
Food Myths or Food Facts? Study about Perceptions and Knowledge in a Portuguese Sample


Abstract
:1. Introduction
2. Materials and Methods
2.1. Instrument and Data Collection
2.2. Data Analysis
3. Results
3.1. Sample Characterization
3.2. Lifestyle and Anthropometric Data
3.3. Perceptions Regarding Food Myths and Facts
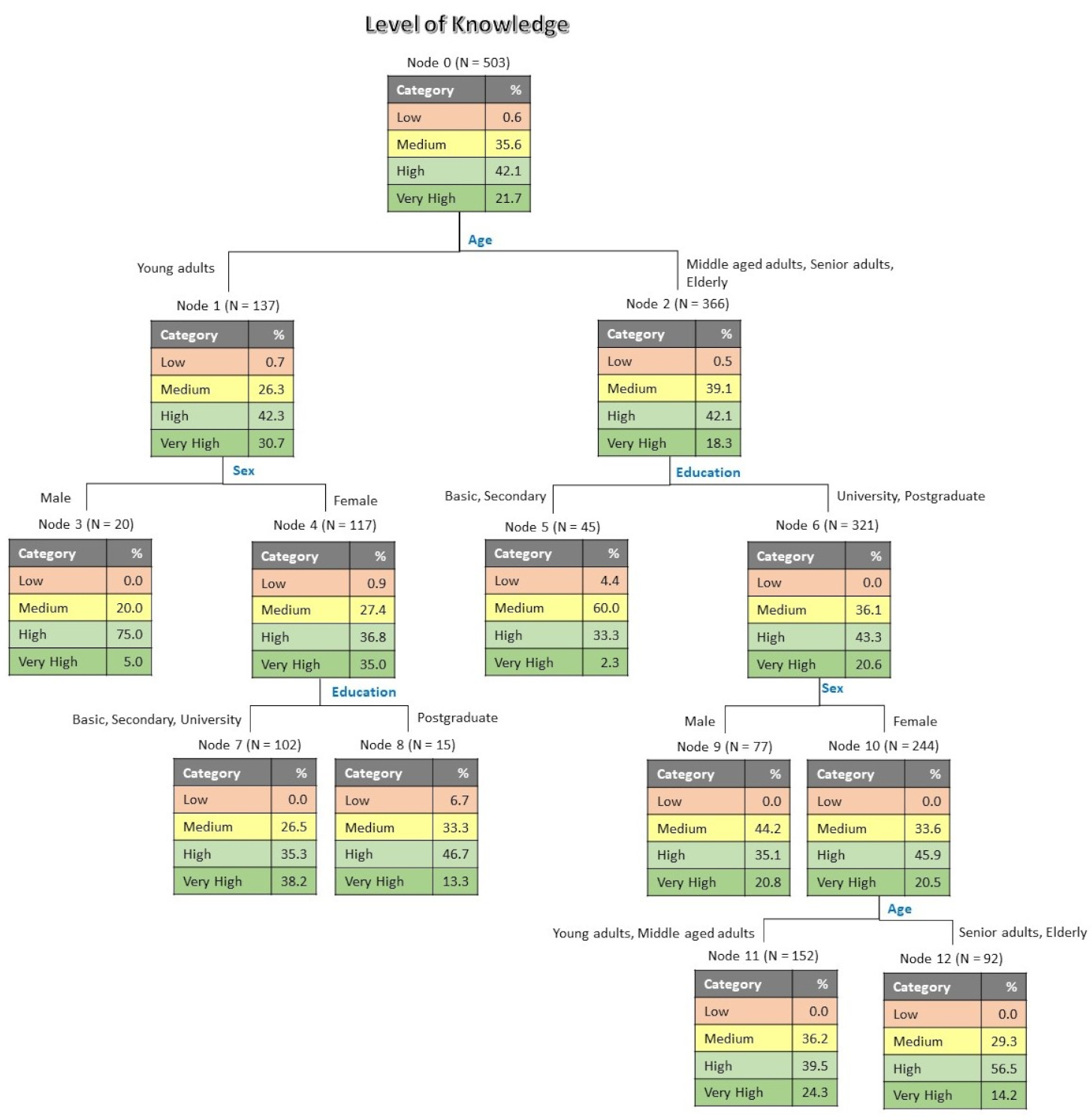
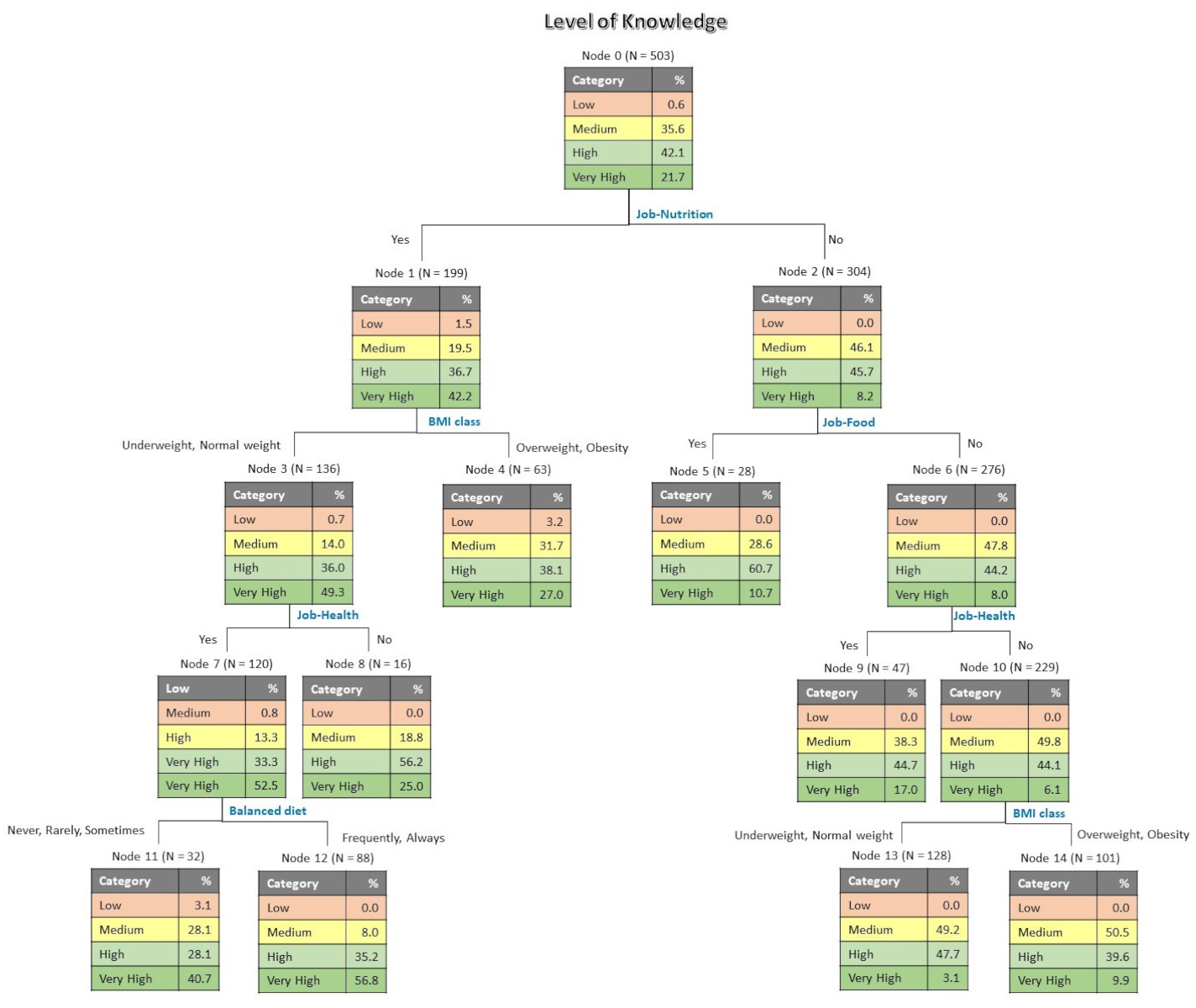
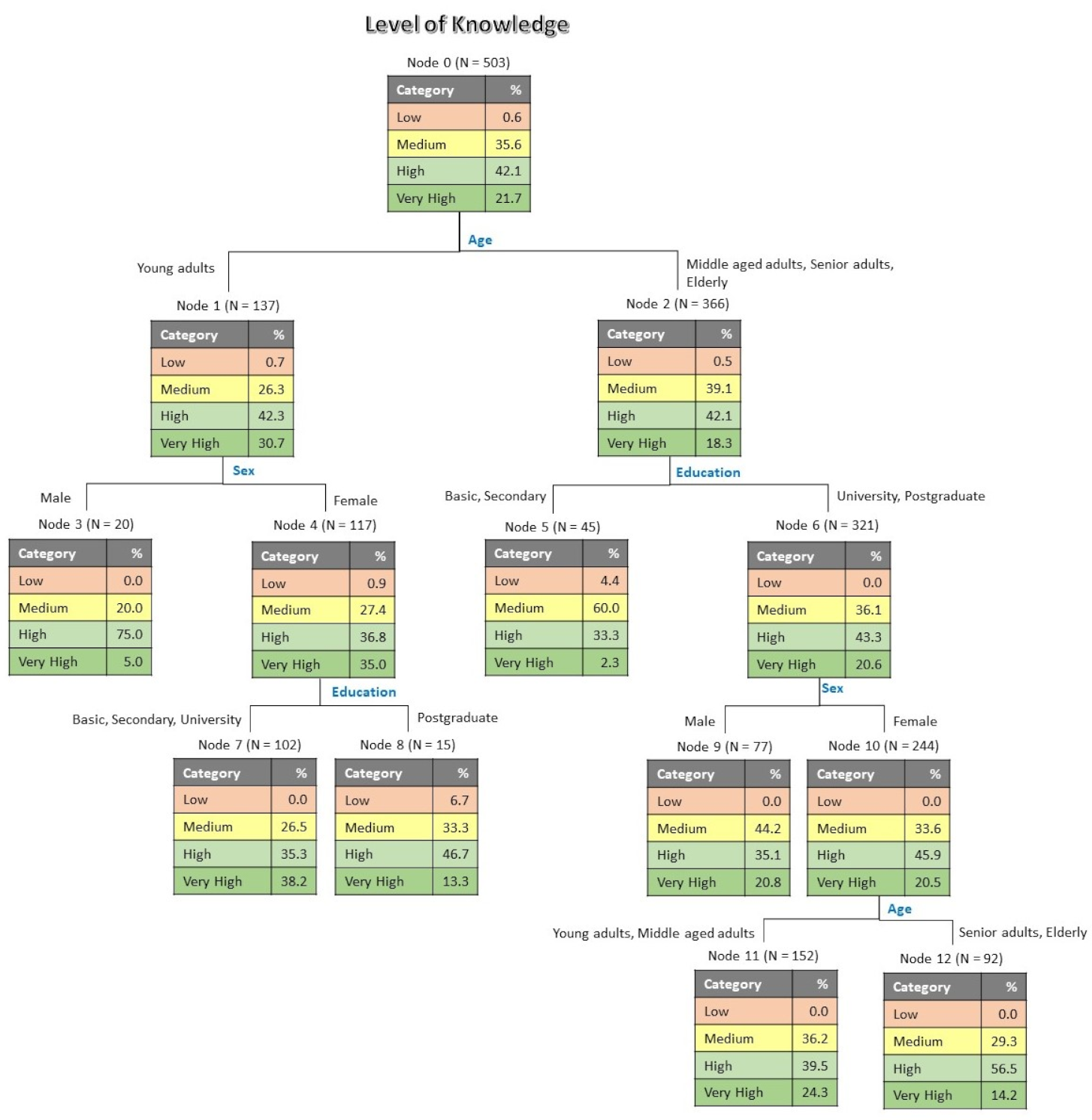
3.4. Level of Knowledge
3.5. Sources of Information
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Code | Item | Age | Sex | Education | Environment | Marital | Nutrition | Food | Sport | Health | Bal. Diet | BMI Class |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| S1 | Drink water at meals | 0.286 ** | 0.037 | 0.049 | −0.039 | 0.172 ** | 0.286 ** | 0.281 ** | 0.045 | 0.183 ** | −0.106 * | 0.113 * |
| S2 | Beginning of digestion | 0.033 | −0.002 | 0.089 * | 0.032 | −0.028 | −0.202 ** | −0.158 ** | −0.024 | −0.167 ** | 0.130 ** | 0.001 |
| S3 | Fruit before meals | 0.361 ** | −0.013 | 0.083 | 0.038 | 0.259 ** | 0.307 ** | 0.186 ** | 0.046 | 0.113 * | −0.042 | 0.134 ** |
| S4 | Eggs and cholesterol | 0.041 | 0.089 * | −0.035 | 0.143 ** | 0.042 | 0.095 | 0.064 | −0.084 | 0.018 | −0.128 ** | −0.060 |
| S5 | Milk is bad for health | 0.143 ** | 0.044 | −0.083 | 0.012 | 0.104 * | 0.282 ** | 0.326 ** | −0.026 | 0.214 ** | −0.046 | 0.101 * |
| S6 | Carbohydrates at night and weight | 0.309 ** | −0.002 | 0.061 | 0.011 | 0.266 ** | 0.464 ** | 0.299 ** | 0.087 | 0.296 ** | −0.144 ** | 0.158 ** |
| S7 | Importance of fat | −0.195 ** | −0.042 | 0.049 | 0.043 | −0.174 ** | −0.369 ** | −0.331 ** | −0.075 | −0.225 ** | 0.132 ** | −0.117 ** |
| S8 | Fruit after meals | −0.138 ** | 0.130 ** | 0.008 | 0.047 | −0.141 ** | −0.008 | −0.042 | −0.011 | 0.053 | −0.012 | −0.024 |
| S9 | Fiber and bowel function. | 0.164 ** | −0.069 | 0.108 * | −0.006 | 0.103 * | −0.226 ** | −0.188 ** | −0.043 | −0.114 * | 0.136 ** | 0.008 |
| S10 | Gluten-free foods are better for all | 0.148 ** | 0.099 * | −0.073 | 0.002 | 0.107 * | 0.275 ** | 0.203 ** | −0.052 | 0.177 ** | −0.086 | 0.133 ** |
| S11 | Cheese is bad for memory | −0.071 | 0.011 | −0.086 | 0.007 | −0.049 | 0.040 | 0.015 | −0.028 | 0.112 * | 0.006 | −0.001 |
| S12 | Coconut oil versus olive oil | −0.066 | 0.072 | −0.023 | −0.091 * | −0.001 | 0.306 ** | 0.261 ** | 0.033 | 0.182 ** | −0.117 ** | 0.084 |
| S13 | Lactose-free foods are better for all | 0.120 ** | 0.059 | −0.144 ** | −0.029 | 0.070 | 0.363 ** | 0.331 ** | −0.007 | 0.279 ** | −0.056 | 0.098 * |
| S14 | Children’s nutritional needs | −0.066 | −0.109 * | −0.007 | 0.001 | −0.045 | −0.147 ** | −0.118 * | −0.004 | −0.103 * | 0.026 | 0.004 |
| S15 | Fruits/vegetables and weight gain | 0.061 | 0.052 | −0.090 * | −0.017 | 0.014 | 0.133 ** | 0.058 | 0.041 | 0.085 | −0.071 | 0.107 * |
| S16 | Sweet potatoes have less calories | 0.180 ** | 0.042 | 0.060 | 0.008 | 0.149 ** | 0.376 ** | 0.295 ** | 0.119 * | 0.220 ** | −0.128 ** | 0.039 |
