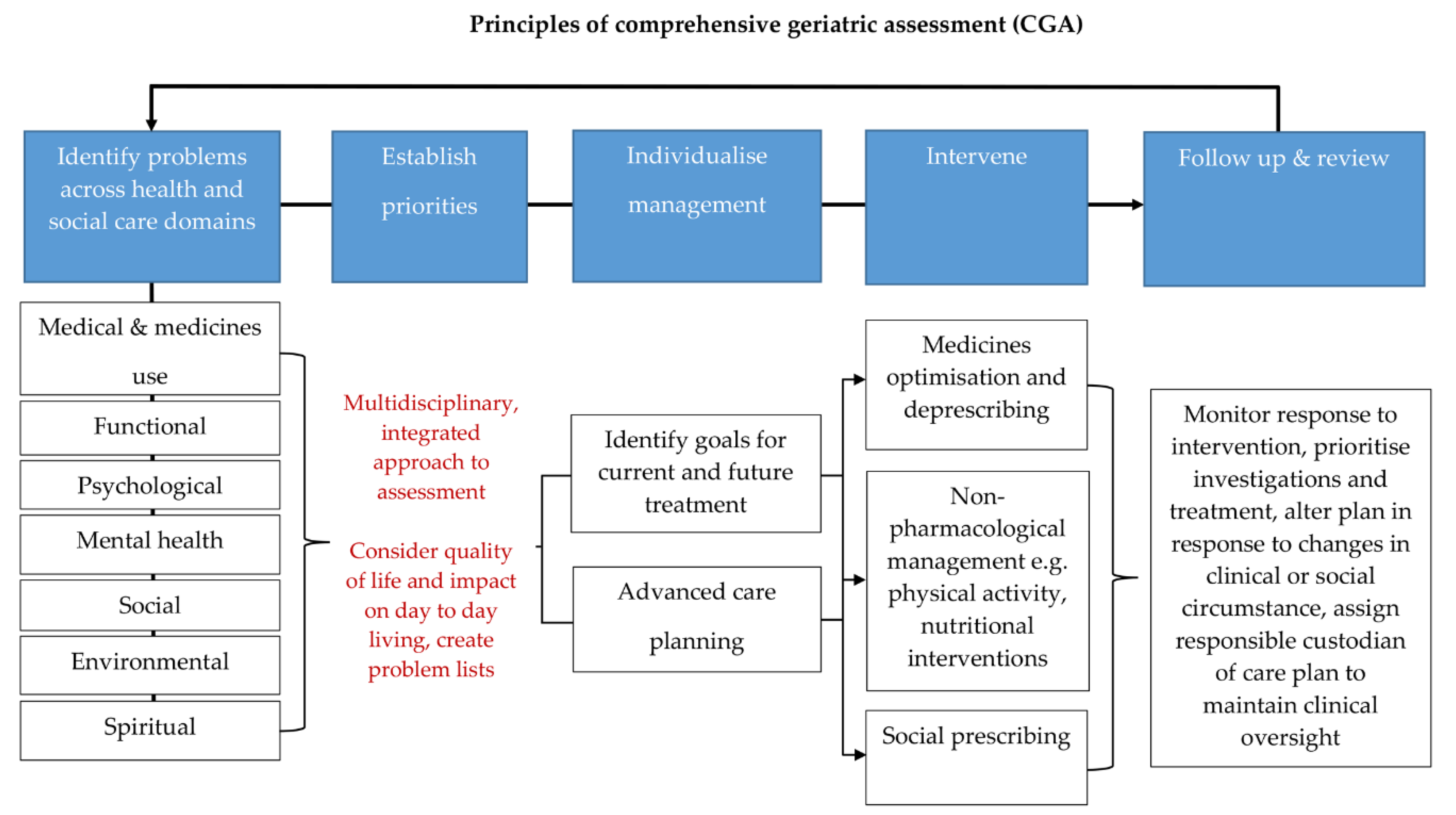
2.4. Management of Multi-Morbidity and Polypharmacy
3. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
| 1 | Justification of the article’s importance for the readership | ||
| The importance is not justified | 0 | ||
| The importance is alluded to, but not explicitly justified | 1 | ||
| The importance is explicitly justified | 2 | X | |
| 2 | Statement of concrete aims or formulation of questions | ||
| No aims of questions are formulated | 0 | ||
| Aims are formulated generally but not concretely or in terms of clear questions | 1 | ||
| One or more concrete aims or questions are formulated | 2 | X | |
| 3 | Description of literature search | ||
| The search strategy is not presented | 0 | ||
| The literature search is described briefly | 1 | X | |
| The literature search is described in detail, including search terms and inclusion criteria | 2 | ||
| 4 | Referencing | ||
| Key statements are not supported by references | 0 | ||
| The referencing of key statements is inconsistent | 1 | ||
| Key statements are supported by references | 2 | X | |
| 5 | Scientific reasoning (e.g., incorporation of appropriate evidence, such as RCTs in clinical medicine | ||
| The article’s point is not based on appropriate arguments | 0 | ||
| Appropriate evidence is introduced selectively | 1 | ||
| Appropriate evidence is generally present | 2 | X | |
| 6 | Appropriate presentation of data (e.g., absolute vs. relative risk; effect sizes without confidence intervals) | ||
| Data are presented inadequately | 0 | ||
| Data are often presented in the most appropriate way | 1 | X | |
| Relevant outcome data are generally presented appropriately | 2 | ||
| Sum score | 10 | ||
References
- Chatterji, S.; Byles, J.; Cutler, D.; Seeman, T.; Verdes, E. Health, functioning, and disability in older adults--present status and future implications. Lancet 2015, 385, 563–575. [Google Scholar]
- United Nations, Department of Economic and Social Affairs, Population Division World Population Ageing 2015 (ST/ESA/SER.A/390). 2015. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2015_Report.pdf (accessed on 27 October 2020).
