Abstract
Background and Objectives: Dental caries remains one of the most prevalent chronic conditions among children worldwide, with considerable variation in burden shaped by differences in health-system organization and preventive program implementation. Some countries have reported notable progress through coordinated school-based programs and supportive policy environments, while others continue to face challenges despite extensive public health efforts. This study aims to explore how selected structural and programmatic elements within national health systems may be associated with childhood caries outcomes, using Germany and Saudi Arabia as illustrative contexts. Materials and Methods: A descriptive comparative secondary-data analysis combined with legal and policy mapping was conducted using published national oral health surveys, systematic reviews, and governmental reports. Caries indicators (dmft/DMFT) for children aged 6–7 and 12 years were extracted following WHO criteria. Health system organization, preventive program coverage, and policy enforcement mechanisms were mapped and critically reviewed. No new primary data were collected, and no inferential modeling was performed. Results: Germany has achieved substantial reductions in childhood caries prevalence through a legally mandated school-based prevention program, supported by individual prophylaxis covered by health insurance. This framework corresponds with low mean dmft (1.73) among 6–7-year-olds and mean DMFT (0.5) among 12-year-olds. By contrast, Saudi Arabia continues to report elevated caries rates despite substantial public-health investments, with mean dmft (5.0) and mean DMFT (3.5), with over 90% of children affected. Preventive initiatives in Saudi Arabia remain fragmented across sectors and lack a unified legal mandate. Conclusions: The findings suggest that structured governance, coordinated prevention strategies, and reliable monitoring systems may be associated with more favorable oral health outcomes. In the context of Saudi Arabia, the persistently high caries burden suggests that strengthening national legislation, implementing an interoperable digital surveillance system, and improving the consistency of school-based preventive programs could support more equitable and effective oral health delivery.
1. Introduction
Dental caries remains one of the most common chronic diseases affecting children worldwide and continue to pose significant public health challenges due to their impact on well-being, daily functioning, and quality of life [1]. Although many high-income countries have achieved substantial reductions in childhood caries over recent decades, marked disparities persist both between and within nations [2].
Germany is among the most successful examples of sustained caries reduction. National surveillance data show that children and adolescents in Germany have healthier teeth than ever before, with a mean dmft (1.7) among 6–7-year-olds and a mean DMFT (0.5) among 12-year-olds—the WHO reference age group for international comparisons [3,4,5,6]. These values classify Germany as a low-caries-prevalence country according to WHO criteria.
By contrast, dental caries remains a significant public health concern among children in Saudi Arabia. Despite multiple public health initiatives, the prevalence of untreated caries remains high, with approximately 80% of primary dentition affected (mean dmft of 5.0) and 70% of permanent dentition affected (mean DMFT of 3.5) [3]. According to the Saudi Ministry of Health, the caries prevalence is 96% among 6-year-olds and 93.7% among 12-year-olds, underscoring the severity of the burden among school-aged children [4].
Understanding these differences requires examining not only epidemiological trends but also the structural and organizational characteristics of national health systems. To enhance the effectiveness of caries prevention programs for schoolchildren in Saudi Arabia, it is essential to assess the structure of the healthcare system, evaluate the public oral health framework, review preventive program organization, and analyze epidemiological patterns. Many developed countries refine their healthcare and oral health strategies by comparing their systems with those of others to identify strengths and weaknesses, thereby improving public health outcomes [5].
Therefore, this study aims to analyze how health system structures, preventive program organization, and policy frameworks may be associated with differences in childhood caries prevalence between Germany and Saudi Arabia. By comparing healthcare models, public oral health programs, and preventive strategies in both countries, this study seeks to identify key structural factors that could support more effective caries prevention efforts in Saudi Arabia.
2. Materials and Methods
2.1. Study Design
This study employed a descriptive comparative secondary data analysis combined with legal and policy mapping to examine differences in dental caries patterns and oral-health system structures relevant to schoolchildren in Germany and Saudi Arabia. The analysis drew on published epidemiological studies, national oral health surveys, and governmental oral health reports. No new primary data were collected, and no inferential modeling was performed.
2.2. Study Population
Data on dental caries prevalence for children aged 6–7 years (primary dentition) and 12 years (permanent dentition) were extracted following WHO guidelines using the DMFT/dmft indices [6]. In Germany, data were obtained from the National Oral Health Surveys conducted by the German Association for Youth Dental Care (DAJ e.V.). For Saudi Arabia, relevant studies meeting WHO criteria and reporting on these age groups were identified through targeted literature searches in PubMed, Scopus and Google Scholar that adhered to WHO diagnostic criteria for reporting caries prevalence in children. This standardized selection approach supports comparability between countries, although full one-to-one equivalence cannot be achieved because of differences in the health system structures and data availability.
2.3. Inclusion and Exclusion Criteria
The approach to data identification differed between Germany and Saudi Arabia due to differences in the availability of national epidemiological data. For Germany, caries data were obtained primarily from the standardized national oral health surveys conducted by the German Association for Youth Dental Care (DAJ e.V.), which provide population-based estimates for the WHO reference age groups of 6–7 and 12 years. Because DAJ surveys have been available only since the early 1990s, earlier caries trends were identified through peer-reviewed epidemiological studies reporting caries levels in the former East and West Germany.
In contrast to Germany, Saudi Arabia does not have a unified national surveillance system reporting age specific caries indicator. Therefore, a targeted literature search was conducted in PubMed, Scopus, and Google Scholar using combinations of the terms “dental caries,” “dmft,” “DMFT,” “children,” “schoolchildren,” “Saudi Arabia,” “oral health survey,” and “epidemiology.” Titles and abstracts were screened, and full texts of potentially eligible studies were reviewed.
Eligibility criteria: Included studies were required to report caries prevalence or mean dmft/DMFT values for schoolchildren of any school-age range, and to adhere to the WHO diagnostic criteria for caries assessment. Although data were extracted for all school-age groups, the 6–7-year and 12-year reference ages were used specifically for cross-country comparison between Germany and Saudi Arabia. Studies focusing on non-school-age children or on specific clinical populations, including children with special healthcare needs or those undergoing orthodontic treatment, were excluded to maintain comparability with the general schoolchild population. For Saudi Arabia, caries experience and prevalence data were extracted from studies published between 1982 and 2022, and all extracted data were cross-checked for accuracy. For Germany, the analysis incorporated all available national and regional data sources, including DAJ survey cycles from 1994/95 to 2016 and earlier epidemiological studies dating back to 1973.
2.4. Comparative Framework
A structured comparative framework was used to examine the differences in health system organization, preventive program structures, and oral health policies between Germany and Saudi Arabia. The comparison focused on domains emphasized in the WHO oral health system guidance, including governance and system structure, organization and coverage of school-based preventive programs, availability of individual preventive services, and national monitoring and surveillance mechanisms [7,8,9,10]. This approach allowed for the identification of system-level features that may be associated with variations in childhood caries outcomes across the two countries.
