
Is There a Deficit in Product and Process of Handwriting in Children with Attention Deficit Hyperactivity Disorder? A Systematic Review and Recommendations for Future Research

Abstract
:
1. Introduction
1.1. Attention Deficit Hyperactivity Disorder (ADHD)
1.2. Handwriting Deficits in ADHD
1.3. Aim of the Systematic Review
2. Method
2.1. Search Strategy
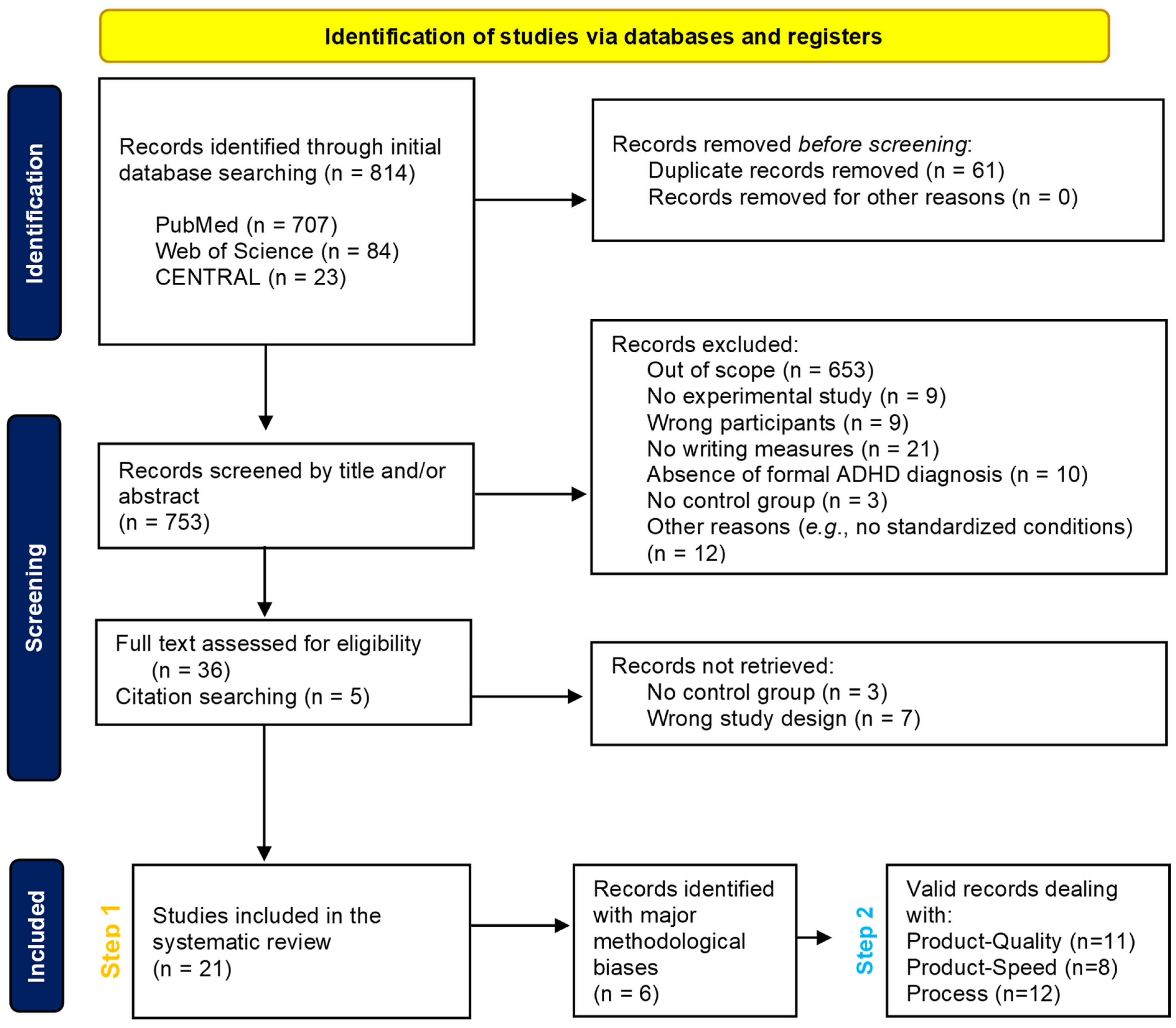
2.2. Identification
2.3. Study Selection
2.4. Methodological Quality
3. Results
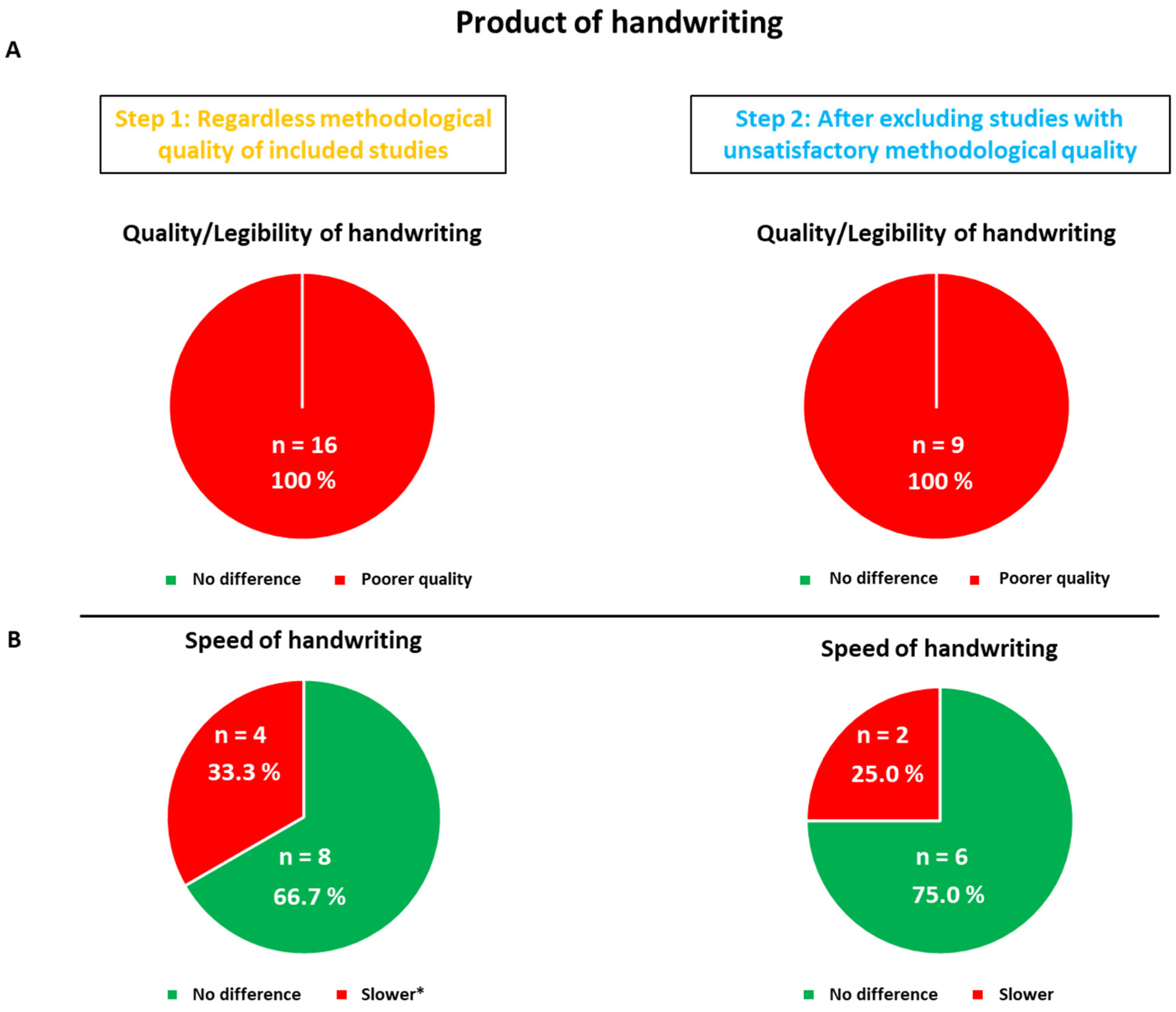
3.1. Product of Handwriting Results
3.1.1. Quality/Legibility
3.1.2. Primary Conclusions with Respect to Quality/Legibility of Handwriting
3.1.3. Speed of Handwriting
3.1.4. Primary Conclusions with Respect to Speed of Handwriting
3.2. Process of Handwriting
Primary Conclusions Regarding the Process of Handwriting
4. Discussion
4.1. Is Handwriting Performance in Children with ADHD Really Impaired?
4.2. Are All Children with ADHD Affected by Handwriting Deficits?
4.3. Suggested Recommendations for the Conduct of Studies on ADHD and Comorbid Handwriting Deficits
4.3.1. Dysgraphia Evaluation
4.3.2. Confounding Factors
4.3.3. Medication and Behavioral Treatments
4.4. Theoretical Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Faraone, S.V.; Mick, E. Molecular genetics of attention deficit hyperactivity disorder. Psychiatr. Clin. 2010, 33, 159–180. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.V.; Willcutt, E.G.; Salum, G.A.; Kieling, C.; Rohde, L.A. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Sanders, S.; Doust, J.; Beller, E.; Glasziou, P. Prevalence of attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. Pediatrics 2015, 135, e994–e1001. [Google Scholar] [CrossRef]
- Wolraich, M.L.; Hagan, J.F.; Allan, C.; Chan, E.; Davison, D.; Earls, M.; Evans, S.W.; Flinn, S.K.; Froehlich, T.; Frost, J.; et al. Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics 2019, 144, e20192528. [Google Scholar] [CrossRef] [PubMed]
- Fayyad, J.; Sampson, N.A.; Hwang, I.; Adamowski, T.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Andrade, L.H.S.G.; Borges, G.; de Girolamo, G.; Florescu, S.; et al. The descriptive epidemiology of DSM-IV adult ADHD in the world health organization world mental health surveys. ADHD Atten. Deficit Hyperact. Disord. 2017, 9, 47–65. [Google Scholar] [CrossRef] [PubMed]
- Breda, V.; Rohde, L.A.; Menezes AM, B.; Anselmi, L.; Caye, A.; Rovaris, D.L.; Vitola,, E.S.; Bau, C.H.D.; Grevet, E.S. Revisiting ADHD age-of-onset in adults: To what extent should we rely on the recall of childhood symptoms? Psychol. Med. 2020, 50, 857–866. [Google Scholar] [CrossRef]
- Faraone, S.V.; Banaschewski, T.; Coghill, D.; Zheng, Y.; Biederman, J.; Bellgrove, M.A.; Newcorn, J.H.; Gignac, M.; Al Saud, N.M.; Manor, I.; et al. The world federation of ADHD international consensus statement: 208 evidence-based conclusions about the disorder. Neurosci. Biobehav. Rev. 2021, 128, 789–818. [Google Scholar] [CrossRef]
- Tistarelli, N.; Fagnani, C.; Troianiello, M.; Stazi, M.A.; Adriani, W. The nature and nurture of ADHD and its comorbidities: A narrative review on twin studies. Neurosci. Biobehav. Rev. 2020, 109, 63–77. [Google Scholar] [CrossRef]
- Daley, D.; Birchwood, J. ADHD and academic performance: Why does ADHD impact on academic performance and what can be done to support ADHD children in the classroom? Child Care Health Dev. 2010, 36, 455–464. [Google Scholar] [CrossRef]
- DuPaul, G.J.; Gormley, M.J.; Laracy, S.D. Comorbidity of LD and ADHD: Implications of DSM-5 for assessment and treatment. J. Learn. Disabil. 2013, 46, 43–51. [Google Scholar] [CrossRef]
- Tannock, R. Rethinking ADHD and LD in DSM-5: Proposed changes in diagnostic criteria. J. Learn. Disabil. 2013, 46, 5–25. [Google Scholar] [CrossRef] [PubMed]
- Berninger, V.W.; Richards, T.L.; Abbott, R.D. Differential diagnosis of dysgraphia, dyslexia, and OWL LD: Behavioral and neuroimaging evidence. Read. Writ. 2015, 28, 1119–1153. [Google Scholar] [CrossRef] [PubMed]
- Hamstra-Bletz, L.; Blöte, A.W. A longitudinal study on dysgraphic handwriting in primary school. J. Learn. Disabil. 1993, 26, 689–699. [Google Scholar] [CrossRef] [PubMed]
- Asselborn, T.; Chapatte, M.; Dillenbourg, P. Extending the spectrum of dysgraphia: A data driven strategy to estimate handwriting quality. Sci. Rep. 2020, 10, 3140. [Google Scholar] [CrossRef] [PubMed]
- Guilbert, J.; Alamargot, D.; Morin, M.F. Handwriting on a tablet screen: Role of visual and proprioceptive feedback in the control of movement by children and adults. Hum. Mov. Sci. 2019, 65, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, S.; Dror, G. Identifying developmental dysgraphia characteristics utilizing handwriting classification methods. IEEE Trans. Hum.-Mach. Syst. 2016, 47, 293–298. [Google Scholar] [CrossRef]
- Bartoň, M.; Fňašková, M.; Rektorová, I.; Mikl, M.; Mareček, R.; Rapcsak, S.Z.; Rektor, I. The role of the striatum in visuomotor integration during handwriting: An fMRI study. J. Neural Transm. 2020, 127, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Palmis, S.; Danna, J.; Velay, J.L.; Longcamp, M. Motor control of handwriting in the developing brain: A review. In Developmental Dysgraphia; Routledge: London, UK, 2019; pp. 123–140. [Google Scholar]
- Palmis, S.; Velay, J.L.; Habib, M.; Anton, J.L.; Nazarian, B.; Sein, J.; Longcamp, M. The handwriting brain in middle childhood. Dev. Sci. 2021, 24, e13046. [Google Scholar] [CrossRef]
