Highlights
What are the main findings?
- Video game-based interventions are effective tools for increasing visual acuity in children with amblyopia.
- The combination of video games and traditional patching therapy demonstrates superior effectiveness compared to patching alone.
What are the implications of the main findings?
- Clinicians should consider incorporating video games as an adjuvant to traditional patching.
- Non-immersive systems represent a clinically viable and effective tool, suggesting that specialized or expensive immersive hardware is not strictly necessary to achieve positive visual improvements.
Abstract
Background: Novel approaches such as video games represent a promising tool in increasing visual acuity (VA) in children with amblyopia. The aim was to determine the effectiveness of video game-based interventions (VGBIs) in increasing VA in children with amblyopia. Secondarily, to estimate safety, satisfaction, and compliance with VGBIs. Methods: According to the PRISMA guidelines, a systematic review with meta-analysis (SRMA) was conducted, including studies retrieved from PubMed Medline, SCOPUS, WOS, CINAHL, and PEDro without publication date and language restrictions. We included randomized controlled trials (RCTs) and pilot RCTs, comprising children with amblyopia, that compared the effectiveness of VBGI vs. others in improving VA. Pooled effect was estimated with the Cohen’s standardized mean difference (SMD) and its 95% confidence interval (95%CI). Results: Twenty-one RCTs, providing data from 1515 children, were included. VGBIs are effective (SMD = 0.38; 95%CI 0.08 to 0.68; p = 0.013) in increasing VA. Subgroup analyses suggested that non-immersive video games are the most appropriate for improving VA (SMD = 0.35; 95%CI 0.02 to 0.68; p = 0.039) and that VGBI is more effective than patching therapy, especially in combination with patching therapy (SMD = 0.63; 95%CI 0.29 to 0.97; p < 0.001). Conclusion: This SRMA, including a large number of RCTs to date, demonstrates that VGBI is effective in improving VA in children with amblyopia.
1. Introduction
Amblyopia is a neurodevelopmental disorder that significantly affects the visual cortex, defined as the selective suppression of visual information from one or both eyes during the critical period of childhood development [1]. This suppression results in a quantifiable deficit in visual acuity (VA). The global prevalence of amblyopia is estimated at 1.75%, although recent studies highlight a marked geographical variability [2] of 3.67% in Europe and around 0.5% in Africa [3]. Despite regional variations, amblyopia remains a leading cause of pediatric visual disability worldwide [4]. Its incidence in school-aged children, which ranges from 0.1% to 5.5%, highlights the importance of early detection. Amblyopia can affect the performance of daily living activities that require visual information, manifesting in deficiencies in the precision, speed, and variability of movements such as reaching and grasping with the upper extremities, as well as postural stability [5,6]. Studies indicate that children with visual dysfunctions, including amblyopia, may present with comorbidities such as attention deficit hyperactivity disorder [7], dyslexia, and learning difficulties [8]. These alterations can result in decreased academic, physical, and athletic performance, in addition to psychosocial implications such as reduced social contact and stress associated with vision loss [9].
To guarantee the therapy’s success, it is crucial to diagnose it before the age of 7, performing a complete visual examination [10]. The goal of amblyopia treatment is to maximize the connection between the brain and the amblyopic eye to improve VA. The main treatment option is occlusion of the non-amblyopic eye with a patch [11]. Another treatment option is visual penalization with atropine, which has a very similar effect to the patch but a greater degree of acceptance and adherence; however, it can have several systemic adverse effects [12]. Another alternative for penalization is the use of lenses with inaccurate refractive correction, but several studies show that these methods may not be very effective in more severe amblyopia, and they also have a high degree of non-compliance with the therapy [13,14].
On the other hand, the development of alternative therapeutic interventions focused on reducing suppression mechanisms present in the visual cortex has been promoted [15], such as dichoptic training [16]. This type of training, together with the evolution of novel technology, has made virtual reality (VR) and video games and/or serious games emerge as promising tools for the treatment of amblyopia. VR devices can be categorized into immersive VR devices, which provide a complete sense of presence through head-mounted displays (HMDs), and non-immersive systems, where interaction occurs via screens without a full virtual presence [17]. The use of video games with therapeutic purposes using VR devices (video game-based interventions [VGBIs]) aims to induce cortical reorganization and promote the activation of different neuronal connections through the presentation of different and complementary images to each eye [18]. This could translate into improvements in various functional skills, such as VA and stereoacuity [19]. Another great advantage of the use of VR devices is the patient acceptability rate, because children find it striking and attractive.
To date, some studies have assessed the use of VR devices and video games in pediatric ophthalmology therapy. Firstly, a recent systematic review has reported the promising use of VR devices as eye-tracking tools in the field of pediatric ophthalmology [20]. The other three systematic reviews compiled the most recent management options in amblyopia, including a few studies focused on VGBI and VR [21,22,23]. Henández-Rodríguez, CJ, Piñeo, DP et al. (2020), suggested that active vision therapy, including VR and VGBI, could be a promising tool in the recovery of visual acuity in amblyopic children [23]. Alrasheed, SH, and Aldakhil, S (2024) assessed traditional and novel approaches in the management of amblyopia, suggesting that adherence and satisfaction with the therapy can be favored using binocular treatment approaches [21]. Yeritsyan, A et al. (2024) noted that VR aids post-surgical alignment and that dichoptic training involving movies and games has been found to be superior to traditional occlusion therapy for amblyopia recovery [22]. Finally, only one systematic review with meta-analysis (SRMA) directly compared the efficacy of VGBI versus patching therapy in improving VA in children with amblyopia, including 10 trials [24]. Shao, W et al. (2023) [24] concluded that VR interventions significantly improve VA compared to traditional patching, particularly in children under seven years of age and in treatment protocols lasting less than 20 h. Some restrictions shared for all these reviews, such as the application of English language restriction, the inclusion of experimental, observational, and review studies in the same systematic review, and the large number of studies that were not detected in their search strategies, justify the elaboration of a new SRMA. Therefore, the objective of this SRMA was to assess the effectiveness of VGBI in improving VA in children with amblyopia. Secondarily, to assess the VR modality more appropriate to be used and, specifically, to compare the efficacy of VGBI with conventional therapies (patching therapy, spectacles, or sham).