2.5. Data Analysis
Descriptive statistics were used to compare mean caries experience (dmft/DMFT) between Germany and Saudi Arabia across the standardized reference age groups (6–7 and 12 years). Longitudinal patterns in caries prevalence were examined using historical data where available, with particular attention to trends associated with national preventive strategies [11]. A thematic comparative approach was applied to evaluate the differences in healthcare system structures, legal frameworks, examiner calibration practices, and data documentation processes. Interpretive emphasis was placed on contextual factors that influence oral health outcomes, while acknowledging limitations such as regional data variability and inconsistent methodological standards, particularly within the Saudi Arabia literature.
3. Results
The findings of this comparative analysis highlight clear differences in the production, reporting, and processing of epidemiological data on dental caries among school-aged children in Germany and Saudi Arabia.
3.1. Historical Caries Trends in Germany
Caries prevalence among children in Germany has shown substantial improvements since the 1970s. In West Germany, DMFT scores among 13–14-year-olds peaked at 8.8 before declining to 5.1 by the 1980s. In East Germany, DMFT values remained relatively stable at 3.3 during the same period, followed by a modest reduction to 4.3 by 1992. Between 1983 and 1989, a 42% decrease in caries rates was observed among West German adolescents [12].
3.2. Current Caries Trends in Germany
Germany has seen significant improvements in children’s oral health over the past few decades. According to the German Association for Youth Dental Care (DAJ e.V.) [11], the mean DMFT score for 12-year-olds decreased by approximately 60%, from 2.44 in 1994/95 to 0.98 in 2004. Meanwhile, dmft scores for 6–7-year-olds declined by 25%, from 2.89 to 2.16 over the same period, further dropping to 1.87 by 2009.
DAJ’s 2016 report indicates that caries-free dentition among 6–7-year-olds more than doubled—from 20% in 1995 to 42.6% in 2016. Among 12-year-olds, the proportion with naturally healthy teeth rose markedly from 15.3% to 75.8% over the same timeframe [11]. The Figure 1 illustrates these trends using a line chart, depicting the steady decline in DMFT/dmft scores across both dentitions from 1973 to 2023. Although the IDZ and DAJ studies employed differing recruitment methodologies for participants and examiners, their findings show a high degree of consistency across time points. The latest data point from DAJ (2016) reports a mean DMFT of 0.44 for 12-year-olds, based on a positively selected sample from sixth grade [11]. After statistical adjustment for educational background bias (≈15%) [13], this corrected DMFT aligns with the 2016 and 2023 IDZ benchmark of 0.5 DMFT [14], indicating stabilization in caries reduction among school-aged children in Germany with a low caries prevalence of ~20%.
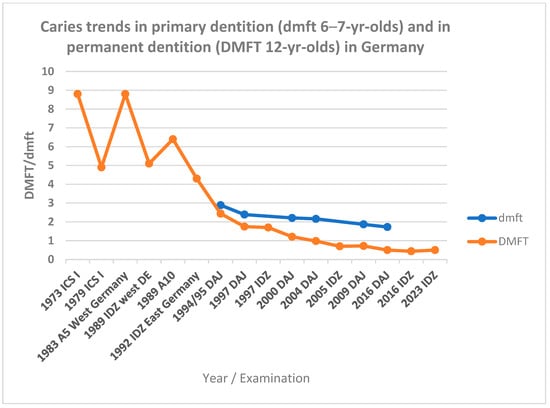
Figure 1.
Trends in caries prevalence in Germany (1973–2023): Mean dmft scores for primary dentition in 6–7-yr-olds in first grade and DMFT scores for permanent dentition mostly in 12-yr-olds. Abbreviations: ICS = International Caries Surveillance; DAJ = German Association for Youth Dental Care; IDZ = Institute of German Dentists. Data sources: [10].
Several federal states in Germany, such as Brandenburg and Thuringia, have established robust systems for collecting and publishing detailed caries data. These platforms provide annual updates based on compulsory dental examinations in kindergartens and schools, covering nearly all children up to 12 years of age and offering a comprehensive view of oral health trends. Although data collection was temporarily disrupted during the COVID-19 pandemic, the continuity and depth of these datasets remain exemplary and serve as valuable benchmarks for systemic evaluations and policy planning [11,13,14].
3.3. Historical Caries Trends in Saudi Arabia
In contrast to Germany’s standardized national surveillance system, Saudi Arabia lacks comprehensive population-wide data on dental caries prevalence. Most studies have been geographically limited, clinic-based, or age-specific, resulting in a fragmented epidemiological landscape and inconsistent indices across regions [3].
Despite these limitations, the available evidence spanning four decades consistently indicates high caries prevalence among Saudi children and adolescents. Early research conducted in 1982 reported a DMFT of 2.90 and 77.7% caries prevalence among 13–15-year-olds in Riyadh [15]. Through the 1990s, oral health surveys across five cities revealed DMFT scores ranging from 0.19 in 6-year-olds in Riyadh to 5.8 in 15-year-olds in Jeddah, with dmft values ranging from 2.1 in Rabagh to 6.4 in Madina [16].
Between 2000 and 2010, the observed DMFT rates varied significantly, from 0.16 in 6-year-olds in Riyadh to 7.35 in adolescents aged 15–19, while the dmft scores ranged from 2.68 in 12–13-year-olds to 7.77 in 5–7-year-olds in Tabuk [17].
From 2011 to 2022, this variability persisted. Studies reported DMFT scores from 0.26 among 6–7-year-olds in Jeddah to 7.0 among 15–19-year-olds in Al-Ahsa and dmft scores ranging from 1.4 in 12-year-olds in Madina to a high value of 9.0 in 4–6-year-olds in Jeddah [18,19,20,21]. Figure 2 presents the distribution of reported caries values across Saudi regions from 1982 to 2022.
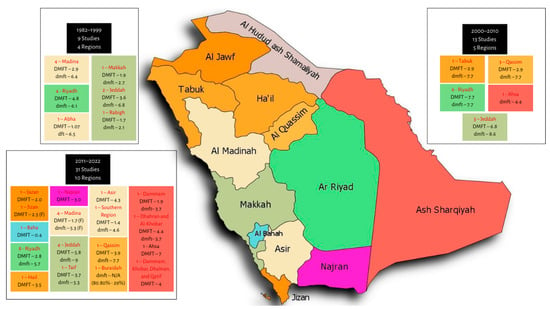
Figure 2.
Geographical distribution of dental caries data across Saudi Arabia based on studies conducted between 1982 and 2022. Data sources: [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39].
3.4. Legal and Policy Framework
Available national data from Germany, as reported in international analyses of the National Oral Health Survey [12,40,41] and data from the regional School Health Units in Qassim indicate that both Germany and Saudi Arabia have implemented school-based oral health programs targeting children at key developmental stages. Children aged 6–7 years (typically in first grade) and 12 years (typically in sixth grade) commonly receive preventive dental services in both countries. In addition, oral health examinations prior to school entry—conducted either during kindergarten or upon enrollment in first grade—are mandated by both German and Saudi health authorities.
