
Moderating Effect of Changes in Perceived Social Support during Pregnancy on the Emotional Health of Mothers and Fathers and on Baby’s Anthropometric Parameters at Birth

 ,
,
Abstract

1. Introduction
2. Methods
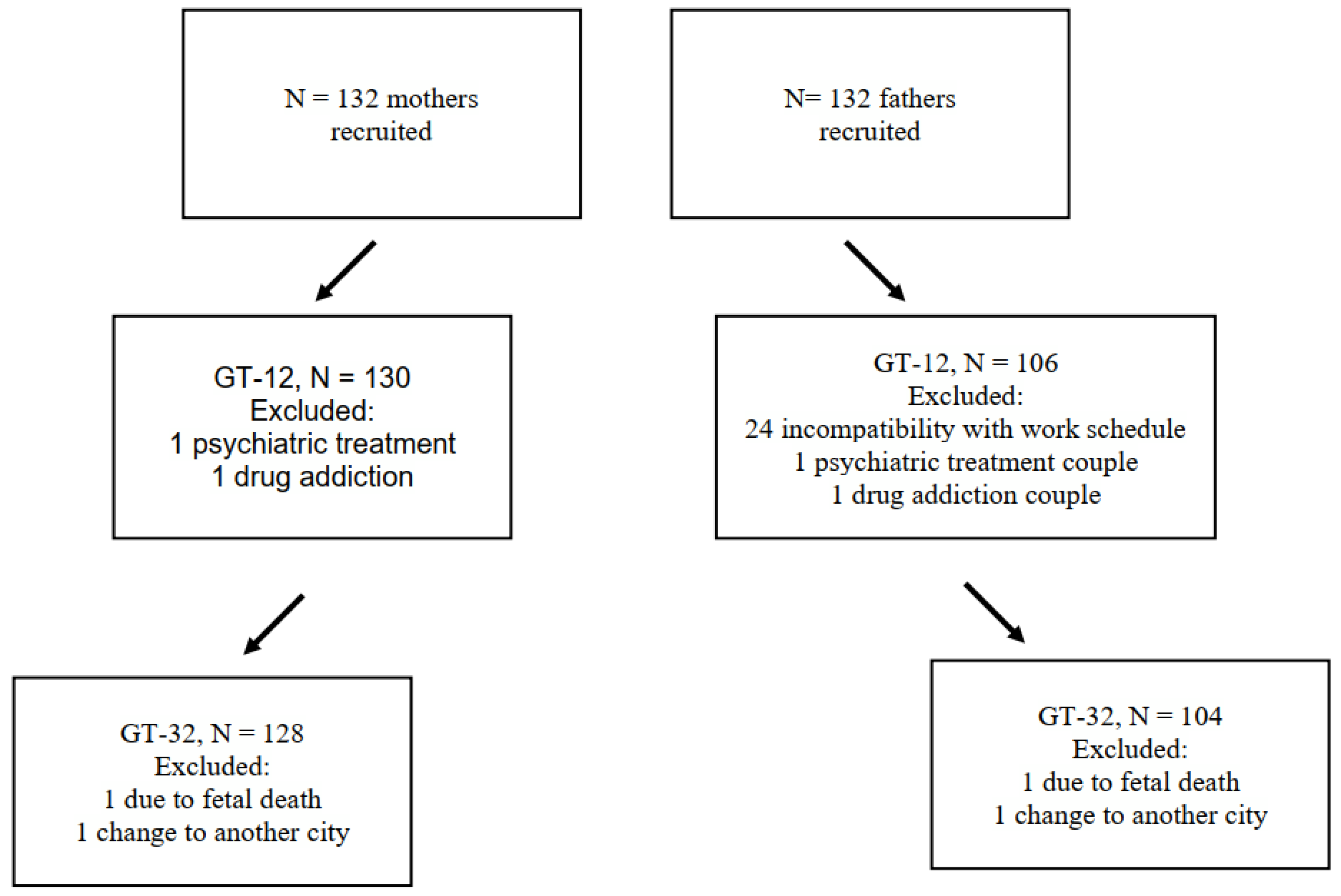
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Data Analysis
3. Results