| S17 | Diet and blood group | 0.070 | 0.072 | 0.023 | −0.030 | 0.049 | 0.335 ** | 0.234 ** | 0.038 | 0.282 ** | −0.101* | 0.110 * |
| S18 | Balanced varied diet and diseases | 0.047 | −0.130 ** | 0.102 * | 0.028 | 0.061 | −0.133 ** | −0.099 * | 0.107 * | −0.026 | 0.096 * | −0.009 |
| S19 | Alkaline diet and blood acidity | 0.211 ** | 0.129 ** | −0.043 | −0.014 | 0.175 ** | 0.410 ** | 0.321 ** | 0.028 | 0.258 ** | −0.058 | 0.145 ** |
| S20 | Water with lemon and weight loss | 0.238 ** | 0.051 | −0.030 | 0.019 | 0.218 ** | 0.396 ** | 0.313 ** | 0.030 | 0.247 ** | −0.149 ** | 0.201 ** |
| S21 | Eating habits and risk of disease | 0.160 ** | −0.064 | 0.026 | −0.037 | 0.132 ** | −0.079 | −0.056 | −0.096 | −0.068 | 0.077 | 0.046 |
| S22 | Protein and muscle formation | −0.087 | 0.049 | −0.023 | −0.032 | −0.099 * | 0.128 * | 0.076 | −0.017 | 0.174 ** | −0.016 | 0.044 |
| S23 | Pregnant women eating for two | −0.106 * | 0.208 ** | −0.036 | 0.070 | −0.194 ** | 0.191 ** | 0.086 | 0.037 | 0.133 * | −0.073 | 0.029 |
| S24 | Cold water should not be drunk | 0.153 ** | 0.022 | −0.086 | −0.035 | 0.058 | 0.271 ** | 0.184 ** | −0.073 | 0.208 ** | −0.016 | 0.022 |
| S25 | Importance of breakfast | 0.191 ** | 0.087 | −0.043 | −0.021 | 0.158 ** | 0.223 ** | 0.163 ** | 0.083 | 0.090 | −0.087 | 0.092 * |
| S26 | Water is essential for organs | 0.115 ** | −0.065 | 0.051 | 0.007 | 0.046 | 0.125 * | 0.062 | 0.213 ** | 0.090 | 0.082 | −0.053 |
| S27 | Soy milk is healthier | 0.051 | 0.058 | −0.139 ** | −0.012 | 0.045 | 0.359 ** | 0.313 ** | −0.005 | 0.228 ** | −0.135 ** | 0.117 ** |
| S28 | Orange and dairy products | 0.040 | −0.006 | −0.034 | −0.076 | 0.016 | 0.227 ** | 0.210 ** | 0.007 | 0.186 ** | −0.010 | 0.067 |
| S29 | Portions of dairy products | −0.117 ** | −0.152 ** | −0.004 | −0.020 | −0.094 * | −0.389 ** | −0.321 ** | −0.104 | −0.273 ** | 0.162 ** | −0.057 |
| S30 | Food additives (E’s) and health | 0.135 ** | −0.059 | −0.043 | −0.121 ** | 0.118 ** | 0.356 ** | 0.354 ** | 0.060 | 0.141 ** | −0.090 * | 0.057 |
References
- Tucker, K.L. Human Nutrition. In Reference Module in Biomedical Sciences; Elsevier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Verbanac, D.; Maleš, Ž.; Barišić, K. Nutrition-facts and myths. Acta Pharm. 2019, 69, 497–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.; King, J.M.; Prinyawiwatkul, W. A review of measurement and relationships between food, eating behavior and emotion. Trends Food Sci. Technol. 2014, 36, 15–28. [Google Scholar] [CrossRef]
- Milošević, J.; Žeželj, I.; Gorton, M.; Barjolle, D. Understanding the motives for food choice in Western Balkan Countries. Appetite 2012, 58, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Cunha, L.M.; Cabral, D.; Moura, A.P.; de Almeida, M.D.V. Application of the Food Choice Questionnaire across cultures: Systematic review of cross-cultural and single country studies. Food Qual. Prefer. 2018, 64, 21–36. [Google Scholar] [CrossRef]