- Willcox, D.C.; Willcox, B.J.; Poon, L.W. Centenarian studies: Important contributors to our understanding of the aging process and longevity. Curr. Gerontol. Geriatr. Res. 2010, 2010. [Google Scholar] [CrossRef]
- Fabbri, E.; An, Y.; Zoli, M.; Simonsick, E.M.; Guralnik, J.M.; Bandinelli, S. Aging and the burden of multimorbidity: Associations with inflammatory and anabolic hormonal biomarkers. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 70, 63–70. [Google Scholar] [CrossRef]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA-a scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- The National Institute for Health and Care Excellence (NICE): Multimorbidity: Clinical Assessment and Management. 2016. Available online: https://www.nice.org.uk/guidance/ng56 (accessed on 27 October 2020).
- Aiden, H. Multimorbidity: Understanding the Challenge. 2018. Available online: www.richmondgroupofcharitiesorguk (accessed on 27 October 2020).
- Fortin, M.; Lapointe, L.; Hudon, C.; Vanasse, A.; Ntetu, A.L.; Maltais, D. Multimorbidity and quality of life in primary care: A systematic review. Health Qual. Life Outcomes 2004, 2, 51. [Google Scholar] [CrossRef] [PubMed]
- Payne, R.A.; Abel, G.A.; Guthrie, B.; Mercer, S.W. The effect of physical multimorbidity, mental health conditions and socioeconomic deprivation on unplanned admissions to hospital: A retrospective cohort study. Cmaj 2013, 185, E221–E228. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Larrañaga, A.; Poblador-Plou, B.; González-Rubio, F.; Gimeno-Feliu, L.A.; Abad-Díez, J.M.; Prados-Torres, A. Multimorbidity, polypharmacy, referrals, and adverse drug events: Are we doing things well? Br. J. Gen. Pract. 2012, 62, e821–e826. [Google Scholar] [CrossRef]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Nunes, B.P.; Flores, T.R.; Mielke, G.I.; Thume, E.; Facchini, L.A. Multimorbidity and mortality in older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2016, 67, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef]
- Garin, N.; Koyanagi, A.; Chatterji, S.; Tyrovolas, S.; Olaya, B.; Leonardi, M. Global Multimorbidity Patterns: A Cross-Sectional, Population-Based, Multi-Country Study. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2015, 71, 205–214. [Google Scholar] [CrossRef]
- Afshar, S.; Roderick, P.J.; Kowal, P.; Dimitrov, B.D.; Hill, A.G. Multimorbidity and the inequalities of global ageing: A cross-sectional study of 28 countries using the World Health Surveys. BMC Public Health 2015, 15, 776. [Google Scholar] [CrossRef] [PubMed]
- Prados-Torres, A.; Poblador-Plou, B.; Calderón-Larrañaga, A.; Gimeno-Feliu, L.A.; González-Rubio, F.; Poncel-Falcó, A. Multimorbidity patterns in primary care: Interactions among chronic diseases using factor analysis. PLoS ONE 2012, 7, e32190. [Google Scholar] [CrossRef]
- Zimmet, P.; Alberti, K.; Shaw, J. International Diabetes Federation: The IDF consensus worldwide definition of the metabolic syndrome. Diabetes Voice 2005, 50, 31–33. [Google Scholar]
- Sattar, N.; Gaw, A.; Scherbakova, O.; Ford, I.; O’Reilly, D.S.J.; Haffner, S.M. Metabolic syndrome with and without C-reactive protein as a predictor of coronary heart disease and diabetes in the West of Scotland Coronary Prevention Study. Circulation 2003, 108, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Hu, G.; Qiao, Q.; Tuomilehto, J.; Balkau, B.; Borch-Johnsen, K.; Pyorala, K. Prevalence of the metabolic syndrome and its relation to all-cause and cardiovascular mortality in nondiabetic European men and women. Arch. Intern. Med. 2004, 164, 1066–1076. [Google Scholar] [CrossRef]
- Schubert, C.C.; Boustani, M.; Callahan, C.M.; Perkins, A.J.; Carney, C.P.; Fox, C. Comorbidity profile of dementia patients in primary care: Are they sicker? J. Am. Geriatr. Soc. 2006, 54, 104–109. [Google Scholar] [CrossRef]