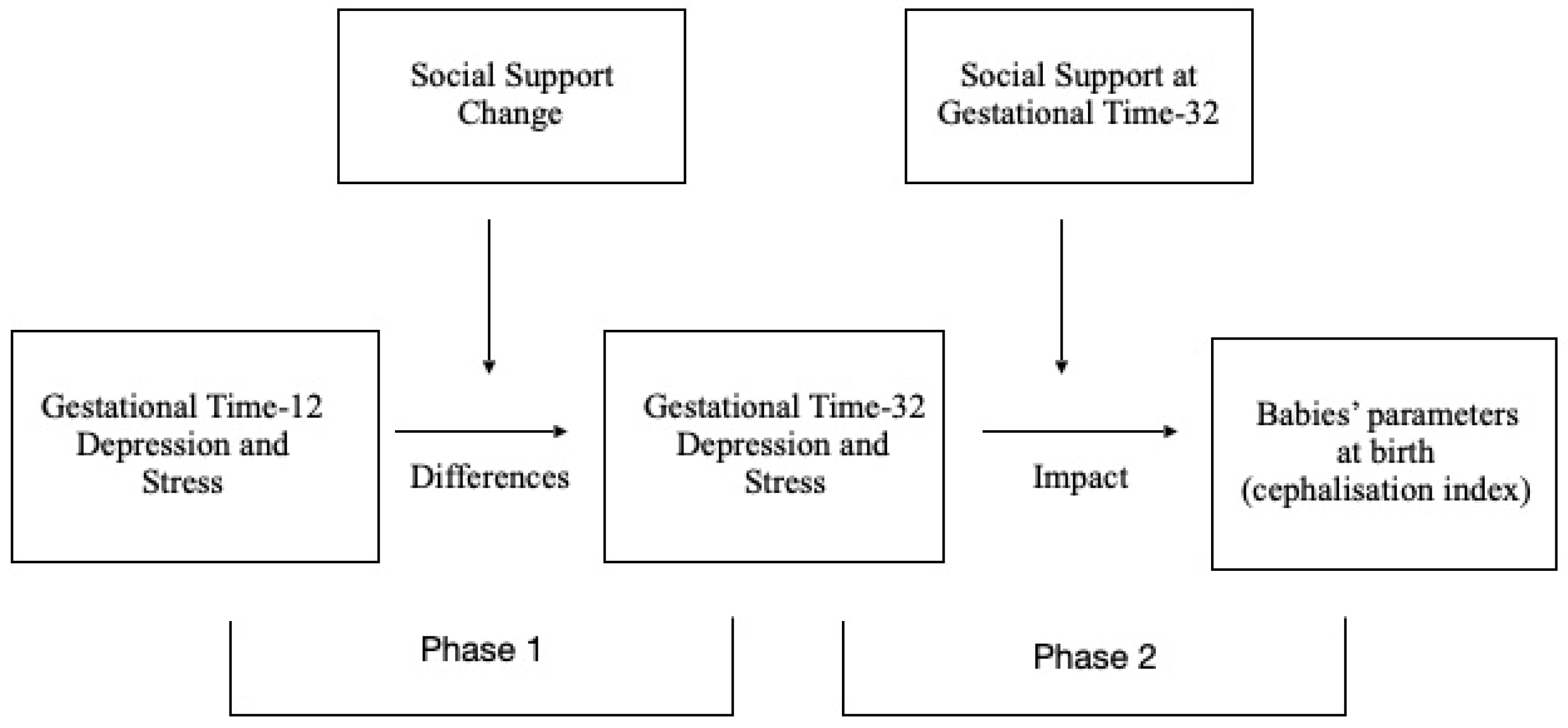
3.1. Aim 1: To Determine the Outcomes of Perceived Changes in Social Support during Pregnancy, with Particular Reference to the Moderation of Depression and Stress in This Period
3.2. Aim 2: Social Support as a Mitigating or Protective Factor Moderating the Relationship between Parents’ Levels of Depression/Stress and Their Babies’ Anthropometric Measures
4. Discussion
5. Limitations
6. Conclusions
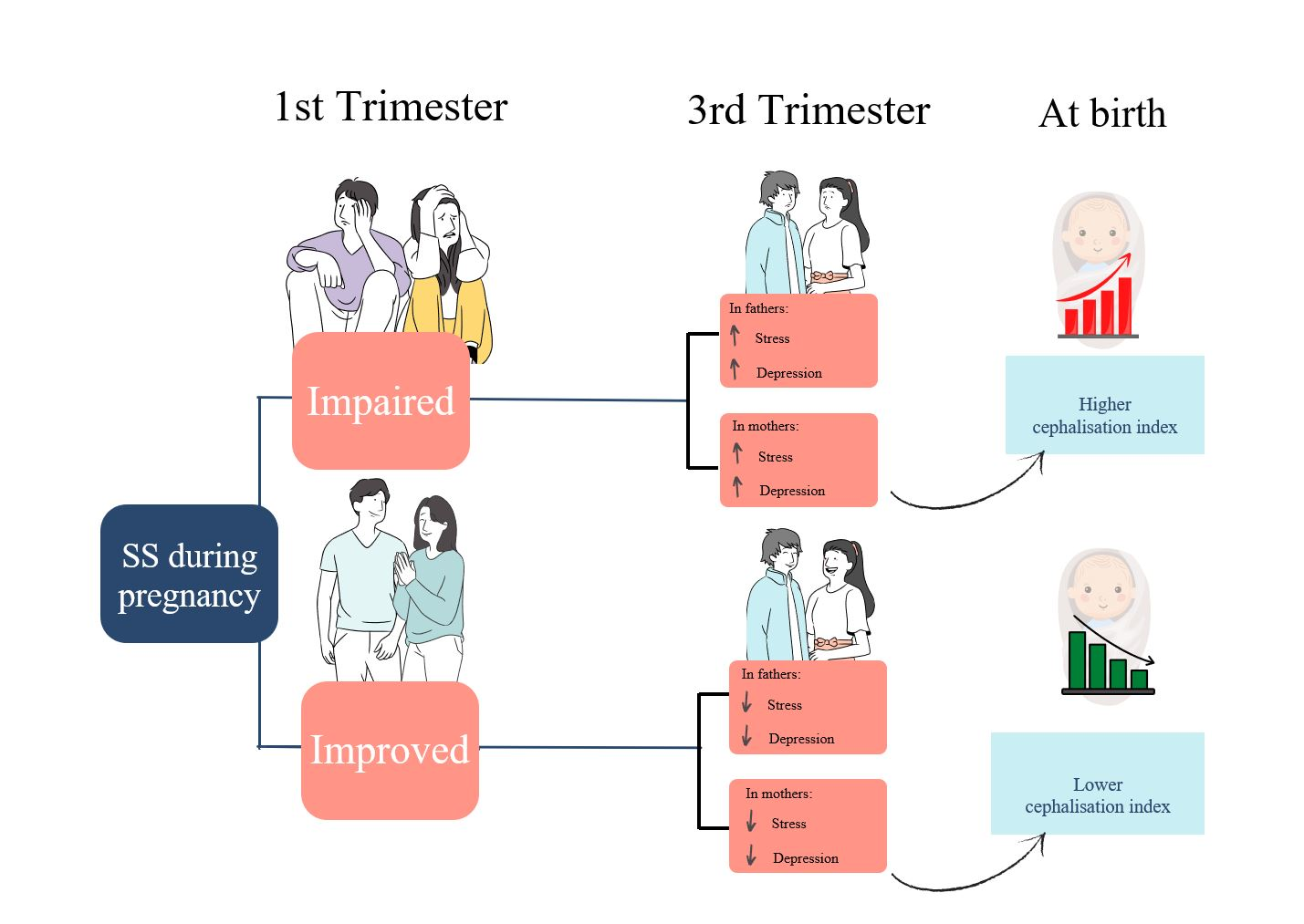
- The moderating effect of social support is powerful, such that a change in this protective variable produces changes in stress and depression outcomes, for both parents.