- Guiné, R.P.F.; Bartkiene, E.; Szűcs, V.; Tarcea, M.; Ljubičić, M.; Černelič-Bizjak, M.; Isoldi, K.; El-Kenawy, A.; Ferreira, V.; Straumite, E.; et al. Study about Food Choice Determinants According to Six Types of Conditioning Motivations in a Sample of 11,960 Participants. Foods 2020, 9, 888. [Google Scholar] [CrossRef] [PubMed]
- Worsley, A. Nutrition knowledge and food consumption: Can nutrition knowledge change food behaviour? Asia Pac. J. Clin. Nutr. 2002, 11 (Suppl. 3), S579–S585. [Google Scholar] [CrossRef] [Green Version]
- Spronk, I.; Kullen, C.; Burdon, C.; O’Connor, H. Relationship between nutrition knowledge and dietary intake. Br. J. Nutr. 2014, 111, 1713–1726. [Google Scholar] [CrossRef] [Green Version]
- Marsola, C.d.M.; Carvalho-Ferreira, J.P.d.; Cunha, L.M.; Jaime, P.C.; da Cunha, D.T. Perceptions of risk and benefit of different foods consumed in Brazil and the optimism about chronic diseases. Food Res. Int. 2021, 143, 110227. [Google Scholar] [CrossRef]
- Goodman, S.; Hammond, D.; Pillo-Blocka, F.; Glanville, T.; Jenkins, R. Use of Nutritional Information in Canada: National Trends between 2004 and 2008. J. Nutr. Educ. Behav. 2011, 43, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Downer, S.; Berkowitz, S.A.; Harlan, T.S.; Olstad, D.L.; Mozaffarian, D. Food is medicine: Actions to integrate food and nutrition into healthcare. BMJ 2020, 369, m2482. [Google Scholar] [CrossRef]
- Lesser, L.I.; Mazza, M.C.; Lucan, S.C. Nutrition myths and healthy dietary advice in clinical practice. Am. Fam. Physician 2015, 91, 634–638. [Google Scholar] [PubMed]
- Hemmer, A.; Hitchcock, K.; Lim, Y.S.; Butsch Kovacic, M.; Lee, S.-Y. Development of Food Literacy Assessment Tool Targeting Low-Income Adults. J. Nutr. Educ. Behav. 2021. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, R.; Adinolfi, P.; Annarumma, C.; Catinello, G.; Tonelli, M.; Troiano, E.; Vezzosi, S.; Manna, R. Unravelling the food literacy puzzle: Evidence from Italy. Food Policy 2019, 83, 104–115. [Google Scholar] [CrossRef]
- Vidgen, H.A.; Gallegos, D. Defining food literacy and its components. Appetite 2014, 76, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Perez, A.; Brown, A.; Elmore, S.; Hartson, K.; O’Neal, C.; King, K. P123 Nourishing Food Literacy, Community Health, and Sense of Place in Louisville, KY. J. Nutr. Educ. Behav. 2020, 52, S74. [Google Scholar] [CrossRef]
- Steils, N.; Obaidalahe, Z. “Social food”: Food literacy co-construction and distortion on social media. Food Policy 2020, 95, 101932. [Google Scholar] [CrossRef]
- Thomas, H.; Azevedo Perry, E.; Slack, J.; Samra, H.R.; Manowiec, E.; Petermann, L.; Manafò, E.; Kirkpatrick, S.I. Complexities in Conceptualizing and Measuring Food Literacy. J. Acad. Nutr. Diet. 2019, 119, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Gartaula, H.; Patel, K.; Shukla, S.; Devkota, R. Indigenous knowledge of traditional foods and food literacy among youth: Insights from rural Nepal. J. Rural Stud. 2020, 73, 77–86. [Google Scholar] [CrossRef]