2. Materials and Methods
2.1. Registration
This SRMA followed the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement [25] and in the Cochrane Handbook for Systematic Reviews of Interventions [26]. The methodological quality of this SRMA was checked using the AMSTAR 2 checklist [27], and it was prospectively registered in PROSPERO (CRD42025603936).
2.2. Literature Search Strategy
Two authors, independently, conducted systematic searches in PubMed Medline, SCOPUS, Web of Science, CINHAL Complete, and PEDro from inception to November 2025, without publication date and language restrictions. Complementarily, authors screened reference lists of previously published studies and gray literature. The search strategy was designed considering the PICOS system [28], as follows: Population (children with amblyopia), Intervention (VGBI), Comparison (others such as patching therapy, spectacles, or sham), Outcome (VA), and Study Design (randomized controlled trials [RCTs] or pilot RCTs). The search strategy was customized for each database according to syntax and index rules, using a combination of Medical Subject Headings (MeSH) and entry terms, combined with the Boolean operators “AND” and “OR”. Table 1 displays the search strategies used in the different databases.

Table 1.
Search strategies used in each database.
2.3. Inclusion Criteria
Two authors, independently, meticulously reviewed all references retrieved by title and abstract. When a record was identified as potentially eligible for inclusion in the SRMA, it was examined in detail by both authors. Any discrepancy was resolved by a third author. The Cohen’s kappa coefficient (κ) was used to assess the agreement of inclusion judgments between these authors [29]. The values of this coefficient were interpreted as degrees of agreement according to Landis and Koch: κ < 0 (non-existent); 0 ≤ κ ≤ 0.2 (non-significant); 0.2 < κ ≤ 0.4 (discrete); 0.4 < κ ≤ 0.6 (moderate); 0.6 < κ ≤ 0.8 (substantial); 0.8 < κ ≤ 1 (excellent) [30].
To be included in this SRMA, each study must meet all inclusion criteria related to the PICOS system. Additionally, the RCTs included must provide quantitative data to assess the variables of interest (VA) in the meta-analysis. On the other hand, studies whose samples mixed healthy and case children, and children with impairments other than amblyopia were excluded.
2.4. Data Extraction
Two authors, independently, extracted the following data from the studies included in the review using a specifically designed Microsoft Excel spreadsheet: (1) general study characteristics (authorship, year of publication, country, setting and funding); (2) sample characteristics (total participants, mean age, sex, number of groups, and number of participants in each group); (3) characteristics of VGBI (type of video game, modality of VR, duration and frequency of sessions); (4) characteristics of comparison intervention (type of comparison therapy and duration and frequency of sessions); (5) time of evaluation (immediate assessment or follow-up); and (6) data from the analyzed variables (mean and standard deviation for VA assessment). Additionally, authors registered other data related to satisfaction, compliance, and adverse events of patients in the VGBI group.
2.5. Risk of Bias and Evidence Quality Assessment
All these assessments were carried out separately by two authors, and disagreements were solved with a third author. First, the risk of bias was analyzed using the Cochrane Risk of Bias tool [31]. It assesses six domains with seven items: selection bias (sequence generation and concealed allocation), performance bias (blinding of participants and therapists), detection bias (blinding of evaluators), attrition bias (incomplete outcomes data), reporting bias (selective outcomes), and other biases. Each item is scored as “+”, “−”, or “?” for low, high, and unclear risk, respectively.
The evidence quality reported for each outcome was assessed using the GRADE statement and the checklist of Meader (2014) [32,33]. Considering the risk of bias of the RCTs included, inconsistency, imprecision, evidence indirectness, and risk of publication bias, the level of evidence of each finding’s meta-analysis can be quantified as high, moderate, low, or very low.
2.6. Statistical Analysis
Comprehensive Meta-Analysis Version 4 (Biostat, Englewood, NY, USA) was used for all analyses [34]. The meta-analysis of an outcome only was performed if at least 2 comparisons per outcome were available. Cohen’s standardized mean difference and 95% confidence interval (95% CI) were calculated in a random-effects model for continuous data [35,36]. The effect size was interpreted as null (SMD 0), low (SMD 0.2), medium (SMD 0.4), and large (SMD > 0.7). Each meta-analysis was graphically displayed in the forest plot [37]. Risk of publication bias was assessed using more than one method: the funnel plot, p-value for the Egger test, and the trim-and-fill estimation [38,39,40]. Inconsistency or heterogeneity was calculated with the degree of inconsistency of Higgins (I2), the χ-square test, and its p-value [41,42]. According to this, heterogeneity can be large (I2 > 50%), medium (I2 > 50–25%), low (I2 25–5%), or null (I2 < 5%) [43].
As additional quantitative analyses, the authors carried out a sensitivity analysis using the leave-one-out method, and two subgroup analyses: (1) to assess the effectiveness of VGBI according to VR modality of video game employed (non-immersive [NIVR] or immersive VR [IVR]); (2) to assess the effectiveness of VGBI according to specific comparisons detected in the RCTs included (VGBI vs. patching therapy, VGBI plus patching vs. patching therapy, VGBI vs. spectacle, and VGBI vs. sham).
2.7. Other Analyses
Due to the impossibility of performing more meta-analyses, data related to satisfaction, compliance, and adverse events were assessed using qualitative synthesis.
3. Results
3.1. Study Selection
A total of 1847 references were retrieved from databases (n = 1845) and from reference lists of retrieved studies (n = 2). After removing duplicates from the initial screening by title and abstract, 21 RCTs met the inclusion criteria and were included [44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64]. The authors demonstrated excellent inter-rater agreement (k = 0.89). Figure 1 shows the PRISMA flow diagram of the study selection process.
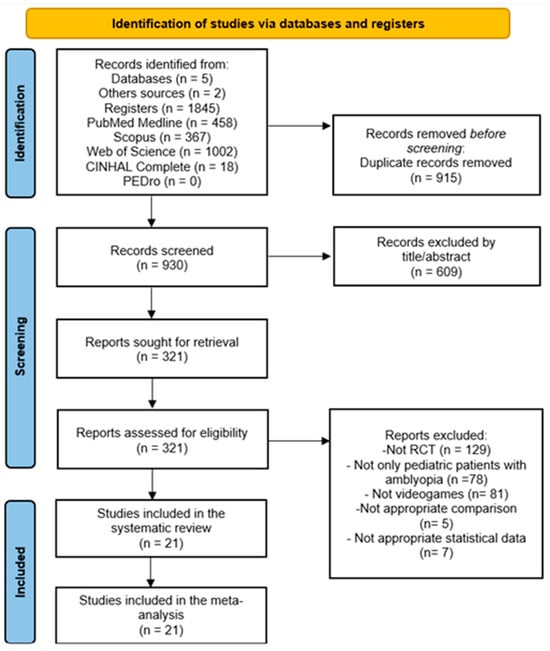
Figure 1.