- Babies whose mothers were more depressed or stressed presented higher rates of cephalisation.
- Interventions tailored to each stage of pregnancy should be implemented to provide parents with the means to reinforce social support as a protective factor.
- Finally, the present study is focused on parents whose pregnancy follows the normal course. However, it may be assumed that if an intervention to foster social support is beneficial for these mothers and fathers, it would be even more so for those having to cope with a high-risk pregnancy.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schetter, C.D. Psychological science on pregnancy: Stress processes, biopsychosocial models, and emerging research issues. Annu. Rev. Psychol. 2011, 62, 531–558. [Google Scholar] [CrossRef] [PubMed]
- Madhavanprabhakaran, G.K.; D’Souza, M.S.; Nairy, K.S. Prevalence of pregnancy anxiety and associated factors. Int. J. Afr. Nurs. Sci. 2015, 3, 1–7. [Google Scholar] [CrossRef][Green Version]
- Rallis, S.; Skouteris, H.; McCabe, M.; Milgrom, J.A. prospective examination of depression, anxiety and stress throughout pregnancy. Women Birth 2014, 27, e36–e42. [Google Scholar] [CrossRef] [PubMed]
- Obrochta, C.A.; Chambers, C.; Bandoli, G. Psychological distress in pregnancy and postpartum. Women Birth 2020, 33, 583–591. [Google Scholar] [CrossRef]
- Gokoel, A.R.; Abdoel Wahid, F.; Zijlmans, W.C.W.R.; Shankar, A.; Hindori-Mohangoo, A.D.; Covert, H.H.; MacDonald-Ottevanger, M.S.; Lichtveld, M.; Harville, E.W. Influence of perceived stress on prenatal depression in Surinamese women enrolled in the CCREOH study. Reprod. Health 2021, 18, 136. [Google Scholar] [CrossRef]
- Mélançon, J.; Bernard, N.; Forest, J.C.; Tessier, R.; Tarabulsy, G.M.; Bouvier, D.; Giguère, Y. Impact of maternal prenatal psychological stress on birth weight. Health Psychol. 2020, 39, 1100. [Google Scholar] [CrossRef]
- Bellido-González, M.; Robles-Ortega, H.; Castelar-Ríos, M.J.; Díaz-López, M.A.; Gallo-Vallejo, J.L.; Moreno-Galdó, M.F.; de los Santos-Roig, M. Psychological distress and resilience of mothers and fathers with respect to the neurobehavioral performance of small-for-gestational-age newborns. Health Qual. Life Outcomes 2019, 17, 54. [Google Scholar] [CrossRef]
- Glover, V. Prenatal stress and its effects on the fetus and the child: Possible underlying biological mechanisms. In Perinatal Programming of Neurodevelopment. Advances in Neurobiology; Antonelli, M., Ed.; Springer: New York, NY, USA, 2014; Volume 10, pp. 269–293. [Google Scholar] [CrossRef]
- Glover, V.; Ahmed-Salim, Y.; Capron, L. maternal anxiety, depression, and stress during pregnancy: Effects on the fetus and the child, and underlying mechanisms. In Fetal Development; Reissland, N., Kisilevsky, B., Eds.; Springer: New York, NY, USA, 2015; pp. 213–227. [Google Scholar] [CrossRef]
- Cheng, E.R.; Rifas-Shiman, S.L.; Perkins, M.E.; Rich-Edwards, J.W.; Gillman, M.W.; Wright, R.; Taveras, E.M. The influence of antenatal partner support on pregnancy outcomes. J. Women’s Health 2016, 25, 672–679. [Google Scholar] [CrossRef]