3.4.1. Children’s Oral Health Legislation and Policies
Germany and Saudi Arabia differ substantially in the legal foundations and organizational structures governing children’s oral health. Germany operates under a legally codified preventive framework defined in the Social Code Book V (SGB V) [42], which mandates nationwide group and individual prophylaxis programs with age-specific entitlements. These include supervised brushing, fluoride varnish, fissure sealants, and structured early-detection examinations beginning in infancy. These entitlements are chronologically aligned with the child’s oral development, as illustrated in Figure 3, which maps Germany’s preventive services across key age intervals and corresponding SGB V provisions.
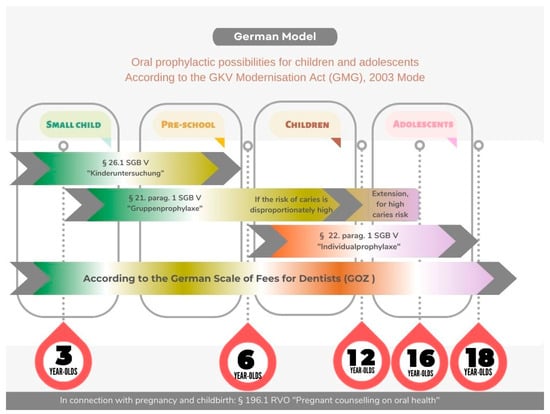
Figure 3.
German oral prophylactic pathways for children and adolescents, based on age-specific entitlements outlined in Social Code Book V (SGB V) and the GKV Modernisation Act (GMG), 2003. Source: IDZ, 2004; Federal Law Gazette (BGBL) of 19 November 2003, p. 2190 [42].
In Saudi Arabia, oral health services for children operate under general health provisions (Saudi Health Law Article 4) without equivalent statutory mandates for prophylaxis programs. Oversight is provided by the Ministry of Health’s Central Department of School Health, which delivers program-based services through regional Primary Health Care Centers (Saudi MOH Primary Health Care and Preventive Health Organization Structure, Figure 4). Programs such as the School Dental Prevention Program (SDPP) and the National Initiative for Preventing Dental Caries (NIPDC) provide fluoride application and screenings but function under programmatic rather than legislative frameworks. Germany additionally mandates early-detection examinations for children aged 6–72 months covered by public health insurance, as illustrated in Figure 5.
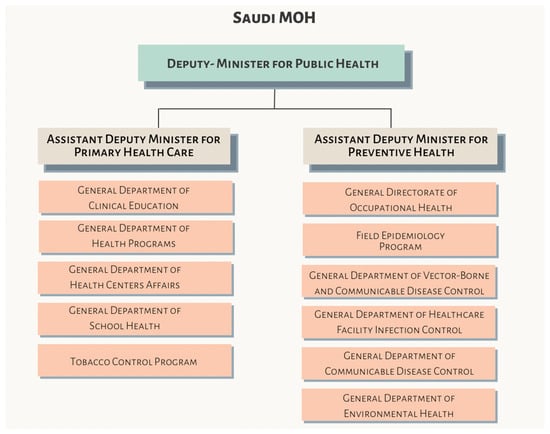
Figure 4.
Saudi MOH primary health care and preventive health organization structure. Source: Saudi Ministry of Health website: https://www.moh.gov.sa/en/Ministry/About/Pages/Organizational-Structure.aspx (accessed on 5 February 2026).
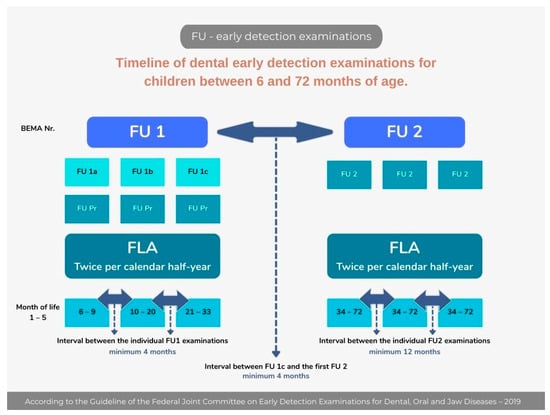
Figure 5.
Timeline of early dental examinations for children between 6 and 72 months of age covered by statuary health insurance [43,44,45].
Table 1 summarizes the key differences in children’s oral health legislation and preventive frameworks between Germany and Saudi Arabia.

Table 1.
Comparison of children’s oral health legislation and preventive frameworks in Germany and Saudi Arabia.
3.4.2. Oral Health Monitoring Projects and Working Teams
Beyond legislation, school-based oral health systems in both countries rely on monitoring institutions and interdisciplinary working teams. Germany and Saudi Arabia differ in how these monitoring structures are organized. In Germany, a coordinated national framework is led by the German Association for Youth Dental Care (DAJ) and the Institute of German Dentists (IDZ). These institutions define the methodological framework for the German National Oral Health Surveys (DMS), while data collection is carried out by regional working teams in each federal state. Examination procedures follow national guidance, with some regional variation in diagnostic criteria and calibration practices. In addition to the DMS, several specialized epidemiological initiatives—including SHIP [46]; Gekokids [47]; KiGGS [48]; Gesunde Zähne ein Leben lang [49]; IPKiSuN, MundZaRR [50], MuMi [51], MundPflege, InSEMaP and EFAFU [52], collect oral-health related data across different age groups and regions. The Robert Koch Institute (RKI), as the national public health authority, includes oral health indicators in federal health reporting. The organizational structure of the DAJ regional working teams is shown in Figure 6.

Figure 6.
Organizational concept for German dental group prophylaxis according to section 21, SGB V. Source: www.daj.de.
In Saudi Arabia, oral health monitoring activities are conducted through regional School Health teams and Primary Health Care Centers. The National Initiative for Preventing Dental Caries (NIPDC) outlines the responsibilities across the Ministry of Health, regional Health Affairs, Primary Health Care Centers, and schools [44]. Publicly available reports or datasets from NIPDC are not currently accessible. The operational structure of NIPDC, as presented in internal Ministry of Health materials, is illustrated in Figure 7.
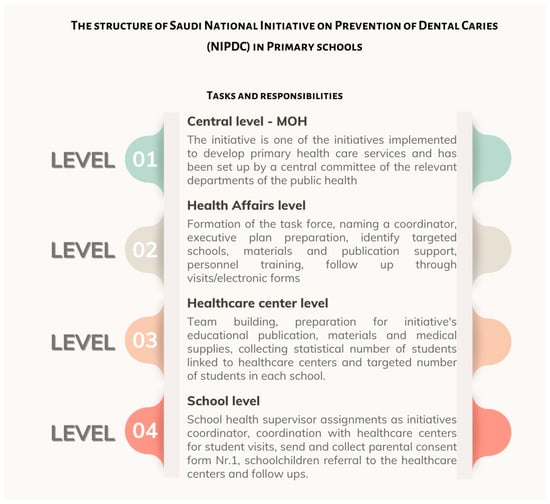
Figure 7.