PRISMA flow diagram.
3.2. Characteristics of the Studies Included in the Systematic Review
The 21 RCTs included, carried out between 2001 and 2024, included 1515 children with amblyopia (mean age of 7.9 ± 2.3 years old), and approximately 46% were boys. The intervention group (VGBI) comprised 750 children, and the comparison group comprised 765 children. In the intervention group, in 17 RCTs, the video games and VR devices used were non-immersive, and only 4 RCTs used immersive VR devices. The duration of the VGBI protocol ranged from 2 to 24 weeks, 1–7 sessions per week, and 20–90 min per session. As a comparison intervention, patching intervention was used in 16 RCTs (of which 3 combined VGBI plus patching therapy), spectacle in 3, and sham in 2. All assessments were carried out just to the end of the intervention (immediate assessment). Finally, 11 RCTs received external funding. More details about the characteristics of these RCTs are summarized in Table 2.
Table 2.
Characteristics of the included RCTs in this SRMA.
3.3. Risk of Bias Assessment
Random sequence generation, incomplete outcome data, and selective reporting presented low risk in 100% of the studies. Allocation concealment was adequate in 18 studies (85.7%), while two presented a high risk (9.5%) and one presented an uncertain risk (4.8%). Blinding of participants and personnel represented the most affected domain, with high risk in 20 studies (95.2%) due to the impossibility of masking the interventions, and only one study with low risk (4.8%). In contrast, blinding of evaluators was adequate in 20 studies (95.2%), and only one presented a high risk. Finally, the “other sources of bias” domain showed greater variability: 11 studies (52.4%) were classified as low risk, 8 (38.1%) as high risk, and 2 (9.5%) as uncertain. Figure 2 shows the Cochrane Risk of Bias tool assessment.
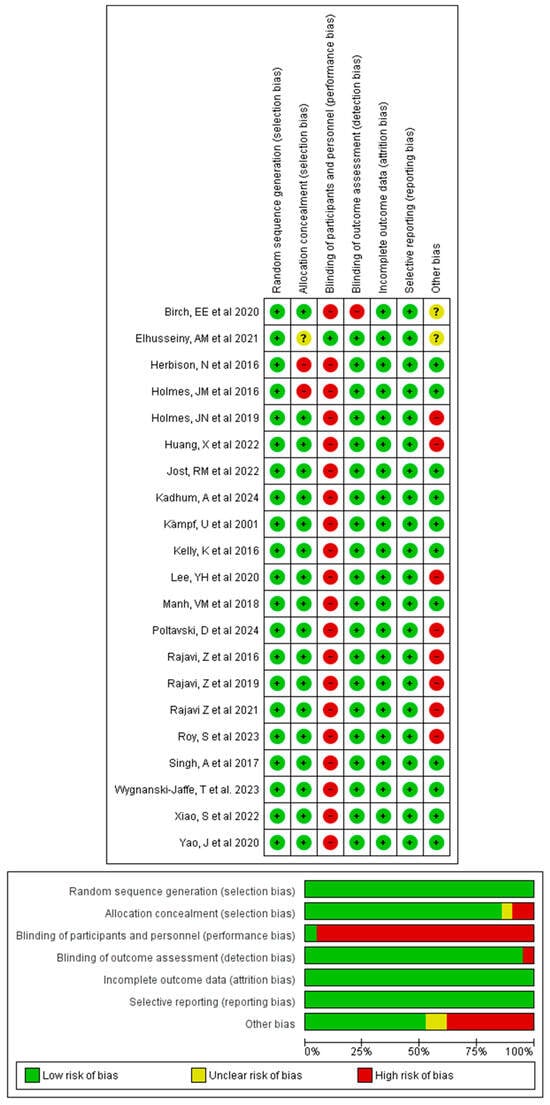
Figure 2.
Cochrane Risk of Bias tool assessment [44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64].
3.4. Quantitative Synthesis: Effect of VGBI on Visual Acuity
Twenty-one RCTs with 23 independent comparisons [44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64], providing data from 1550 children with amblyopia (749 receiving VGBI and 801 receiving other interventions), to assess the effectiveness of VGBI on VA. Our meta-analysis showed a low quality of evidence of a medium effect (SMD = 0.38; 95% CI 0.08 to 0.68; p = 0.013; I2 = 61%; x = 66.1; df = 21; p < 0.001) in improving VA favors VGBI (Figure 3). Risk of publication bias was confirmed with the asymmetric funnel plot, Egger test (p = 0.004), and trim-and-fill evaluation. Trim-and-fill analysis showed an adjusted pooled effect (adjusted SMD = 0.7; 95% CI 0.37 to 1.1) (Figure 4). This analysis suggests that the risk of publication bias was largely underestimating the true effect of VGBI in improving visual acuity. Finally, sensitivity analysis showed an equal contribution of the studies included in the pooled effect.
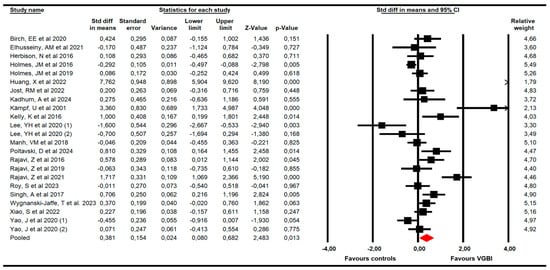
Figure 3.
Forest plot of the effect of VGBI on visual acuity in children with amblyopia [44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64].
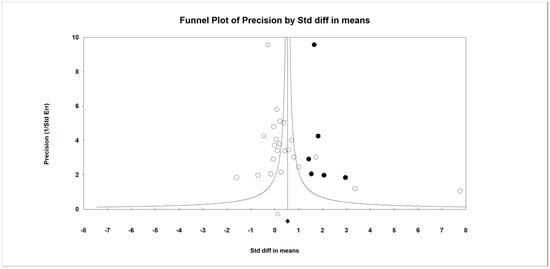
Figure 4.