- Brossard-Racine, M.; Majnemer, A.; Shevell, M.; Snider, L. Handwriting performance in children with attention deficit hyperactivity disorder (ADHD). J. Child. Neurol. 2008, 23, 399–406. [Google Scholar] [CrossRef]
- Brossard-Racine, M.; Shevell, M.; Snider, L.; Belanger, S.A.; Julien, M.; Majnemer, A. Persistent handwriting difficulties in children with ADHD after treatment with stimulant medication. J. Atten. Disord. 2015, 19, 620–629. [Google Scholar] [CrossRef]
- Graham, S.; Fishman, E.J.; Reid, R.; Hebert, M. Writing Characteristics of Students with Attention Deficit Hyperactive Disorder: A Meta-Analysis. Learn. Disabil. Res. Pract. 2016, 31, 75–89. [Google Scholar] [CrossRef]
- Mayes, S.D.; Frye, S.S.; Breaux, R.P.; Calhoun, S.L. Diagnostic, demographic, and neurocognitive correlates of dysgraphia in students with ADHD, autism, learning disabilities, and neurotypical development. J. Dev. Phys. Disabil. 2018, 30, 489–507. [Google Scholar] [CrossRef]
- Kaiser, M.L.; Schoemaker, M.M.; Albaret, J.M.; Geuze, R.H. What is the evidence of impaired motor skills and motor control among children with attention deficit hyperactivity disorder (ADHD)? Systematic review of the literature. Res. Dev. Disabil. 2015, 36, 338–357. [Google Scholar] [CrossRef] [PubMed]
- Lelong, M.; Zysset, A.; Nievergelt, M.; Luder, R.; Götz, U.; Schulze, C.; Wieber, F. How effective is fine motor training in children with ADHD? A scoping review. BMC Pediatr. 2021, 21, 490. [Google Scholar] [CrossRef] [PubMed]
- Shen, I.H.; Lee, T.Y.; Chen, C.L. Handwriting performance and underlying factors in children with Attention Deficit Hyperactivity Disorder. Res. Dev. Disabil. 2012, 33, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Adi-Japha, E.; Landau, Y.E.; Frenkel, L.; Teicher, M.; Gross-Tsur, V.; Shalev, R.S. ADHD and dysgraphia: Underlying mechanisms. Cortex 2007, 43, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Brossard-Racine, M.; Majnemer, A.; Shevell, M.; Snider, L.; Bélanger, S.A. Handwriting capacity in children newly diagnosed with attention deficit hyperactivity disorder. Res. Dev. Disabil. 2011, 32, 2927–2934. [Google Scholar] [CrossRef]
- Hung, Y.F.; Chang, C.J. The performance and predictors of Chinese character writing in children with attention deficit hyperactivity disorder. Res. Dev. Disabil. 2022, 126, 104244. [Google Scholar] [CrossRef]
- Tucha, O.; Lange, K.W. Handwriting and attention in children and adults with attention deficit hyperactivity disorder. Mot. Control 2004, 8, 461–471. [Google Scholar] [CrossRef]
- Rosenblum, S.; Epsztein, L.; Josman, N. Handwriting performance of children with attention deficit hyperactive disorders: A pilot study. Phys. Occup. Ther. Pediatr. 2008, 28, 219–234. [Google Scholar] [CrossRef]
- Brossard-Racine, M.; Shevell, M.; Snider, L.; Bélanger, S.A.; Majnemer, A. Motor skills of children newly diagnosed with Attention Deficit Hyperactivity Disorder prior to and following treatment with stimulant medication. Res. Dev. Disabil. 2012, 33, 2080–2087. [Google Scholar] [CrossRef] [PubMed]
- CASP. Critical Appraisal Skills Programme—Making Sense of Evidence about Clinical Effectiveness—Case-Control Studies. CASP. 2010. Available online: https://casp-uk.net/images/checklist/documents/archive/CASP-Randomised-Controlled-Trial-Checklist-2018_fillable_form.pdf (accessed on 23 February 2023).
- Åsberg Johnels, J.; Kopp, S.; Gillberg, C. Spelling difficulties in school-aged girls with attention-deficit/hyperactivity disorder: Behavioral, psycholinguistic, cognitive, and graphomotor correlates. J. Learn. Disabil. 2014, 47, 424–434. [Google Scholar] [CrossRef] [PubMed]
- Borella, E.; Chicherio, C.; Re, A.M.; Sensini, V.; Cornoldi, C. Increased intraindividual variability is a marker of ADHD but also of dyslexia: A study on handwriting. Brain Cogn. 2011, 77, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Capodieci, A.; Lachina, S.; Cornoldi, C. Handwriting difficulties in children with attention deficit hyperactivity disorder (ADHD). Res. Dev. Disabil. 2018, 74, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Capodieci, A.; Serafini, A.; Dessuki, A.; Cornoldi, C. Writing abilities and the role of working memory in children with symptoms of attention deficit and hyperactivity disorder. Child. Neuropsychol. 2019, 25, 103–121. [Google Scholar] [CrossRef] [PubMed]
- Dirlikov, B.; Younes, L.; Nebel, M.B.; Martinelli, M.K.; Tiedemann, A.N.; Koch, C.A.; Fiorilli, D.; Bastian, A.J.; Denckla, M.D.; Miller, M.I.; et al. Novel automated morphometric and kinematic handwriting assessment: A validity study in children with ASD and ADHD. J. Occup. Ther. Sch. Early Interv. 2017, 10, 185–201. [Google Scholar] [CrossRef]
- Farhangnia, S.; Hassanzadeh, R.; Ghorbani, S. Handwriting Performance of Children with Attention Deficit Hyperactivity Disorder: The Role of Visual-Motor Integration. Int. J. Pediatr. 2020, 8, 12317–12326. [Google Scholar]
- Flapper, B.C.; Houwen, S.; Schoemaker, M.M. Fine motor skills and effects of methylphenidate in children with attention-deficit–hyperactivity disorder and developmental coordination disorder. Dev. Med. Child. Neurol. 2006, 48, 165–169. [Google Scholar] [CrossRef]
- Frings, M.; Gaertner, K.; Buderath, P.; Christiansen, H.; Gerwig, M.; Hein-Kropp, C.; Schoch, B.; Hebebrand, J.; Timmann, D. Megalographia in children with cerebellar lesions and in children with attention-deficit/hyperactivity disorder. Cerebellum 2010, 9, 429–432. [Google Scholar] [CrossRef]
- Johnson, B.P.; Papadopoulos, N.; Fielding, J.; Tonge, B.; Phillips, J.G.; Rinehart, N.J. A quantitative comparison of handwriting in children with high-functioning autism and attention deficit hyperactivity disorder. Res. Autism Spectr. Disord. 2013, 7, 1638–1646. [Google Scholar] [CrossRef]