- Racine, N.; Plamondon, A.; Hentges, R.; Tough, S.; Madigan, S. Dynamic and bidirectional associations between maternal stress, anxiety, and social support: The critical role of partner and family support. J. Affect. Disord. 2019, 25, 19–24. [Google Scholar] [CrossRef]
- Stapleton, L.R.T.; Schetter, C.D.; Westling, E.; Rini, C.; Glynn, L.M.; Hobel, C.J.; Sandman, C.A. Perceived partner support in pregnancy predicts lower maternal and infant distress. J. Fam. Psychol. 2012, 26, 453. [Google Scholar] [CrossRef]
- Rondó, P.H.; Ferreira, R.F.; Nogueira, F.; Ribeiro, M.C.; Lobert, H.; Artes, R. Maternal psychological stress and distress as predictors of low birth weight, prematurity and intrauterine growth retardation. Eur. J. Clin. Nutr. 2003, 57, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zeng, Y.; Zhu, W.; Cui, Y.; Li, J. Path model of antenatal stress and depressive symptoms among Chinese primipara in late pregnancy. BMC Pregnancy Childbirth 2016, 16, 180. [Google Scholar] [CrossRef] [PubMed]
- Appleton, A.A.; Kiley, K.; Holdsworth, E.A.; Schell, L.M. Social support during pregnancy modifies the association between maternal adverse childhood experiences and infant birth size. Matern. Child Health J. 2019, 23, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Kothari, A.; Thayalan, K.; Dulhunty, J.; Callaway, L. The forgotten father in obstetric medicine. Obstet. Med. 2019, 12, 57–65. [Google Scholar] [CrossRef]
- Leach, L.S.; Poyser, C.; Cooklin, A.R.; Giallo, R. Prevalence and course of anxiety disorders (and symptom levels) in men across the perinatal period: A systematic review. J. Affect. Disord. 2016, 190, 675–686. [Google Scholar] [CrossRef]
- Philpott, L.F.; Savage, E.; FitzGerald, S.; Leahy-Warren, P. Anxiety in fathers in the perinatal period: A systematic review. Midwifery 2019, 76, 54–101. [Google Scholar] [CrossRef]
- Poh, H.L.; Koh, S.S.L.; He, H.G. An integrative review of fathers’ experiences during pregnancy and childbirth. Int. Nurs. Rev. 2014, 61, 543–554. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression: Development of the 10-item Edinburgh Postnatal Depression scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Garcia-Esteve, L.; Ascaso, C.; Ojuel, J.; Navarro, P. Validation of the Edinburgh Postnatal Depression Scale (EPDS) in Spanish mothers. J. Affect. Disord. 2003, 75, 71–76. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Remor, E. Psychometric properties of a European Spanish Version of the Perceived Stress Scale (PSS). Span. J. Psychol. 2006, 9, 86–93. [Google Scholar] [CrossRef]
- Zimet, G.; Dahlem, N.; Zimet, S.; Farley, G. The Multidimensional Scale of Perceived Social Support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef]
- Skouteris, H.; Wertheim, E.H.; Rallis, S.; Milgrom, J.; Paxton, S.J. Depression and anxiety through pregnancy and the early postpartum: An examination of prospective relationships. J. Affect. Disord. 2009, 113, 303–308. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Antenatal Care for Uncomplicated Pregnancies. Clinical Guideline [CG62]. Available online: https://www.nice.org.uk/guidance/cg62 (accessed on 25 April 2022).