Funnel plot of the effect of VGBI on visual acuity in children with amblyopia (trim-and-fill correction).
Subgroup Analyses
The first subgroup analysis (Figure 5) showed statistically significant differences in increasing VA after using NIVR (K = 19; SMD = 0.35; 95% CI 0.02 to 0.68; p = 0.039; I2 = 71.13%; x = 62.4; df = 18; p < 0.001) [44,45,47,48,49,50,51,52,53,54,57,59,60,61,62,63,64], but not for IVR devices (K = 4; SMD = 0.54; 95% CI −0.28 to 1.36; p = 0.199; I2 = 0%; x = 2.9; df = 3; p = 0.41).
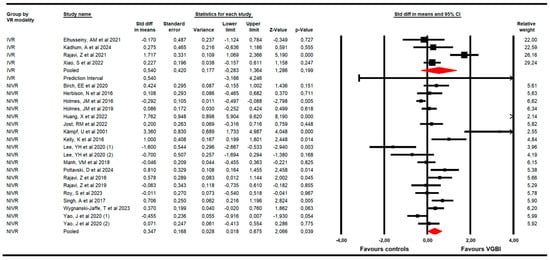
Figure 5.
Forest plot of the subgroup analysis according to VR modality [44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64].
The second subgroup analysis (Figure 6) reported that (1) VGBI was better than patching therapy (K = 14; SMD = 0.22; 95% CI 0.07 to 0.38; p = 0.004; I2 = 25.4%; x = 17.4; df = 13; p = 0.18) [44,45,51,52,53,54,55,58,59,60,61,63]; and that VGBI plus patching treatment showed a major effect compared to only patching treatment (K = 3; SMD = 0.63; 95% CI 0.29 to 0.97; p < 0.001; I2 = 69.3%; x = 9.17; df = 2; p = 0.001) [48,62,64]. Opposite, non-statistically significant differences were found between VGBI and sham [46,49,57] (SMD = 0.31; 95% CI −0.16 to 0.78; p = 0.193; I2 = 76.62%; x = 12.9; df = 2; p < 0.001), and between VGBI and spectacle [47,50,56] (SMD = −0.12; 95% CI −0.28 to 0.04; p = 0.144; I2 = 61.3%; x = 6.9; df = 2; p = 0.03).
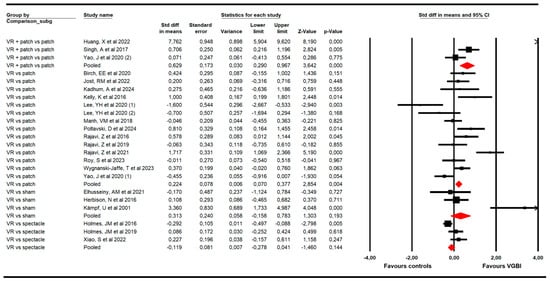
Figure 6.
Forest plot of the subgroup analysis according to specific comparisons [44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64].
3.5. Certainty of Evidence
According to the GRADE assessment and the Meader checklist, overall findings reported low quality of evidence, while findings in the different subgroup analyses ranged from low to very low. Table 3 details the certainty of evidence of the findings of the meta-analyses.
Table 3.
Certainty of evidence (GRADE assessment).
3.6. Qualitative Synthesis: Satisfaction, Compliance, and Adverse Events
The qualitative findings reported by RCTs concerning satisfaction, compliance, and adverse events related to the use of VGBI are summarized in Table 4.
Table 4.
Qualitative findings about satisfaction, adherence, and adverse events in VGBI groups of the studies included.
Firstly, 3 RCTs [49,56,63] suggested a high level of satisfaction with the therapy, as, overall, 90% of the participating children reported enjoying the therapy and found the systems engaging and easy to use, being recommended for future treatments. Second, 16 RCTs provided data regarding the adherence or compliance of children to VGBI [44,45,46,47,49,50,51,52,53,55,56,58,59,61,63,64], reporting a significantly higher level of adherence in the group receiving VGBI. In the majority of RCTs included, over 60% of participants completed the prescribed treatment [44,45,46,49,51,52,55,56,58,59,63,64]. Finally, 9 RCTs provided relevant data about the safety of VGBI [46,47,49,50,53,56,61,63,64]. Two of these studies reported no adverse effects [46,64], and the remaining seven studies reported a low incidence of mild adverse effects associated with immersive VR, such as double vision, symptoms related to cybersickness, diplopia, blurred vision, or eye discomfort.
4. Discussion
Amblyopia presents a significant clinical challenge. Traditionally, passive or conventional therapies, mainly patching and occlusive contact lenses, have demonstrated effectiveness in managing this condition [21,22], with reduced levels of therapy compliance. More recently, “active vision therapy” [23], encompassing methods such as dichoptic therapy, perceptual learning, and particularly vision game-based intervention (VGBI) [24], has emerged as a promising avenue to enhance visual neuroplasticity and improve VA in amblyopic children. The ludic and gamified nature of VGBI is particularly noteworthy, as it has the potential to significantly increase treatment adherence, a common challenge with traditional methods. Given these considerations, this SRMA of RCTs was conducted to systematically elucidate the effectiveness of VGBI in the management of amblyopia in children. We identified 21 RCTs that provide data from 1515 children with amblyopia. Through these RCTs, our meta-analysis elucidates that VGBI can indeed improve VA in amblyopic children.
The primary outcome assessed in this SRMA was VA in amblyopia. Our findings indicate a moderate effect of VGBI in improving VA in children with amblyopia. It is important to note that the presence of publication bias likely led to an underestimation of this effect. Our analysis suggests the true effect could be as much as 84% greater than initially observed. These results align with previous systematic reviews [21,22,23] and meta-analyses [24]. A significant strength of our SRMA is the high level of evidence provided, attributable to the larger number of included studies, the absence of language and publication date restrictions, and the exclusive inclusion of RCTs. This SRMA also yielded other interesting findings from subgroup analyses. Firstly, the video games and virtual VR devices used in the included RCTs were categorized as either non-immersive or immersive. Our SRMA demonstrated that NIVR was the more effective VR modality or VGBI type for increasing VA in amblyopic children. This could be attributed to their simplicity, ease of use, and understanding. This finding represents a novel contribution, as no previous reviews have assessed this specific distinction. Furthermore, when directly comparing the efficacy of VGBI with other interventions included in the RCTs, our results indicate that VGBI was superior to patching therapy in improving VA. This finding directly corroborates the results of Shao et al. (2023) [24], though our SRMA included more RCTs, thereby strengthening the evidence level of these previous observations. Additionally, we uncovered another novel finding: the combination of VGBI and patching therapy appears to be the most effective management strategy for VA, surpassing traditional methods such as patching therapy alone.