- Langmaid, R.A.; Papadopoulos, N.; Johnson, B.P.; Phillips, J.G.; Rinehart, N.J. Handwriting in children with ADHD. J. Atten. Disord. 2014, 18, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Langmaid, R.A.; Papadopoulos, N.; Johnson, B.P.; Phillips, J.; Rinehart, N.J. Movement scaling in children with ADHD-combined type. J. Atten. Disord. 2016, 20, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Laniel, P.; Faci, N.; Plamondon, R.; Beauchamp, M.H.; Gauthier, B. Kinematic analysis of fast pen strokes in children with ADHD. Appl. Neuropsychol. Child. 2020, 9, 125–140. [Google Scholar] [CrossRef] [PubMed]
- Lotfy, A.S.; Darwish ME, S.; Ramadan, E.S.; Sidhom, R.M. The incidence of dysgraphia in Arabic language in children with attention-deficit hyperactivity disorder. Egypt. J. Otolaryngol. 2021, 37, 115. [Google Scholar] [CrossRef]
- Okuda, P.M.M.; Pinheiro, F.H.; Germano, G.D.; Padula, N.A.d.M.R.; Lourencetti, M.D.; Santos, L.C.A.d.; Capellini, S.A. Fine motor, sensory and perceptive function of students with attention deficit disorder with hyperactivity. J. Da Soc. Bras. De. Fonoaudiol. 2011, 23, 351–357. [Google Scholar] [CrossRef]
- Tucha, O.; Lange, K.W. Effects of methylphenidate on kinematic aspects of handwriting in hyperactive boys. J. Abnorm. Child. Psychol. 2001, 29, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Yoshimasu, K.; Barbaresi, W.J.; Colligan, R.C.; Killian, J.M.; Voigt, R.G.; Weaver, A.L.; Katusic, S.K. Written-language disorder among children with and without ADHD in a population-based birth cohort. Pediatrics 2011, 128, e605–e612. [Google Scholar] [CrossRef]
- Zanone, P.-G.; Athènes, S.; Sallagoity, I.; Albaret, J.-M. Switching among Graphic Patterns is Governed by Coordination Dynamics of Handwriting. In Proceedings of the 12th Biennial Conference of the International Graphonomics Society, Salerno, Italy, 26–29 June 2005; pp. 255–260. [Google Scholar]
- Coradinho, H.; Melo, F.; Almeida, G.; Veiga, G.; Marmeleira, J.; Teulings, H.L.; Matias, A.R. Relationship between Product and Process Characteristics of Handwriting Skills of Children in the Second Grade of Elementary School. Children 2023, 10, 445. [Google Scholar] [CrossRef]
- Lopez, C.; Hemimou, C.; Golse, B.; Vaivre-Douret, L. Developmental dysgraphia is often associated with minor neurological dysfunction in children with developmental coordination disorder (DCD). Neurophysiol. Clin. 2018, 48, 207–217. [Google Scholar] [CrossRef]
- O’Hare, A.; Khalid, S. The association of abnormal cerebellar function in children with developmental coordination disorder and reading difficulties. Dyslexia 2022, 8, 234–248. [Google Scholar] [CrossRef]
- Bieber, E.; Smits-Engelsman, B.C.; Sgandurra, G.; Cioni, G.; Feys, H.; Guzzetta, A.; Klingels, K. Manual function outcome measures in children with developmental coordination disorder (DCD): Systematic review. Res. Dev. Disabil. 2016, 55, 114–131. [Google Scholar] [CrossRef] [PubMed]
- Biotteau, M.; Danna, J.; Baudou, É.; Puyjarinet, F.; Velay, J.L.; Albaret, J.M.; Chaix, Y. Developmental coordination disorder and dysgraphia: Signs and symptoms, diagnosis, and rehabilitation. Neuropsychiatr. Dis. Treat. 2019, 15, 1873–1885. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, S.; Parush, S.; Weiss, P.L. Computerized temporal handwriting characteristics of proficient and non-proficient handwriters. Am. J. Occup. Ther. 2003, 57, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Feder, K.P.; Majnemer, A. Children’s handwriting evaluation tools and their psychometric properties. Phys. Occup. Ther. Pediatr. 2003, 23, 65–84. [Google Scholar] [CrossRef] [PubMed]
- Rothe, J.; Kattlun, F.A.; Kaufmann, J.; Uhlmann, A.; Wanderer, S.; Bluschke, A.; Beste, C.; Roessner, V. Effects of methylphenidate and physiotherapeutic treatment on graphomotor movements in children with ADHD. Eur. Child. Adolesc. Psychiatry 2023. [Google Scholar] [CrossRef] [PubMed]
- Kuntsi, J.; Klein, C. Intraindividual Variability in ADHD and Its Implications for Research of Causal Links. In Behavioral Neuroscience of Attention Deficit Hyperactivity Disorder and Its Treatment; Springer: Berlin/Heidelberg, Germany, 2012; pp. 67–91. [Google Scholar]
- Vaivre-Douret, L.; Lalanne, C.; Ingster-Moati, I.; Boddaert, N.; Cabrol, D.; Dufier, J.L.; Golse, B.; Falissard, B. Subtypes of developmental coordination disorder: Research on their nature and etiology. Dev. Neuropsychol. 2011, 36, 614–643. [Google Scholar] [CrossRef] [PubMed]
- Karlsdottir, R.; Stefansson, T. Problems in developing functional handwriting. Percept. Mot. Ski. 2002, 94, 623–662. [Google Scholar] [CrossRef] [PubMed]
- Maeland, A.F. Handwriting and perceptual-motor skills in clumsy, dysgraphic, and normal children. Percept. Mot. Ski. 1992, 75, 1207–1217. [Google Scholar]
- Naider-Steinhart, S.; Katz-Leurer, M. Analysis of proximal and distal muscle activity during handwriting tasks. Am. J. Occup. Ther. 2007, 61, 392–398. [Google Scholar] [CrossRef]
- Katusic, S.K.; Colligan, R.C.; Weaver, A.L.; Barbaresi, W.J. The forgotten learning disability: Epidemiology of written-language disorder in a population-based birth cohort (1976–1982), Rochester, Minnesota. Pediatrics 2009, 123, 1306–1313. [Google Scholar] [CrossRef]
- Lopez, C.; Vaivre-Douret, L. Exploratory Investigation of Handwriting Disorders in School-Aged Children from First to Fifth Grade. Children 2023, 10, 1512. [Google Scholar] [CrossRef] [PubMed]