- Harel, S.; Tomer, A.; Barak, Y.; Binderman, I.; Yavin, E. The cephalization index: A screening device for brain maturity and vulnerability in normal and intrauterine growth retarded newborns. Brain Dev. 1985, 7, 580–584. [Google Scholar] [CrossRef]
- Leitner, Y.; Fattal-Valevski, A.; Geva, R.; Eshel, R.; Toledano-Alhadef, H.; Rotstein, M.; Bassan, H.; Radianu, B.; Bitchonsky, O.; Jaffa, A.J.; et al. Neurodevelopmental outcome of children with intrauterine growth retardation: A longitudinal, 10-year prospective study. J. Child Neurol. 2007, 22, 580–587. [Google Scholar] [CrossRef]
- Rothman, K.J.; Greenland, S. Modern Epidemiology, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; pp. 1–851. [Google Scholar] [CrossRef]
- Montoya, A.K. Moderation analysis in two-instance repeated measures designs: Probing methods and multiple moderator models. Behav. Res. Methods. 2019, 51, 61–82. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2018; pp. 1–692. [Google Scholar]
- Bedaso, A.; Adams, J.; Peng, W.; Sibbritt, D. The relationship between social support and mental health problems during pregnancy: A systematic review and meta-analysis. Reprod. Health 2021, 18, 162. [Google Scholar] [CrossRef]
- Figueiredo, B.; Conde, A. Anxiety and depression in women and men from early pregnancy to 3-months postpartum. Arch. Women’s Ment. Health 2011, 14, 247–255. [Google Scholar] [CrossRef]
- Feldman, P.J.; Dunkel-Schetter, C.; Sandman, C.A.; Wadhwa, P.D. Maternal social support predicts birth weight and fetal growth in human pregnancy. Psychosom. Med. 2000, 62, 715–725. [Google Scholar] [CrossRef]
- Accortt, E.E.; Cheadle, A.C.D.; Dunkel Schetter, C. Prenatal depression and adverse birth outcomes: An updated systematic review. Matern. Child Health J. 2015, 19, 1306–1337. [Google Scholar] [CrossRef]
- O’Donnell, K.J.; Glover, V. Maternal prenatal stress and the developmental origins of mental health: The role of epigenetics. In The Epigenome and Developmental Origins of Health and Disease; Rosenfeld, C.S., Ed.; Academic Press: Cambridge, MA, USA, 2015; pp. 103–126. [Google Scholar]
- Miranda, A.; Olhaberry, M.; Morales-Reyes, I. Intervención grupal en embarazadas: Respuestas diferenciales de acuerdo al tipo de depresión y patrón de apego. Psykhe 2017, 26, 1–17. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Mother (N = 130) | Partner (N = 106) | Test | |
|---|---|---|---|
| Age, mean (SD) | 30.53 (5.79) | 32.87 (5.69) | t222 = −3.80 ** |
| Range | 16–44 | 16–47 | |
| Duration of relationship, mean (SD) | 7.58 (6.53) | 7.58 (6.53) | |
| Range | 1–25 | 1–25 | |
| Parity status, n (%) | |||
| Primiparous | 69 (53.37) | ||
| Multiparous | 61 (46.63) | ||
| Spanish language fluency, n (%) | 130 (100) | 106 (100) | |
| Education, n (%) | |||
| Primary | 39 (30.06) | 32 (29.83) | |
| Secondary | 44 (33.74) | 35 (33.33) | χ2 = 5.00 n.s. |
| Higher | 47 (36.20) | 39 (36.84) | |
| In paid employment, n (%) | |||
| Yes | 82 (63.19) | 78 (73.39) | χ24 = 7.89 ** |
| No | 38 (28.83) | 13 (11.93) | |
| Not answered | 10 (7.98) | 15 (14.68) |
| R2 | F | S.E. | β | t | p | |||
|---|---|---|---|---|---|---|---|---|
| Depression differences | ||||||||
| Mothers | 0.146 | 21.40 | 29.44 | <0.0001 | ||||
| SS change | −0.227 | −4.72 | <0.0001 | |||||
| Fathers | 0.085 | 9.06 | 27.18 | <0.01 | ||||
| SS change | −0.168 | −3.01 | <0.01 | |||||
| Stress differences | ||||||||
| Mothers | 0.109 | 15.54 | 107.33 | <0.001 | ||||