A significant challenge in managing amblyopia in children is therapy adherence. While traditional methods, such as patching, have proven effective, they often lead to physical discomfort and social stigma, among others, ultimately reducing compliance [65]. In contrast, video games and VR offer an engaging alternative, supported by recent research highlighting their potential to significantly improve adherence. Studies have shown that gamification, through video games or serious games, by integrating playful elements into visual therapy, increases patient motivation and engagement, transforming the therapeutic routine into an enjoyable and participatory experience [66]. In line with this, our review suggests that VGBI leads to high levels of satisfaction in children, specifically revealing that 90% of children who used these interventions found the therapy enjoyable. Furthermore, the included studies consistently reported higher levels of adherence/compliance in the VGBI group. In most included studies, children completed more prescribed therapy, demonstrating high adherence to VGBI. Beyond the playful component, another crucial element is to know if VGBI produces minimal adverse effects. In this regard, our review demonstrates that the included interventions are safe, showing only minimal adverse effects such as eye discomfort, symptoms of motion cybersickness, or blurred vision.
The effectiveness of VGBI and VR devices in treating amblyopia in children could be attributed to several key factors. Firstly, these video games facilitate the presentation of distinct visual stimuli to each eye, which is crucial for binocular training. Studies have shown that dichoptic visual stimulation (presenting different images to each eye) can induce cortical changes, promoting the recovery of binocular function. VGBI engaging visual stimuli directed at the amblyopic eye stimulates its activity and strengthens these connections. This process gradually restores synaptic balance in the visual cortex, allowing for a more equitable representation of information from both eyes [67]. Secondly, video games and VR foster improved VA through perceptual learning, a process that optimizes the ability to discriminate and recognize visual stimuli through repetitive practice [68]. Research has demonstrated that immediate visual feedback and intrinsic rewards provided in interactive virtual environments accelerate perceptual learning, strengthening neural connections associated with visual processing [69]. VR, by integrating multisensory stimulation such as auditory and haptic feedback, further enhances this learning by increasing patient attention and immersion [70]. This adaptability of VR allows for the customization of visual stimuli, which is crucial given the heterogeneity of amblyopia. Finally, the accessibility of VR systems and video games through portable and home-use devices facilitates remote monitoring of treatment progress, allowing for early interventions [71]. In this sense, it is crucial to increase parents’ involvement in the therapy [72]. Investigations have confirmed that parental supervision and support significantly increase treatment compliance and, consequently, the achieved outcomes.
Although the findings of this SRMA update the scientific evidence about the effectiveness of VGBI in the treatment of amblyopia, some limitations can be considered. Firstly, although the number of studies included in the SRMA is large, specifically, the number of studies in which immersive VR or other specific comparisons have been assessed is low. Second, the presence of potential selection, performance, and detection biases in the studies included may obscure the true effect of VGBI [73,74]. Thirdly, meta-analysis showed a large risk of publication bias that can alter the true effect of VGBI. Trim-and-fill evaluation demonstrated that the risk of publication bias underestimates the true effect. Another limitation is related to the large statistical heterogeneity found in the meta-analyses, related to VGBI protocols, measurement tools, and control comparisons in the studies included. However, sensitivity analysis showed a homogeneous contribution of studies in the pooled effect. Finally, these findings show the effectiveness of VGBI in the short-term (post-intervention assessment), and no follow-up could be assessed because the studies included did not provide data. Future studies must focus on the evaluation of the effectiveness of IVR devices and on the assessment of whether the effect of VGBI is maintained over time. Additionally, future research is needed to determine the optimal parameters for visual stimulation, the duration of treatment, and the frequency of sessions. These studies will guarantee to consolidate these promising findings.
5. Conclusions
This systematic review with meta-analysis conclusively demonstrated the effectiveness of vision game-based intervention for improving visual acuity in children with amblyopia. On the one hand, non-immersive virtual reality is the most appropriate virtual reality modality to use it, and specifically, vision game-based intervention was more effective than patching therapy. Our systematic review with meta-analysis reported that the major effectiveness was found when vision game-based intervention was combined with patching therapy. Additionally, children involved in vision game-based intervention reported higher levels of satisfaction and compliance with the prescribed therapy. Finally, vision game-based intervention is safe therapy due to the minimal adverse events reported for amblyopic children.