- Gannetion, L.; Wong, K.Y.; Lim, P.Y.; Chang, K.H.; Abdullah AF, L. An exploratory study on the handwritten allographic features of multi-ethnic population with different educational backgrounds. PLoS ONE 2022, 17, e0268756. [Google Scholar] [CrossRef] [PubMed]
- Danna, J.; Paz-Villagrán, V.; Velay, J.L. Signal-to-Noise velocity peaks difference: A new method for evaluating the handwriting movement fluency in children with dysgraphia. Res. Dev. Dsabilities 2013, 34, 4375–4384. [Google Scholar] [CrossRef]
- Paz-Villagrán, V.; Danna, J.; Velay, J.L. Lifts and stops in proficient and dysgraphic handwriting. Hum. Mov. Sci. 2014, 33, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Gemelli, A.; Marinai, S.; Vivoli, E.; Zappaterra, T. Deep-Learning for Dysgraphia Detection in Children Handwritings. In Proceedings of the ACM Symposium on Document Engineering 2023, Limerick, Ireland, 22–25 August 2023; pp. 1–4. [Google Scholar]
- Faraone, S.V.; Asherson, P.; Banaschewski, T.; Biederman, J.; Buitelaar, J.K.; Ramos-Quiroga, J.A.; Rohde, L.A.; Sonuga-Barke, E.J.; Tannock, R.; Franke, B. Attention-deficit/hyperactivity disorder. Nat. Rev. Dis. Primers 2015, 1, 15020. [Google Scholar] [CrossRef] [PubMed]
- Mergl, R.; Juckel, G.; Rihl, J.; Henkel, V.; Karner, M.; Tigges, P.; Schröter, A.; Hegerl, U. Kinematical analysis of handwriting movements in depressed patients. Acta Psychiatr. Scand. 2004, 109, 383–391. [Google Scholar] [CrossRef]
- Cousins, M.; Smyth, M.M. Developmental coordination impairments in adulthood. Hum. Mov. Sci. 2003, 22, 433–459. [Google Scholar] [CrossRef]
- Willcutt, E.G. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: A meta-analytic review. Neurotherapeutics 2012, 9, 490–499. [Google Scholar] [CrossRef]
- Doyle, S.; Wallen, M.; Whitmont, S. Motor skills in Australian children with attention deficit hyperactivity disorder. Occup. Ther. Int. 1995, 2, 229–240. [Google Scholar] [CrossRef]
- Elia, J.; Arcos-Burgos, M.; Bolton, K.L.; Ambrosini, P.J.; Berrettini, W.; Muenke, M. ADHD latent class clusters: DSM-IV subtypes and comorbidity. Psychiatry Res. 2009, 170, 192–198. [Google Scholar] [CrossRef]
- Feder, K.P.; Majnemer, A. Handwriting development, competency, and intervention. Dev. Med. Child. Neurol. 2007, 49, 312–317. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, P.; Dempsey, M.; Killeen, H. Handwriting speed: Duration of testing period and relation to socio-economic disadvantage and handedness. Occup. Ther. Int. 2008, 15, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Vlachos, F.; Bonoti, F. Handedness and writing performance. Percept. Mot. Ski. 2004, 98, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Thapar, A.; Martin, J.; Mick, E.; Arias Vásquez, A.; Langley, K.; Scherer, S.W.; Schachar, R.; Crosbie, J.; Williams, N.; Franke, B.; et al. Psychiatric gene discoveries shape evidence on ADHD’s biology. Mol. Psychiatry 2016, 21, 1202–1207. [Google Scholar] [CrossRef] [PubMed]
- Danielson, M.L.; Visser, S.N.; Chronis-Tuscano, A.; DuPaul, G.J. A national description of treatment among United States children and adolescents with attention-deficit/hyperactivity disorder. J. Pediatr. 2018, 192, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Froehlich, T.E.; Fogler, J.; Barbaresi, W.J.; Elsayed, N.A.; Evans, S.W.; Chan, E. Using ADHD medications to treat coexisting ADHD and reading disorders: A systematic review. Clin. Pharmacol. Ther. 2018, 104, 619–637. [Google Scholar] [CrossRef]
- Gangadhar, G.; Joseph, D.; Chakravarthy, V.S. An oscillatory neuromotor model of handwriting generation. Int. J. Doc. Anal. Recognit. 2007, 10, 69–84. [Google Scholar] [CrossRef]
- Feldman, A.G.; Latash, M.L. Testing hypotheses and the advancement of science: Recent attempts to falsify the equilibrium point hypothesis. Exp. Brain Res. 2005, 161, 91–103. [Google Scholar] [CrossRef]
- Schmidt, R.A.; Lee, T.D.; Winstein, C.; Wulf, G.; Zelaznik, H.N. Motor Control and Learning: A Behavioral Emphasis; Human Kinetics: Champaign, IL, USA, 2018. [Google Scholar]
- Van Galen, G.P.; Teulings, H.L. The independent monitoring of form and scale factors in handwriting. Acta Psychol. 1983, 54, 9–22. [Google Scholar] [CrossRef]
- Kelso, J.S. Dynamic Patterns: The Self-Organization of Brain and Behavior; The MIT Press: Cambridge, MA, USA, 1995. [Google Scholar]
- Plamondon, R.; Djioua, M. A multi-level representation paradigm for handwriting stroke generation. Hum. Mov. Sci. 2006, 25, 586–607. [Google Scholar] [CrossRef]
- Engelbrecht, S.E. Minimum principles in motor control. J. Math. Psychol. 2001, 45, 497–542. [Google Scholar] [CrossRef] [PubMed]
- Wada, Y.; Kawato, M. A theory for cursive handwriting based on the minimization principle. Biol. Cybern. 1995, 73, 3–13. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section | Question | Formulation |
|---|---|---|
| A: Are the results of the trial valid? | 1 | Did the study address a clearly focused issue? |
| 2 | Did the authors use an appropriate method to answer their question? | |
| 3a | Were the cases recruited in an acceptable way? | |
| 3b | Was there a sufficient number of cases selected? | |
| 4 | Were the control groups selected in an acceptable way? | |
| 5 | Was the exposure clearly defined and accurately measured? | |
| 6 | Have the authors taken account of the potential confounding factors in the design and/or in their analysis? | |
| B: What are the results? | 7 | Was the group effect large? |
| 8 | Was the estimate of the group effect precise? | |
| 9 | Do you believe the results? | |