Structure of the Saudi National Initiative for the Prevention of Dental Caries in Primary Schools, outlining tasks across MOH, regional health affairs, health centers, and schools. Source: Presentation by Dr. Saeed M. S. Almohammadi (in Arabic) [53].
To provide a structured comparison of national child oral health projects and their monitoring tools, Table 2 contrasts the DAJ- and IDZ-supported projects in Germany with the NIPDC framework in Saudi Arabia across key domains such as surveillance, data standards, dissemination, and project continuity.
Table 2.
Comparison of national child oral health project structures and monitoring frameworks in Germany and Saudi Arabia.
3.4.3. Calibration of Examiners
Germany and Saudi Arabia differ in the standardization and transparency of examiner calibration within child oral-health programs. Germany implements structured calibration protocols, with DAJ reporting inter-examiner agreement (κ ≥ 0.65) among 482 calibrated dentists. According to DAJ (2016), a total of 482 dentists underwent online calibration for dental screening [11]. These reliability scores are reported in the DAJ calibration data and are used within Germany’s national oral health surveillance framework [33,34].
By contrast, Saudi Arabia’s National Initiative for the Prevention of Dental Caries (NIPDC) has no publicly available documentation describing examiner calibration protocols. Despite its nationwide implementation, there is no evidence of standardized training, reliability assessments, or formal inter-examiner calibration within the available sources. This absence is documented in the available sources, and no information is provided on whether diagnostic practices are applied consistently across regions, although dmft/DMFT examinations are generally robust.
3.4.4. Data Management
Germany and Saudi Arabia differ in the maturity, transparency, and structure of their oral health data management systems. Germany operates a digitally integrated infrastructure that supports standardized data entry, cross-regional comparability, and routine evaluation. Dental services across federal states employ established software platforms—such as ISGA (InformationsSystem GesundheitsAmt, Computer Zentrum Strausberg GmbH, Strausberg, Germany), Gudental (software.house informationstechnik AG. 24105 Kiel, Germany), Micropro (Mikroprojekt GmbH, Kaiserslautern, Germany), and Octoware®NT (easy-soft GmbH, Dresden, Germany)—which enable the systematic recording of demographic variables, examination findings, and program-level indicators. This digital infrastructure also supports longitudinal linkage with national surveys (e.g., DAJ) and facilitates dissemination through regular public reporting [11]. Conversely, Saudi Arabia’s National Initiative for the Prevention of Dental Caries (NIPDC) has no publicly available information describing its data management protocols, including software systems, integration platforms, or standardized recording procedures. Despite formal inquiries, no documentation has been disclosed regarding data flow, quality-control mechanisms, or interoperability across regions. This absence of publicly available documentation means that information on data completeness, program performance, or regional comparability cannot be assessed from the available sources, limiting the ability to compare outcomes across regions. The lack of publicly accessible datasets also precludes trend analysis, dissemination, and assessment of goal attainment.
4. Discussion
This section synthesizes the key findings from the comparative analysis of Germany and Saudi Arabia’s children’s oral health and integrates contextual information that supports interpretation of the epidemiological results. By combining caries trends, legal frameworks, operational structures, and governance mechanisms, the discussion highlights how systemic organization shapes preventive coverage, data quality, and long-term outcomes [54].
4.1. Caries Epidemiology
Global oral health surveillance began in the late 1960s under the World Health Organization (WHO) leadership, and early international mapping revealed marked disparities in childhood caries between industrialized and developing countries [9].
In Germany, caries monitoring was formally introduced in the 1970s through participation in WHO’s International Collaborative Study (ICS I, 1973–1979), which documented elevated DMFT scores among adolescents [6,55]. Subsequent national surveys have tracked a steady decline in caries experience, with recent data indicating a 90% reduction over the past 45 years [56]. This sustained improvement may be associated with Germany’s legally mandated preventive programs in group and individual settings, standardized diagnostic criteria, calibrated examiners and continuous long-term surveillance [5,57,58]. Despite slight methodological variations between institutions, DMFT remains a reliable and comparable indicator across sources, reinforcing the robustness of Germany’s epidemiological credibility [40].
In contrast, Saudi Arabia faces persistent challenges in oral health data collection and has not participated in global initiatives like WHO ICS. Although some studies report declining dmft scores over the past 10–15 years [39,40,41,42], many combine broad age ranges, potentially confounding age-specific trends. Other investigations—such as Al-Banyan et al. (2000) and Al-Rafee et al. (2019)—continue to report alarmingly high caries prevalence rates in children and adolescents [59,60]. These inconsistencies reflect the absence of calibrated national surveys and highlight the need for a cohesive oral health strategy that establishes reliable baseline indicators, enabling trend analysis, and guiding evidence-based prevention efforts in Saudi Arabia.
4.2. Legal Mapping
Legal mapping provides a framework to understand how preventive responsibilities are distributed across institutions and how policies evolved over time [61]. In Germany, preventive dental care is a statutory entitlement enshrined in the Social Code Book V (§21 SGB V). This legal foundation ensures consistent service delivery, regular evaluation, and public accountability. Institutions such as the Federal Joint Committee (G-BA) and the German Association for Youth Dental Care (DAJ) operate under clearly defined mandates, supported by transparent scientific methods and rigorous quality control [11].
In contrast, Saudi Arabia’s legal–epidemiological framework remains underdeveloped. According to Al-Ansari et al. (2019), “no government body is assigned the task of collecting oral health data and in most cases, information about caries is available through published scientific publications without national oral health surveys; mostly due to logistic difficulties than lack of resources [62]”. This finding aligns with Quadri et al. (2018), who observed that supervision of school oral health activities and regular monitoring visits appear limited or insufficiently structured [63].
Saudi Arabia’s Vision 2030 offers a strategic opportunity to strengthen oral health governance through national capacity-building and enhanced institutional transparency. The Vision 2030 Achievements Booklet reports a 65% increase in healthcare professionals between 2016 and 2020, reflecting substantial investment in workforce development. Aldossary (2022) emphasizes Vision 2030’s supportive foundation for healthcare system advancement [64], while Mani and Goniewicz (2024) highlight its transformative impact on governance, digital health, and systemic reform [65].
Despite this progress, establishing a legal basis for school-based oral health—including clearly defined roles, national data mandates, and sustained funding—remains critical. Without legislative codification, programs like the National Initiative for the Prevention of Dental Caries (NIPDC) risk fragmentation, regional inconsistency, and limited accountability. This concern is echoed in recent implementation research on the Child Oral Health Initiative, which underscores how policy innovation and systemic coordination were essential to overcoming fragmented service delivery and achieving preventive care goals [66].
4.3. Operational Structures and Monitoring Capacity
Germany’s operational model is characterized by a coordinated national surveillance ecosystem. DAJ and IDZ provide methodological guidance for national oral health surveys (DMS), while regional working teams conduct standardized examinations. Although minor regional variations exist, Germany benefits from harmonized diagnostic criteria (BZÖG), calibrated examiners, and a long-standing research infrastructure that supports longitudinal monitoring.