Author Contributions
Conceptualization, M.P.-L., I.C.-P., S.G.-M., R.L.-V., H.G.-L. and E.O.-G.; methodology, M.P.-L., I.C.-P., S.G.-M., R.L.-V., H.G.-L. and E.O.-G.; software, M.P.-L. and I.C.-P.; validation, E.O.-G.; formal analysis, M.P.-L., I.C.-P., S.G.-M., R.L.-V., H.G.-L. and E.O.-G.; investigation, M.P.-L., I.C.-P., S.G.-M., R.L.-V., H.G.-L. and E.O.-G.; data curation, M.P.-L., S.G.-M. and H.G.-L.; writing—original draft preparation, M.P.-L., I.C.-P., R.L.-V. and E.O.-G.; writing—review and editing, M.P.-L., I.C.-P., S.G.-M., R.L.-V., H.G.-L. and E.O.-G.; visualization, M.P.-L., I.C.-P., S.G.-M., R.L.-V., H.G.-L. and E.O.-G.; supervision, I.C.-P. and E.O.-G.; project administration, I.C.-P. and E.O.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author, the data are not publicly available due to privacy.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| 95% CI | 95% confidence interval |
| SMD | Standardized mean difference |
| SRMA | Systematic review and meta-analysis |
| RCTs | Randomized controlled trials |
| VA | Visual acuity |
| VGBIs | Video game-based interventions |
| VR | Virtual reality |
References
- Meier, K.; Giaschi, D. Unilateral Amblyopia Affects Two Eyes: Fellow Eye Deficits in Amblyopia. Investig. Ophthalmol. Vis. Sci. 2017, 58, 1779–1800. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, H.; Pakzad, R.; Yekta, A.; Bostamzad, P.; Aghamirsalim, M.; Sardari, S.; Valadkhan, M.; Pakbin, M.; Heydarian, S.; Khabazkhoob, M. Global and Regional Estimates of Prevalence of Amblyopia: A Systematic Review and Meta-Analysis. Strabismus 2018, 26, 168–183. [Google Scholar] [CrossRef] [PubMed]
- Vega, L.L. Diseño, Desarrollo y Evaluación de Un Nuevo Sistema Basado En Realidad Virtual Para El Tratamiento de La Ambliopía. Doctoral Dissertation, Universidad de Valladolid, Valladolid, Spain, 2024. [Google Scholar]
- McKee, S.P.; Levi, D.M.; Movshon, J.A. The Pattern of Visual Deficits in Amblyopia. J. Vis. 2003, 3, 380–405. [Google Scholar] [CrossRef] [PubMed]
- Goodale, M.A. Transforming Vision into Action. Vision Res. 2011, 51, 1567–1587. [Google Scholar] [CrossRef]
- Niechwiej-Szwedo, E.; Colpa, L.; Wong, A.M.F. Visuomotor Behaviour in Amblyopia: Deficits and Compensatory Adaptations. Neural Plast. 2019, 2019, 6817839. [Google Scholar] [CrossRef]
- Ho, J.-D.; Sheu, J.-J.; Kao, Y.-W.; Shia, B.-C.; Lin, H.-C. Associations between Attention-Deficit/Hyperactivity Disorder and Ocular Abnormalities in Children: A Population-Based Study. Ophthalmic Epidemiol. 2020, 27, 194–199. [Google Scholar] [CrossRef]
- Birch, E.E.; Kelly, K.R. Pediatric Ophthalmology and Childhood Reading Difficulties: Amblyopia and Slow Reading. J. AAPOS 2017, 21, 442–444. [Google Scholar] [CrossRef]
- Ghasia, F.; Wang, J. Amblyopia and Fixation Eye Movements. J. Neurol. Sci. 2022, 441, 120373. [Google Scholar] [CrossRef]
- Holmes, J.M.; Lazar, E.L.; Melia, B.M.; Astle, W.F.; Dagi, L.R.; Donahue, S.P.; Frazier, M.G.; Hertle, R.W.; Repka, M.X.; Quinn, G.E.; et al. Effect of Age on Response to Amblyopia Treatment in Children. Arch. Ophthalmol. 2011, 129, 1451–1457. [Google Scholar] [CrossRef]
- Webber, A.L.; Wood, J. Amblyopia: Prevalence, Natural History, Functional Effects and Treatment. Clin. Exp. Optom. 2005, 88, 365–375. [Google Scholar] [CrossRef]
- Glaser, S.R.; Matazinski, A.M.; Sclar, D.M.; Sala, N.A.; Vroman, C.M.; Tanner, C.E.; Stager, D.R.; Berry, P.M.; Stager, D.R.; Felius, J.; et al. A Randomized Trial of Atropine vs Patching for Treatment of Moderate Amblyopia in Children. Arch. Ophthalmol. 2002, 120, 268–278. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, E.; Asproudis, I.; Maconachie, G.; Tsironi, E.E.; Gottlob, I. The Treatment of Amblyopia: Current Practice and Emerging Trends. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 1061–1078. [Google Scholar] [CrossRef] [PubMed]
- Tejedor, J.; Ogallar, C. Comparative Efficacy of Penalization Methods in Moderate to Mild Amblyopia. Am. J. Ophthalmol. 2008, 145, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Hess, R.F.; Mansouri, B.; Thompson, B. A Binocular Approach to Treating Amblyopia: Antisuppression Therapy. Optom. Vis. Sci. 2010, 87, 697–704. [Google Scholar] [CrossRef]
- Knox, P.J.; Simmers, A.J.; Gray, L.S.; Cleary, M. An Exploratory Study: Prolonged Periods of Binocular Stimulation Can Provide an Effective Treatment for Childhood Amblyopia. Investig. Ophthalmol. Vis. Sci. 2012, 53, 817–824. [Google Scholar] [CrossRef]
- Piñar-Lara, M.; Cortés-Pérez, I.; Díaz-Fernández, Á.; Montilla-Ibáñez, M.d.A.; Sedeño-Vidal, A.; Obrero-Gaitán, E. Virtual Reality-Based Therapy Can Enhance Balance and Muscular Endurance in Children and Adolescents with Down Syndrome: A Systematic Review with a Meta-Analysis. Bioengineering 2024, 11, 1112. [Google Scholar] [CrossRef]
- Molina-Martín, A.; Leal-Vega, L.; de Fez, D.; Martínez-Plaza, E.; Coco-Martín, M.B.; Piñero, D.P. Amblyopia Treatment through Immersive Virtual Reality: A Preliminary Experience in Anisometropic Children. Vision 2023, 7, 42. [Google Scholar] [CrossRef]
- Eastgate, R.M.; Griffiths, G.D.; Waddingham, P.E.; Moody, A.D.; Butler, T.K.H.; Cobb, S.V.; Comaish, I.F.; Haworth, S.M.; Gregson, R.M.; Ash, I.M.; et al. Modified Virtual Reality Technology for Treatment of Amblyopia. Eye 2006, 20, 370–374. [Google Scholar] [CrossRef]
- Nikolaidou, A.; Sandali, A.; Chatzidimitriou, E.; Pantelaki, D.; Gianni, T.; Lamprogiannis, L. Virtual Reality with Eye Tracking for Pediatric Ophthalmology: A Systematic Review. J. Pediatr. Ophthalmol. Strabismus 2024, 61, 381–390. [Google Scholar] [CrossRef]