| C: Would the results help locally? | 10 | Can the results be applied to the local population? |
| 11 | Do the results of this study fit with other available evidence? |
| Methodological Quality | Presentation of Results | External Validity | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3a | 3b | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
| Adi-Japha et al., 2007 [28] | Y | Y | Y | Y | Y | Y | Y | C | N | Y | C | Y |
| Åsberg Johnels et al., 2014 [35] | Y | Y | Y | Y | Y | Y | Y | C | N | Y | Y | Y |
| Borella et al., 2011 [36] | Y | Y | C | Y | Y | Y | Y | C | C | Y | Y | Y |
| Capodieci et al., 2018 [37] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Capodieci et al., 2019 [38] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Dirlikov et al., 2017 [39] | Y | Y | Y | Y | Y | Y | Y | C | N | Y | Y | Y |
| Farhangnia et al., 2020 [40] | Y | Y | C | Y | Y | Y | N | C | N | C | C | Y |
| Flapper et al., 2006 [41] | Y | Y | Y | N | Y | Y | Y | C | N | C | Y | Y |
| Frings et al., 2010 [42] | Y | Y | C | N | Y | Y | N | C | N | C | C | Y |
| Hung and Chang, 2022 [30] | Y | Y | C | Y | Y | Y | C | Y | Y | Y | Y | Y |
| Johnson et al., 2013 [43] | Y | Y | Y | N | Y | Y | Y | C | N | Y | Y | Y |
| Langmaid et al., 2014 [44] | Y | Y | Y | N | Y | Y | Y | N | Y | Y | Y | Y |
| Langmaid et al., 2016 [45] | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y |
| Laniel et al., 2020 [46] | Y | Y | N | N | Y | Y | N | Y | Y | C | C | Y |
| Lofty et al., 2011 [47] | Y | Y | C | Y | C | Y | C | C | N | Y | C | Y |
| Okuda et al., 2011 [48] | Y | Y | Y | N | Y | Y | C | C | N | C | C | Y |
| Rosenblum et al., 2008 [32] | Y | Y | Y | N | Y | Y | C | C | N | C | C | Y |
| Shen et al., 2012 [27] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Tucha and Lange, 2001 [49] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Tucha and Lange, 2004 [31] | Y | Y | Y | N | Y | Y | Y | C | N | Y | C | Y |
| Yoshimasu et al., 2011 [50] | Y | Y | Y | Y | Y | Y | N | C | N | Y | C | Y |
| Study | Participants (ADHD and Controls) | Experimental Group | Mean Age (SD) | Gender (Male, Female) | Control Group | Mean Age (SD) | Gender | Inclusion and Exclusion Criteria for ADHD | ADHD Presentation | Medication (Psycho-stimulant) | Handwriting Measures | Q (Quality) S (Speed) P (Process) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adi-Japha et al., 2007 [28] | 40 | 20 | 12.2 (5.7) | 20 M | 20 | 12.8 (3.6) | 20 M | Inclusion criteria: formal diagnosis of ADHD, IQ score > 85, performance within 1.6 SD on a reading test; Exclusion criteria: reading problems. | ADHD/C | Off-state for at least a week before the experiment. | Graphic production on a digitizing tablet; Letters production. | Q and P |
| Åsberg Johnels et al., 2014 [35] | 55 | 20 | 10 to 16 | 20 F | 35 | 10 to 16 | 35 F | Inclusion criteria: formal diagnosis of ADHD, IQ score > 69; Exclusion criteria: ASD, neuropsychiatric and neurodevelopmental disorders, learning disabilities. | n.s | No medication | FTF; Parental ratings. | Q |
| Borella et al., 2011 [36] | 30 | 15 | 9.3 (1.4) | 12 M; 4 F | 15 | 9.4 (1.4) | 12 M; 3 F | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: IQ score < 85, MPH medication, learning disability, mathematical or reading disorders, neurological, sensory, motor, psychiatric or mood disorders. | 5 ADHD/I; 10 ADHD/C | No medication | Batteria per la valutazione delle competenze ortografiche nella scuola dell’obbligo; Continuous letters production. | S and P |
| Capodieci et al., 2018 [37] | 32 | 16 | 10.5 (6.9) | 12 M; 4 F | 16 | 10.1 (6.4) | 12 M; 4 F | Inclusion criteria: formal diagnosis of ADHD for only one child, all others on the basis of an ad-hoc questionnaire; Exclusion criteria: Neurological, psychiatric or serious psychological problems; No child had a learning disability. | n.s | No medication | BVSCO-2; Words production. | Q, S and P |
| Capodieci et al., 2019 [38] | 52 | 26 | 9.6 (1.2) | 22 M; 4 F | 26 | 9.3 (1.1) | n.s | Inclusion criteria: formal diagnosis of ADHD for all but 3 children; Exclusion criteria: neurological or psychological problems, learning disorders. | 10 ADHD/I; 10 ADHD/C; 6 ADHD/HI | No medication | BVSCO-2; Dictation tasks; Sentences and words production; Handwriting legibility scale. | Q, S and P |
| Dirlikov et al., 2017 [39] | 167 | 45 | 9.9 (1.2) | 39 M; 6 F | 65 | 9.9 (1.1) | 56 M; 9 F | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: intellectual disability, seizures, neurological, chronic medical, genetic, psychiatric (except ODD), speech-related, autistic or psychotic disorders. | 7 ADHD/I; 38 ADHD/C | Off-state for at least 24 h before the experiment. | MHA; Copy task. | Q, S and P |
| Farhangnia et al., 2020 [40] | 48 | 24 | 8.0 (0.7) | 17 M; 7 F | 24 | 8.1 (0.6) | 17 M; 7 F | n.s | n.s | n.s | PHAT; Copy task and dictation task. | Q and S |
| Flapper et al., 2006 [41] | 24 | 12 | 9.8 (1.7) | 11 M; 1 F | 12 | 9.7 (1.2) | 11 M; 1 F | Inclusion criteria: formal diagnosis of ADHD+DCD; Exclusion criteria: learning, neurological or psychiatric disorders, IQ score < 70. | 6 ADHD/I; 4 ADHD/C; 2 ADHD/HI | Off-state for the first assessment; On-state for 4 to 5 weeks for the second assessment. | BHK; Copy task. | Q and S |
| Frings et al., 2010 [42] | 21 | 10 | 12.3 (1.3) | 10 M | 11 | 12.1 (1.8) | 9 M; 2 F | Inclusion criteria: formal diagnosis of ADHD. | 10 ADHD/C | On-state | Copy task | Q |