| SS change | −0.371 | −3.94 | <0.001 | |||||
| Fathers | 0.105 | 11.74 | 91.41 | <0.001 | ||||
| SS change | −0.328 | −3.42 | <0.001 |
| Depression | ||||||
|---|---|---|---|---|---|---|
| Mean | S.E. | t | p | |||
| GT-12 | GT-32 | |||||
| Mothers | Improved SS | 7.85 | 5.11 | 0.68 | 4.00 | 0.00 |
| No change | 6.7 | 6.21 | 0.48 | 1.02 | 0.30 | |
| Impaired SS | 5.56 | 7.30 | 0.68 | −2.55 | 0.01 | |
| Fathers | Improved SS | 5.01 | 3.27 | 0.74 | 2.34 | 0.02 |
| No change | 4.51 | 4.36 | 0.52 | 0.29 | 0.76 | |
| Impaired SS | 4.01 | 5.44 | 0.74 | −1.92 | 0.05 | |
| Stress | ||||||
| Mean | S.E. | t | p | |||
| GT-12 | GT-32 | |||||
| Mothers | Improved SS | 27.31 | 24.73 | 1.29 | 1.99 | 0.04 |
| No change | 25.53 | 26.56 | 0.91 | −1.12 | 0.26 | |
| Impaired SS | 23.76 | 28.79 | 1.29 | −3.58 | 0.00 | |
| Fathers | Improved SS | 24.6 | 20.43 | 1.34 | 3.10 | 0.00 |
| No change | 23.27 | 22.37 | 0.94 | 0.95 | 0.34 | |
| Impaired SS | 21.95 | 24.30 | 1.34 | −1.75 | 0.08 | |
| Mothers | ||||||
|---|---|---|---|---|---|---|
| R2 | F | S.E. | β | t | p | |
| Cephalisation Index | 0.584 | 16.02 | 0.01 | <0.0001 | ||
| Depression at GT-32 | 0.066 | 2.61 | 0.01 | |||
| Social Support at GT-32 | 0.008 | 1.80 | 0.07 | |||
| Interaction | −0.001 | −2.28 | 0.02 | |||
| Cephalisation Index | 0.578 | 15.77 | 0.18 | <0.0001 | ||
| Stress at GT-32 | 0.032 | 2.44 | 0.01 | |||
| Social Support at GT-32 | 0.014 | 1.93 | 0.051 | |||
| Interaction | 0.000 | −2.19 | 0.03 | |||
| R2 | F | S.E. | β | t | p | |
| Size at birth | 0.389 | 7.25 | 5.26 | <0.0001 | ||
| Depression at GT-32 | −0.892 | −2.08 | 0.03 | |||
| Social Support at GT-32 | −0.140 | −1.88 | 0.06 | |||
| Interaction | 0.010 | 1.88 | 0.06 | |||
| Size at birth | 0.375 | 6.99 | 5.28 | <0.0001 | ||
| Stress at GT-32 | −0.380 | −1.72 | 0.08 | |||
| Social Support at GT-32 | −0.200 | −1.60 | n.s. | |||
| Interaction | 0.006 | 1.58 | n.s. | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castelar-Ríos, M.J.; De los Santos-Roig, M.; Robles-Ortega, H.; Díaz-López, M.Á.; Maldonado-Lozano, J.; Bellido-González, M. Moderating Effect of Changes in Perceived Social Support during Pregnancy on the Emotional Health of Mothers and Fathers and on Baby’s Anthropometric Parameters at Birth. Children 2022, 9, 648. https://doi.org/10.3390/children9050648
Castelar-Ríos MJ, De los Santos-Roig M, Robles-Ortega H, Díaz-López MÁ, Maldonado-Lozano J, Bellido-González M. Moderating Effect of Changes in Perceived Social Support during Pregnancy on the Emotional Health of Mothers and Fathers and on Baby’s Anthropometric Parameters at Birth. Children. 2022; 9(5):648. https://doi.org/10.3390/children9050648
Chicago/Turabian StyleCastelar-Ríos, María José, Macarena De los Santos-Roig, Humbelina Robles-Ortega, Miguel Ángel Díaz-López, José Maldonado-Lozano, and Mercedes Bellido-González. 2022. "Moderating Effect of Changes in Perceived Social Support during Pregnancy on the Emotional Health of Mothers and Fathers and on Baby’s Anthropometric Parameters at Birth" Children 9, no. 5: 648. https://doi.org/10.3390/children9050648
APA StyleCastelar-Ríos, M. J., De los Santos-Roig, M., Robles-Ortega, H., Díaz-López, M. Á., Maldonado-Lozano, J., & Bellido-González, M. (2022). Moderating Effect of Changes in Perceived Social Support during Pregnancy on the Emotional Health of Mothers and Fathers and on Baby’s Anthropometric Parameters at Birth. Children, 9(5), 648. https://doi.org/10.3390/children9050648