- Alrasheed, S.H.; Aldakhil, S. Childhood Amblyopia: A Systematic Review of Recent Management Options. Saudi J. Ophthalmol. 2024, 38, 201–213. [Google Scholar] [CrossRef]
- Yeritsyan, A.; Surve, A.V.; Ayinde, B.; Chokshi, P.; Adhikari, S.; Jaimalani, A.; Hamid, P. Efficacy of Amblyopia Treatments in Children up to Seven Years Old: A Systematic Review. Cureus 2024, 16, e56705. [Google Scholar] [CrossRef]
- Hernández-Rodríguez, C.J.; Piñero, D.P. Active Vision Therapy for Anisometropic Amblyopia in Children: A Systematic Review. J. Ophthalmol. 2020, 2020, 4282316. [Google Scholar] [CrossRef] [PubMed]
- Shao, W.; Niu, Y.; Wang, S.; Mao, J.; Xu, H.; Wang, J.; Zhang, C.; Guo, L. Effects of Virtual Reality on the Treatment of Amblyopia in Children: A Systematic Review and Meta-Analysis. J. Pediatr. Nurs. 2023, 72, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley Blackwell & Sons: Hoboken, NJ, USA, 2020. [Google Scholar]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews that Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Amir-Behghadami, M.; Janati, A. Population, Intervention, Comparison, Outcomes and Study (PICOS) Design as a Framework to Formulate Eligibility Criteria in Systematic Reviews. Emerg. Med. J. 2020, 37, 387. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef]
- Higgins, J.; Altman, D.; Gotzsche, P.; Juni, P.; Moher, D.; Oxman, A.; Savovic, J.; Schulz, K.; Weeks, L.; Sterne, J. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Meader, N.; King, K.; Llewellyn, A.; Norman, G.; Brown, J.; Rodgers, M.; Moe-Byrne, T.; Higgins, J.P.; Sowden, A.; Stewart, G. A Checklist Designed to Aid Consistency and Reproducibility of GRADE Assessments: Development and Pilot Validation. Syst. Rev. 2014, 3, 82. [Google Scholar] [CrossRef]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading Quality of Evidence and Strength of Recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis Software, version 4; Biostat, Inc.: Englewood, NJ, USA, 2026. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1977. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Rücker, G.; Schwarzer, G. Beyond the Forest Plot: The Drapery Plot. Res. Synth. Methods 2021, 12, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. Br. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Egger, M. Funnel Plots for Detecting Bias in Meta-Analysis: Guidelines on Choice of Axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Higgins, J.; Thompson, S.; Altman, D. Statistical Heterogeneity in Systematic Reviews of Clinical Trials: A Critical Appraisal of Guidelines and Practice. J. Health Serv. Res. Policy 2002, 7, 51–61. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A. Interpretation of Tests of Heterogeneity and Bias in Meta-analysis. J. Eval. Clin. Pract. 2008, 14, 951–957. [Google Scholar] [CrossRef]
- Higgins, J.; Thompson, S.; Deeks, J.; Altman, D. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Birch, E.E.; Jost, R.M.; Kelly, K.R.; Leffler, J.N.; Dao, L.; Beauchamp, C.L. Baseline and Clinical Factors Associated with Response to Amblyopia Treatment in a Randomized Clinical Trial. Optom. Vis. Sci. 2020, 97, 316–323. [Google Scholar] [CrossRef]
- Jost, R.M.; Hudgins, L.A.; Dao, L.M.; Stager, D.R.; Luu, B.; Beauchamp, C.L.; Hunter, J.S.; Giridhar, P.; Wang, Y.-Z.; Birch, E.E. Randomized Clinical Trial of Streaming Dichoptic Movies versus Patching for Treatment of Amblyopia in Children Aged 3 to 7 Years. Sci. Rep. 2022, 12, 4157. [Google Scholar] [CrossRef] [PubMed]
- Elhusseiny, A.M.; Bishop, K.; Staffa, S.J.; Zurakowski, D.; Hunter, D.G.; Mantagos, I.S. Virtual Reality Prototype for Binocular Therapy in Older Children and Adults with Amblyopia. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2021, 25, 217.e1–217.e6. [Google Scholar] [CrossRef] [PubMed]
- Holmes, J.M.; Manh, V.M.; Lazar, E.L.; Beck, R.W.; Birch, E.E.; Kraker, R.T.; Crouch, E.R.; Erzurum, S.A.; Khuddus, N.; Summers, A.I.; et al. Effect of a Binocular IPad Game vs Part-Time Patching in Children Aged 5 to 12 Years with Amblyopia. JAMA Ophthalmol. 2016, 134, 1391. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Xia, H.; Zhang, Q.; Blakemore, C.; Nan, Y.; Wang, W.; Gao, J.; Ng, S.S.; Wen, J.; Huang, T.; et al. New Treatment for Amblyopia Based on Rules of Synaptic Plasticity: A Randomized Clinical Trial. Sci. China Life Sci. 2022, 65, 451–465. [Google Scholar] [CrossRef]
- Herbison, N.; MacKeith, D.; Vivian, A.; Purdy, J.; Fakis, A.; Ash, I.M.; Cobb, S.V.; Eastgate, R.M.; Haworth, S.M.; Gregson, R.M.; et al. Randomised Controlled Trial of Video Clips and Interactive Games to Improve Vision in Children with Amblyopia Using the I-BiT System. Br. J. Ophthalmol. 2016, 100, 1511–1516. [Google Scholar] [CrossRef]
- Holmes, J.M.; Manny, R.E.; Lazar, E.L.; Birch, E.E.; Kelly, K.R.; Summers, A.I.; Martinson, S.R.; Raghuram, A.; Colburn, J.D.; Law, C.; et al. A Randomized Trial of Binocular Dig Rush Game Treatment for Amblyopia in Children Aged 7 to 12 Years. Ophthalmology 2019, 126, 456–466. [Google Scholar] [CrossRef]
- Kelly, K.R.; Jost, R.M.; Dao, L.; Beauchamp, C.L.; Leffler, J.N.; Birch, E.E. Binocular IPad Game vs Patching for Treatment of Amblyopia in Children. JAMA Ophthalmol. 2016, 134, 1402. [Google Scholar] [CrossRef]
- Poltavski, D.; Adams, R.J.; Biberdorf, D.; Patrie, J.T. Effectiveness of a Novel Video Game Platform in the Treatment of Pediatric Amblyopia. J. Pediatr. Ophthalmol. Strabismus 2024, 61, 20–29. [Google Scholar] [CrossRef]