| Hung and Chang, 2022 [30] | 60 | 30 | 7.1 (0.5) | 16 M; 14 F | 30 | 7.2 (0.5) | 16 M; 14 F | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: ASD, seizure disorder, IQ < 80, mental retardation, mood disorders, anxiety or psychotic disorders. | 9 ADHD/I; 18 ADHD/C; 3 ADHD/HI | n.s | BCBL; Copy task and dictation task. | Q, S and P |
| Johnson et al., 2013 [43] | 35 | 14 | 11.0 (1.95) | 14 M | 21 | 11.0 (2.1) | 21 M | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: medical, sensory, genetic or neurodevelopmental disorders, intellectual disability. | 14 ADHD/C | Off-state for at least 24 to 72 h before the experiment. | HPT; Copy task. | Q, S and P |
| Langmaid et al., 2014 [44] | 28 | 14 | 10.9 (2.0) | 14 M | 14 | 10.6 (2.3) | 14 M | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: medical, sensory, genetic or neurodevelopmental disorders, intellectual disability. | 14 ADHD/C | Off-state for at least 24 to 72 h before the experiment. | Cursive letters production on a digitizing tablet. | P |
| Langmaid et al., 2016 [45] | 28 | 14 | 10.8 (2.0) | 14 M | 14 | 10.5 (2.2) | 14 M | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: medical, sensory, genetic or neurodevelopmental disorders, intellectual disability. | 14 ADHD/C | Off-state for at least 24 to 72 h before the experiment. | Cursive letters production at 10 mm and 40 mm on a digitizing tablet. | P |
| Laniel et al., 2020 [46] | 25 | 12 | 9.5 (1.1) | 8 M; 4 F | 12 | 9.9 (1.3) | 6 M; 6 F | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: Intellectual disability; One child had ODD and an anxiety disorder, another had dyspraxia. | n.s | On-state | BHK; Copy task; Pen-stroke test on a digitizing tablet. | Q, S and P |
| Lofty et al., 2011 [47] | 40 | 20 | 7.8 (1.2) | n.s | 20 | 7.8 (1.2) | 20 M | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: sensory or psychiatric disorders; 60% of included children met criteria for dyslexia. | n.s | n.s | DDS; Copy task. | Q |
| Okuda et al., 2011 [48] | 22 | 11 | 8.6 to 11.6 | 11 M | 11 | n.s | n.s | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: sensory or psychiatric disorders. | n.s | On-state | Scale of dysgraphia | Q |
| Rosenblum et al., 2008 [32] | 24 | 12 | 8 to 10 | 10 M; 2 F | 12 | 8 to 10 | 10 M; 2 F | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: another medical diagnosis. | n.s | On-state | HHE on a digitizing tablet; Copy task. | Q, S and P |
| Shen et al., 2012 [27] | 42 | 21 | 8.5 (1.2) | 17 M; 4 F | 21 | 8.5 (1.0) | 17 M; 4 F | Inclusion criteria: formal diagnosis of ADHD, with possible ODD and CD in the ADHD group; Exclusion criteria: epilepsy, severe anxiety, psychotic disorder, DCD (score < 15th percentile on the M-ABC 2). | 6 ADHD/I; 10 ADHD/C; 5 ADHD/HI | Off-state for at least 24 h before the experiment. | THPS; BRWT; Copy task and dictation task on a digitizing tablet. | Q, S and P |
| Tucha and Lange, 2001 [49] | 42 | 21 | 10.7 (0.4) | 21 M | 21 | 10.5 (0.4) | 21 M | Inclusion criteria: formal diagnosis of ADHD, with medication; Exclusion criteria: Concurrent psychotropic medications, ADHD/I or ADHD/HI, reading disability or spelling disorder; Four children had a mathematics disability. | 21 ADHD/C | Off-state for at least 10 h before the experiment and on-state 1 h after the administration. | Copy task and dictation task on a digitizing tablet. | Q and P |
| Tucha and Lange, 2004 [31] | 20 | 10 | 9.9 (n.s) | 5 M; 5 F | 10 | 9.9 (n.s) | 5 M; 5 F | Inclusion criteria: formal diagnosis of ADHD, with possible ODD and CD in the ADHD group; Exclusion criteria: neurological and psychiatric disorders. | n.s | On-state | Sentences production on a digitizing tablet. | P |
| Yoshimasu et al., 2011 [50] | 5699 | 379 | 10.4 (4.6) | 284 M; 95 F | 5320 | n.s | 2666 M; 2654 F | Inclusion criteria: retrospective cohort-based study which has sought formal diagnosis of ADHD (based on DSM criteria); Exclusion criteria: IQ score < 50, written language disorder with or without reading disability. | n.s | Possible medication | Information retrieved from individualized education program goals for written language and/or specific writing subtest scores ≤ 90; Legibility and/or writing subtest scores. | Q |
| Study | Main Results |
|---|---|
| Adi-Japha et al., 2007 [28] | ADHD children made more errors regarding letter insertions, substitutions, transpositions and omissions, produced confusedly shaped letters and replaced the end-of-word letter with its simpler and more common middle-of-the-word version; Speed of handwriting did not differ between groups; No difference considering spatial features; ADHD children displayed poor time utilization, and produced inconsistent and disproportionate writing accompanied by high levels of pressure and multiple corrections; Handwriting problems were associated with attentional problems and reflected an impairment of the graphemic buffer and of kinematic motor production. |
| Åsberg Johnels et al., 2014 [35] | ADHD children obtained lower scores on parental ratings of handwriting. |
| Borella et al., 2011 [36] | ADHD children produced fewer writing sequences than the control groups; ADHD children showed greater IIV than control groups. |
| Capodieci et al., 2018 [37] | No difference between groups considering handwriting speed; In conditions without WM interference, ADHD children produced about 10% fewer graphemes than control groups; In the spatial condition, the difference between groups was slightly greater (−20%), though not statistically significant; In the verbal condition, ADHD children wrote significantly more slowly (−38%) than control groups; The handwriting of ADHD children was generally less legible than the control groups, especially in the verbal and spatial conditions; ADHD group had a higher IIV in the verbal condition than the control groups; High IIV influenced the reduced speed in the case of the verbal condition for both groups. |