Saudi Arabia’s monitoring capacity remains fragmented. School Health teams and Primary Health Care Centers conduct screenings without a unified national surveillance system, leading to substantial variation in diagnostic criteria, examiner calibration, and reporting pathways. Where examiner calibration is not standardized, inter-examiner variability may increase and contribute to regional differences in diagnostic consistency; by contrast, Germany’s calibrated workforce supports more reliable and comparable surveillance data. The NIPDC represents the most structured national attempt to coordinate preventive activities, but the absence of publicly available reports, datasets, or methodological documentation limits evaluation of its effectiveness. The lack of centralized coordination and longitudinal surveillance restricts the ability to monitor national trends, assess program performance, or align preventive strategies with international benchmarks.
4.4. Data Management and Digital Infrastructure
Germany operates a digitally integrated data infrastructure that supports standardized data entry, cross-regional comparability, and timely evaluation. Software platforms such as ISGA, Gudental, Micropro, and Octoware/Easy-Soft enable systematic recording of demographic variables, examination findings, and program indicators [11]. This digital ecosystem minimizes documentation errors, facilitates linkage with national surveys, and supports regular public reporting, thereby strengthening the validity and comparability of national surveillance outputs.
Conversely, Saudi Arabia’s NIPDC lacks publicly available information on data-management protocols, software systems, or quality-control mechanisms. Despite formal inquiries, no documentation has been disclosed regarding data flow, interoperability, or regional standardization. This absence of transparency limits the ability to assess data completeness, evaluate program performance, compare outcomes across regions, or conduct trend analysis—a component essential for evidence-based policy development.
4.5. Strengths and Limitations
This study presents several strengths, notably offering the first comparative review of legal frameworks underpinning the implementation of school-based oral health policies in Germany and Saudi Arabia. It delivers a structured assessment of prevention strategies, supported by the integration of previously unpublished insights from Saudi health and education authorities. Notable contributions include
- Contextual observations on service outreach and school health unit involvement in local school-health programs;
- Observational insights on oral health program distribution at the local level;
- Comparative analysis integrating national surveillance benchmarks from Germany.
Such inclusions strengthen the study’s empirical contribution and provide fresh insight into Saudi Arabia’s evolving oral health landscape.
However, limitations must be acknowledged. In Saudi Arabia, data accuracy on caries prevalence and prevention efforts is challenged by fragmented reporting, lack of calibrated examiners, and inconsistent digital infrastructure—a concern documented in national implementation studies [23]. These methodological disparities contrast with Germany’s calibrated workforce, standardized electronic surveillance systems and widespread mandatory oral examinations [67]. Additionally, variability in sample sizes and age classification—such as first-grade cohorts in Saudi Arabia ranging from 5 to 8 years old—affects cross-national comparability and limits age-specific analysis.
Despite these constraints, the study identifies a consistently higher caries burden in Saudi Arabia, underscoring the need for improved surveillance, legal codification, and targeted prevention strategies. While data asymmetry precludes direct statistical comparison, the structural analysis may offer valuable guidance for future policy refinement and system-building efforts.
4.6. Suggestions
The absence of a nationally coordinated children’s oral health strategy in Saudi Arabia appears to have contributed to fragmented service delivery and inconsistent monitoring across sectors. Limited integration between key ministries and providers—particularly the Ministry of Health and the Ministry of Education—may weaken the implementation and sustainability of preventive dental initiatives for children. Current school-based programs vary in scope, reach, and follow-up mechanisms, which may contribute to unequal access and persistent gaps in oral health outcomes.
Drawing on international benchmarks, valuable insights can be extracted from Germany’s centralized oral health system. The German model, implemented through the German Association for Youth Dental Care (DAJ e.V.) and supported by national legislation, is cohesive and unified, helping to ensure more equitable access to preventive dental care for children, irrespective of school sector or governing authority. This structure supports consistent service delivery, standardized monitoring, and better nationwide health equity. In contrast, Saudi Arabia’s oral health framework remains sectoral and segmented, with fragmented delivery mechanisms and parallel programs overseen by different ministries and providers. This decentralized structure may underlie the observable gaps and inconsistencies in service coverage and evaluation processes, limiting the reach and long-term impact of school-based initiatives. Integrating lessons from the German model may offer a strategic opportunity for Saudi policymakers to develop a more coordinated and equitable oral health framework. Emphasizing national alignment, legislative support, and inter-ministerial integration could help pave the way for a sustainable system that improves access to preventive care for all schoolchildren. It may be assumed that integrated data governance within pediatric dental programs enables cross-sectoral collaboration, improves transparency, and supports value-based health financing models in oral health. This hypothesis is supported by findings from Germany, where coordinated data-entry protocols across school dental programs enabled consistent examination standards and centralized access to oral health indicators. Consequently, a proposed pilot in Qassim could replicate this by implementing structured examination workflows, digitizing oral-examinations records, and building an intersectoral oral-health coalition. This model would foster transparency, accelerate evidence-based preventive policy formulation, and strengthen accountability across providers, educators, and policymakers.
Reforms must be evidence-based and contextually tailored to Saudi Arabia’s governance structures and social norms. Priorities include formalizing inter-ministerial roles, instituting standardized surveillance protocols, and adopting secure digital tools for routine screening and reporting. Figure 8 consolidates these recommendations into a single logic model that links inputs and activities to measurable outputs and short- and long-term outcomes, offering a practical blueprint for phased implementation and policy evaluation.
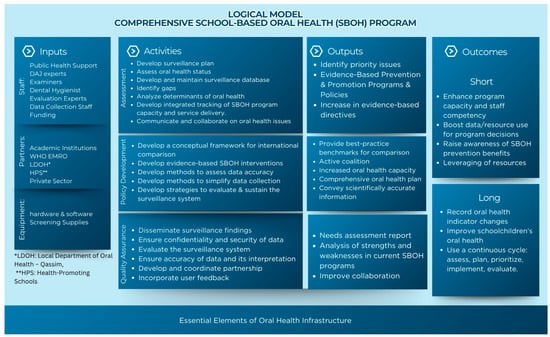
Figure 8.
Proposed logic model for a comprehensive Saudi School-based oral health program (modified framework).
5. Conclusions
This comparative analysis underscores that the systemic structure, not merely the existence of services, is a pivotal determinant of caries prevalence among children. Germany’s success stems from its legally mandated age-specific oral health programs, calibrated workforce, and a unified data strategy. These elements collectively ensure accountability, equity, and measurable outcomes. By contrast, Saudi Arabia’s fragmented framework results in diagnostic variability, uneven implementation, and limited policy traction despite considerable investment.
It appears that the means for transition from scattered initiatives to sustained impact are present in Saudi Arabia, but oral health should be embedded into national legislation, and interoperable digital surveillance platforms should be made available for regular examination by calibrated examiners. These reforms should be augmented by strategic coalitions and evidence-informed interventions across regions. Well-resourced areas such as Qassim can serve as innovation hubs to pilot scalable programs, implement AI-integrated school–health models, and support nonprofit research centers that inform national policy.