- Højer, R.; Wistoft, K.; Frøst, M.B. Yes I can cook a fish; effects of a five week sensory-based experiential theme course with fish on 11- to 13- year old children’s food literacy and fish eating behaviour–A quasi-experimental study. Food Qual. Prefer. 2021, 92, 104232. [Google Scholar] [CrossRef]
- Rhea, K.C.; Cater, M.W.; McCarter, K.; Tuuri, G. Psychometric Analyses of the Eating and Food Literacy Behaviors Questionnaire with University Students. J. Nutr. Educ. Behav. 2020, 52, 1008–1017. [Google Scholar] [CrossRef] [PubMed]
- Quaidoo, E.Y.; Ohemeng, A.; Amankwah-Poku, M. Sources of nutrition information and level of nutrition knowledge among young adults in the Accra metropolis. BMC Public Health 2018, 18, 1323. [Google Scholar] [CrossRef] [PubMed]
- Liska, D.; Mah, E.; Brisbois, T.; Barrios, P.L.; Baker, L.B.; Spriet, L.L. Narrative Review of Hydration and Selected Health Outcomes in the General Population. Nutrients 2019, 11, 70. [Google Scholar] [CrossRef] [Green Version]
- Popkin, B.M.; D’Anci, K.E.; Rosenberg, I.H. Water, hydration, and health. Nutr. Rev. 2010, 68, 439–458. [Google Scholar] [CrossRef] [PubMed]
- Pereira, P.C. Milk nutritional composition and its role in human health. Nutrition 2014, 30, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Thorning, T.K.; Raben, A.; Tholstrup, T.; Soedamah-Muthu, S.S.; Givens, I.; Astrup, A. Milk and dairy products: Good or bad for human health? An assessment of the totality of scientific evidence. Food Nutr. Res. 2016, 60, 32527. [Google Scholar] [CrossRef] [Green Version]
- Jones, A.L. The Gluten-Free Diet: Fad or Necessity? Diabetes Spectr. 2017, 30, 118–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission. EU Food Additives: Making Our Food Safer; Memo/13/480; European Commission: Brussels, Belgium, 2013; pp. 1–5. [Google Scholar]
- Commision, E. COMMISSION REGULATION (EU) No 1129/2011 of 11 November 2011 amending Annex II to Regulation (EC) No 1333/2008 of the European Parliament and of the Council by establishing a Union list of food additives. Off. J. Eur. Union 2011, 295, 1–177. [Google Scholar]
- Schwingshackl, L.; Hoffmann, G.; Kalle-Uhlmann, T.; Arregui, M.; Buijsse, B.; Boeing, H. Fruit and Vegetable Consumption and Changes in Anthropometric Variables in Adult Populations: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. PLoS ONE 2015, 10, e0140846. [Google Scholar] [CrossRef]
- Dreher, M.L. Whole Fruits and Fruit Fiber Emerging Health Effects. Nutrients 2018, 10, 1833. [Google Scholar] [CrossRef] [Green Version]