| Capodieci et al., 2019 [38] | ADHD children made more spelling mistakes than control groups in all conditions; ADHD children who better coped with a concurrent verbal WM load had better spelling performance; ADHD children obtained lower scores for handwriting quality than control groups; No difference between groups in terms of writing speed. |
| Dirlikov et al., 2017 [39] | ADHD children showed worse letter-form scores compared to control groups across conditions (copy, trace and fast trace); No difference in letter-spacing errors between groups; ADHD children made fewer speed inflections across conditions compared to control groups; Both groups showed a significant correlation between letter form and WM performance in the copy condition only. |
| Farhangnia et al., 2020 [40] | For the copy task, ADHD children had lower global legibility scores compared to control groups; No significant difference between the two groups in terms of space, alignment, size of letters and slant components of writing, as well as for speed of writing; For the dictation task, ADHD children had lower legibility scores compared to control groups, while there was no difference between the groups in terms of space, alignment and slant components and size of letters. |
| Flapper et al., 2006 [41] | ADHD+DCD children showed lower scores for quality of handwriting, but there was no difference in speed of handwriting between groups; When on-state, of the 11 children with ADHD+DCD who could be assessed a second time, 6 improved their handwriting quality on the BHK, 4 did not improve and one child deteriorated When assessed off-state, ADHD+DCD children did not improve their handwriting speed. |
| Frings et al., 2010 [42] | Mean letter height did not differ between groups; Letter height increased during repeated writing of the same sentence in the ADHD group only. |
| Hung and Chang, 2022 [30] | ADHD children had poorer writing performance than the control groups for both character dictation and character copying; ADHD children wrote less fluently and correctly compared to the control groups; Inattention was the stronger predictor of character dictation in ADHD children; Manual dexterity was significantly correlated with character copying in the ADHD group. |
| Johnson et al., 2013 [43] | ADHD children made more total handwriting errors than control groups (i.e., correction and formation errors); No difference between groups in average height or width; No difference in the coefficient of variability of phrase height and width; No difference in average word spacing; ADHD children included additional strokes more often than control groups; There was a trend towards significant difference between the groups in terms of speed of handwriting, yet it was not significant; In the ADHD group, more corrections were associated with slower handwriting speed and maturational processes contributed to handwriting performance. |
| Langmaid et al., 2014 [44] | ADHD children were more variable in terms of stroke length and showed inconsistent stroke height when compared to the control groups; No difference in the other kinematic variables; Symptom severity scores were correlated to variability of stroke height (vertical size); Higher scores on the inattentive and total ADHD subtests were significantly correlated with more variable writing size; Stroke duration was significantly related to hyperactive behavior, such that a more hyperactive child had strokes of shorter duration (faster writing); Ballisticity was significantly associated with hyperactive behavior (more ballistic movement when symptoms of hyperactivity increased). |
| Langmaid et al., 2016 [45] | Despite both groups being significantly more inaccurate on the 40 mm task compared to the 10 mm, ADHD children were unable to maintain the size of their cursive letter at the 40 mm size, contrary to control groups; Groups were comparable on the 10 mm task; ADHD children had more ballistic movements on both tasks; Only pen pressure was positively correlated with inattention scores during the 10 mm task. |
| Laniel et al., 2020 [46] | ADHD children showed poorer performance on quality scores (BHK), lower writing speed and higher writing size than control groups; On the Pen-stroke test, ADHD children displayed poorer motor planning and execution and greater variability in motor control than the control groups; In the ADHD group only, motor planning on the handwriting task correlated with speed of handwriting on the BHK (the faster a child wrote, the shorter the motor production delay); ADHD children showed greater amplitude of movement on the Pen-stroke test, which was associated with faster motor speed; No relationship between inattention and hyperactivity symptoms with motor control skills was measured for the Pen-stroke test. |
| Lofty et al., 2011 [47] | A total of 10% of ADHD children had normal handwriting with no disability, 40% had excellent handwriting with a minimum of disability and 50% of ADHD children showed mild to moderate handwriting disability; ADHD children had poorer performance in respecting lines, spacing between words, letter direction, spelling a sentence and punctuation (item of the DDS); No difference between males and females in the ADHD group only on DDS scores; No correlation between DDS scores and age in the ADHD group only. |