Inspired by international best practices—as Germany itself learned from Scandinavian prevention models—the path forward requires more than replication. It calls for adaptation that respects local contexts while aligning with global benchmarks. Future research should not only fill epidemiological gaps but also rigorously assess structural reforms. Only through such systemic re-engineering can Saudi Arabia progress toward equitable, preventive oral health care for every child.
Author Contributions
Conceptualization, Y.M.A., C.H.S. and J.S.; methodology, Y.M.A. and J.S.; formal analysis, Y.M.A.; investigation, Y.M.A.; data curation, Y.M.A.; writing—original draft preparation, Y.M.A.; writing—review and editing, J.S. and C.H.S.; supervision, C.H.S.; visualization, Y.M.A.; project administration, Y.M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study, because it involved secondary analysis of previously published anonymized data and did not involve the collection of new data from human participants.
Informed Consent Statement
Patient consent was waived, because the study used publicly available anonymized data from published sources, with no direct involvement of human subjects.
Data Availability Statement
All data used in this study are derived from previously published sources, including national oral health surveys, peer reviewed literature, and official reports. All datasets are publicly available as cited in the references. No new or unpublished data were generated or analyzed in this study.
Acknowledgments
The first author gratefully acknowledges the regional School Health Units in Qassim for providing access to unpublished data and frameworks that informed comparative analysis.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization WHO|Oral Health. Available online: https://www.who.int/health-topics/oral-health (accessed on 27 February 2026).
- Tudoroniu, C.; Popa, M.; Iacob, S.M.; Pop, A.L.; Năsui, B.A. Correlation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits among 10 to 19-Year-Old Cluj-Napoca Romanian Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 6923. [Google Scholar] [CrossRef]
- Al Agili, D.E. A Systematic Review of Population-Based Dental Caries Studies among Children in Saudi Arabia. Saudi Dent. J. 2013, 25, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health; Saudi Arabia. Dental Caries: Facts and Guidelines. Available online: https://www.moh.gov.sa/en/awarenessplateform/OralHealth/Pages/DentalCaries.aspx (accessed on 27 February 2026).
- Chen, M.; Andersen, R.; Barmes, D. Comparing Oral Health Care Systems: A Second International Collaborative Study; World Health Organization: Geneva, Switzerland; University of Chicago Center for Health Administration Studies: Chicago, IL, USA, 1997; ISBN 9241561882. [Google Scholar]
- Petersen, P.E.; Baez, R.J.; World Health Organization (Eds.) Oral Health Surveys—Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013; ISBN 9789241548649. [Google Scholar]
- Petersen, P.E. The World Oral Health Report 2003: Continuous Improvement of Oral Health in the 21st Century—The Approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Eaton, K.; Yusuf, H.; Vassallo, P. The WHO Global Oral Health Action Plan 2023–2030. Community Dent. Health 2023, 40, 68–69. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Bourgeois, D.; Bratthall, D.; Ogawa, H. Oral Health Information Systems—Towards Measuring Progress in Oral Health Promotion and Disease Prevention. Bull. World Health Organ. 2005, 83, 686–693. [Google Scholar]
- Almalki, M.; Fitzgerald, G.; Clark, M. Health Care System in Saudi Arabia: An Overview. East. Mediterr. Health J. 2011, 17, 784–793. [Google Scholar] [CrossRef]
- Team DAJ. Epidemiologische Begleituntersuchungen Zur Gruppenprophylaxe 2016; Deutsche Arbeitsgemeinschaft für Jugendzahnpflege e.V. (DAJ): Bonn, Germany, 2017. [Google Scholar]
- Splieth, C.H.; Santamaria, R.M.; Basner, R.; Schüler, E.; Schmoeckel, J. 40-Year Longitudinal Caries Development in German Adolescents in the Light of New Caries Measures. Caries Res. 2019, 53, 609–616. [Google Scholar] [CrossRef]
- Schmoeckel, J.; Wahl, G.; Santamaría, R.M.; Basner, R.; Schankath, E.; Splieth, C.H. Influence of School Type and Class Level on Mean Caries Experience in 12-Year-Olds in Serial Cross-Sectional National Oral Health Survey in Germany—Proposal to Adjust for Selection Bias. Int. J. Environ. Res. Public Health 2024, 21, 467. [Google Scholar] [CrossRef]
- Schmoeckel, J.; Santamaría, R.M.; Basner, R.; Schüler, E.; Splieth, C.H. Introducing a Specific Term to Present Caries Experience in Populations with Low Caries Prevalence: Specific Affected Caries Index (SaC). Caries Res. 2019, 53, 527–531. [Google Scholar] [CrossRef]
- Younes, S.A.E.S.; El-Angbawi, M.F. Dental Caries Prevalence in Intermediate Saudi Schoolchildren in Riyad. Community Dent. Oral Epidemiol. 1982, 10, 74–76. [Google Scholar] [CrossRef]
- Al-Shammery, A.R. Caries Experience of Urban and Rural Children in Saudi Arabia. J. Public Health Dent. 1999, 59, 60–64. [Google Scholar] [CrossRef]
- Aldosari, A.M.; Akpata, E.S.; Khan, N. Associations among Dental Caries Experience, Fluorosis, and Fluoride Exposure from Drinking Water Sources in Saudi Arabia. J. Public Health Dent. 2010, 70, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Farooqi, F.A.; Khabeer, A.; Moheet, I.A.; Khan, S.Q.; Farooq, I.; Arrejaie, A.S. Prevalence of Dental Caries in Primary and Permanent Teeth and Its Relation with Tooth Brushing Habits among Schoolchildren in Eastern Saudi Arabia. Saudi Med. J. 2015, 36, 737. [Google Scholar] [CrossRef]
- Al-shammery, A.R.; Saeed, H.I.; Khan, N. Caries Increment Over A 3-Year Period in Adolescent Children in Riyadh, Saudi Arabia. Saudi Dent. J. 1996, 8, 69–76. [Google Scholar]