- Abdul Hakim, B.N.; Yahya, H.M.; Shahar, S.; Abdul Manaf, Z.; Damanhuri, H. Effect of Sequence of Fruit Intake in a Meal on Satiety. Int. J. Environ. Res. Public Health 2019, 16, 4464. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.W.; Baird, P.; Davis, R.H., Jr.; Ferreri, S.; Knudtson, M.; Koraym, A.; Waters, V.; Williams, C.L. Health benefits of dietary fiber. Nutr. Rev. 2009, 67, 188–205. [Google Scholar] [CrossRef]
- Ramage, S.; Farmer, A.; Eccles, K.A.; McCargar, L. Healthy strategies for successful weight loss and weight maintenance: A systematic review. Appl. Physiol. Nutr. Metab. 2014, 39, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Madjd, A.; Taylor, M.A.; Delavari, A.; Malekzadeh, R.; Macdonald, I.A.; Farshchi, H.R. Beneficial effect of high energy intake at lunch rather than dinner on weight loss in healthy obese women in a weight-loss program: A randomized clinical trial. Am. J. Clin. Nutr. 2016, 104, 982–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raynor, H.A.; Li, F.; Cardoso, C. Daily pattern of energy distribution and weight loss. Physiol. Behav. 2018, 192, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Guiné, R.P.; Correia, P.; Fernandes, S.; Ramalhosa, E. Consumption of Nuts and Similar Dried Foods in Portugal and Level of Knowledge about their Chemical Composition and Health Effects. J. Nuts 2021, 12, 171–200. [Google Scholar] [CrossRef]
- Leng, G.; Adan, R.A.H.; Belot, M.; Brunstrom, J.M.; de Graaf, K.; Dickson, S.L.; Hare, T.; Maier, S.; Menzies, J.; Preissl, H.; et al. The determinants of food choice. Proc. Nutr. Soc. 2017, 76, 316–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank-Podlech, S.; Watson, P.; Verhoeven, A.A.C.; Stegmaier, S.; Preissl, H.; de Wit, S. Competing influences on healthy food choices: Mindsetting versus contextual food cues. Appetite 2021, 166, 105476. [Google Scholar] [CrossRef] [PubMed]
- Djekic, I.; Bartkiene, E.; Szűcs, V.; Tarcea, M.; Klarin, I.; Černelić-Bizjak, M.; Isoldi, K.; El-Kenawy, A.; Ferreira, V.; Klava, D.; et al. Cultural dimensions associated with food choice: A survey based multi-country study. Int. J. Gastron. Food Sci. 2021, 26, 100414. [Google Scholar] [CrossRef]

| Code | Statement | Nature |
|---|---|---|
| S1 | Drinking water during meals, contributes to weight gain. | Myth |
| S2 | The digestion process begins in the mouth. | Fact |
| S3 | Fruit should be eaten before meals. | Myth |
| S4 | Egg consumption increases blood cholesterol. | Myth |
| S5 | Drinking milk is bad for health. | Myth |
| S6 | Eating carbohydrates at night leads to an increase in weight gain. | Myth |
| S7 | Fat is important to the human body. | Fact |
| S8 | Fruit should be eaten after meals. | Myth |
| S9 | Fiber intake is important for normal bowel function. | Fact |
| S10 | Gluten-free foods are better for health and should, there-fore, be adopted by all. | Myth |
| S11 | Cheese consumption is bad for memory. | Myth |
| S12 | Coconut oil is healthier than olive oil. | Myth |
| S13 | Lactose-free foods are better for health and should, there-fore, be adopted by all. | Myth |