- Chamberlain, A.M.; Rutten, L.J.F.; Jacobson, D.J.; Fan, C.; Wilson, P.M.; Rocca, W.A. Multimorbidity, functional limitations, and outcomes: Interactions in a population-based cohort of older adults. J. Comorb. 2019, 9. [Google Scholar] [CrossRef]
- Guthrie, B.; Payne, K.; Alderson, P.; McMurdo, M.E.; Mercer, S.W. Adapting clinical guidelines to take account of multimorbidity. BMJ 2012, 345, e6341. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Esterson, J.; Ferris, R.; Posner, P.; Blaum, C.S. Patient Priority-Directed Decision Making and Care for Older Adults with Multiple Chronic Conditions. Clin. Geriatr. Med. 2016, 32, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Masoudi, F.A.; Havranek, E.P.; Wolfe, P.; Gross, C.P.; Rathore, S.S.; Steiner, J.F. Most hospitalized older persons do not meet the enrollment criteria for clinical trials in heart failure. Am. Heart J. 2003, 146, 250–257. [Google Scholar] [CrossRef]
- Travers, J.; Marsh, S.; Caldwell, B.; Williams, M.; Aldington, S.; Weatherall, M. External validity of randomized controlled trials in COPD. Respir. Med. 2007, 101, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- Saunders, C.; Byrne, C.D.; Guthrie, B.; Lindsay, R.; McKnight, J.; Philip, S. External validity of randomized controlled trials of glycaemic control and vascular disease: How representative are participants? Diabetic Med. 2013, 30, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Boyd, C.M.; Vollenweider, D.; Puhan, M.A. Informing evidence-based decision-making for patients with comorbidity: Availability of necessary information in clinical trials for chronic diseases. PLoS ONE 2012, 7, e41601. [Google Scholar] [CrossRef]
- Jadad, A.R.; To, M.J.; Emara, M.; Jones, J. Consideration of multiple chronic diseases in randomized controlled trials. JAMA 2011, 306, 2670–2672. [Google Scholar] [CrossRef] [PubMed]
- Kuchel, G.A. Inclusion of Older Adults in Research: Ensuring Relevance, Feasibility, and Rigor. J. Am. Geriatr. Soc. 2019, 67, 203–204. [Google Scholar] [CrossRef]
- Hughes, L.D.; McMurdo, M.E.; Guthrie, B. Guidelines for people not for diseases: The challenges of applying UK clinical guidelines to people with multimorbidity. Age Ageing 2013, 42, 62–69. [Google Scholar] [CrossRef]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R. Frailty and multimorbidity: A systematic review and meta-analysis. J. Gerontol. Ser. A 2019, 74, 659–666. [Google Scholar] [CrossRef]
- Duerden, M.A.T.; Payne, R. Polypharmacy and Medicines Optimisation: Making it Safe and Sound; The King’s Fund: London, UK, 2013. [Google Scholar]
- Lavan, A.H.; Gallagher, P.F.; O’Mahony, D. Methods to reduce prescribing errors in elderly patients with multimorbidity. Clin. Interv. Aging 2016, 11, 857–866. [Google Scholar]
- Payne, R.A.; Avery, A.J.; Duerden, M.; Saunders, C.L.; Simpson, C.R.; Abel, G.A. Prevalence of polypharmacy in a Scottish primary care population. Eur. J. Clin. Pharmacol. 2014, 70, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Betteridge, T.; Frampton, C.; Jardine, D. Polypharmacy–we make it worse! A cross-sectional study from an acute admissions unit. Intern. Med. J. 2012, 42, 208–211. [Google Scholar] [CrossRef]
- Viktil, K.K.; Blix, H.S.; Eek, A.K.; Davies, M.N.; Moger, T.A.; Reikvam, A. How are drug regimen changes during hospitalisation handled after discharge: A cohort study. BMJ Open 2012, 2, e001461. [Google Scholar] [CrossRef] [PubMed]
- The National Institute for Health and Care Excellence (NICE): Multimorbidity and polypharmacy. 2019. Available online: www.nice.org.uk/guidance/ktt18 (accessed on 27 October 2020).