- Alshiha, S.A.; Alwayli, H.M.; Hattan, M.A.; Alfraih, Y.K.; Alamri, A.A.; Aldossary, M.S. Prevalence of Dental Caries among Elementary School Girls in Riyadh, Kingdom of Saudi Arabia: A Cross-Sectional Survey. J. Oral Health Community Dent. 2017, 11, 29–33. [Google Scholar] [CrossRef]
- Alwabari, M.A.; Alquraini, A.M.; Albakheet, A.S.; Alsaljah, R.S.; Alkuhl, H.; Ashraf, J.; Alotaibi, A.R.; Bokhari, S.A.H. Oral Health Status and Use of Sugary Products among Adolescents in Urban and Rural Schools in Al-Ahsa, Saudi Arabia. Saudi J. Oral Sci. 2021, 8, 14–21. [Google Scholar] [CrossRef]
- AlDosari, A.M.; Wyne, A.H.; Akpata, E.S.; Khan, N.B. Caries Prevalence and Its Relation to Water Fluoride Levels among Schoolchildren in Central Province of Saudi Arabia. Int. Dent. J. 2004, 54, 424–428. [Google Scholar] [CrossRef]
- Alhabdan, Y.A.; Albeshr, A.G.; Yenugadhati, N.; Jradi, H. Prevalence of Dental Caries and Associated Factors among Primary School Children: A Population-Based Cross-Sectional Study in Riyadh, Saudi Arabia. Environ. Health Prev. Med. 2018, 23, 60. [Google Scholar] [CrossRef]
- Farsi, N. Dental Caries in Relation to Salivary Factors in Saudi Population Groups. J. Contemp. Dent. Pract. 2008, 9, 16–22. [Google Scholar] [CrossRef]
- Elfaki, N.K.; Elsheikh Elgarrai, A.S.; Shwail, A.I.; Brair, S.L.; Alsheikh, M.A. Prevalence of Dental Caries among Primary School Attendees in Najran-Saudi Arabia. IOSR J. Dent. Med. Sci. 2014, 13, 37–41. [Google Scholar] [CrossRef]
- Al-wazzan, K.A. Dental Caries Prevalence in 6–7 Year-Old Schoolchildren in Riyadh Region: A Comparative Study with the 1987 Oral Health Survey of Saudi Arabia Phase I. Saudi Dent. J. 2004, 16, 54–60. [Google Scholar]
- Alzahrani, A.A. The Oral Health Status and Attitudes of Saudi Adolescent Male Students in Albaha Province: A Cross-Sectional Study. Adv. Dent. Oral Health 2018, 10, 10–19080. [Google Scholar] [CrossRef]
- Al-Zahrani, A.; Al-Qahtani, M.; Al-Barti, M.; Bakhurji, E.A. Dietary Determinants of Dental Caries Prevalence and Experience in Saudi Schoolchildren: Frequency versus Quantity. Sci. World J. 2022, 2022, 5447723. [Google Scholar] [CrossRef] [PubMed]
- Aqeeli, A.; Alsharif, A.T.; Kruger, E.; Tennant, M.; Bakeer, H. Caries Prevalence and Severity in Association with Sociodemographic Characteristics of 9-to-12-Year-Old School Children in Al-Madinah, Saudi Arabia. Saudi Dent. J. 2021, 33, 897–903. [Google Scholar] [CrossRef]
- Abdulkareem Al Zahidy, H.; Ahmed Bafail, K.; Mustafa Saidi, K.; Saleh Fairag, A.; Khalid Enayah, S.; Sulaiman Alsayegh, A.; khalid Abdullah, N.; Mohammed Alwah, S.; Saleh Alharthi, A.; Sameer Sindi, N.; et al. Prevalence of Dental Caries among Children in Jeddah-Saudi Arabia-2015. EC Dent. Sci. 2017, 8, 15–20. [Google Scholar]
- Gokul, K.; Kasabah, S.; Alrubaian, A.M.; Alrubaian, A.M.; Zahi, N.; Al Rashidi, B. Prevalence of Dental Caries Among Girl Students of Primary School in Buraydah City. Int. J. Contemp. Res. Rev. 2018, 9, 10400–10413. [Google Scholar]
- Khan, N.B.; Al-Ghannam, N.A.; Al-Shammery, A.R.; Wyne, A.H. Caries in Primary School Children: Prevalence, Severity and Pattern in Al-Ahsa, Saudi Arabia. Saudi Dent. J. 2001, 13, 71–74. [Google Scholar]
- Kotha, S.B.; Terkawi, S.A.; Mubaraki, S.A.; Al Saffan, A.D.; Kotha, S.L.; Mallineni, S.K. Association between Body Mass Index (BMI) and Dental Caries among 6–12-Year-Old School Children. Children 2022, 9, 608. [Google Scholar] [CrossRef]
- Gandeh, M.B.S.; Milaat, W.A. Dental Caries among Schoolchildren: Report of a Health Education Campaign in Jeddah, Saudi Arabia. East. Mediterr. Health J. 2000, 6, 396–401. [Google Scholar] [CrossRef]
- Madhan, G.; Togoo, R.; Abumelha, M.; Aljahdal, M.; Alkahtani, Z.; Ain, T. Intelligence Quotient and Dental Caries: An Analytical Cross-Sectional Study among Saudi Arabian Children. Niger. J. Basic Clin. Sci. 2021, 18, 42–47. [Google Scholar] [CrossRef]
- Mahrous, M.S.; Bhayat, A.; Hifnawy, T.; Bakeer, H.; Ahmad, M.S. Can the Prevalence of Dental Caries Be Used as an Indicator of the Quality of Dental Services? A Cross-Sectional Study among Children in Almadinah Almunawwarah, KSA. J. Taibah Univ. Med. Sci. 2016, 11, 41–45. [Google Scholar] [CrossRef]
- Mannaa, A.; Carlén, A.; Lingström, P. Dental Caries and Associated Factors in Mothers and Their Preschool and School Children—A Cross-Sectional Study. J. Dent. Sci. 2013, 8, 101–108. [Google Scholar] [CrossRef]
- Magda, M.; Shahid, A.; Cynthia, P. Comparison of Caries in 6-7 Year Old Saudi Girls Attending Public and Armed Forces Schools in Riyadh, Saudi Arabia. Saudi Dent. J. 2000, 12, 33–36. [Google Scholar]
- Quadri, M.F.A.; Hakami, B.M.; Hezam, A.A.A.; Hakami, R.Y.; Saadi, F.A.; Ageeli, L.M.; Alsagoor, W.H.; Faqeeh, M.A.; Dhae, M.A. Relation between Dental Caries and Body Mass Index- for-Age among Schoolchildren of Jazan City, Kingdom of Saudi Arabia. J. Contemp. Dent. Pract. 2017, 18, 277–282. [Google Scholar] [CrossRef]
- Santamaria, R.M.; Schmoeckel, J.; Basner, R.; Schüler, E.; Splieth, C.H. Caries Trends in the Primary Dentition of 6- to 7-Year-Old Schoolchildren in Germany from 1994 to 2016: Results from the German National Oral Health Surveys in Children. Caries Res. 2019, 53, 659–666. [Google Scholar] [CrossRef]
- Santamaría, R.M.; Splieth, C.H.; Basner, R.; Schankath, E.; Schmoeckel, J. Caries Level in 3-Year-Olds in Germany: National Caries Trends and Gaps in Primary Dental Care. Children 2024, 11, 1426. [Google Scholar] [CrossRef]
- Bundesministerium der Justiz Sozialgesetzbuch (SGB) Fünftes Buch (V)—Gesetzliche Krankenversicherung—(Artikel 1 Des Gesetzes v. 20. Dezember 1988, BGBl. I S. 2477) § 21 Verhütung von Zahnerkrankungen (Gruppenprophylaxe). Available online: https://www.gesetze-im-internet.de/sgb_5/__21.html (accessed on 3 August 2025).