| S14 | Children have different nutritional needs than those for adults. | Fact |
| S15 | Fruits and vegetables do not contribute to weight gain. | Myth |
| S16 | Normal potatoes are more caloric than sweet potatoes. | Myth |
| S17 | Diet should be adapted to a person’s blood group. | Myth |
| S18 | Not having a balanced and varied diet can lead to the development of multiple diseases. | Fact |
| S19 | The alkaline diet allows balancing the acidity in the blood. | Myth |
| S20 | Drinking, while fasting, a glass of water with lemon helps in weight loss. | Myth |
| S21 | Inadequate eating habits are the third risk factor for the loss of years of healthy life. | Fact |
| S22 | Ingesting high amounts of protein helps in the faster formation of muscles. | Myth |
| S23 | Pregnant women should be eating for two. | Myth |
| S24 | Cold water should not be drunk. | Myth |
| S25 | The day should always start with breakfast. | Fact |
| S26 | Water is essential to the normal function of all organs. | Fact |
| S27 | Soy milk is healthier than cow’s milk. | Myth |
| S28 | Orange should not be eaten at the same time as milk or yogurt. | Myth |
| S29 | Dairy products should be consumed in between two and three portions per day. | Fact |
| S30 | All food additives (E’s) are harmful to health. | Myth |
| Variable | N | % | |
|---|---|---|---|
| Age group | Young adults (18–30 years) | 137 | 27.2 |
| Middle aged adults (31–50 years) | 216 | 42.9 | |
| Senior adults (51–65 years) | 126 | 25.0 | |
| Elderly (≥66 years) | 24 | 4.8 | |
| Sex | Women | 390 | 77.8 |
| Men | 111 | 22.2 | |
| Education level | Basic | 10 | 2.0 |
| Secondary | 87 | 17.3 | |
| University | 232 | 46.1 | |
| Post-graduation | 174 | 34.6 | |
| Living environment | Urban | 287 | 68.4 |
| Suburban | 57 | 11.3 | |
| Rural | 102 | 20.3 | |
| Marital status | Single | 172 | 34.2 |
| Married/Union | 287 | 57.1 | |
| Divorced/Separate | 38 | 7.6 | |
| Widowed | 6 | 1.2 | |
| Total | 503 | 100 | |
| Profession | N | % | Diet | N | % |
| Other | 197 | 39.2 | Calorie Restriction | 178 | 35.4 |
| Food | 175 | 34.8 | Flexitarianism | 43 | 8.5 |
| Health | 168 | 33.4 | Vegetarianism | 22 | 4.4 |
| Nutrition | 142 | 28.2 | Fruitarianism | 21 | 4.2 |
| Biology | 94 | 18.7 | Crudism | 10 | 2.0 |
| Agriculture | 81 | 16.1 | Veganism | 8 | 1.6 |
| Environment | 77 | 15.3 | Religious Restriction | 7 | 1.4 |
| Sports | 40 | 8.0 | |||
| BMI percentile | BMI (kg/m2) | BMI Class 1 | % | ||
| 5% | 19.1 | Underweight | 3.4 | ||
| 10% | 20.0 | Normal weight | 57.5 | ||
| 25% | 21.4 | Overweight | 32.6 | ||
| 50% | 23.7 | Obesity | 6.6 | ||
| 75% | 26.3 | ||||
| 90% | 28.9 | ||||
| 95% | 31.3 | ||||
| Items | Mean ± SD 1 | Sum Score 2 |
|---|---|---|
| S26. Water is essential to the normal function of all organs. | 0.96 ± 0.18 | 484.5 |
| S9. Fiber intake is important for normal bowel function. | 0.89 ± 0.25 | 445.0 |
| S11. Cheese consumption is bad for memory. | 0.88 ± 0.31 | 441.5 |