| Okuda et al., 2011 [48] | ADHD children manifested poorer performance regarding flowing lines, descending lines, retouched letters, curvatures and angles of “m”, “n” and “u” letters; They produced more collisions and adherences, sudden movements, irregular sizes and incorrect forms of letters. |
| Rosenblum et al., 2008 [32] | Poorer performance of ADHD children on most handwriting process and product measures when off-state versus on-state; When off-medication, ADHD children showed more total time and more in-air time than when on-medication and compared to control groups; No difference in handwriting speed when on-state and off-state were compared, while on-state and off-state ADHD children wrote faster than control groups; No difference in product handwriting between on-state and off-state, but ADHD children, regardless of on- or off-state, differed in comparison to control groups. |
| Shen et al., 2012 [27] | ADHD children scored lower on THSPC and on BSRWT; Despite the speed of writing per se being no different between the two groups, ADHD children spent more on-paper time on the copy task and, hence, needed more time to finish a copy task. |
| Tucha and Lange, 2001 [49] | When off-state, the quality of handwriting specimens of hyperactive boys was poorer than on-state but more fluent; When off-state, ADHD children did not differ from control groups in handwriting movements; Hyperactive behavior improvement through MPH was associated with increased legibility and greater accuracy of handwriting. |
| Tucha and Lange, 2004 [31] | When on-state, ADHD children displayed significantly more inversions in the direction of their velocity profiles than control groups; When off-state, there was no difference between the groups; The medication resulted in increased dysfluency during handwriting. |
| Yoshimasu et al., 2011 [50] | ADHD girls tended to have a single specific writing difficulty, whereas ADHD boys were more likely to have multiple writing difficulties (e.g., legibility + poor paragraph organization). |
| Recommendations | Level of Importance |
|---|---|
| Eligible Population | |
| Ensure a reasonable sample size necessary to conduct the study. | High |
| Verify the diagnosis of ADHD with a formal diagnosis following DSM-5 indications and the use of gold-standard tools. | High |
| Verify the diagnosis of HD using standardized, valid and reliable tools. | High |
| Harmonize the comparator group(s) with previous studies to facilitate comparison: | |
| ADHD only; | High |
| HD only; | High |
| Typical. | High |
| Harmonize the reference group with previous studies to facilitate comparison: | |
| ADHD + HD. | High |
| Ensure children acceptability (motivation to study participation). | Low |
| Subgroup Analysis | |
| Consider demographic characteristics: | |
| Age; | High |
| Gender; | High |
| Handless; | Low |
| IQ. | High |
| Socioeconomic factors. | Low |
| Ethnicity. | Low |
| Cultural background. | Low |
| Include documentation of ADHD subtypes. | High |
| Screen for comorbid emotional or behavioral conditions (e.g., anxiety, depression, sleep disturbance). | High |
| Screen for comorbid neurodevelopmental conditions (e.g., learning and language disorders, autism spectrum disorders).s | High |
| Screen for comorbid physical conditions (e.g., tics). | Low |
| Treatment and Care | |
| Considered ADHD specific treatments. | |
| Methylphenidate. | High |
| Other medication. | Low |
| Behavioral interventions for treatment of ADHD or comorbidities. | High |
| Motor behavioral interventions (psychomotricity). | High |
| Expert Panel | |
| Harmonize measurement of key handwriting elements to facilitate pooling of and comparisons between study findings. | High |
| Use common outcome measures to facilitate pooling of and comparisons between study findings. | High |
| Supervise the experimental handwriting testing without knowing the child’s group (blind test). | Low |
| Assess the handwriting performance without knowing the child’s group (blind evaluation). | High |
| Assess the handwriting performance by an expert panel of experiment judges (two or more). | High |
| Theoretical Considerations | |
| Discuss clinical findings with more fundamental work addressing the theoretical models of handwriting applied to the specific context of ADHD. | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puyjarinet, F.; Chaix, Y.; Biotteau, M. Is There a Deficit in Product and Process of Handwriting in Children with Attention Deficit Hyperactivity Disorder? A Systematic Review and Recommendations for Future Research. Children 2024, 11, 31. https://doi.org/10.3390/children11010031
Puyjarinet F, Chaix Y, Biotteau M. Is There a Deficit in Product and Process of Handwriting in Children with Attention Deficit Hyperactivity Disorder? A Systematic Review and Recommendations for Future Research. Children. 2024; 11(1):31. https://doi.org/10.3390/children11010031
Chicago/Turabian StylePuyjarinet, Frédéric, Yves Chaix, and Maëlle Biotteau. 2024. "Is There a Deficit in Product and Process of Handwriting in Children with Attention Deficit Hyperactivity Disorder? A Systematic Review and Recommendations for Future Research" Children 11, no. 1: 31. https://doi.org/10.3390/children11010031
APA StylePuyjarinet, F., Chaix, Y., & Biotteau, M. (2024). Is There a Deficit in Product and Process of Handwriting in Children with Attention Deficit Hyperactivity Disorder? A Systematic Review and Recommendations for Future Research. Children, 11(1), 31. https://doi.org/10.3390/children11010031