- Routledge, P.A.; O’Mahony, M.S.; Woodhouse, K.W. Adverse drug reactions in elderly patients. Br. J. Clin. Pharm. 2004, 57, 121–126. [Google Scholar] [CrossRef]
- Pirmohamed, M.; James, S.; Meakin, S.; Green, C.; Scott, A.K.; Walley, T.J. Adverse drug reactions as cause of admission to hospital: Prospective analysis of 18 820 patients. BMJ 2004, 329, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Davies, E.C.; Green, C.F.; Taylor, S.; Williamson, P.R.; Mottram, D.R.; Pirmohamed, M. Adverse drug reactions in hospital in-patients: A prospective analysis of 3695 patient-episodes. PLoS ONE 2009, 4, e4439. [Google Scholar] [CrossRef]
- Farmer, C.; Fenu, E.; O’Flynn, N.; Guthrie, B. Clinical assessment and management of multimorbidity: Summary of NICE guidance. BMJ 2016, 354, i4843. [Google Scholar] [CrossRef]
- Muth, C.; Blom, J.W.; Smith, S.M.; Johnell, K.; Gonzalez-Gonzalez, A.I.; Nguyen, T.S. Evidence supporting the best clinical management of patients with multimorbidity and polypharmacy: A systematic guideline review and expert consensus. J. Intern. Med. 2019, 285, 272–288. [Google Scholar] [CrossRef]
- Yarnall, A.J.; Sayer, A.A.; Clegg, A.; Rockwood, K.; Parker, S.; Hindle, J.V. New horizons in multimorbidity in older adults. Age Ageing 2017, 46, 882–888. [Google Scholar] [CrossRef]
- Cullinan, S.; Raae, H.C.; Byrne, S.; O’Mahony, D.; Kearney, P.; Sahm, L. Challenges of deprescribing in the multimorbid patient. Eur. J. Hosp. Pharm. 2017, 24, 43–46. [Google Scholar] [CrossRef]
- Fulmer, T.; Mate, K.S.; Berman, A. The Age-Friendly Health System Imperative. J. Am. Geriatr. Soc. 2018, 66, 22–24. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.; Dindo, L.; Smith, C.D.; Blaum, C.; Costello, D.; Ouellet, G. Challenges and strategies in patients’ health priorities-aligned decision-making for older adults with multiple chronic conditions. PLoS ONE 2019, 14, e0218249. [Google Scholar] [CrossRef] [PubMed]
- Newell, S.; Jordan, Z. The patient experience of patient-centered communication with nurses in the hospital setting: A qualitative systematic review protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 76–87. [Google Scholar] [CrossRef]
- Hanlon, J.T.; Schmader, K.E. The medication appropriateness index at 20: Where it started, where it has been, and where it may be going. Drugs Aging 2013, 30, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Lewis, T. Using the NO TEARS tool for medication review. BMJ 2004, 329, 434. [Google Scholar] [CrossRef]
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2015, 44, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Avery, A.J.; Rodgers, S.; Cantrill, J.A.; Armstrong, S.; Cresswell, K.; Eden, M. A pharmacist-led information technology intervention for medication errors (PINCER): A multicentre, cluster randomised, controlled trial and cost-effectiveness analysis. Lancet 2012, 379, 1310–1319. [Google Scholar] [CrossRef]
- Thompson, W.; Farrell, B. Deprescribing: What is it and what does the evidence tell us? Can. J. Hosp. Pharm. 2013, 6, 201–202. [Google Scholar] [CrossRef]
- Sergi, G.; De, R.M.; Sarti, S.; Manzato, E. Polypharmacy in the elderly: Can comprehensive geriatric assessment reduce inappropriate medication use? Drugs Aging 2011, 28, 509–518. [Google Scholar] [CrossRef]
- O’Mahony, M.S.; Parbhoo, A. Deprescribing in older people. Br. J. Hosp. Med. (Lond.) 2020, 81, 1–9. [Google Scholar] [CrossRef]
- Rudolph, J.L.; Salow, M.J.; Angelini, M.C.; McGlinchey, R.E. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch. Intern. Med. 2008, 168, 508–513. [Google Scholar] [CrossRef]
- Woodford, H.J.; Fisher, J. New horizons in deprescribing for older people. Age Ageing 2019, 48, 768–775. [Google Scholar] [CrossRef]