- Ministry of National Guard Health Affairs School Dental Prevention Programs. Available online: https://ngha.med.sa/English/MedicalCities/AlRiyadh/SDPP/Pages/sdpps.aspx (accessed on 27 July 2025).
- Ministry of Health; Saudi Press Agency. National Initiative on Prevent Tooth Caries. Available online: https://www.moh.gov.sa/en/Ministry/Projects/tooth-decay/Pages/default.aspx (accessed on 27 July 2025).
- Public Health Authority; National Committee of Periodic Health Examination. Saudi Clinical Preventive Guideline, 3rd ed.; Saudi Public Health Authority (Weqaya): Riyadh, Saudi Arabia, 2023. [Google Scholar]
- Schmoeckel, J.; Haq, J.; Samietz, S.; Santamaría, R.M.; Mourad, M.S.; Völzke, H.; Kocher, T.; Splieth, C.H.; Holtfreter, B. Ten-Year Trends in DMF-S and DMF-T in a Northeast German Adult Population. J. Dent. 2021, 111, 103727. [Google Scholar] [CrossRef]
- Splieth, C.H.; Christiansen, J.; Foster Page, L.A. Caries Epidemiology and Community Dentistry: Chances for Future Improvements in Caries Risk Groups. Outcomes of the ORCA Saturday Afternoon Symposium, Greifswald, 2014. Part 1. Caries Res. 2016, 50, 9–16. [Google Scholar] [CrossRef]
- Krause, L.; Kuntz, B.; Schenk, L.; Knopf, H. Oral Health Behaviour of Children and Adolescents in Germany Results of the Cross-Sectional KiGGS Wave 2 Study and Trends. J. Health Monit. 2018, 3, 38. [Google Scholar]
- Splieth, C.H. Gesunde Zähne ein Leben Lang—8-Jahres-Evaluation 2012: Kariesintensivprophylaxe für Risikokinder in Mecklenburg-Vorpommern; Universität Greifswald: Greifswald, Germany, 2012. [Google Scholar]
- Hertrampf, K.; Schlattmann, P.; Meyer, G.; Gassmann, G.; Abraham, J.; Hammen, V.; Schwendicke, F. Oral Health Improvement for Nursing Home Residents through Delegated Remotivation and Reinstruction (MundZaRR Study): Study Protocol of a Cluster-Randomised Controlled Trial. BMJ Open 2020, 10, e035999. [Google Scholar] [CrossRef]
- Spinler, K.; Weil, M.T.; Valdez, R.; Walther, C.; Dingoyan, D.; Seedorf, U.; Heydecke, G.; Lieske, B.; Kofahl, C.; Aarabi, G. Oral Health Literacy of Persons with Migration Background—First Results of the MuMi Study. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2021, 64, 977. [Google Scholar] [CrossRef] [PubMed]
- Huettig, F.; Schwendicke, F. Versorgungsforschung in Der Zahnmedizin in Deutschland. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2021, 64, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Almohammadi, S.M. (Strategic Management Society, Chicago, IL, USA). National Initiative for Pediatric Dental Caries (NIPDC): Overview and Data Presentation. Unpublished presentation, 2023. [Google Scholar]
- Listl, S.; Baltussen, R.; Carrasco-Labra, A.; Carrer, F.C.; Lavis, J.N. Evidence-Informed Oral Health Policy Making: Opportunities and Challenges. J. Dent. Res. 2023, 102, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Splieth, C.; Meyer, G. Factors for Changes of Caries Prevalence among Adolescents in Germany. Eur. J. Oral Sci. 1996, 104, 444–451. [Google Scholar] [CrossRef]
- Jordan, R.A.; Bodechtel, C.; Hertrampf, K.; Hoffmann, T.; Kocher, T.; Nitschke, I.; Schiffner, U.; Stark, H.; Zimmer, S.; Micheelis, W. The Fifth German Oral Health Study (Fünfte Deutsche Mundgesundheitsstudie, DMS V)—Rationale, Design, and Methods. BMC Oral Health 2014, 14, 161. [Google Scholar] [CrossRef]
- Schmoeckel, J.; Santamaría, R.M.; Basner, R.; Schankath, E.; Splieth, C.H. Oral Health Trends in Children: Results from the Epidemiological Surveys Accompanying Group Prophylaxis in Germany. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2021, 64, 772. [Google Scholar] [CrossRef]
- Ziller, S.; Jordan, A.R.; Oesterreich, D. Mundgesundheitsziele Für Deutschland 2030: Karies Und Parodontitis Weiter Reduzieren Sowie Prävention Verbessern. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2021, 64, 821–829. [Google Scholar] [CrossRef]
- Al-Banyan, R.A.; Echeverri, E.A.; Narendran, S.; Keene, H.J. Oral Health Survey of 5–12-Year-Old Children of National Guard Employees in Riyadh, Saudi Arabia. Int. J. Paediatr. Dent. 2000, 10, 39–45. [Google Scholar] [CrossRef]
- Al-Rafee, M.A.; Al Shammery, A.R.; Al Rumikan, A.S.; Pani, S.C. A Comparison of Dental Caries in Urban and Rural Children of the Riyadh Region of Saudi Arabia. Front. Public Health 2019, 7, 195. [Google Scholar] [CrossRef]
- WHO. WHO Information Series on School Health. In Oral Health Promotion: An Essential Element of a Health-Promoting School; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Al-Ansari, A. Prevalence, Severity, and Secular Trends of Dental Caries among Various Saudi Populations: A Literature Review. Saudi J. Med. Med. Sci. 2014, 2, 142–150. [Google Scholar] [CrossRef]
- Quadri, M.F.A.; Shubayr, M.A.; Hattan, A.H.; Wafi, S.A.; Jafer, A.H. Oral Hygiene Practices among Saudi Arabian Children and Its Relation to Their Dental Caries Status. Int. J. Dent. 2018, 2018, 3234970. [Google Scholar] [CrossRef]
- Aldossary, M.S. Dental Governance and the Saudi Vision 2030: A Narrative Review. Saudi J. Health Syst. Res. 2022, 3, 35–41. [Google Scholar] [CrossRef]
- Mani, Z.A.; Goniewicz, K. Transforming Healthcare in Saudi Arabia: A Comprehensive Evaluation of Vision 2030’s Impact. Sustainability 2024, 16, 3277. [Google Scholar] [CrossRef]
- Alkarimi, H.A.; Jawadi, A.; Tayeb, S.; Ismail, R.; AlShareef, E.J.; Sherbini, N. Implementing the Child Oral Health Initiative (COHI): Improving Access to Preventive Dental Care to Achieve Saudi Vision 2030 Healthcare Goals. BMJ Open Qual. 2025, 14, e003070. [Google Scholar] [CrossRef]
- Samietz, S.; Borof, K.; Hertrampf, K.; Aarabi, G.; Ciardo, A.; Finke, H.; Hagenfeld, D.; Kühnisch, J.; Rütters, M.; Baumeister, S.-E.; et al. Dental and Oral Health Assessments in the German National Cohort (NAKO). BMC Oral Health 2025, 25, 149. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.