| S18. Not having a balanced and varied diet can lead to the development of multiple diseases. | 0.87 ± 0.30 | 437.0 |
| S23. Pregnant women should be eating for two. | 0.83 ± 0.33 | 418.0 |
| S14. Children have different nutritional needs than those for adults. | 0.82 ± 0.33 | 410.5 |
| S2. The digestion process begins in the mouth. | 0.77 ± 0.49 | 385.0 |
| S1. Drinking water during meals, contributes to weight gain. | 0.70 ± 0.50 | 351.5 |
| S11. Cheese consumption is bad for memory. | 0.88 ± 0.31 | 441.5 |
| S18. Not having a balanced and varied diet can lead to the development of multiple diseases. | 0.87 ± 0.30 | 437.0 |
| S23. Pregnant women should be eating for two. | 0.83 ± 0.33 | 418.0 |
| S14. Children have different nutritional needs than those for adults. | 0.82 ± 0.33 | 410.5 |
| S2. The digestion process begins in the mouth. | 0.77 ± 0.49 | 385.0 |
| S1. Drinking water during meals, contributes to weight gain. | 0.70 ± 0.50 | 351.5 |
| S25. The day should always start with breakfast. | 0.68 ± 0.52 | 341.5 |
| S21. Inadequate eating habits are the third risk factor for the loss of years of healthy life. | 0.66 ± 0.43 | 330.5 |
| S7. Fat is important to the human body. | 0.54 ± 0.53 | 269.5 |
| S17. Diet should be adapted to a person’s blood group. | 0.52 ± 0.58 | 259.0 |
| S12. Coconut oil is healthier than olive oil. | 0.51 ± 0.56 | 257.0 |
| S13. Lactose-free foods are better for health and should, therefore, be adopted by all. | 0.50 ± 0.59 | 250.5 |
| S5. Drinking milk is bad for health. | 0.47 ± 0.59 | 237.5 |
| S4. Egg consumption increases blood cholesterol. | 0.43 ± 0.54 | 217.5 |
| S10. Gluten-free foods are better for health and should, therefore, be adopted by all. | 0.41 ± 0.60 | 206.5 |
| S27. Soy milk is healthier than cow’s milk. | 0.35 ± 0.60 | 175.0 |
| S20. Drinking, while fasting, a glass of water with lemon helps in weight loss. | 0.34 ± 0.61 | 172.5 |
| S28. Orange should not be eaten at the same time as milk or yogurt. | 0.32 ± 0.62 | 160.5 |
| S19. The alkaline diet allows balancing the acidity in the blood. | 0.24 ± 0.59 | 118.5 |
| S15. Fruits and vegetables do not contribute to weight gain. | 0.24 ± 0.59 | 118.0 |
| S22. Ingesting high amounts of protein helps in the faster formation of muscles. | 0.14 ± 0.57 | 68.5 |
| S29. Dairy products should be consumed in between two and three portions per day. | 0.13 ± 0.58 | 66.5 |
| S24. Cold water should not be drunk. | 0.11 ± 0.66 | 57.0 |
| S16. Normal potatoes are more caloric than sweet potatoes. | 0.10 ± 0.68 | 50.0 |
| S3. Fruit should be eaten before meals. | 0.08 ± 0.62 | 38.0 |
| S30. All food additives (E’s) are harmful to health. | 0.07 ± 0.65 | 37.0 |
| S8. Fruit should be eaten after meals. | 0.05 ± 0.58 | 25.5 |
| S6. Eating carbohydrates at night leads to an increase in weight gain. | −0.02 ± 0.71 | −10.0 |
| Information Sources | Frequency of Use (% of Respondents) | Level of Trust (% of Respondents) | Spearman Correlation 1 | |||||