- Manh, V.M.; Holmes, J.M.; Lazar, E.L.; Kraker, R.T.; Wallace, D.K.; Kulp, M.T.; Galvin, J.A.; Shah, B.K.; Davis, P.L. A Randomized Trial of a Binocular IPad Game Versus Part-Time Patching in Children Aged 13 to 16 Years with Amblyopia. Am. J. Ophthalmol. 2018, 186, 104–115. [Google Scholar] [CrossRef]
- Lee, Y.H.; Maniglia, M.; Velez, F.; Demer, J.L.; Seitz, A.R.; Pineles, S. Short-Term Perceptual Learning Game Does Not Improve Patching-Resistant Amblyopia in Older Children. J. Pediatr. Ophthalmol. Strabismus 2020, 57, 176–184. [Google Scholar] [CrossRef]
- Kadhum, A.; Tan, E.T.C.; Fronius, M.; Baart, S.J.; Levi, D.M.; Joosse, M.V.; Simonsz, H.J.; Loudon, S.E. Supervised Dichoptic Gaming versus Monitored Occlusion Therapy for Childhood Amblyopia: Effectiveness and Efficiency. Acta Ophthalmol. 2024, 102, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Angjeli, E.; Wu, H.C.; Gaier, E.D.; Gomez, S.; Travers, D.A.; Binenbaum, G.; Langer, R.; Hunter, D.G.; Repka, M.X. Randomized Controlled Trial of a Dichoptic Digital Therapeutic for Amblyopia. Ophthalmology 2022, 129, 77–85. [Google Scholar] [CrossRef]
- Kämpf, U.; Muchamedjarow, F.; Seiler, T. Unterstützende Amblyopiebehandlung Durch Computerspiele Mit Hintergrundstimulation: Eine 10-Tägige Plazebokontrollierte Pilot-Studie. Klin. Monbl. Augenheilkd. 2001, 218, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Rajavi, Z.; Soltani, A.; Vakili, A.; Sabbaghi, H.; Behradfar, N.; Kheiri, B.; Reza, M. Virtual Reality Game Playing in Amblyopia Therapy: A Randomized Clinical Trial. J. Pediatr. Ophthalmol. Strabismus 2021, 58, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Rajavi, Z.; Sabbaghi, H.; Amini Sharifi, E.; Behradfar, N.; Kheiri, B. Comparison between Patching and Interactive Binocular Treatment in Amblyopia: A Randomized Clinical Trial. J. Curr. Ophthalmol. 2019, 31, 426–431. [Google Scholar] [CrossRef]
- Rajavi, Z.; Sabbaghi, H.; Amini Sharifi, E.; Behradfar, N.; Yaseri, M. The Role of Interactive Binocular Treatment System in Amblyopia Therapy. J. Curr. Ophthalmol. 2016, 28, 217–222. [Google Scholar] [CrossRef]
- Roy, S.; Saxena, R.; Dhiman, R.; Phuljhele, S.; Sharma, P. Comparison of Dichoptic Therapy Versus Occlusion Therapy in Children With Anisometropic Amblyopia: A Prospective Randomized Study. J. Pediatr. Ophthalmol. Strabismus 2023, 60, 210–217. [Google Scholar] [CrossRef]
- Singh, A.; Sharma, P.; Saxena, R. Evaluation of the Role of Monocular Video Game Play as an Adjuvant to Occlusion Therapy in the Management of Anisometropic Amblyopia. J. Pediatr. Ophthalmol. Strabismus 2017, 54, 244–249. [Google Scholar] [CrossRef]
- Wygnanski-Jaffe, T.; Kushner, B.J.; Moshkovitz, A.; Belkin, M.; Yehezkel, O.; Gan, R.; Spierer, A.; Wygnanski-Jaffe, T.; Zitzer, N.; Cohen, D.; et al. An Eye-Tracking–Based Dichoptic Home Treatment for Amblyopia. Ophthalmology 2023, 130, 274–285. [Google Scholar] [CrossRef]
- Yao, J.; Moon, H.-W.; Qu, X. Binocular Game versus Part-Time Patching for Treatment of Anisometropic Amblyopia in Chinese Children: A Randomised Clinical Trial. Br. J. Ophthalmol. 2020, 104, 369–375. [Google Scholar] [CrossRef]
- Kaur, S.; Bhatia, I.; Beke, N.; Jugran, D.; Raj, S.; Sukhija, J. Efficacy of Part-Time Occlusion in Amblyopia in Indian Children. Indian J. Ophthalmol. 2021, 69, 112–115. [Google Scholar] [CrossRef]
- Argilés, M.; Jurado, L.A.; Junyent, L.Q. Gamification, Serious Games and Action Video Games in Optometry Practice. J. Optom. 2020, 13, 210–211. [Google Scholar] [CrossRef] [PubMed]
- Li, R.W.; Ngo, C.; Nguyen, J.; Levi, D.M. Video-Game Play Induces Plasticity in the Visual System of Adults with Amblyopia. PLoS Biol. 2011, 9, e1001135. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Rodríguez, C.J.; Ferrer-Soldevila, P.; Artola-Roig, A.; Piñero, D.P. Rehabilitation of Amblyopia Using a Digital Platform for Visual Training Combined with Patching in Children: A Prospective Study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2024, 262, 3007–3020. [Google Scholar] [CrossRef] [PubMed]
- Levi, D.M.; Li, R.W. Perceptual Learning as a Potential Treatment for Amblyopia: A Mini-Review. Vision Res. 2009, 49, 2535–2549. [Google Scholar] [CrossRef]
- Adamovich, S.V.; Fluet, G.G.; Tunik, E.; Merians, A.S. Sensorimotor Training in Virtual Reality: A Review. NeuroRehabilitation 2009, 25, 29–44. [Google Scholar] [CrossRef]
- Li, L.; Xue, H.; Lai, T.; Xue, Y.; Luo, G. Comparison of Compliance among Patients with Pediatric Amblyopia Undergoing Virtual Reality-Based and Traditional Patching Method Training. Front. Public Health 2022, 10, 1037412. [Google Scholar] [CrossRef]
- Li, Y.; Sun, H.; Zhu, X.; Su, Y.; Yu, T.; Wu, X.; Zhou, X.; Jing, L. Efficacy of Interventions for Amblyopia: A Systematic Review and Network Meta-Analysis. BMC Ophthalmol. 2020, 20, 203. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Saltaji, H.; da Costa, B.R.; Fuentes, J.; Ha, C.; Cummings, G.G. What Is the Influence of Randomisation Sequence Generation and Allocation Concealment on Treatment Effects of Physical Therapy Trials? A Meta-Epidemiological Study. BMJ Open 2015, 5, e008562. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Fuentes, J.; da Costa, B.R.; Saltaji, H.; Ha, C.; Cummings, G.G. Blinding in Physical Therapy Trials and Its Association with Treatment Effects. Am. J. Phys. Med. Rehabil. 2017, 96, 34–44. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.