- Ouellet, G.M.; Ouellet, J.A.; Tinetti, M.E. Principle of rational prescribing and deprescribing in older adults with multiple chronic conditions. Ther. Adv. Drug Saf. 2018, 9, 639–652. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.; Freeman, C.; Foster, M.; Scott, I. GP-Led Deprescribing in Community-Living Older Australians: An Exploratory Controlled Trial. J. Am. Geriatr. Soc. 2020, 68, 403–410. [Google Scholar] [CrossRef]
- Garfinkel, D. Poly-de-prescribing to treat polypharmacy: Efficacy and safety. Ther. Adv. Drug Saf. 2018, 9, 25–43. [Google Scholar] [CrossRef]
- Potter, K.; Flicker, L.; Page, A.; Etherton-Beer, C. Deprescribing in Frail Older People: A Randomised Controlled Trial. PLoS ONE 2016, 11, e0149984. [Google Scholar] [CrossRef]
- Bezreh, T.; Laws, M.B.; Taubin, T.; Rifkin, D.E.; Wilson, I.B. Challenges to physician-patient communication about medication use: A window into the skeptical patient’s world. Patient Prefer. Adher. 2012, 6, 11–18. [Google Scholar]
- Farrell, B.; Mangin, D. Deprescribing Is an Essential Part of Good Prescribing. Am. Fam. Phys. 2019, 99, 7–9. [Google Scholar]
- Damarell, R.A.; Morgan, D.D.; Tieman, J.J. General practitioner strategies for managing patients with multimorbidity: A systematic review and thematic synthesis of qualitative research. Bmc Fam. Pract. 2020, 21, 131. [Google Scholar] [CrossRef] [PubMed]
- Fraser, A.; Ross, S.; Aggarwal, P. Walk in another’s shoes: GP-consultant exchange schemes. BMJ 2018, 363, 2. [Google Scholar]
- Vermunt, N.; Elwyn, G.; Westert, G.; Harmsen, M.; Olde, R.M.; Meinders, M. Goal setting is insufficiently recognised as an essential part of shared decision-making in the complex care of older patients: A framework analysis. BMC Fam. Pract. 2019, 20, 76. [Google Scholar] [CrossRef] [PubMed]
- Lea, S.C.; Watts, K.L.; Davis, N.A.; Panayiotou, B.; Bankart, M.J.; Arora, A. The potential clinical benefits of medicines optimisation through comprehensive geriatric assessment, carried out by secondary care geriatricians, in a general practice care setting in North Staffordshire, UK: A feasibility study. BMJ Open 2017, 7, e015278. [Google Scholar] [CrossRef] [PubMed]
- Laursen, J.; Kornholt, J.; Betzer, C.; Petersen, T.S.; Christensen, M.B. General Practitioners’ Barriers toward Medication Reviews in Polymedicated Multimorbid Patients: How can a Focus on the Pharmacotherapy in an Outpatient Clinic Support GPs? Health Serv. Res. Manag. Epidemiol. 2018, 5. [Google Scholar] [CrossRef]
- Ellis, G.; Sevdalis, N. Understanding and improving multidisciplinary team working in geriatric medicine. Age Ageing 2019, 48, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Woolford, S.J.; Sohan, O.; Dennison, E.M.; Cooper, C.; Patel, H.P. Approaches to the diagnosis and prevention of frailty. Aging Clin. Exp. Res. 2020, 32, 1629–1637. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aggarwal, P.; Woolford, S.J.; Patel, H.P. Multi-Morbidity and Polypharmacy in Older People: Challenges and Opportunities for Clinical Practice. Geriatrics 2020, 5, 85. https://doi.org/10.3390/geriatrics5040085
Aggarwal P, Woolford SJ, Patel HP. Multi-Morbidity and Polypharmacy in Older People: Challenges and Opportunities for Clinical Practice. Geriatrics. 2020; 5(4):85. https://doi.org/10.3390/geriatrics5040085
Chicago/Turabian StyleAggarwal, Pritti, Stephen J. Woolford, and Harnish P. Patel. 2020. "Multi-Morbidity and Polypharmacy in Older People: Challenges and Opportunities for Clinical Practice" Geriatrics 5, no. 4: 85. https://doi.org/10.3390/geriatrics5040085
APA StyleAggarwal, P., Woolford, S. J., & Patel, H. P. (2020). Multi-Morbidity and Polypharmacy in Older People: Challenges and Opportunities for Clinical Practice. Geriatrics, 5(4), 85. https://doi.org/10.3390/geriatrics5040085