|---|---|---|---|---|---|---|---|---|
| Never | Few Times | Many Times | No Trust | Some Trust | Much Trust | Full Trust | ||
| YouTube channels of influencers | 77.3 | 19.7 | 3.0 | 81.3 | 18.3 | 0.4 | 0 | 0.568 ** |
| Nutritionist blogs | 32.6 | 46.5 | 20.9 | 10.9 | 60.0 | 25.6 | 3.4 | 0.383 ** |
| DGS website | 25.3 | 43.3 | 31.4 | 2.0 | 22.7 | 39.2 | 36.2 | 0.335 ** |
| Natural food stores | 55.9 | 36.8 | 7.4 | 35.0 | 50.3 | 11.9 | 2.8 | 0.539 ** |
| Scientific journals | 27.0 | 38.6 | 34.4 | 2.4 | 23.7 | 39.8 | 34.2 | 0.362 ** |
| Internet pages | 28.2 | 53.3 | 18.5 | 39.0 | 56.5 | 4.0 | 0.6 | 0.483 ** |
| Social media | 54.5 | 36.6 | 8.9 | 67.0 | 30.8 | 2.0 | 0.2 | 0.570 ** |
| Television | 36.2 | 54.1 | 9.7 | 28.8 | 56.1 | 13.5 | 1.6 | 0.649 ** |
| Technical books | 28.6 | 40.4 | 31.0 | 3.0 | 25.0 | 38.2 | 33.8 | 0.304 ** |
| WHO website | 34.2 | 38.6 | 27.2 | 2.4 | 20.7 | 34.4 | 42.5 | 0.337 ** |
| Pharmacies | 58.3 | 33.4 | 8.3 | 13.7 | 43.7 | 29.0 | 3.5 | 0.341 ** |
| Health centers | 38.6 | 44.9 | 16.5 | 4.8 | 30.2 | 40.2 | 24.9 | 0.301 ** |
| Appointments with Medical doctors/ nutritionists | 27.6 | 43.1 | 29.2 | 2.0 | 18.7 | 34.6 | 44.7 | 0.263 ** |
| Information Sources | Spearman Correlation between Level of Knowledge and Frequency of Utilization of Information Sources | Spearman Correlation between Level of Knowledge and Level of Trust in the Information Sources |
|---|---|---|
| YouTube channels of influencers | −0.240 ** | −0.234 ** |
| Nutritionist blogs | −0.063 | −0.021 |
| DGS Website | 0.320 ** | 0.357 ** |
| Natural food stores | −0.355 ** | −0.416 ** |
| Scientific journals | 0.385 ** | 0.380 ** |
| Internet pages | −0.121 ** | 0.006 |
| Social media | −0.209 ** | −0.161 ** |
| Television | −0.285 ** | −0.266 ** |
| Technical books | 0.283 ** | 0.263 ** |
| WHO website | 0.357 ** | 0.342 ** |
| Pharmacies | −0.124 ** | −0.179 ** |
| Health centers | 0.083 | 0.086 |
| Appointments with Medical doctors/nutritionists | 0.072 | 0.213 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Florença, S.G.; Ferreira, M.; Lacerda, I.; Maia, A. Food Myths or Food Facts? Study about Perceptions and Knowledge in a Portuguese Sample. Foods 2021, 10, 2746. https://doi.org/10.3390/foods10112746
Florença SG, Ferreira M, Lacerda I, Maia A. Food Myths or Food Facts? Study about Perceptions and Knowledge in a Portuguese Sample. Foods. 2021; 10(11):2746. https://doi.org/10.3390/foods10112746
Chicago/Turabian StyleFlorença, Sofia G., Manuela Ferreira, Inês Lacerda, and Aline Maia. 2021. "Food Myths or Food Facts? Study about Perceptions and Knowledge in a Portuguese Sample" Foods 10, no. 11: 2746. https://doi.org/10.3390/foods10112746
APA StyleFlorença, S. G., Ferreira, M., Lacerda, I., & Maia, A. (2021). Food Myths or Food Facts? Study about Perceptions and Knowledge in a Portuguese Sample. Foods, 10(11), 2746. https://doi.org/10.3390/foods10112746